
Abstract

In the fight against the two-headed dragon that surfaced from musings of the mind, the one champion that has reigned supreme for more than half a century is lithium. Surviving precariously from one decade to the next, this humble, silvery white element continues to demonstrate its silverback status amongst the burgeoning pharmacological armamentarium that is presently used to ‘treat’ bipolar disorder. Numerous combatants belonging to the armies of antidepressants and anticonvulsants, flanked by their armigers brandishing pharmaceutical coats of arms, have successively thrown down the gauntlet to lithium, resulting in interregna marked by its displacement from prescription use. However, on each occasion the shining knight, true to its mettle, has risen to the challenge and managed to reclaim its succession to the throne.
Alas, once again, uncertainty looms as another army of medicaments descends upon the realm of mood stability. Whether lithium will retain its crown or whether for once, the outcome is ‘atypical’, only time will tell ...
1
The story of an old element
The story of lithium has been told and retold many times. But perhaps the most impressive account of its history, especially in recent years, is that by Schioldann (2009), who manages to provide a comprehensive and detailed account, melding both narrative and fact into an enjoyable and readable text. Similarly, the science of lithium therapy and its translation into practice has been captured in a book published earlier this year (Malhi et al., 2017). Both of these texts have been made possible because of the sustained interest in lithium for over half a century – reflected by its enduring primacy both in practice and in clinical guidelines for the treatment of mood disorders, all of which is simply a consequence of its lasting efficacy. Time and again lithium has proven its worth and managed to remain a ‘signature dish’ among the menu of medications made available to treat bipolar disorder and depression. Remarkably, it has achieved this despite repeated efforts by competitors to displace it from pole position. After being discovered and rediscovered by the Lange brothers and Cade, respectively, lithium was popularised clinically by the efforts of many others.
John Cade
The role of John Cade in realising the potential of lithium has been lauded and described as ‘pivotal’, ‘visionary’ and ‘astounding’. But at the same time, others have expressed disbelief and described his discovery as ‘serendipitous’, and perhaps even ‘inevitable’, given that the basic properties of lithium were already known and Cade’s observations were somewhat derivative and therefore not a novel breakthrough per se. However, in my view, his role was fundamental because it was his seminal paper that ignited meaningful interest in lithium in the 20th century, and it is this fire that continues today. Whether he was the first to discover the mood-stabilising properties of lithium is a moot point and maybe a reasonable way forward is to recognise the role of all concerned; Cade can be regarded as the ‘father of lithium’ and the Lange brothers, perhaps the ‘grandfathers of lithium’.
Once the possibility of lithium having a role in the treatment of psychiatric disorders was realised, the next step was to determine which patients it benefitted most, and how it could be delivered effectively and safely. This required the efforts of many including, for example, Trautner, Schou and Gershon to name but a few.
Australian and New Zealand Journal of Psychiatry: setting its sights on lithium
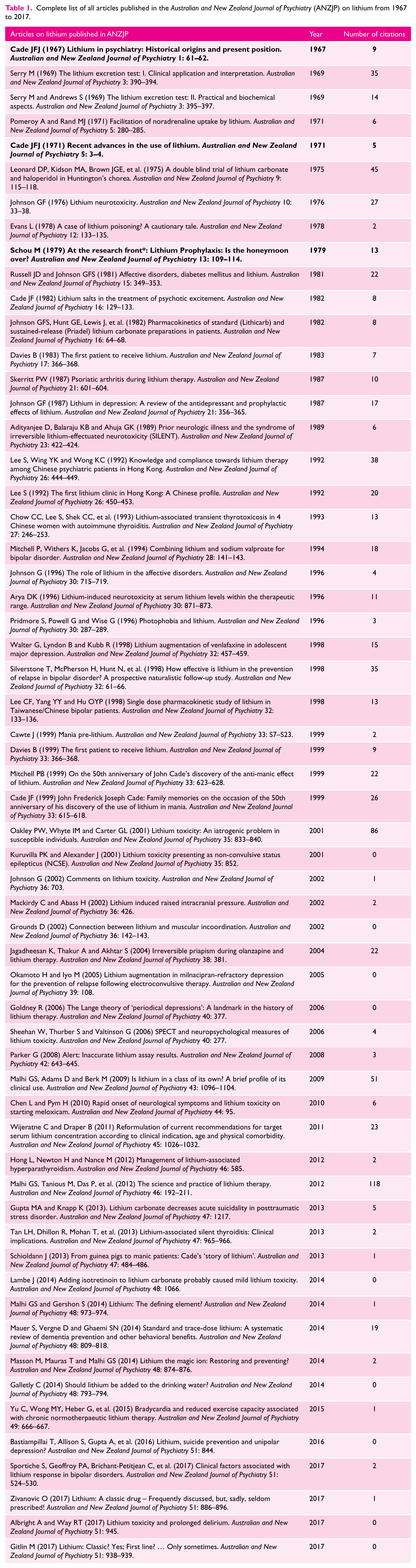
In its own way, the Australian and New Zealand Journal of Psychiatry (ANZJP) has also made a contribution to the ‘lithium story’. Remarkably, in its very first volume in 1967, there is a paper published by John Cade and then another a few years later that together outline lithium’s historical origin and role at the time, and provide an update on advances on its use in clinical practice and the science that underpins this. Cade’s publications in the journal reflect the important role he played not only in the history of lithium as a medication but also in the development of psychiatry in Australia and New Zealand (see Table 1). Since then, many other important contributions have appeared in the pages of ANZJP, notable among these is the 1979 paper by Schou who was asking almost four decades ago whether lithium’s honeymoon was over? Evidently not, as shown by the trend within ANZJP with the number of publications on lithium in the journal increasing over the years rather than diminishing (see Figure 1).
Complete list of all articles published in the Australian and New Zealand Journal of Psychiatry (ANZJP) on lithium from 1967 to 2017.

Total number of articles about lithium published in the Australian and New Zealand Journal of Psychiatry (ANZJP) per year from 1967 to 2017.
Over the past five decades, citations to lithium articles in the ANZJP have almost always been greater than the average (compared to other articles in the journal and the impact factor of the journal when this became available) with only correspondence occasionally failing to attract any citations at all (see Table 1 and Figure 2). And in the last 25 years, ANZJP citations to lithium articles have exceeded 50 in half a dozen of those years; a few articles have even managed to attract more than 50 cites individually. I like to think this is because lithium is an Australian element – at least with respect to its use as a mood stabiliser.

Total number of citations generated from articles about lithium published in the Australian and New Zealand Journal of Psychiatry (ANZJP) per year from 1967 to 2017.
Beyond ANZJP
Trends in the ANZJP reflect worldwide interest in lithium – in particular a resurgence of enthusiasm for its medicinal properties. The use of lithium in bipolar disorder, or at least advocacy for its use, has increased globally in recent years; partly because of key studies that have re-established its clinical benefit (BALANCE Investigators and Collaborators et al., 2010) and studies that have put into context the previously exaggerated risks associated with lithium use (McKnight et al., 2012). As a consequence, lithium is recommended as first line for the treatment of bipolar disorder in virtually all clinical practice guidelines, at least for mania and maintenance therapy, and is recognised as an effective augmentation strategy in the management of major depressive disorder when faced with partial response to an antidepressant (Malhi et al., 2015). In day-to-day practice, the side effects of lithium are often the first thing to be discussed when the prescription of lithium is considered. Its acute side effects can be troublesome but usually pass, and more problematic and serious side effects (e.g. thyroid and renal dysfunction) only emerge after years of therapy, but these too can be successfully limited with careful monitoring. Monitoring the levels of lithium is integral to therapy, but is often regarded an encumbrance. However, once steady state is achieved, monitoring does not need to be frequent, and in fact regular blood sampling should be regarded as an advantage because it ensures compliance and allows fine titration of the medication to clinical response.
Clinically, the continued use and popularity of lithium is not surprising to those familiar with its effects in practice, although, it has to be noted that despite this resurgence of interest, its overall use has not discernibly increased in comparison to alternatives. This suggests that concerns about its use and/or perhaps simply a lack of familiarity with its potential side effects still limits its wholesale uptake – alongside the fact that it lacks significant promotion by Big Pharma. Perhaps lithium is destined to remain an option among mood disorder medications and any further increase in its use is only likely to stem from its additional properties.
Additional lithium properties
The renewed interest in lithium has drawn attention to its additional properties, which are of at least equal importance as its mood stabilisation effects, and certainly have potential to be hugely impactful. First, lithium is anti-suicidal, that is to say it reduces the likelihood of suicide. This has been known for some time but only demonstrated more convincingly in recent years. It has been shown to be an effect that is separate to its effect on mood. Clarification and identification of this action has huge clinical potential, as it would mean lithium can be utilised beyond mood disorders to specifically address suicidality. It may also assist with ameliorating precursors to suicide, such as irritability and impulsivity. Second, lithium appears to be neuroprotective. It is unclear, however, whether lithium achieves this by staving off insults to the brain, or whether it facilitates and accelerates intrinsic neuroprotective and regenerative processes within brain tissues. Either way, this property, if borne out to be true, once again has enormous potential in assisting, for example, with the treatment and prevention of cognitive disorders and neurodegenerative illnesses.
Conclusion
Lithium is an extremely important medication not only because of its key role in the management of mood disorders and its promising additional properties, but because it has unequivocally shown that psychiatric disorders have a biological element. Research attempting to further understand its mysteries and refine its clinical application will no doubt continue to be a feature of ANZJP, which has long been home to its champions.
Footnotes
Acknowledgements
Many thanks to Grace Morris and Amber Hamilton for their assistance with the figures and table.
Declaration of Conflicting Interests
Gin S Malhi has received grant or research support from Australian Rotary Health, the NHMRC (APP1073041), and the American Foundation for Suicide Prevention (PRG-0-09014; SRG-0-089-16).
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.