
Abstract

To the Editor
Early and accurate diagnosis of dementia aetiology might improve clinical outcomes because the progression of clinical symptoms and optimal drug management approaches often differ between dementia subtypes (Mendez et al., 2007; Ong et al., 2015). However, access to adjunct diagnostic tools like brain magnetic resonance imaging (MRI) and fluorodeoxyglucose positron emission tomography (FDG PET), that can improve diagnostic accuracy (Weiner et al., 2015), varies widely across healthcare settings in Australia. Notwithstanding, practice data from tertiary memory clinics that extensively use such tools might provide best practice evidence for clinicians working in settings with limited access to these tools.
A randomly selected sample of 54 elderly patients (mean age = 73.5 years, standard deviation [SD] = 12.5; mean Mini-Mental State Examination score = 21.9, SD = 4.8) presenting to the Austin cognitive dementia and memory service in Melbourne, Australia, with cognitive concerns were retrospectively studied. All patients underwent a comprehensive cognitive work-up that often included a brain MRI (n = 38), a brain FDG PET (n = 32) and an extensive neuropsychology assessment (n = 39). Their informants were also interviewed privately in a separate room. Clinical diagnoses and management plans were made by consensus during a post work-up case conference attended by geriatricians, psychogeriatricians, neurologists, neuropsychologists, nurses trained in dementia care and other allied health staff. We compared the predictive utilities of memory-related symptoms (MRS) for both clinically probable Alzheimer’s disease (AD) and the results of neuroimaging.
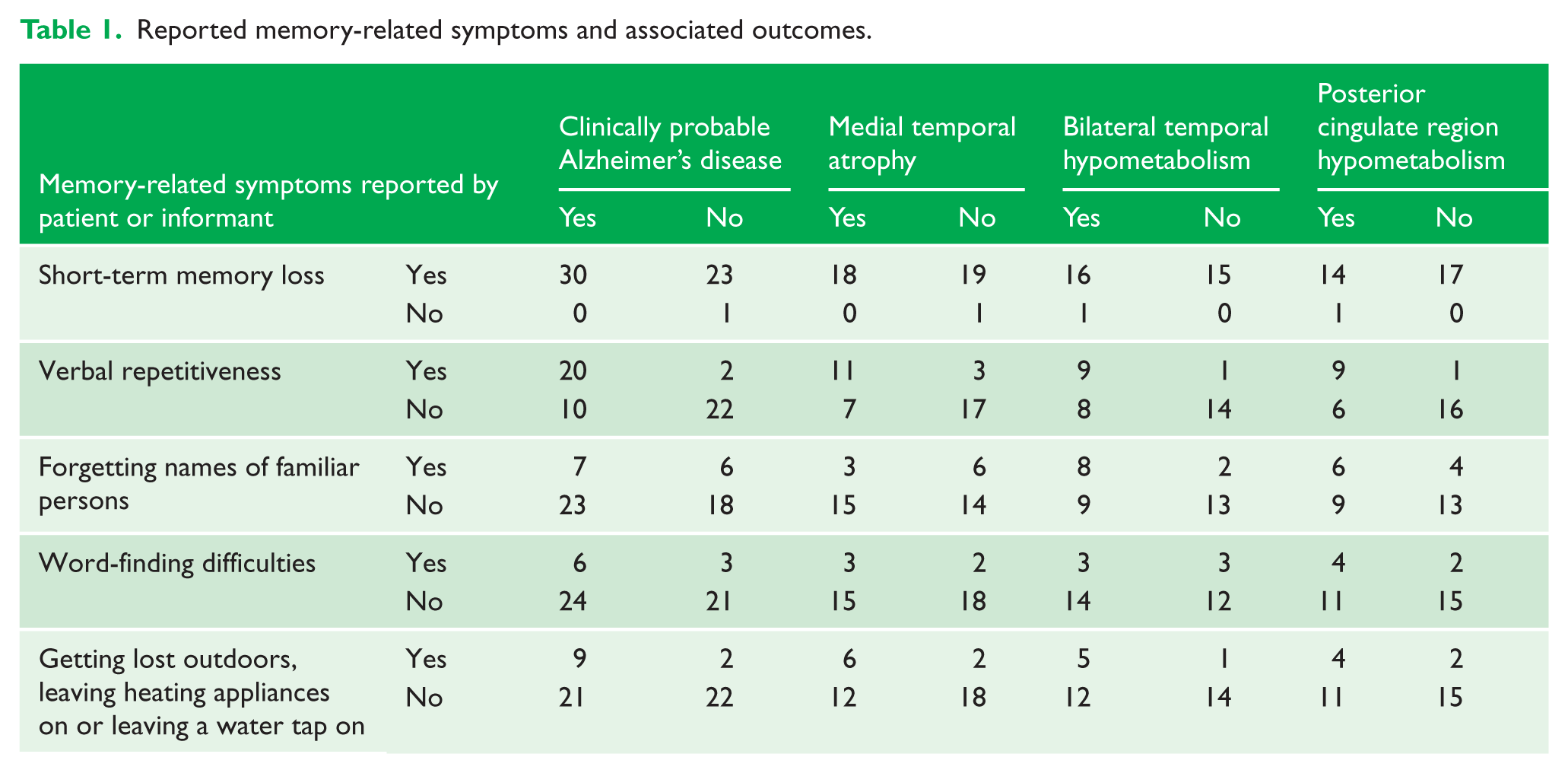
Thirty patients were diagnosed with AD. Seven most frequently documented MRS in these patients’ records were short-term memory loss, verbal repetitiveness, word-finding difficulties, forgetting names of familiar persons, getting lost outdoors, leaving heating appliances on and leaving a water tap on. Only the verbal repetitiveness MRS was specific for and predicted AD (sensitivity, 67%; specificity, 92%; positive predictive value [PPV], 91%; negative predictive value [NPV], 69%; p < 0.0001), hippocampal atrophy on MRI (sensitivity, 61%; specificity, 85%; PPV, 79%; NPV, 71%; p < 0.01), and hypometabolism in the bilateral temporal lobes (sensitivity, 53%; specificity, 93%; PPV, 90%; NPV, 64%; p < 0.01) and posterior cingulate region (sensitivity, 60%; specificity, 94%; PPV, 90%; NPV, 73%; p < 0.01) on FDG PET (Table 1). None of the other MRS had predictive utility for AD.
Reported memory-related symptoms and associated outcomes.
These initial findings might increase confidence during memory clinic assessments that the predominant neuropathology causing an elderly patient with cognitive concerns to present to a memory clinic, who does not also report verbal repetitiveness, might be of non-AD aetiology. Also, verbal repetitiveness may indicate dysfunction in AD signature cerebral regions. Further studies should be conducted to validate these findings which have health economic implications in managing dementia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
This study has been approved by the Austin Health Human Research Ethics Committee.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.