
Abstract
Objective:
Few studies have examined the contribution of specific disaster-related experiences to symptoms of depression. The aims of this study were to do this by examining the roles of peri-traumatic stress and distress due to lingering disaster-related disruption in explaining linkages between disaster exposure and major depressive disorder symptoms among a cohort exposed to the 2010–2011 Canterbury (New Zealand) earthquakes.
Methods:
Structural equation models were fitted to data obtained from the Christchurch Health and Development Study at age 35 (n = 495), 20–24 months following the onset of the disaster. Measures included earthquake exposure, peri-traumatic stress, disruption distress and symptoms of major depressive disorder.
Results:
The associations between earthquake exposure and major depression were explained largely by the experience of peri-traumatic stress during the earthquakes (β = 0.180, p < 0.01) and not by disruption distress following the earthquakes (β = 0.048, p = 0.47).
Conclusion:
The results suggest that peri-traumatic stress has been under-recognised as a predictor of major depressive disorder.
Natural disasters have devastating impacts on affected populations because of both the acute, often frightening and life-threatening experiences, and the consequent negative life events that may follow. Although there has been emphasis on disasters causing post-traumatic stress disorder (PTSD) (Andrews et al., 2007; Brewin et al., 2000; Galea et al., 2005; Neria et al., 2008; Utzon-Frank et al., 2014), there has been increasing recent interest in the relationship between disasters and major depression (MD) (Bonde et al., 2016; Salguero et al., 2011; Tang et al., 2014). Indeed, these studies conclude that depression (not only PTSD) should be considered to be a consequence of traumatic exposure (Bonde et al., 2016).
There is, of course, a well-established literature linking life events to mental health problems including depression (Hammen, 2005; Kessler, 1997; Wittchen et al., 1994). In addition, there has been increasing recognition that a disaster is often the start of a complex series of events including not only the acute exposure but also stressful life events that may follow, including death or injury of family and friends, loss of housing, loss of employment/earning and widespread damage to the living environment (Forbes et al., 2015; Lock et al., 2012).
Recent systematic reviews and meta-analyses (Bonde et al., 2016; Salguero et al., 2011; Tang et al., 2014) consistently report an increased prevalence of MD after exposure to a disaster with an average odds ratio of 1.41 (95% confidence interval [CI]: 1.06, 1.87) from the relatively few high-quality studies that have been reported (Bonde et al., 2016). Characteristics that have been found to increase the risk of MD after a disaster include pre-event factors (female gender, a previous or family history of depression, having experienced traumatic events or more stressful situations before the disaster) (Galea et al., 2007), peri-event factors that impact during or immediately after the disaster (experience of fear for life [Bryant et al., 2014; Miguel-Tobal et al., 2006] or a panic attack at the time of the event, injury or bereavement) (Galea et al., 2002; Salguero et al., 2011; Tang et al., 2014) and post-event factors (the occurrence of more stressful events, loss of financial resources, little social support [Armenian et al., 2002; Kaniasty and Norris, 1993; Person et al., 2006], or loss of property/house damage [Tang et al., 2014]).
There is debate about the mechanisms linking MD to a disaster. Some studies but not all (Shalev et al., 1998) suggest that the risk of MD after a disaster may be related to personal loss (bereavement and psychosocial loss) rather than the experience of severe acute psychological trauma which may be more closely involved with the development of PTSD (Bonde et al., 2016; Salguero et al., 2011). Studies have also reported that MD is not always concurrent with PTSD (Bleich et al., 1997; Shalev et al., 1998), suggesting that MD is a different but related post-traumatic reaction to a potentially traumatic event.
We have previously reported that the associations between disaster exposure (an earthquake) and PTSD were explained not just by the experience of peri-traumatic stress during the earthquakes but also by disruption distress following the earthquakes (Boden et al., 2015). In this paper, we use a similar methodology to examine the relative contributions of peri-traumatic stress and post-disaster disruption distress on the development of MD symptoms in a birth cohort, the Christchurch Health and Development Study (CHDS). Beginning in September 2010, the city of Christchurch, New Zealand, and the surrounding Canterbury region were struck by a series of over 10,000 earthquakes and aftershocks, with four major earthquakes causing widespread damage to the city, and one (22 February 2011) resulting in 185 deaths. Christchurch is home to the long-running CHDS, a birth cohort of 1265 children born in 1977. Of this cohort, more than 50% were exposed to the Canterbury earthquakes, and at age 35, those exposed were interviewed about their experiences of these earthquakes. The purpose of the present investigation was to examine the linkages between earthquake exposure and MD symptoms, comparing the roles played by (a) peri-traumatic stress as a result of the earthquakes and (b) disruption distress in the aftermath of the earthquakes.
The aims of this analysis were to fit a structural equation model estimating the relative contribution of peri-traumatic stress and disruption distress in explaining MD following exposure to the Canterbury Earthquakes, net of a series of covariate factors (including a measure of relative exposure to the earthquakes). Details of model fitting and model specifications are provided in the ‘Method’ section. Using structural equation modelling (SEM), it proves possible to estimate the direct and indirect pathways in the model and to compare the fractions of the correlation between earthquake exposure and MD symptoms that are explained by each pathway in this model.
Method
Participants
The data were collected at the age 35 assessment of the CHDS, a longitudinal study of a cohort of 1265 children born in the Christchurch (New Zealand) urban region over a 4-month period from April to August 1977. The cohort comprised 98% of all children born in the Christchurch region during this period. This cohort has now been studied from birth to age 35 years (Fergusson and Horwood, 2001). All aspects of data collection have received ethical approval by the Canterbury Regional Health and Disability Ethics Committee, and all data were collected with the explicit consent of study participants.
Data collection
In 2012, members of the CHDS cohort were approached to respond to the age 35 assessment for the study. This process identified 962 cohort members available for contact, who represented 79% of the surviving cohort. Of these, 505 were resident in Canterbury during the earthquakes. These cohort members were invited to participate in a further interview concerning their exposure to the Canterbury earthquakes. Of those eligible, 495 respondents completed an interview of approximately 1 hour that assessed their earthquake experiences and reactions to the earthquakes. These interviews took place approximately 20–24 months following the start of the Canterbury earthquakes in September 2010. By the time the interviews began, cohort members could have been exposed to four major earthquakes ranging in Richter scale magnitude from 7.1 to 6.0. These earthquakes occurred on 4 September 2010, 22 February 2011, 13 June 2011 and 23 December 2011. Interviews took place during the period May–October 2012.
Symptoms of MD, age 34–35
At age 35, participants were assessed on a comprehensive mental health interview that examined aspects of psychosocial adjustment since the previous assessment. As part of interview, depression symptomatology was assessed using the Diagnostic Interview Schedule (DIS) (Robins et al., 1995). Participants were asked a series of questions concerning their experience of symptoms of depression during the 12 months prior to the assessment at age 35. Each item was answered using a 3-point scale for each symptom with the following answer options: 1 = ‘doesn’t apply’, 2 = ‘applies somewhat’ and 3 = ‘definitely applies’ (those answering ‘3’ were coded as having the symptom). This information was used to create a measure of the number of Diagnostic and Statistical Manual of Mental Disorders–Fourth Edition (DSM-IV) symptoms of MD reported by the participant during the 12 months prior to the assessment at age 35. The mean score for the number of MD symptoms in the sample was 1.31 (standard deviation [SD] = 2.85). The symptom score measure was found to have excellent reliability (α = 0.98).
For the purposes of conducting supplementary analyses, data on current MD symptoms, obtained in the same manner as described above, were used to create a measure of current (past month) MD symptoms. The mean score for the number of current MD symptoms in the sample was 0.52 (SD = 1.94). The current symptom score measure was found to have excellent reliability (α = 0.97).
Peri-traumatic stress
Peri-traumatic stress was assessed via the Peri-traumatic Distress Inventory (PDI) (Brunet et al., 2001), which was supplemented by three custom-written survey items relating to fear/panic and dissociative symptomatology. The PDI is a 13-item scale designed to assess the distress experienced during and immediately after exposure to a critical event such as a natural disaster. Questions were asked using a 5-point Likert scale response format ranging from 1 = ‘not at all’ to 5 = ‘a great deal’, regarding peri-traumatic stress experienced during any of the four Canterbury Earthquakes of magnitude 6.0 or greater. The scale included such items as ‘felt afraid for your own safety’, ‘felt horrified by what you saw’ and ‘thought you might die’. A scale score was derived for each participant by summing the 13 items and the three additional items and dividing by the number of items. The scale was found to have good reliability (α = 0.89). The mean score for the present sample was 2.02 (SD = 0.71; range: 1–4.5).
Disruption distress
Participants were also asked a series of 12 questions regarding the extent to which the earthquakes had caused distress related to disruption of their living situation, activities and daily routines. These questions assessed the level of distress caused by having to move house or leave the area, disruption of family life and children’s schooling and uncertainty about the future, disruption of services (power, water, sewerage), disruption to employment, loss of community, family and friends moving house or leaving the area, uncertainty about the continuing aftershocks and difficulties in getting answers about property status or repair/rebuilding of the family home (Fergusson et al., 2014, 2015).
In all cases, items were scored on a 5-point scale ranging from 1 = ‘not at all’ to 5 = ‘a great deal’. For the purposes of the present investigation, the 12 items described above were used to create a summary measure of distress by summing the scores for each item dividing by the number of items to produce an overall mean score. The scale was found to have good reliability (α = 0.83). The mean score for the present sample was 1.90 (SD = 0.75; range 1–4.42).
Covariate factors for SEM
For the purposes of the present investigation, a series of covariate factors were chosen from the study database, on the basis of a prior investigation of mental health outcomes following exposure to the Canterbury Earthquakes. These factors were as follows.
Gender
Measured at birth.
Cognitive ability (IQ; ages 8–9 years)
Cohort members’ IQ was assessed at age 8–9 years using the Revised Wechsler Intelligence Scale for Children (Wechsler, 1974). The full scale score was used for the purposes of the present analyses.
New Zealand Māori ethnicity (age 21)
At age 21, respondents were asked about their ancestry, ethnic identification, level of participation in Māori cultural domains and proficiency in the Māori language (Broughton et al., 2000). On the basis of this questioning, 11.1% of sample members self-identified as New Zealand Māori.
Prior history of mental disorder (age 25–30 years)
At age 30, participants were assessed on a comprehensive mental health interview that examined aspects of psychosocial adjustment since the previous assessment. This interview was similar to that used at age 35 and enabled classification of participants on a range of mental disorder outcomes for each of the interval 25–30 years. This information was combined over the four assessment periods to provide two measures. The first measure was a count of the number of mental disorders for which the individual met DSM-IV (American Psychiatric Association, 1994) criteria during the period 25–30 years, including MD; anxiety disorders; nicotine, alcohol and illicit drug dependence; and suicidal ideation/attempt over the period from age 25 to 30 years. The second measure was a dichotomous classification as to whether the individual met criteria for PTSD during the period 25–30 years.
Family socioeconomic status (age 30)
The socioeconomic status of each cohort member’s family was assessed at age 30 using the New Zealand Socioeconomic Index–2006 (NZSEI-2006) (Elley and Irving, 1976). The NZSEI classifies individuals and families on a scale ranging from 10 (lowest) to 90 (highest) based on occupational status. For the purposes of the present investigation, the family NZSEI score was the higher of the scores for the cohort member or the cohort member’s partner (where applicable).
Extent of earthquake exposure (age 35)
For each of the four major earthquakes, participants were asked a series of questions relating to the severity and immediate impact of the earthquakes. Items were based on the Modified Mercalli Earthquake Intensity Scale (Dowrick, 1996) and designed to examine the consequences of the earthquakes for property, buildings, land and infrastructure. Using this information, a series of 11 indices were constructed to reflect the severity of the four major earthquakes. These indices were scaled on a 3-point scale ranging from 0 = no/minor impact, 1 = mild/moderate impact to 2 = severe/major impact. Individuals not exposed to a specific earthquake were coded as zero on all indices for that earthquake. To reduce the dimensionality of the data, for each index, scores were summed across the four earthquakes to produce a total score. These scores were then used in a confirmatory factor model to test for unidimensionality (Fergusson et al., 2014). This analysis showed that, with some allowance for correlated item specificity, the scale items fitted a single factor model representing the severity of the individual’s earthquake exposure (details of the development of this measure are available in Fergusson et al., 2014). The scale was found to have good reliability (α = 0.92). The mean score for the present sample was 32.91 (SD = 14.66; range: 0–84.0).
Statistical analyses
The associations between the measures of (a) MD symptoms, (b) peri-traumatic stress and (c) disruption distress were modelled via latent variable SEM. The fitted model is shown in Figure 1. This model assumes (a) peri-traumatic stress and disruption distress were correlated factors and (b) MD symptoms were influenced by peri-traumatic stress and disruption distress.
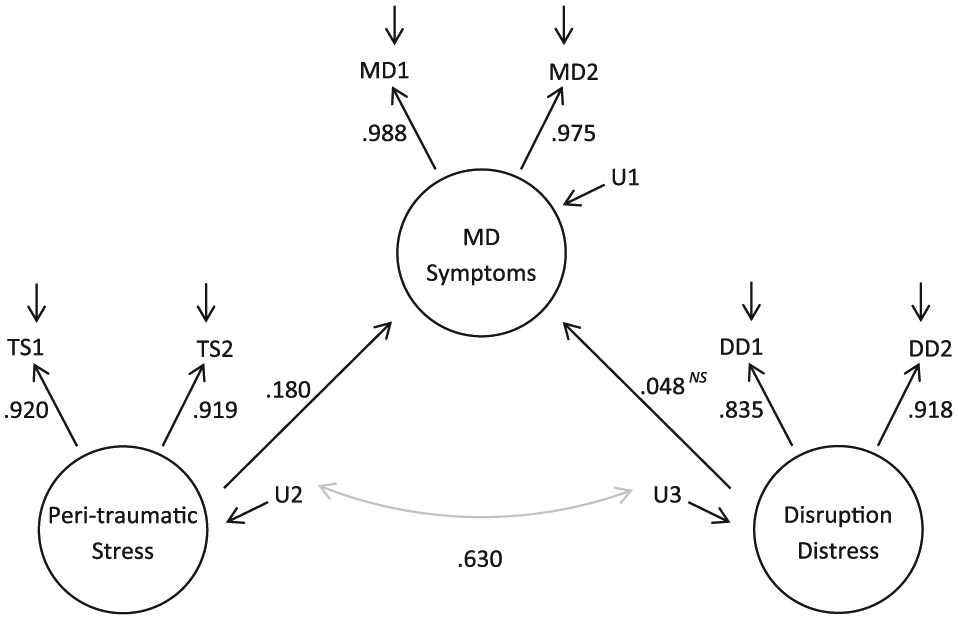
Fitted structural equation model of the latent measures of MD symptoms, peri-traumatic stress and disruption distress, with standardised coefficients.
In Figure 1, MD1, MD2, TS1, TS2 and DD1, DD2 are assumed to be a set of observed indicators of underlying latent constructs representing the severity of MD, peri-traumatic stress and disruption distress, respectively. For the purposes of the present analysis, the observed indicators MD1, MD2, TS1, TS2 and DD1, DD2, were constructed using split-half score measures of MD symptoms, peri-traumatic stress and disruption distress scores during the period following the earthquakes. These indicators are assumed to be linked to the underlying latent constructs via a so-called ‘true score’ model (Alwin and Jackson, 1980) in which the variance in the observed indicators can be partitioned into true score variance reflecting (a) the individual’s underlying level of MD, peri-traumatic stress and disruption distress; and (b) random error due to unreliability in the observed indicators. The use of split-half indicators reduces the influence of measurement error, as compared with SEM with observed measures (Alwin and Jackson, 1980). It should be noted, also, that the model in Figure 1 omits the earthquake exposure portion of a model used in a previous analysis of this cohort (Boden et al., 2015). The reason for this is that the earthquake exposure portion of the present model is identical to the earlier published model.
The model in Figure 1 was fitted to the variance–covariance matrix of the split-half indicators of the latent variables of MD symptoms, peri-traumatic stress and disruption distress, using Mplus (Muthen and Muthen, 2007) and methods of maximum likelihood estimation that were robust to non-normality. Model goodness of fit was assessed on the basis of the model chi-square, the root mean square error of approximation (RMSEA) and the comparative fit index (CFI). In well-fitting models, the RMSEA should be less than 0.05 and the CFI close to 1 (Muthen and Muthen, 2007).
In order to examine whether the final fitted model was robust to the potential influence of covariate factors, the model was then extended to include a set of observed covariate factors (described in the supplementary material online) drawn from the study database (earthquake exposure impact, mental health and substance use disorders during the period 25–30 years, PTSD during the period 25–30 years, family living standards at age 30, gender, New Zealand Māori ethnicity, IQ as measured at ages 8–9, that were significantly (p < 0.05) correlated with peri-traumatic stress, disruption distress and MD symptoms. For the structural model, the covariate factors were permitted to be correlated, and peri-traumatic stress, disruption distress and MD symptoms were regressed onto the set of covariate factors.
Finally, to examine the robustness of the findings to alternative conceptualisations of the MD measure, a supplementary analysis was conducted in which the latent measure of MD symptoms over the previous 12 months was replaced by a latent measure of MD symptoms currently experienced by the participant at the age 35 assessment (with all other variables remaining the same), and the analysis repeated.
Results
Structural model of the associations between peri-traumatic stress, disruption distress and MD symptoms
The SEM depicted in Figure 1 was fitted to the variance–covariance matrix of the split-half indicators of the latent measures of MD symptoms, peri-traumatic stress and disruption distress (see the ‘Method’ section and Figure 1). This model assumed direct linkages to MD symptoms from both peri-traumatic stress and disruption distress, as well as direct and indirect paths from each of the covariate factors to MD symptoms, with indirect paths fitted via peri-traumatic stress and disruption distress. The model showed a good fit to the observed data, χ2(6) = 10.403, p = 0.11; RMSEA = 0.039; CFI = 0.998.
Table 1 shows the matrix of estimated correlations between the latent measures of MD symptoms, peri-traumatic stress and disruption distress implied by the fitted model. The table shows that when measurement unreliability was taken into account, there were strong and statistically significant correlations between all three latent measures, with correlation coefficients ranging from 0.169 to 0.627.
Correlation matrix for latent measures of MD symptoms, peri-traumatic stress and disruption distress.
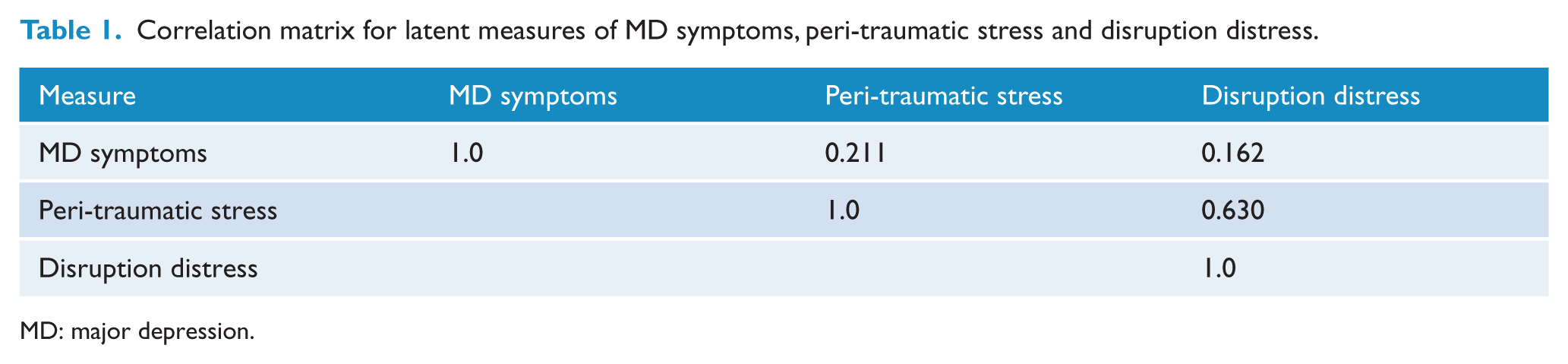
MD: major depression.
Fitted model results
The key results of model fitting are displayed in Figure 1 which shows the standardised regression coefficients for each path in the model. Inspection of the figure shows the following:
There was a statistically significant (p < 0.01) pathway from peri-traumatic stress to MD symptoms (β = 0.180).
Despite the significant (p < 0.05) estimated correlation between disruption distress and MD symptoms, the fitted model reveals that the pathway from disruption distress to MD symptoms was not statistically significant (β = 0.048; p = 0.47).
Peri-traumatic stress and disruption distress remained strongly correlated in the fitted model (r = 0.63; p < 0.0001)
The above results suggest that while both peri-traumatic stress and disruption distress were significantly correlated with MD symptoms, the linkages between these factors were largely explained by the direct effect of peri-traumatic stress on MD symptoms, and the correlation between peri-traumatic stress and disruption distress.
Accounting for possible covariate factors
As noted in the ‘Method’ section, the model was then extended to include a series of covariate factors which were significantly (p < 0.05) correlated with peri-traumatic distress and disruption distress. These covariate factors included gender, IQ (as measured at ages 8–9), Māori ethnicity, mental health and substance use disorders (ages 25–30), PTSD (ages 25–30), family living standards at age 30 and a measure of earthquake exposure. The results of these analyses showed that the model parameters and goodness-of-fit indices were not materially affected by the inclusion of these covariate factors, suggesting that the linkages between peri-traumatic stress, disruption distress and MD symptoms were best represented by the more parsimonious model presented in Figure 1. However, the model parameters for the associations between the covariate factors and peri-traumatic stress, disruption distress and depression are presented in Supplementary Table S1.
Supplementary analysis
To examine the robustness of the findings to using an alternative measure of MD, the above analysis was repeated using the latent measure of current MD symptoms in place of the latent measure of MD symptoms over the previous 12 months. The model showed an excellent fit to the observed data, χ2(10) = 7.47, p = 0.28; RMSEA = 0.022; CFI = 0.999.
The results of this analysis were very similar to those reported above, with a statistically significant (p < 0.0001) pathway from peri-traumatic stress to MD symptoms, and a non-significant (p = 0.32) pathway from disruption distress to MD symptoms. Also, as in the previous model, peri-traumatic stress and disruption distress were significantly correlated (p = 0.0001).
Discussion
This study examined MD symptoms, disruption distress and peri-traumatic stress in response to a major disaster, the Canterbury Earthquakes of 2010–2011, among members of a well-studied birth cohort, using SEM to examine the linkages between these factors. This analysis leads to several general conclusions.
The analysis shows that while MD symptoms, peri-traumatic stress and disruption distress were correlated, the experience of peri-traumatic stress following exposure to the earthquakes had a direct influence on MD, whereas distress related to disruption caused by the disaster sequence did not have a direct influence on MD. These results were robust both to control for a series of covariate factors and to the use of an alternative measure of MD symptoms (current symptoms). The results of these analyses suggest that any increased risk of MD symptoms following exposure to a major disaster is likely due to the experience of peri-traumatic stress during and immediately following the experience of the events of the disaster, and is not directly related to distress associated with any disruption to daily living that may be experienced as a result of the disaster.
These results suggest two important conclusions. The first is that the extent to which the individual experienced intense fear/peri-traumatic distress during the earthquake was a determinant of depressive symptomatology in response to this disaster. Peri-traumatic stress has been extensively cited as a risk factor for PTSD (Cenat and Derivois, 2014; Goenjian et al., 2011; Nishi et al., 2012), and we also reported this association in a previous paper (Boden et al., 2015). However, the association of peri-traumatic distress with depression has not been emphasised, although similar findings have been reported. These studies report that peri-traumatic distress and early dissociative symptoms have been shown to be a reliable predictor of depressive symptoms (Cenat and Derivois, 2014; Fullerton et al., 2004). In addition, other experiences not included in this study but previously described as peri-disaster factors such as having a peri-event panic attack (Person et al., 2006), fear for life (Bryant et al., 2014), bereavement during disaster (Bryant et al., 2014; Tang et al., 2014), sustaining severe property damage (David et al., 1996; Seplaki et al., 2006) and being injured (Maes et al., 2000) have also been reported to increase the risk of depression. This suggests that peri-traumatic events have perhaps been under-recognised as risk factors for MD. There is an extensive literature from animal models suggesting that there are individual differences in fear responses to the same aversive stimuli (Liu et al., 2014). The findings from this study would similarly suggest that an individual’s emotional response during the disaster may play a critical role in the development of MD. It may also suggest that it is important to research the impact of early intervention for those identified as having high levels of peri-traumatic distress on the subsequent development of both PTSD and MD.
The results also somewhat counterintuitively suggest that the lingering disruptive effects of disaster exposure do not increase the risk of MD. The Conservation of Resources Theory in which capacity to recover from mass trauma is shaped by material and social resources and loss (Bleich et al., 2006; Hobfoll, 2001) is often cited as an explanation for depression occurring after a disaster (Hall et al., 2008). Consistent with this theory, studies report that the number of post-disaster stressful life events, financial loss or job loss increase the risk of depression (Person et al., 2006). However, consistent with our findings, a recent study in survivors of the Haiti earthquake reported that although life events were an important predictor of PTSD symptoms, they did not predict depressive symptoms (Cenat and Derivois, 2014). Interestingly, although high perceived social support has been shown to be protective for the onset of PTSD (Galea et al., 2005), the results for MD are less consistent (Gabriel et al., 2007; Person et al., 2006). Although we did not specifically measure social support, there was a well-organised and ongoing response to the earthquakes in Canterbury with widespread community action and support for those afflicted. This strong community-based approach may have acted as a mitigating factor for those with high levels of earthquake-related adversity (Wang et al., 2000).
Strengths and limitations
The strengths of this study include the availability of data from a well-studied cohort and the use of a model which tests for both peri-traumatic and post-event distress simultaneously. Previous studies which report that MD is related to post-event factors have not looked at confounders of this association. However, one limitation of this approach is that the strong correlation between peri-traumatic stress and disruption distress may have made it difficult to detect an association between disruption distress and depression. This was further compounded by the fact that only a portion of the variability in depression would have been explained by events related to the earthquake (as compared with PTSD) (Boden et al., 2015).
A limitation of the study relates to it being of a cohort of people which means that the findings are limited to a population in their mid-30s who potentially may have been less financially impacted than other age groups by the earthquakes (Norris et al., 2002). A further limitation may be the timeframe of the assessment, which was 20–24 months after the onset of the earthquake sequence, which may limit conclusions about longer term reactions to the earthquakes. It is possible that the finding in this study that post-event disruption stress does not increase the risk of MD may be explained by the timing of our study. Although it was nearly 2 years post-disaster, for many people with complex post-disaster difficulties such as unresolved housing insurance claims, the impacts of this had not at this stage been at their height. We may find when we re-survey people 5 years post-disaster that the results are different reflecting this.
A further limitation is that the assessment of earthquake exposure may be limited to the extent to which self-reported personal perceptions of the events may be subject to the usual biases inherent in self-report, and in particular the use of some retrospective data. This is due to the nature of longitudinal studies for which data are collected every 5 years, which will inevitably therefore include situations (such as the present one) in which retrospective data are used. However, the analytical plan in the present paper is the same as that used in a number of similar CHDS papers (Boden et al., 2015).
In addition, it should be noted that only a small minority of respondents (11.7%) met criteria for MD during the 12 months prior to the assessment at age 35, which implies that the parameter estimates obtained in the analyses may be subject to some degree of imprecision (as smaller base rates of an event mean that there is more error likely to be attached to the estimate).
For the future
There have been very few prospective and longitudinal studies after natural disasters, and the outcome of the planned further assessment of this birth cohort 5 years after the start of the earthquakes will provide important information on the course of MD and the trajectory of responses which are fields of increasing interest (Bonde et al., 2016; Nandi et al., 2009).
Conclusion
We found that the extent to which the individual experienced intense fear/peri-traumatic distress during the event was a determinant of depressive symptomatology and somewhat counterintuitively, not the lingering disruptive effects of disaster exposure. This suggests that peri-traumatic distress has been under-recognised as a predictor of major depressive disorder after a disaster. It also points to the importance of researching the impact of early intervention for those identified as having high levels of peri-traumatic distress on the subsequent development of both PTSD and MD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by grants from the Health Research Council of New Zealand, National Child Health Research Foundation, The Canterbury Medical Research Foundation and the New Zealand Lottery Grants Board.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.