
Abstract

To the Editor
Nitrous oxide (N2O) is a commonly abused inhalant that is legally obtained. It is associated with varied psychiatric complications including confusion, mania, depression, memory problems and hallucinations. N2O is known to precipitate Vitamin B12 deficiency, which can cause neurological complications such as myeloneuropathy, subacute degeneration of the spine and peripheral neuropathy (Garakani et al., 2016).
This case provides a novel presentation of significant N2O abuse resulting in co-occurring psychiatric and medical complications.
A 45-year-old male was admitted to an acute psychiatric unit with florid psychosis, presenting with persecutory delusions of control and vivid visual hallucinations. A fluctuating course was noted, with episodic periods of severe distress and paranoia. There was a history of significant N2O abuse. Up to 480 N2O cream charger bulbs were inhaled via whipped cream canister per session. Psychiatric history was significant for a brief psychotic episode in the context of nitrous oxide abuse, although Vitamin B12 levels were not measured.
Biochemistry results were significant for absolute and functional Vitamin B12 deficiency, with a low serum Vitamin B12 and raised homocysteine level (Table 1). As Vitamin B12 has a role in the reduction of homocysteine, raised homocysteine indicates a functional Vitamin B12 deficiency. This can occur in the absence of an absolute Vitamin B12 deficiency (Weinberger et al., 2001). Intrinsic factor and parietal cell antibodies were negative.
Biochemistry Results.
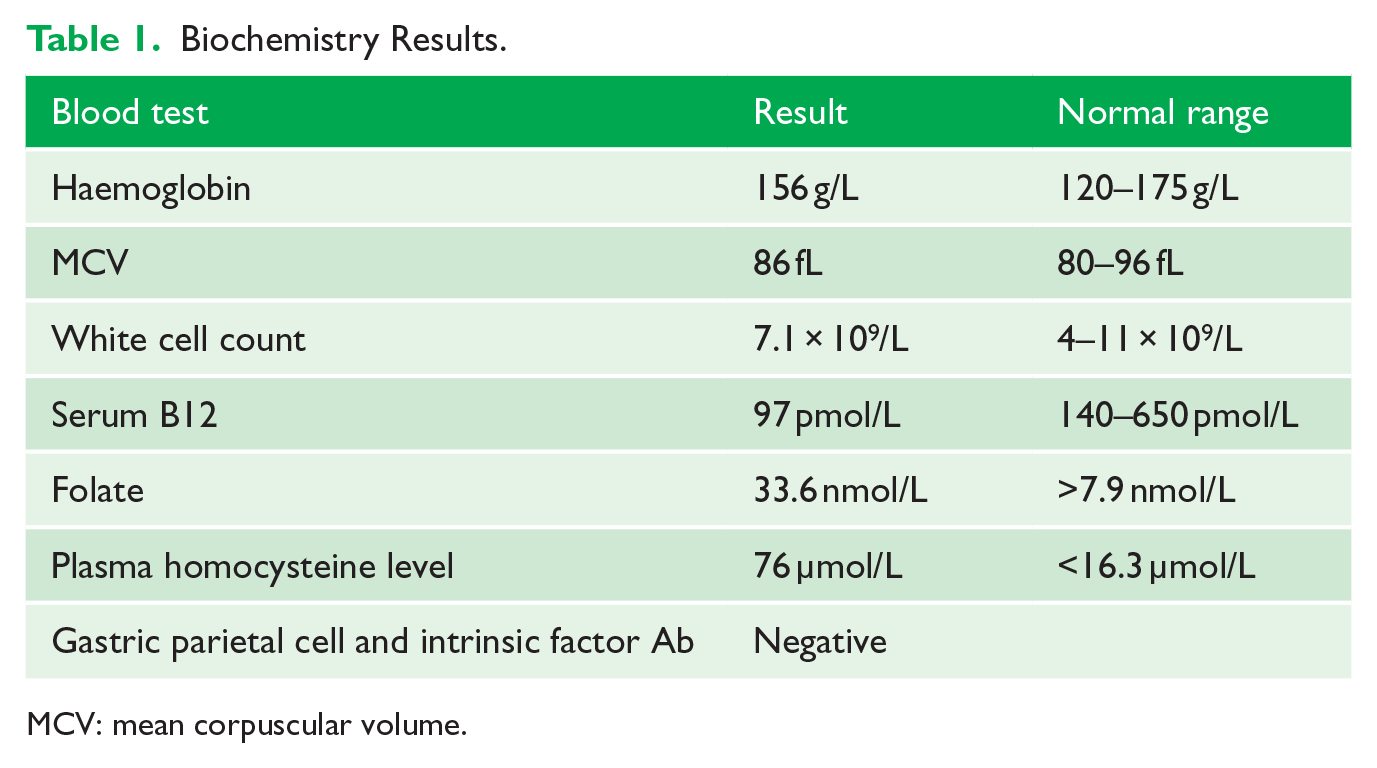
MCV: mean corpuscular volume.
Prior to his admission, intermittent paraesthesia, sharp leg pains and short-term memory issues were described. Neurological examination was significant for a broad-based gait, reduced power to plantar and dorsiflexion (4/5), reduced lower limb reflexes and reduced vibration sense. Nerve conduction studies found electrophysiological evidence of a length-dependent sensorimotor axonal neuropathy of the lower limbs. This was consistent with a peripheral neuropathy secondary to Vitamin B12 deficiency. A multisequence magnetic resonance imaging (MRI) of brain did not demonstrate classical radiological hallmarks of Vitamin B12 deficiency, but did reveal mild generalised cerebral atrophy.
Initial treatment with multiple high-dose antipsychotics, including intramuscular zuclopenthixol acetate 100 mg, showed no improvement in symptoms. On commencement of intramuscular hydroxycobalamin 1000 µg/mL, there was an immediate improvement in psychiatric and neurological symptoms.
This case highlights the need to recognise the psychiatric and neurological manifestations of N2O abuse. These symptoms can be varied and also severe. Prompt investigation and management for Vitamin B12 deficiency is required. Replacement of deficient Vitamin B12 is recommended for complications associated with N2O abuse (Sethi et al., 2006).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.