
Abstract
Objectives:
There is a growing body of research investigating the relationship between child sexual abuse and a range of adverse outcomes. However, very little is known about the long-term co-occurrence of psychiatric disorders and behavioral problems among this vulnerable population, or the interaction between characteristics of the abuse, such as the nature and timing of the child sexual abuse, and the extent of subsequent adversities. This study aimed to determine the rate and co-occurrence of mental health morbidity, criminal justice system contact, and fatal self-harm among medically confirmed victims of child sexual abuse, and to identify abuse variables associated with a greater likelihood of cumulative adverse experiences.
Methods:
The forensic medical records of 2759 cases of child sexual abuse assessed between 1964 and 1995 were linked with public psychiatric, criminal justice and coronial administrative databases between 13 and 44 years following abuse. Cases were compared to 2677 matched comparisons from the general population.
Results:
Abuse victims were more likely (odds ratio = 7.2, 95% confidence interval = [4.9, 10.4], p < 0.001) to experience cumulative adverse psychiatric and behavioral problems relative to comparisons. Almost half (47.6%) of victims who died of suicide or drug overdose had a history of offending, further victimization and mental illness. Relative to comparisons, female victims demonstrated the largest increase in odds for cumulative outcomes (odds ratio = 9.8, 95% confidence interval = [5.8, 16.8], p < 0.001), whereas in absolute terms, male victims were at an elevated risk for all types and combinations of adverse outcomes, except fatal self-harm. Boys who were older at abuse, had multiple abuse episodes or who were abused by an extra-familial perpetrator were most likely to experience poorer clinical trajectories. Only being older at abuse was associated with cumulative adverse experiences for females.
Conclusions:
Sexual abuse, particularly during adolescence (ages 12–16 years), appears to be a risk factor for co-occurring adverse experiences. This study identifies particular groups of child sexual abuse victims as at-risk and requiring targeted intervention.
Introduction
Child sexual abuse (CSA) is all too frequent, with approximately 15% of children exposed to contact abuse, one-third of which involves penetration (Fergusson and Mullen, 1999; Finkelhor, 1994). Increased risk for adverse outcomes including mental illness, behavioral problems and social problems has been associated with a CSA history (Fergusson and Mullen, 1999; Gilbert et al., 2009; Hillberg et al., 2011; MacMillan et al., 2009; Paolucci et al., 2001; Putnam, 2003). The vast majority of available studies in this area have utilized retrospective cross-sectional methodologies (DiLillo et al., 2006; Fergusson and Mullen, 1999), which have been criticized due to their dependence on the reliability of informants, sampling biases and their limited capacity to reliably ascertain the temporal order, and therefore causality, between retrospective reports of CSA exposure and relevant outcomes (Fergusson et al., 2008; Hardt and Rutter, 2004; Maughan and Rutter, 1997; Widom et al., 2004). Although more recent research indicates that biases associated with the retrospective recall of CSA are in fact likely to be small (Fergusson et al., 2011, 2013), longitudinal prospective analyses that determine the contemporaneous exposure to CSA among a sample of children, and then follow the developmental course of these children over a protracted period to ascertain the presence of a variety of outcomes, have the potential to deliver several methodological advantages (Cutajar et al., 2011). These may include avoidance of selective sampling and errors or biases related to recall (e.g. forgetting, reconstruction, reluctance to disclose), the ability to account for potentially confounding factors and the establishment of temporal sequencing and causal priority (Cutajar et al., 2011; Fergusson and Mullen, 1999; Gilbert et al., 2009).
Unfortunately, however, traditional longitudinal prospective studies create several substantive, economic and ethical challenges that are rarely overcome. Thus, an alternative methodology that is both cost and time efficient, and that preserves several qualities of prospective longitudinal methodologies, involves the linkage of official medical records of CSA to a variety of current administrative databases related to outcomes of interest (Cutajar et al., 2011; Widom, 1997). Although it is acknowledged that the use of official records to ascertain cases of CSA may still introduce a source of systematic bias, including an overrepresentation of children subject to more severe forms of sexual abuse and/or who experience a range of other childhood adversities, thereby affecting the generalizability of findings to unreported or unascertained cases of CSA (Fergusson et al., 2011, 2013), this approach has methodological value as the ordering of events can be more reliably determined and epidemiological questions regarding the putative risks of CSA occurring at the more severe end of the continuum can be investigated with greater precision (Cutajar et al., 2011).
Notwithstanding the issues raised above, both retrospective and prospective studies provide compelling evidence that supports a link between CSA and mental health problems (Calam et al., 1998; Cutajar et al., 2010a; Dube et al., 2005; Fergusson et al., 1996, 2008; Kendler et al., 2000), self-destructive behaviors (Cutajar et al., 2010c; Nickel et al., 2004; Nuemann et al., 1996; Paolucci et al., 2001; Plunkett et al., 2001), offending (Cutajar et al., 2011; Johnson et al., 2006; Nathan and Ward, 2002; Siegel and Williams, 2003; Widom and Ames, 1994) and further victimization (Briere and Elliott, 2003; Cutajar et al., 2011; Elliott et al., 2004; Finkelhor et al., 2007, 2011; Widom et al., 2008). In one program of prospective research, relative to comparisons, CSA victims were significantly more likely to develop all types of psychological disorders, with the exception of eating disorders (Cutajar et al., 2010a, 2010b, 2010c), and were at a remarkably increased risk of suicide and fatal drug overdose. This research also demonstrated that a significantly greater proportion of CSA survivors experienced a subsequent sexual assault, threat of violence or actual violence, and engaged in all types of offending behavior at higher rates, with odds of up to seven and eight times higher observed for sexual and violent offenses, respectively (Cutajar et al., 2011).
The nature and extent of the problems identified in CSA survivors can, however, vary considerably. Some are wide-ranging and incapacitating, whereas in others, no or very few obvious disturbances are found (Australian Institute of Family Studies, 2014). Problems associated with histories of CSA can often be inter-related, whereby the presence of one may increase the likelihood of another (Australian Institute of Family Studies, 2014). Although there has been an expanding evidence base investigating the psychosocial sequelae of CSA, the majority of studies have considered a limited range of outcomes. Few studies, with a handful of notable exceptions (e.g. Fergusson et al., 2013; Trickett et al., 2011), have investigated the negative effects of CSA across a host of domains measured over an extended period of time. In addition, where studies do explore several outcomes independently, even fewer still investigate the extent to which a range of disorders and disturbances across various domains of functioning may co-occur among survivors of CSA. Factors such as victim gender, age at abuse and the nature of the abuse, which may be associated with more problematic clinical trajectories, characterized by cumulative adverse experiences, remain to be clarified. These are key empirical and clinical questions, the answers to which may be used to inform an evidence base for policy and therapeutic responses to CSA.
This study investigated the rate and co-occurrence of adverse experiences found among CSA victims, including psychopathology, offending, further victimization and fatal self-harm. Furthermore, it considered whether victim gender, age at abuse and characteristics of the abuse were associated with the extent of subsequent problems. It was hypothesized that adverse experiences would co-occur at significantly higher rates among CSA victims relative to non-abused comparisons, and that victim gender and abuse variables would be related to the degree of adversities experienced. This research overcomes several shortcomings of previous studies by prospectively examining the long-term impact of CSA among a large sample of both male and female victims, with a matched comparison sample.
Methodology
Design
The current study used a historical cohort design employing data linkage for a sample of cases with substantiated CSA and a comparison sample matched on age and gender (see Cutajar et al., 2010a, 2010b, 2010c, 2011). This research was conducted in the Australian state of Victoria. Victoria has a diverse and multicultural population of approximately 5.9 million people, of whom 4.2 million live in the capital city, Melbourne.
Sample sources
Cases
The CSA sample was obtained from records collected by the Office of Forensic Medicine, which collated the evidence and performed examinations on children in Victoria, at the request of police and/or child welfare and protection agencies following allegations of CSA. The CSA cohort comprised all 2759 (2201 females, 558 males) cases assessed as having been victims of contact sexual abuse between 1964 and 1995. The following abuse-related information was extracted from the records and used in the present research: the age at which the index abuse occurred (dichotomized by approximate age of puberty onset; under age 12 and ages 12–16 years), whether the abuse was penetrative or non-penetrative and, where available, whether it involved a single occurrence or multiple episodes, an intra-familial or extra-familial perpetrator and a single abuser or multiple abusers.
Comparisons
A comparison group without a known history of CSA was established using the Australian Electoral Commission, which drew a random community sample of 5000 individuals from Victoria’s electoral roll aged 16–61 years. A subsample of 2677 individuals was matched on gender and 2-year age banding (e.g. 20–21 years) to the CSA cases (nil matches identified for 82 cases). Givenvoting registration is compulsory in Australia for those aged 18 years and older, 93.74% of the voting-eligible population appears on the electoral rolls (Victorian Electoral Commission, 2014).
Data sources and data linkage
The CSA cohort was linked with three administrative databases: public mental health, Victoria Police (offending and victimization) and coronial services (fatal self-harm—suicide and drug overdose). Comparison cases were linked with the mental health and police databases but, in accordance with ethical approval, not the database containing self-harm-related deaths. Data linkage to the coronial databases occurred in 2008, and linkage to the police and psychiatric databases was completed in 2009 and 2008/2009, respectively. All extracted matches were provided to researchers in a de-identified encrypted format to ensure anonymity. A more detailed account of all data linkage protocols can be found in earlier studies utilizing this dataset (see Cutajar et al., 2010a, 2010b, 2010c, 2011).
Mental health
Contacts with public mental health services for the CSA and comparison cohorts were obtained from the Victorian Psychiatric Case Register (and its successor, the Redevelopment of the Acute and Psychiatric Information Directions database), a statewide patient information system, which contains individual records of all public psychiatric inpatient admissions and, since 1990, contacts with community mental health and emergency room services. Contacts with the private health sector are not contained within the database. The linkage procedure used a deterministic then probabilistic approach using SOUNDEX (a phonetic algorithm used for indexing names by their sound), extracting exact and possible matches using iterations of identifying information (i.e. date of birth, gender, first name and surname).
For the present research, mental health service contact was coded as a dichotomous variable indicating whether a CSA case or comparison had at least one life-time contact with public mental health services in Victoria, up until the time of data linkage. Diagnostic information according to the International Classification of Diseases–9th/10th Revision (ICD-9/10) was also extracted from the mental health register and used in supplementary analyses.
Offending and subsequent victimization
Offending and further victimization histories were established using the Victoria Police criminal records database (Law Enforcement Assistance Program; LEAP), within which crime-related information collected by the police during the course of their work is routinely documented. The LEAP database contains all contacts (e.g. witnesses, victims, alleged offenders, offenders) with police in Victoria since 1993. Information prior to 1993 is maintained as hard copy files, with limited data from these files contained within LEAP. We utilized criminal charges as the measure of offending because at court, charges are frequently combined or dropped during progress toward a guilty plea. A CSA case or comparison was coded as having an offense or victimization history if, at the time of data linkage, they had at least one life-time criminal charge or reported victimization incident (of any nature), respectively, as per the LEAP database.
If charges were laid or victimization incidents had occurred prior to the index episode of CSA, these were excluded. Furthermore, officially recorded sexual victimization incidents that corresponded with the time of forensic examination were also excluded. Linkages with the LEAP database were established first by manually searching the police database for matches on the basis of name, date of birth and gender. Deterministic then probabilistic matching procedures using SOUNDEX were used to enhance matching.
Fatal self-harm
The Victorian Coronial Information Database and the National Coroners Information System provided information on deaths caused by suicide and drug overdose in victims of CSA. Australian legislation requires that all deaths of an unexpected, unnatural, violent, traumatic or unexplained manner be reported to the state coroner, who has a statutory responsibility to investigate. A suicide would be determined as such by the coroner, only in cases where the evidence suggested, beyond reasonable doubt, that the death was caused by the intentional effort of the deceased person to end his or her own life. Fatal self-harm data were not obtained for the comparison cohort; thus, the current study primarily focuses on absolute rather than relative rates for coronial data; our previous study using this CSA cohort has compared the rate of suicide and fatal drug overdose with age-limited statistical data for the general population (Cutajar et al., 2010c), and these comparative data are briefly reported in context within the results section. For data linkage, the surname, first name, gender and date of birth for each CSA case were cross-checked with the coronial databases manually and then using Structure Query Language scripts; only exact matches were extracted.
Statistical analyses
This study investigated the presence (coded as ‘yes/no’) of adverse experiences including public mental health service contacts, criminal histories, further victimization incidents and fatal self-harm. The rate of exposure to combinations of adverse experiences and the inter-relationships among these adverse experiences were compared between the CSA and comparison cohorts. The two samples were compared using chi-squared tests of association, and where significant differences were found, odds ratios (ORs) with 95% confidence intervals (CIs) were reported to facilitate interpretation. Multi-way-frequency analysis was used to investigate whether there was a higher order relationship among the adverse experiences. Within group comparisons were also undertaken to determine which abuse variables were associated with cumulative adverse experiences. Due to the small N for deaths involving suicide or drug overdose, these data were utilized for descriptive purposes only and were excluded from statistical analyses. The alpha level was set at 0.05, two-tailed, for all analyses.
Ethics
Ethical approval, including a consent waiver, was granted by six independent human research ethics committees: Monash University, Victoria Police, Department of Human Services, Department of Justice, Victorian Institute of Forensic Medicine and Swinburne University of Technology.
Results
Description of the CSA cohort
Of the 2759 CSA cases, 71 (2.57%) had recorded contact with public mental health services prior to the index episode of CSA and thus were excluded from analyses. Excluded cases did not differ significantly to CSA victims who had mental health service contact subsequent to their index abuse on study variables, except that they were approximately 1 year older at the time of abuse (M = 12.04 years, SD = 3.58 years vs M = 10.85 years, SD = 4.27 years; t = 2.27; p < 0.05). The Mean age of the retained 2688 cases (80.1% female) at examination was 10.17 years (SD = 4.46 years; range = 0.27–16.99 years); females were slightly older (M = 10.38 years, SD = 4.49 years) than males (M = 9.34 years, SD = 4.23 years) (t = 5.01; p < 0.001). Completed, partial or attempted penetration of an orifice by a penis, finger or other object was present in 63.1% of cases, and was higher for females than males (65.1% vs 55.4%; χ2 = 17.15; p < 0.001). The perpetrator was a relative for 51.5% of female victims and 36.1% of male victims (χ2 = 25.17; p < 0.001). The majority was abused by a single offender (94.4%), on multiple occasions (61.8%). The mean age of the CSA cohort at the time of the most recent data linkage was 35.55 years (SD = 11.02 years; range = 16.29–59.58), with a mean follow-up period of 25.37 years (SD = 8.12 years; range 13.97–44.77 years).
Subsequent adverse experiences
CSA victims were significantly more likely than comparisons to have subsequently had one or more of the adverse experiences (52.0% vs 39.2%; p < 0.001) (Table 1). CSA victims were significantly more likely than comparisons to have had a contact history with public mental health services (OR = 3.7, 95% CI = [3.1, 4.3]; p < 0.001), to have been charged with a criminal offense (OR = 4.8, 95% CI = [4.0, 5.7]; p < 0.001) and to have been victimized further for any type of crime subsequent to their index episode of abuse (OR = 1.1, 95% CI = [1.0, 1.3]; p < 0.05). The ORs for all pairs of adverse experiences were found to be significantly elevated for CSA victims over comparisons (Table 1). Having had both mental health service contact and a criminal history was markedly elevated relative to comparisons (OR = 7.0, 95% CI = [5.0, 9.7]; p < 0.001). The odds of mental health problems, offending and victimization co-occurring were also significantly higher among CSA cases relative to comparisons.
Rates of exposure to types and combinations of adverse experiences a for the CSA and comparison cohorts.
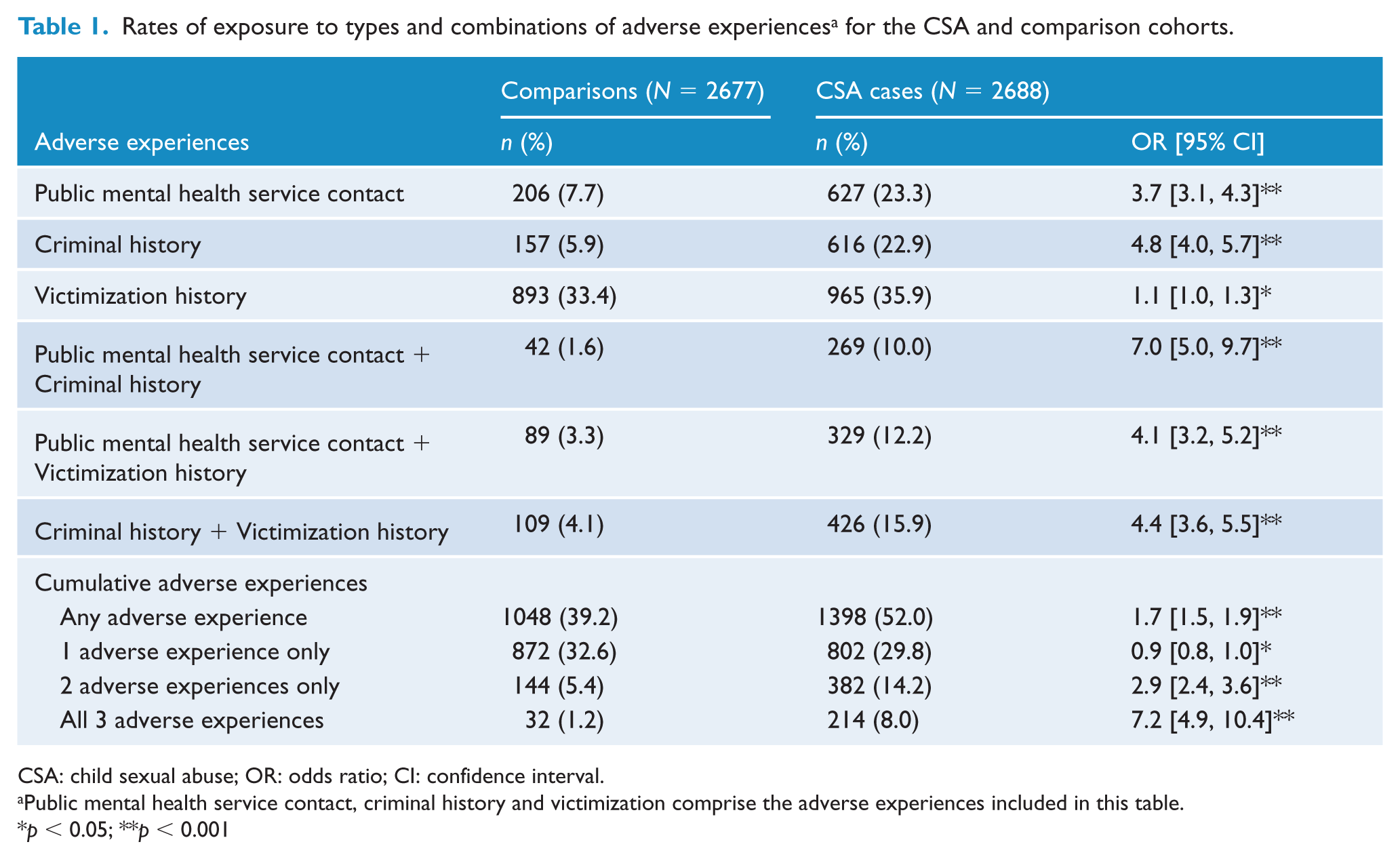
CSA: child sexual abuse; OR: odds ratio; CI: confidence interval.
Public mental health service contact, criminal history and victimization comprise the adverse experiences included in this table.
p < 0.05; **p < 0.001
A number of reportable deaths were recorded in the CSA group (n = 21, 0.8%; 16 females, 5 males); differences between male and female victims with respect to rates of fatal self-harm were non-significant (0.9% vs 0.7%; p = 0.66). Our previous study utilizing this CSA sample demonstrated that these rates denoted a marked increase in relative risks for suicide (relative risk = 18.09) and fatal drug overdose (relative risk = 49.22) compared with age-limited national data for the general population (Cutajar et al., 2010c). The current findings also indicated that of the 21 reportable deaths, 95.2% experienced at least one other adverse outcome (i.e. 16, 76.2%, had mental health services contact; 15, 71.4%, had a criminal history; and 12, 57.1%, had been victimized further). Almost half (n = 10, 47.6%) of the reportable deaths among CSA victims were known to police for both offending and further victimization, and also had contact with public mental health services.
Gender differences
Increases in adverse experiences were examined by gender (Table 2). All types and combinations of adverse experiences were more common in male CSA victims relative to female CSA victims; however, female victims relative to female comparisons had rates elevated to a similar degree to, and sometimes higher than, males. For exposure to all three adverse experiences, in relative terms, female victims fared more poorly than males.
Rates of exposure to types and combinations of adverse experiences a for the CSA and comparison cohorts according to gender.
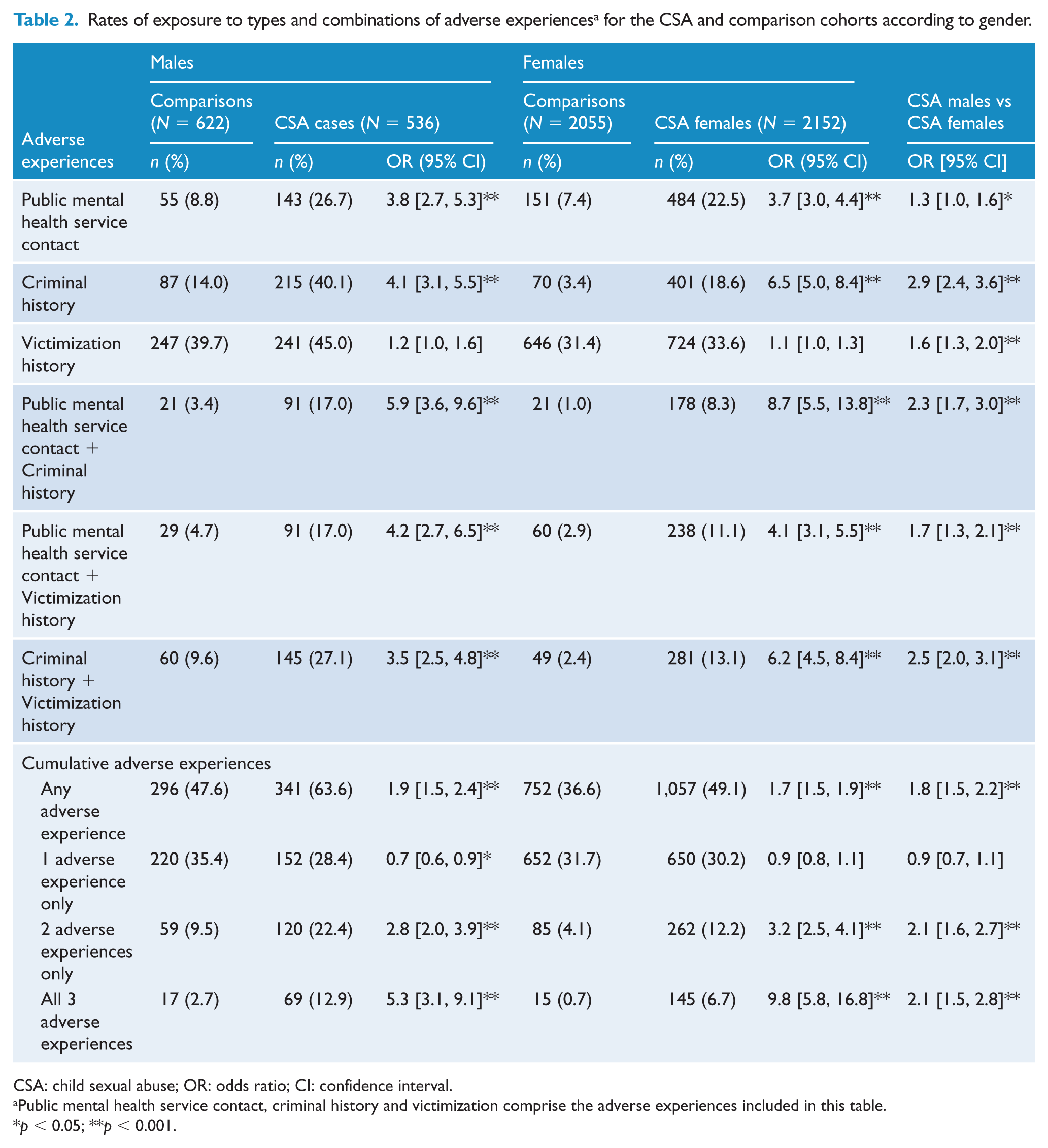
CSA: child sexual abuse; OR: odds ratio; CI: confidence interval.
Public mental health service contact, criminal history and victimization comprise the adverse experiences included in this table.
p < 0.05; **p < 0.001.
Relationships among adverse experiences
A significant three-way association between public mental health service contact, offending and further victimization was observed among the CSA cohort (partial χ2 = 5.35; p < 0.05) but not the comparison cohort; the four-way association, which included gender, was not found to be significant for CSA victims or comparisons. To investigate the nature of this three-way interaction, chi-square analyses for each pair of variables were performed separately for each level of the third variable, which revealed that each two-way association was significantly strengthened (or moderated) by the presence of the third variable. This was particularly prominent for the relationship between criminal history and subsequent victimization, where the odds that these two adverse experiences would co-occur increased from 4.8 (95% CI = [3.8, 6.1]; χ2 = 178.79; p < 0.001), when there was no contact with public mental health services, to 8.2 (95% CI = [5.7, 11.9]; χ2 = 138.55; p < 0.001) when there was.
To determine whether there was a particular psychiatric diagnostic category (i.e. clinical disorder, substance-use disorder) that could account for the effect of public mental health service contact on the relationship between criminal history and further victimization among CSA cases, additional ORs were calculated according to three major diagnostic groupings. Specifically, among CSA victims, the odds of both offending and being victimized further were higher if they had a known Axis-I clinical disorder (OR = 9.2; 95% CI = [5.8, 14.5]; χ2 = 102.55; p < 0.001), substance-use disorder (OR = 7.8; 95% CI = [3.5, 17.1]; χ2 = 29.47; p < 0.001) or personality disorder (OR = 13.5; 95% CI = [4.9, 37.1]; χ2 = 29.83; p < 0.001).
Abuse variables and cumulative adverse experiences
Children abused when they were aged between 12 and 16 years were significantly more likely than younger children to accumulate all three adverse experiences (Table 3). Although particularly prominent among males (OR = 2.4, 95% CI = [1.4, 3.9]; p < 0.01), this difference was consistent for both males and females. Having multiple episodes of abuse (OR = 2.6, 95% CI = [1.0, 6.6]; p < 0.05) and an extra-familial perpetrator (OR = 3.6, 95% CI = [1.6, 8.3]; p < 0.01) emerged as significant risk factors for cumulative problems for male CSA victims but not females. Whether victims were sexually penetrated or whether they had more than one perpetrator did not significantly increase their likelihood of accumulating all three adverse experiences.
Comparison of risk of CSA victims developing cumulative adverse experiences a as a function of abuse-related characteristics.
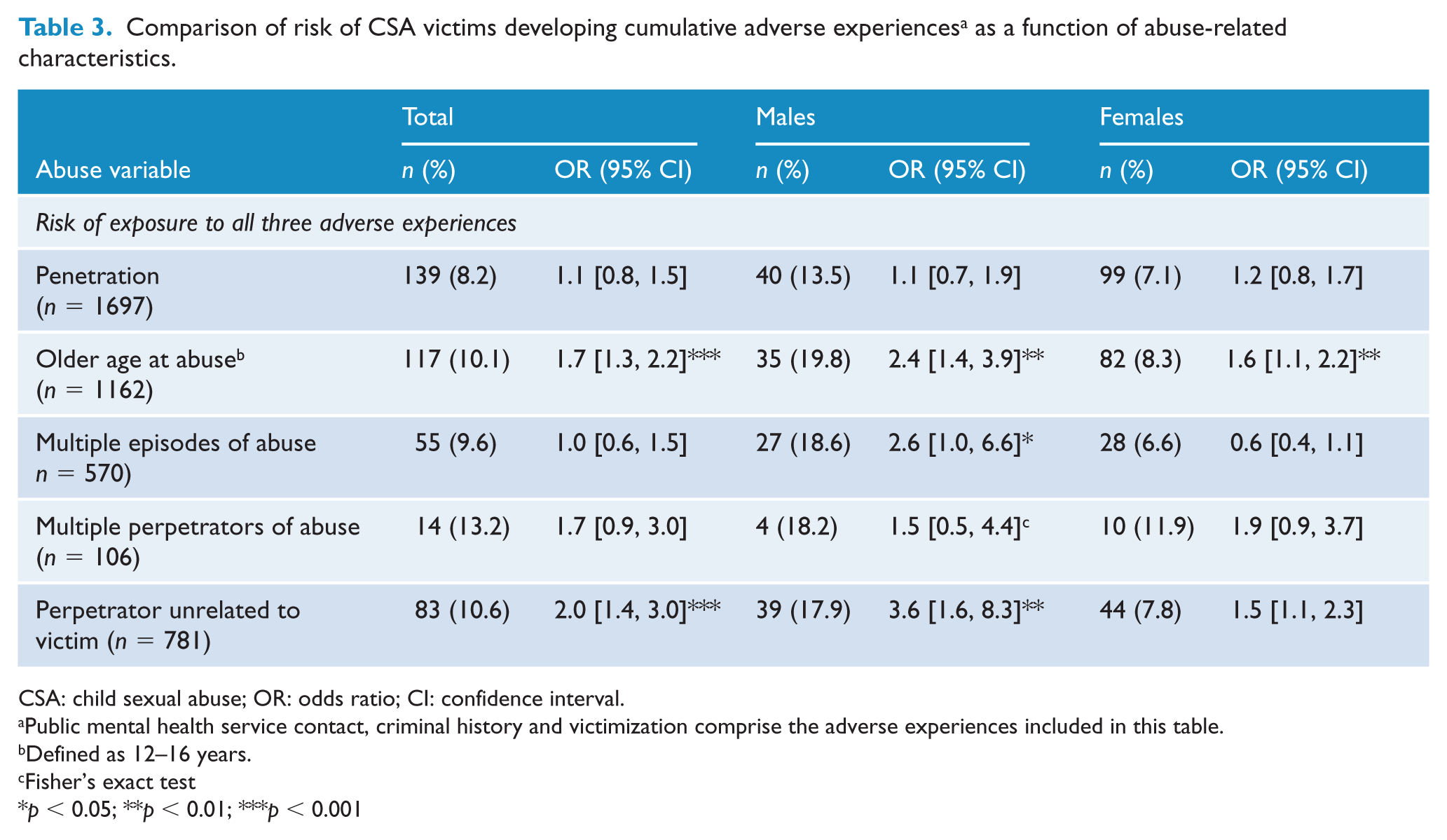
CSA: child sexual abuse; OR: odds ratio; CI: confidence interval.
Public mental health service contact, criminal history and victimization comprise the adverse experiences included in this table.
Defined as 12–16 years.
Fisher’s exact test
p < 0.05; **p < 0.01; ***p < 0.001
Discussion
Subsequent adverse experiences among victims of CSA
More than half (52%) of CSA victims later experienced problems in one or more of the following domains: mental health problems, offending, further victimization or fatal self-harm. The prospective methodology addresses several limitations of previous research by relying on cases of sexual abuse confirmed at the time, with officially recorded outcomes. The results indicate that as the number of adverse experiences accumulated, the strength of CSA as a relevant risk factor also increased, where the odds of mental health problems, offending and further victimization co-occurring were markedly higher among CSA cases relative to comparisons.
Our previous studies have established that, individually, public mental health service contacts, offending, subsequent victimization and deaths by suicide or drug overdose occur at significantly higher rates among this CSA cohort relative to comparisons (Cutajar et al., 2010a, 2010c, 2011). It is perhaps noteworthy that while the OR comparing the likelihood of further victimization (of any nature) among CSA victims relative to comparisons was found to approach one suggesting limited clinical relevance, our previous research has demonstrated that when we specifically focus on victimization experiences of an interpersonal nature (e.g. actual or threatened violence, sexual offenses, stalking), the ORs increase considerably (see Cutajar et al., 2011).
Aside from the association between CSA and an increased risk for developing any one of these adverse experiences, the current study adds to the literature by revealing the extent to which these adverse experiences co-occur among survivors, and that cumulatively they are associated with significantly increased rates of subsequent problems. The results are consistent with the general non-CSA literature, confirming a link between offending and victimization (Baron, 1997; Jennings et al., 2012), and between psychopathology and offending (Ogloff, 2009; Short et al., 2013). The finding that these adverse experiences co-occur at significantly higher rates among CSA victims in particular, however, confirms further that CSA is associated with a range of detrimental and often inter-related experiences. Similarly, the finding that almost half of the reportable deaths among CSA victims were marked by exposure to all other investigated adverse experiences is consistent with previous findings (Beautrais, 2000; Fergusson et al., 2000). Of course, most CSA victims who experienced co-occurring problems across the three domains (95.3%) did not subsequently die by suicide or drug overdose.
Regarding the role of gender in subsequent adverse experiences, relative to comparisons without a known history of abuse, females fared equally or more poorly than males with respect to risk for all types and combinations of adverse experiences. However, in absolute terms, male CSA victims demonstrated more troublesome clinical trajectories than their female counterparts, except for fatal self-harm, where no gender differences were observed (Cutajar et al., 2010c). This is not surprising given the base rate of adverse experiences was greater for males than females in the comparison cohort. Irrespective of such, the findings suggest that CSA is an issue requiring nuanced understanding of both male and female survivors.
Interactions among adverse experiences
Highlighting the complexity of the inter-relationships among adverse experiences found in victims of CSA, a three-way association between public mental health service contact, criminal history and subsequent victimization was found. Most notably, the presence of a psychiatric history significantly elevated the likelihood that offending and further victimization would co-occur among CSA survivors. Again, this is consistent with the broader clinical literature that demonstrates a link between psychopathology and offending (Ogloff, 2009; Short et al., 2013), and victimization (Walsh et al., 2003). It could be hypothesized that CSA, by way of uncertain mechanisms, may have led to subsequent impairments in affect regulation, reality testing, interpersonal functioning and/or impulse control, which in turn precipitated the offending behavior and further victimization. Alternatively, the ‘poly-victimization’ hypothesis posits that it is the perpetual and pervasive nature of victimization experiences frequently seen in victims of CSA (and other forms of maltreatment) which leads to increased levels of additional adversities and psychosocial distress (Finkelhor et al., 2007, 2011). Irrespective, the temporal sequencing and specific nature of mental illness, offending and further victimization could not be explored with these data; thus, at best, these findings highlight a particularly complex and dysfunctional presentation among CSA victims experiencing cumulative difficulties.
At one level, finding that when one type of difficulty occurs the person is more likely to experience other problems is unsurprising. Clinically, however, when assessing and managing someone with a history of CSA, knowing of the linkages between psychiatric problems, behavioral difficulties, victimization and self-harm may be critical.
The role of abuse variables
The characteristics of abuse identified as being associated with cumulative adverse experiences (e.g. older age of abuse) appear to suggest a ‘critical window’ during which CSA may have additional detrimental impacts than CSA that occurs at a younger age. The years between 12 and 16 are a time of rapid change, physically, socially and emotionally. Children are developing their sense of sexuality. Thus, being the victim of CSA during this critical developmental period may significantly affect the child, perhaps leaving them more susceptible to cumulative adverse experiences than their pre-pubescent peers. Unexpectedly, penetrative abuse was not associated with the presence of all three adverse experiences; thus, our findings provide limited support for the dose-response hypothesis for cumulative problems, namely, that the severity of the abuse determines the extent of the consequences (Fergusson and Mullen, 1999).
With the exception of age at abuse, the failure to demonstrate that other characteristics of the CSA reliably correlated with later adverse experiences for both males and female places a question over any simple causal connection between CSA and the putative outcomes. If CSA itself were a major causal factor, then the nature and context of the abuse would be expected to consistently relate to the frequency and severity of any outcome. The lack of such connections among both males and females in a sample of this size might suggest that CSA acts in part at least as a marker for factors carrying greater causal weight. There are well-established associations between the risk of CSA and pre-existing adverse social and family circumstances (MacKenzie et al., 2010; Mullen et al., 2000). These may hold the key to some, if not all, of the now well-established correlations between CSA and subsequent adverse life experiences.
Limitations
Although overcoming weaknesses in previous research, the methods here include some limitations. First, based on previous research, 5–10% of the comparison cohort likely experienced significant CSA themselves, with an additional 5–10% likely subjected to other types of contact sexual abuse not coming to official attention (Fergusson and Mullen, 1999; Finkelhor, 1994). This produces a systematic bias against finding differences between the CSA and comparison cohorts. In addition, methods based on official records for determining the presence of subsequent difficulties to a greater or lesser extent underestimate their actual prevalence. Importantly, however, adverse experiences were established among the comparison and CSA cohorts in the same manner; thus, while there may be some uncertainty with respect to the reliability of the absolute rates, we can be more confident in the relative rates.
The representativeness of the CSA sample is limited by the fact that it is based on official cases reported to police and/or child protective services. These children frequently come from multiply disadvantaged backgrounds, whereby, in addition to sexual abuse, poverty, physical abuse, emotional neglect and family dysfunction may also be present, thus leading to the increased surveillance by such services. Given we did not have data routinely available for such potentially confounding variables, it becomes increasingly difficult to disentangle the unique contribution of CSA to associated problems from that of the broader disadvantage, maltreatment and deprivation that may characterize some of the sample. Relatedly, despite being able to establish that CSA is a risk factor for long-term cumulative adverse experiences, the methods employed do little to elucidate the mechanisms underlying this complex relationship, nor to determine whether such factors are causal in their effect. Taken together, these methodological limitations suggest that caution is needed when attempting to apply our findings to the broader population of abuse victims.
Implications and conclusions
Notwithstanding questions regarding the representativeness of the sample and causality, the finding that children coming to official attention for CSA are an at-risk population for a wide range of officially recognized individual and cumulative adverse experiences may have important clinical implications for psychiatrists and other mental health professionals. This research demonstrates that approximately 8% of children identified contemporaneously with their sexual victimization will subsequently receive mental health treatment, acquire criminal records and be victimized further. This points to the need for targeted intervention aimed at reducing such risks in these children known to have suffered CSA. Interventions targeting primarily the sexual abuse experience have not been demonstrated to have significant clinical efficacy (Cohen et al., 2006; Finkelhor and Berliner, 1995; Trask et al., 2011). Approaches that recognize the complex interplay between childhood maltreatment and subsequent difficulties, addressing victims’ needs in physiological, psychological, interpersonal, behavioral and social spheres, are perhaps more likely to assist in reducing and managing their risks. It may also be beneficial for clinical assessments to seek to identify victims requiring more intensive monitoring and treatment; in particular, adolescent males, who are exposed to multiple episodes of abuse by non-relatives, may be particularly vulnerable to cumulative adverse consequences.
Although our research indicates that CSA is one of several potential risk factors that identify a child who may be vulnerable to several negative consequences, it would be remiss to assume that CSA is the sole element from which subsequent adversities arise. Indeed, almost 48% of the CSA cohort did not subsequently have contact with public mental health services, were not victimized further or charged with a criminal offense and did not die by suicide or drug overdose. A range of mediating and moderating variables is likely to impact upon the extent and expression of subsequent problems in victims of CSA. Prudence dictates that future research should focus on identifying such vulnerability and resiliency factors, while accounting for the possible role of confounding factors (e.g. socioeconomic disadvantage, family functioning, other forms of child maltreatment), if we are to improve our ability to reduce the long-term damage associated with CSA.
Footnotes
Acknowledgements
We would like to thank A/Prof. David Wells, M.B.B.S., of the Victorian Institute of Forensic Medicine, for his guidance and assistance with the overall program of research; and A/Prof. Denny Meyer, B.Sc. (Hons.), M.B.L., D.B.L., of Swinburne University of Technology, for providing statistical consultation (without compensation) during the preparation of this manuscript. An earlier version of this paper was presented at the Centre for Forensic Behavioural Science, Young People and the Law conference, Prato, Italy, 21–23 September 2015.
Data
The primary data utilized in this research can be provided to readers upon request. Please contact the corresponding author for access.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded in part by a grant from the Criminology Research Council of Australia (Grant: 13/09-10). This funding source had no role in the design, collection, analysis and interpretation of data; the writing of the manuscript; and the decision to submit the article for publication.