
Abstract
Targeting Zero is a report commissioned by the Department of Health and Human Services (DHHS) published in October 2016. It was commissioned as a result of a cluster of perinatal deaths at Djerriwarrh Health Service during 2013 and 2014 (Targeting Zero, ©State of Victoria, October 2016, ISBN: 978-0-7311-6966-5; www2.health.vic.gov.au/hospitals-and-health-services/quality-safety-service/hospital-safety-and-quality-review). Targeting Zero concluded that clinical governance around monitoring and responding to adverse clinical outcomes in a timely manner was inadequate and that DHHS lacked processes that were capable of detecting significant deficiencies in clinical governance, particularly regarding safety and quality. It found that across health services, avoidable patient harm continues to occur and variability of care is prevalent at an unacceptable level. Avoidable patient harm was defined as harm that patients suffer, not through their illness or a lack of knowledge about treatment, but because of ineffective systems to help keep them safe while receiving care. Variability of care indicates that valuable knowledge is not being shared and implemented widely, so that many patients are receiving care that diverges from best practice.
High-level recommendations around mental health care included the need to ensure adequate mental health funding and that there is public discussion regarding indicators pertaining to safety, quality and pressure on Mental Health Services (MHS) in order to prevent avoidable harm and reduce variation in practice.
This debate article takes a balcony view of safety and quality within mental health to consider in more detail the issues of avoidable harm, variability of care leading to divergence from best practice and hopes to facilitate a public discussion among psychiatrists regarding what are important indicators of safety, quality and pressure within MHS.
Safety and quality within MHS
Avoidable harm
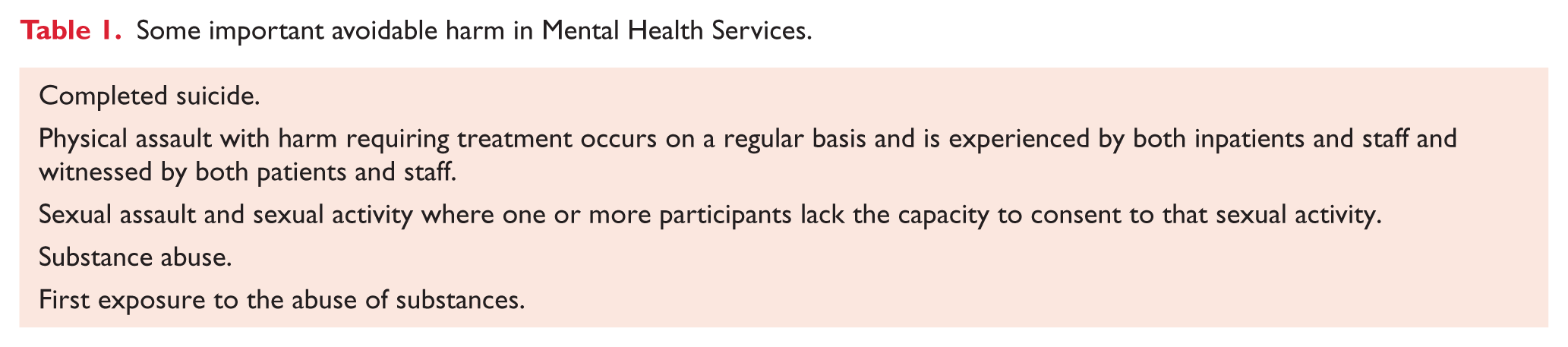
Within specialist MHS, some types of avoidable harm that regularly occur within inpatient services are shown in Table 1.
Some important avoidable harm in Mental Health Services.
Rates of seclusion for some services are presented in Table 2 and are publicly available and documented within the Office of the Chief Psychiatrist’s Annual Report (2015–2016, Victorian Government, 1 Treasury Place, Melbourne, ©State of Victoria, Department of Health and Human Services, November 2016, ISSN: 2207-xxxx; www2.health.vic.gov.au/about/key-staff/chief-psychiatrist/annual-reports). The reports of the Mental Health Complaints Commission (Annual Report 2015–2016, www.mhcc.vic.gov.au/downloads/2015-16%20Annual%20Report.pdf) and the Community Visitors Annual Report on Public MHS (2015–2016, ©2016, Office of the Public Advocate, ISSN 1836-3296; www.publicadvocate.vic.gov.au/our-services/publications-forms/368-community-visitors-annual-report-2015-2016?path) demonstrate the concerns that our consumers have for their safety in psychiatric settings. Firm data regarding frequency of occurrence are not readily available for many adverse outcomes. An online survey published in 2013 of Victorian women admitted to psychiatric wards found 45% reported being victims of sexual assault during their admission (Mental Health Services Annual Report 2015–2016, Victorian Government, ©State of Victoria, Department of Health and Human Services October 2016, ISSN 2206-5970; www2.health.vic.gov.au/Api/downloadmedia/%7B7DB669B0-9714-4CA0-A5D8-5B8E17849E3C%7D). Kulkarni (Zero Tolerance for Sexual Assault, 2013 Victorian Mental Illness Awareness Council; www.abc.net.au/reslib/201305/r1115028_13591277.pdf) suggests that 5–11% of women in psychiatric inpatient units experience significant sexual harassment and/or assault. A 2015 meta-analysis of suicide among psychiatric inpatients found variability in reported rates and estimated across 39 studies that there is one inpatient death per 676 admissions (Walsh et al., 2015). This supports the authors’ observations that there is one inpatient suicide every 1–2 years in an average adult ward of 20–25 beds. Seclusions occur at variable rates across MHS (Table 2), and substance abuse is a major cause of comorbidity and relapse (www2.health.vic.gov.au/Api/downloadmedia/%7BF41E9FFA-57ED-4400-B764-78C2878C18E0%7D) (Kulkarni, 2012).
Variablilty in practice (de-identified extract from DHHS adult mental health quarterly KPI report 2016–2017 Q1).
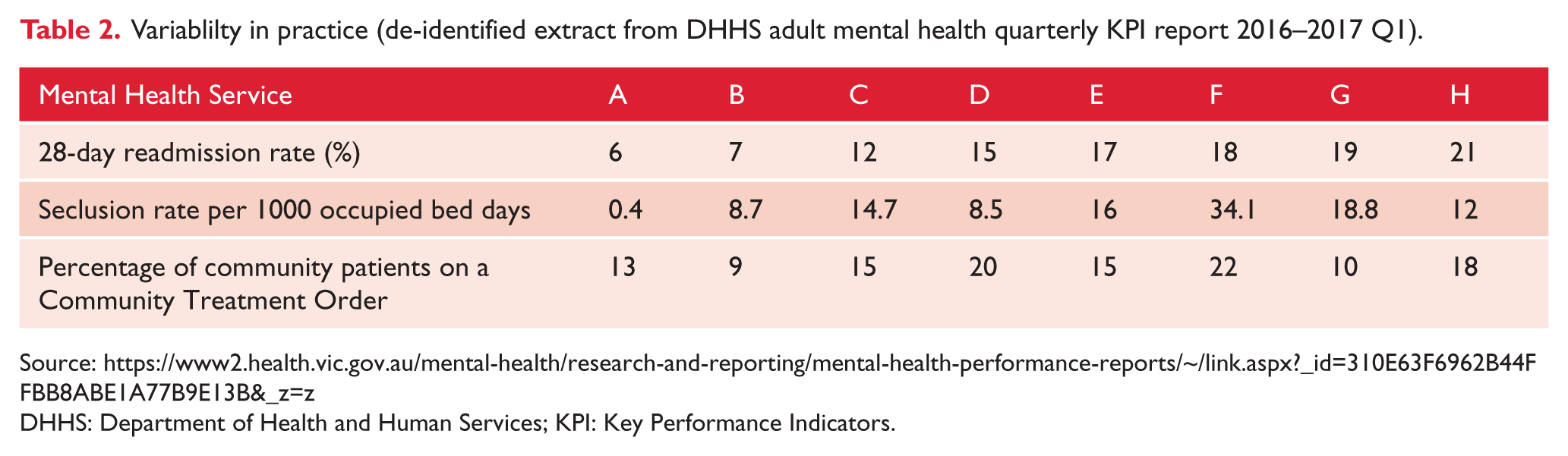
DHHS: Department of Health and Human Services; KPI: Key Performance Indicators.
It is frequently argued that psychiatrists do not have the ability to predict accurately imminent suicide risk or risk of aggression and that we do not have the right to restrict people’s wish to use substances or make relationships that may expose them to a degree of risk. Yet, inpatient MHS look after people at a time of immense vulnerability, usually in emotional turmoil and at risk to themselves or others (Morgan and Large, 2013).
Psychiatrists do not have the ability to read people’s minds, nor control their wants, desires or impulses. Our philosophy of care includes least restrictive environments that empower people to make decisions for themselves and encapsulate a ‘dignity of risk taking’ (A national framework for recovery-oriented MHS, Commonwealth of Australia 2013, ISBN 978-1-74186-011-5; www.health.gov.au/internet/main/publishing.nsf/content/67D17065514CF8E8CA257C1D00017A90/$File/recovgde.pdf). Some Mental Health Acts (including the Victorian one) specifically state that a key role of the psychiatrist is to support people in making decisions relating to the treatment and care that reflect that person’s preferences and wishes, rather than necessarily what the psychiatrist considers to be in the best interest of patients (Mental Health Act 2014, State of Victoria 2014, ISBN 1-74368-069-8; www.health.gov.au/internet/main/publishing.nsf/content/67D17065514CF8E8CA257C1D00017A90/$File/recovgde.pdf).
Should psychiatrists therefore accept that serious harm is unavoidable within mental health?
We believe that it is our responsibility to advocate in the strongest possible way for systems to be resourced and put in place that will reduce and ultimately prevent avoidable harm. No person should be raped while an inpatient in a psychiatric ward; no person should be assaulted on a ward; and no person should die by their own hand while under 24-hour care in a hospital. We will never achieve these outcomes unless we set them as specific goals and work to achieve them. It is imperative that funding is available to support these goals.
Variability of care
Table 2 shows the wide variability in treatment approach across three domains of Key Performance Indicators (KPIs) that are routinely collected by MHS. The services represented are all from the greater Melbourne urban conurbation. Seclusion rates vary across services from 0.4 to 24.1 seclusions per 1000 occupied bed days. Readmissions within 28 days of discharge vary from 6% to 21%. Involuntary treatment rates for community patients vary from 9% to 22%. Some of this variability may be accounted for by the different demographics across that modify rates and complexity of psychiatric presentations. However, this demographic variability does not account for the majority of the variance in these simple but clinically meaningful measures. We speculate that much of the practice variation for these measures is likely to be accounted for by differing approaches to supporting recovery-oriented practices, clinical engagement and risk management practices reflecting long standing cultures in different services that are amenable to change.
There is a firmly held belief that individualised treatment and person centred care must be the cornerstone of psychiatric care. This might be so, but the treatment we offer needs consistently to reflect the best available evidence. If each individual has a disorder that is unique to them and that will respond only to a treatment approach that is unique to them, then our experience and medical knowledge can offer them little assistance. The recovery movement is a consumer-led force that clearly articulates the expectation that people with psychiatric illness are supported in achieving their own goals while receiving the optimal treatment from psychiatric services within a framework that maximises choice, autonomy, and hope. We argue that MHS provision must move away from defending variability in treatment, to consistently aiming to provide for each person seeking care a package of approaches that adhere to clearly articulated best practice treatments. Not only are there social justice and equality access elements to the best evidence-based treatment, there is also an economic argument as patients move from incapacity and dependency to independence and a prospect of re-joining the workforce.
RANZCP guidelines are helpful at collating much of the evidence and identifying elements of good care, but have not set a clear standard of care content that we can be held accountable to (Royal Australian and New Zealand College of Psychiatrists [RANZCP CPG], 2016). Catts has recently published an article that takes the RANZCP Clinical Practice Guideline for Schizophrenia and adds effectiveness evidence and develops a robust treatment pathway for early schizophrenia that should be a call to arms for all service providers in public and private mental health (Catts and O’Toole, 2016). Our clear impression over a long teaching experience is that knowledge and clinical standards in psychopharmacology are variable and the key elements of psychological interventions are still fiercely debated within our sector despite enormous advances in the evidence base. Professional education will be critical to trying to improve treatment standards to the level of best available evidence.
This paper uses the release of Targeting Zero, a report into safety and quality processes in Victorian Health Services as an opportunity to reflect on key safety and quality issues within mental health. What harm should we never accept as inevitable in mental health? Should psychiatrists accept the large variation in practice that currently exists between services and between individual clinicians? We have demonstrated that very significant avoidable harm occurs within psychiatric services that we should not tolerate. This includes serious physical and sexual assault, substance abuse, and inpatient suicide. Variation in practice across MHS occurs in areas that have significant impact on basic clinical outcomes and the variation is so wide as to be unacceptable.
If we are to reduce the gap in psychiatric morbidity and mortality and support people in leading a life worth living and filled with hope and power within the community, then psychiatrists have a responsibility to provide them with the best treatment possible and be strong, clear, and consistent advocates for the resources to provide the treatment and services they need.
There must be clear policy and funding initiatives in mental health to redress these avoidable deficiencies in our MHS that support best practice service provision through training, workforce reform, rebuilding of the care environments, staffing levels, and appropriate health information structures.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.