
Abstract
Objectives:
The prevention of mental illness involves identifying and modifying those characteristics and exposures of an individual that threaten their mental health – commonly referred to as risk factors. Existing categorisations of risk factors for mental illness are either limited in their scope or oversimplified in their description. As part of a large mental health workforce and service planning project, we set out to develop a more detailed and comprehensive categorisation scheme to describe risk factors for mental illness.
Methods:
We conducted a rapid review of MEDLINE and Google Scholar for meta-analytic studies that examined the characteristics and exposures that typify the population with mental illness in order to identify and categorise potential risk factors.
Results:
The search uncovered 1628 relevant studies, from which 10 primary and 23 secondary categories of risk factors were identified, ranging from genetic and biomedical to psychological and sociocultural. The review revealed interesting distortions in the focus of the literature, with the majority of studies focused on a few disorders (schizophrenia, depression and neurodegenerative disorders) and genetic, psychological and physiological risks. In contrast, environmental (e.g. media exposure) and occupational (e.g. employee health) were under-represented.
Conclusion:
The categorisation scheme developed in this paper is a step towards a more detailed taxonomy of risk factors for mental illness; this will be most useful in guiding clinicians, researchers and policy-makers in driving the prevention agenda forward.
Introduction
Mental illness refers to specific diagnosable health conditions/disorders in which an individual’s capacity to think, behave and interact with other people is affected. The burden of mental illness is considerable, contributed in part by the high prevalence of these disorders. According to the 2007 Australian National Survey of Mental Health and Wellbeing (Slade et al., 2009), 45% of the 16 million Australians aged 16–85 years were estimated to have had a mental disorder at some time in their lives.
High prevalence means high costs to the health system. Over AUD$7.6 billion, or AUD$332 per person, was spent on mental health–related services in Australia during 2012–2013 (Australian Institute of Health and Welfare [AIHW], 2014a), with mental illness accounting for the third largest proportion of health spending, behind cardiovascular disease and oral health (AIHW, 2014b). In addition, the Australian Department of Health conservatively estimate that for ‘every dollar allocated to mental health services in the specialised sector, an additional AUD$3.10 is spent on providing support services to people who require such assistance due to their mental illness’ (Department of Health and Ageing, 2007).
Despite the considerable impact of mental illness on the Australian health-care system, a recent review of mental health services in Australia (National Mental Health Commission, 2014) has shown that the mental health system is heavily oriented towards treatment and disability management, with minimal resources devoted to prevention. For example, it was found that of the AUD$9.5 billion invested by the Australian Commonwealth Government on mental health, only AUD$90.6 million (i.e. <1%) was for programmes under the ‘prevention, health promotion, self-help and education services and programmes’ header. The bulk of mental health funding was allocated to income support for those with chronic mental illness (AUD$4.67 billion) and on public and specialised treatment services (AUD$3.26 billion).
Australian mental health researchers have noted this imbalance in mental health spending (Jacka et al., 2013; Jorm, 2014) and have called for a shift in emphasis towards prevention and promotion, pointing out that there have been no improvements in adult mental health over the last 15–20 years (Jorm and Reavley, 2012), that treatment is limited in the extent to which it can reduce disease burden (Andrews et al., 2004) and that there is increasing evidence that prevention programmes can be both efficacious (Sandler et al., 2014) and cost-effective (Knapp et al., 2011; Mihalopoulos et al., 2011).
The prevention of mental illness and its burden involves identifying and modifying the attributes, characteristics and exposures of an individual that threaten their mental health – commonly referred to as risk factors. Such risk factors are typically identified through correlational, longitudinal and interventional research and summarised in reviews. Existing categorisations of risk factors for mental illness (e.g. Fryers and Brugha, 2013; Institute of Medicine, 1994; World Health Organization [WHO], 2004, 2012) are constrained in a number of ways. Some (e.g. Fryers and Brugha, 2013) involve extensive literature reviews and provide detailed summaries, but limit their scope, for example, to risks in childhood and adolescence. Other reports, like those by the WHO, have a wide scope but provide limited detail on how the risks were identified and use simple categorisation schemes. For example, in a 2004 report entitled ‘Prevention of Mental Disorders’ (WHO, 2004), the WHO presents a long list of unreferenced risk factors divided into two broad domains: (1) social, environmental and economic determinants (e.g. isolation, urbanisation, unemployment) and (2) individual and family-related determinants (e.g. excessive substance use, child abuse and neglect). In 2012, the WHO divided these risk factors into three domains: (1) individual attributes and behaviours (e.g. low self-esteem), (2) social and economic circumstances (e.g. low income and poverty) and (3) environmental factors (e.g. injustice and discrimination) (WHO, 2012).
These broad and poorly defined risk factors have limited application for policy, practice and research, particularly with respect to areas like workforce and service planning (Furber et al., 2015), which require a more detailed and comprehensive breakdown of potential risk factors for mental illness. Within a workforce and service planning context, it is important to gain an overarching view of the types of risk factors for mental illness in order to clearly determine where different service sectors (e.g. health, mental health, welfare and education) and researchers might focus their mental illness prevention efforts.
A reasonable starting point to defining these risk factors in an evidence-based way is to review meta-analyses describing the characteristics and exposures of individuals with mental illness and to then organise these factors into meaningful categories. We argue that the categorisation scheme developed in this paper is a useful starting point from which to launch a more detailed taxonomy of risk factors for mental illness.
Method
Study design
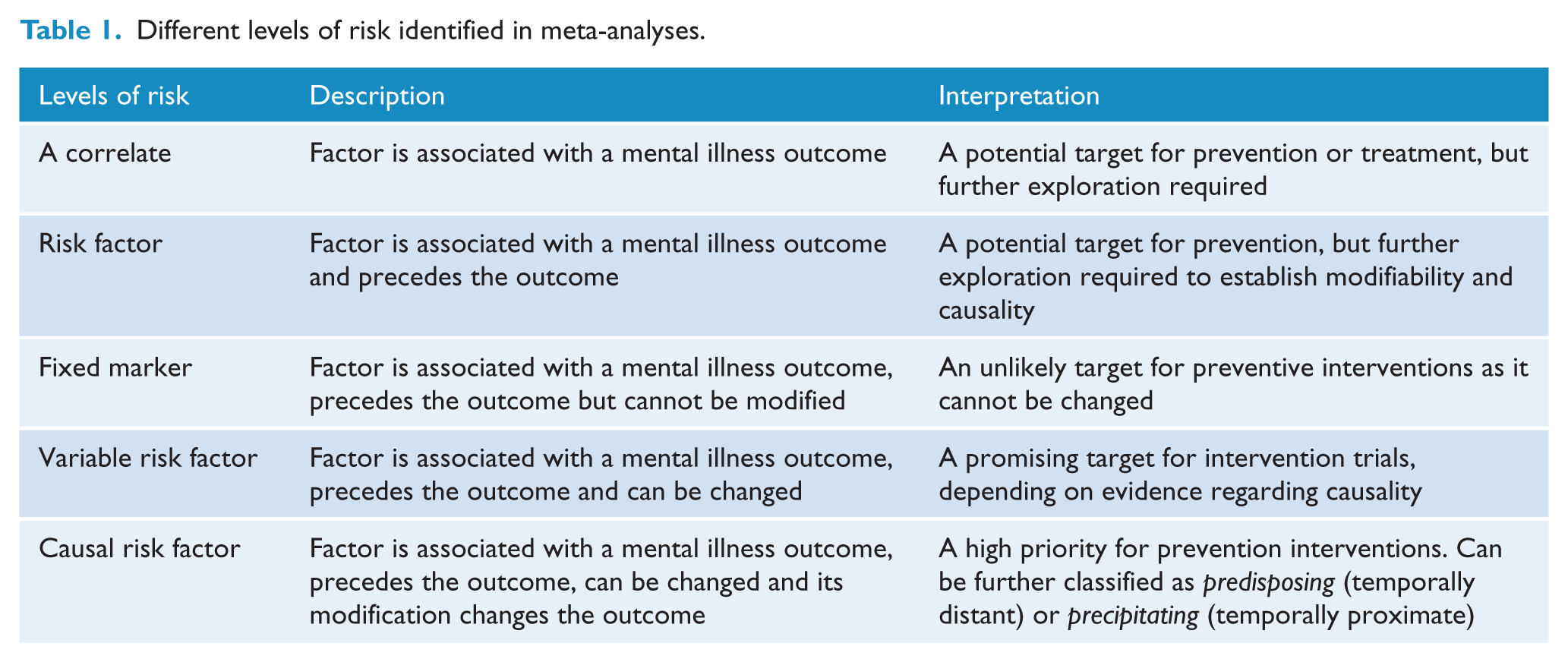
This study was a rapid review of meta-analytic studies. The advantages of this approach are that meta-analyses greatly reduce the number of manuscripts that will meet inclusion criteria while simultaneously covering, at a summary level, potentially thousands of individual studies (feasibility); this approach also identifies factors that have been repeatedly studied (reliability). A disadvantage of using meta-analyses (vs prospective studies, for example), however, is that the illness-factor relationships described within these reviews will fall across the spectrum from correlate to causal risk factor (Table 1; Kraemer et al., 1997). As such, it is acknowledged that some of the factors identified through a review of meta-analyses may not ultimately represent viable targets for prevention intervention.
Different levels of risk identified in meta-analyses.
Inclusion and exclusion criteria
We took an inclusive approach to defining mental illness for the purposes of identifying relevant meta-analyses. Most studies included outcomes that closely followed Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV) or Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5) categories. In addition, we included (1) externalising and internalising disorders, as mental health problems in children and young people are commonly represented using these empirically derived categories; (2) studies of suicide and self-harm as these reflect the strong mental disorder loading on these behaviours; (3) studies of cognitive dysfunction and neurodevelopmental delay, to capture mental health impacts in very young and older individuals; and (4) a ‘mental disorder not specified’ category to capture those studies where different mental disorder outcomes were combined into a single outcome or where generic psychological distress (e.g. neuroticism, stress-related disorder) was a primary outcome.
Some behaviours, indicative of potential mental illness like alcohol consumption, drug use, smoking or disordered eating (e.g. restrictive eating, bulimic behaviours), were only considered as mental disorders if the study specifically referred to ‘abuse’, ‘dependence’ or problematic use suggestive of interference with normal functioning. Similarly, aggression or violence was not assumed to be a disorder unless referred to in the context of disruptive, impulse or conduct disorders or antisocial personality disorder.
The review was limited to meta-analyses that were designed as follows:
Compared affected (i.e. with mental illness) and non-affected (i.e. without mental illness) groups on one or more attributes, characteristics and exposures, for example, comparing differences in brain volume between those with schizophrenia and those without;
Compared exposed versus non-exposed groups on prevalence of mental illness, for example, comparing rates of mental illness in individuals exposed to physical abuse as a child versus those who were not exposed;
Compared the prevalence of mental illness in a specific population enabling comparisons with that of the general population, for example, determining the prevalence of serious mental disorders in prison populations;
Estimated the correlation between continuous measures of mental illness (e.g. depression symptoms) and individual characteristics or exposures (e.g. self-esteem).
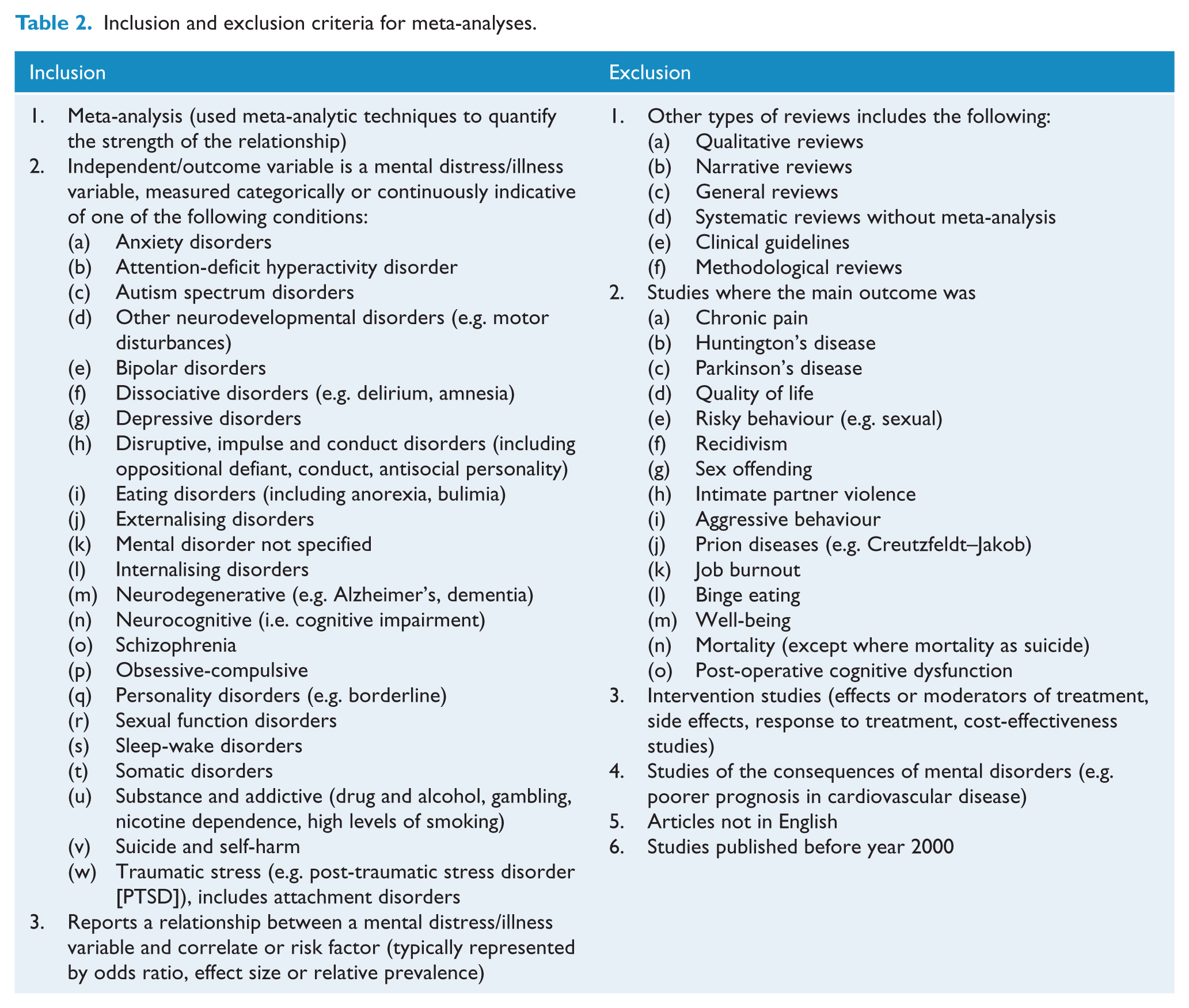
A complete list of the inclusion and exclusion criteria for this review is presented in Table 2.
Inclusion and exclusion criteria for meta-analyses.
Search strategy
Potentially relevant meta-analyses were identified in three ways:
A systematic search of MEDLINE was conducted from 2000 to December 2014, using the MESH terms ‘meta-analysis’ and ‘mental disorder’. The search period was limited in order to reduce the likelihood of repetition and obtaining out-of-date analyses.
A search of Google Scholar, from 2010 to 2015, was conducted using the search terms ‘meta-analysis’ and ‘mental’, ‘psychopathology’, ‘psychiatric’ and other specific risk factor phrases (e.g. genetic, biological, maltreatment, domestic violence, education).
An automatic search was set up in Google Scholar using the terms ‘mental’ and ‘meta-analysis’ to locate emerging papers published from 2015 onwards.
Data collection and management
All references (full reference + abstract) emerging from the search were downloaded into a reference manager. The first author (G.F.) reviewed each abstract; where sufficient information could not be extracted from the abstract or title, G.F. conducted a quick review of the full-text article. No cross-checking by other raters was conducted.
Data extraction and synthesis
Each eligible paper was categorised by disorder and risk factor. The first step involved identifying the mental disorder(s) addressed in the study; these categories aligned with the list of disorders presented in Table 2. The second step involved classifying the key potential risk factors described in the paper.
Because of the significant diversity of potential risks described in the papers, the risk factor categorisation scheme was created and refined by G.F. over successive reviews of the abstracts. This was achieved using the tagging system in the reference manager. G.F. reviewed one abstract at a time and assigned tags to describe the potential risk factors in each paper. Over successive reviews, conceptually similar tags were grouped together into categories, and in consultation with M.L., S.G. and L.S., these categories were further refined. The final categorisation scheme consisted of 10 primary (higher order) categories and 23 secondary (sub) categories, which were approved by all authors. Given that many studies had a wide scope (e.g. multiple disorder, multiple risk factors), it was common for a study to be included in multiple disorder and/or risk factor categories.
After the categorisation scheme was developed, G.F. re-reviewed the abstracts to extract only those potential risk factors where a significant statistical association with a mental health outcome was noted. These factors were recorded in a master list and sorted by primary and secondary categories. There were two exceptions to this: the genetic and neuroanatomical/neurochemical categories, which were not re-reviewed, as it was deemed that interventions modifying genetic or neuroanatomical factors were out-of-scope in the context of current workforce and service planning goals.
A final check of each paper was conducted by G.F. 6 months after developing the categorisation system. This included reviewing each abstract to ensure it was a meta-analysis and that the paper had been appropriately categorised in terms of disorder and potential risk factors. Given the objectives and magnitude of this review, it was neither feasible nor necessary to appraise the quality or risk of bias of included studies.
Results
A total of 3314 studies were identified in the MEDLINE search, of which 1853 were rejected based on the date of publication, title and/or abstract, leaving 1461 eligible studies. An additional 167 studies were added as a result of Google Scholar searches and research alerts. This resulted in a total pool of 1628 eligible studies (Figure 1).
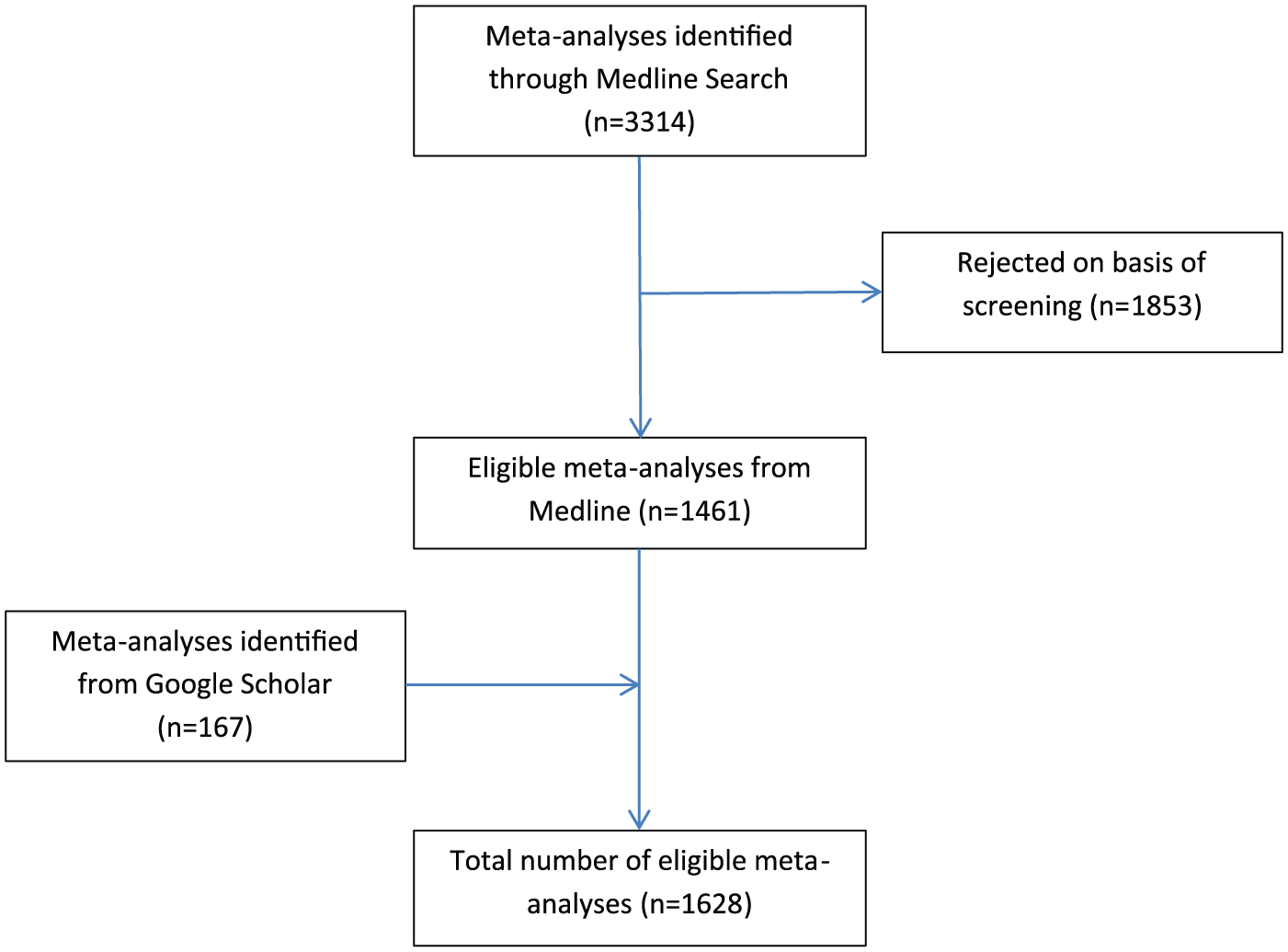
Selection of studies for the review.
Mental disorders
The number of meta-analyses identified by illness is shown in Figure 2. As meta-analyses commonly addressed more than one mental disorder outcome, the sum of studies across disorders is greater than 1628. The greatest number of meta-analyses related to schizophrenia, neurodegenerative (e.g. Alzheimer’s disease, dementia) and depression (n = 907, 46%). There were very few meta-analyses for somatic disorders, sleep–wake disorders and dissociative disorders (n = 25, 1.3%).
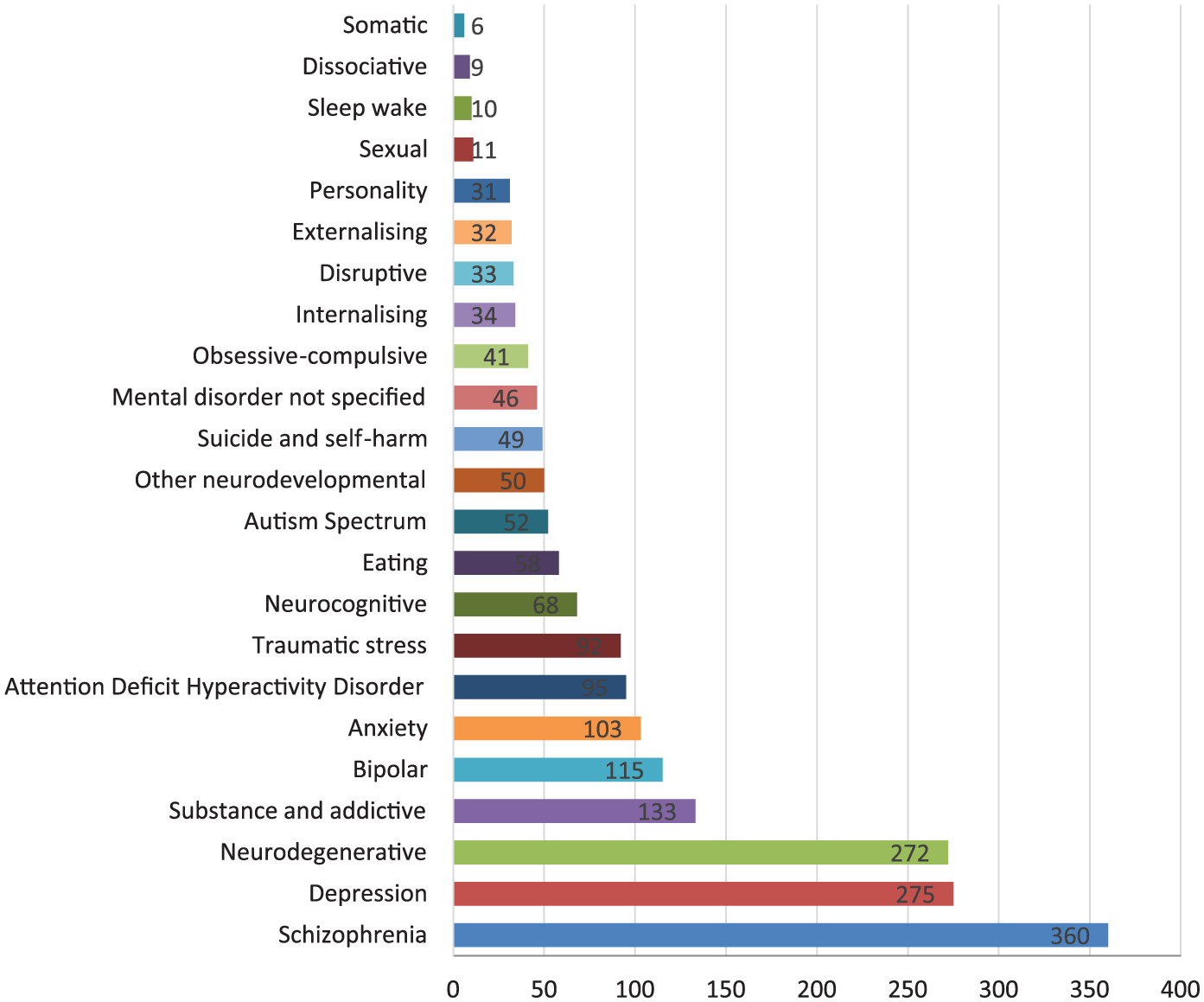
Total number of meta-analyses by mental illness.
Potential risk factors for mental illness
The number of meta-analyses by primary risk category is shown in Figure 3. Meta-analyses of genetic, psychological and physiological factors dominated (n = 1112, 66.5%). Meta-analyses of predictors of response to trauma and negative environmental exposures were relatively few in number (n = 34, 2.0%).
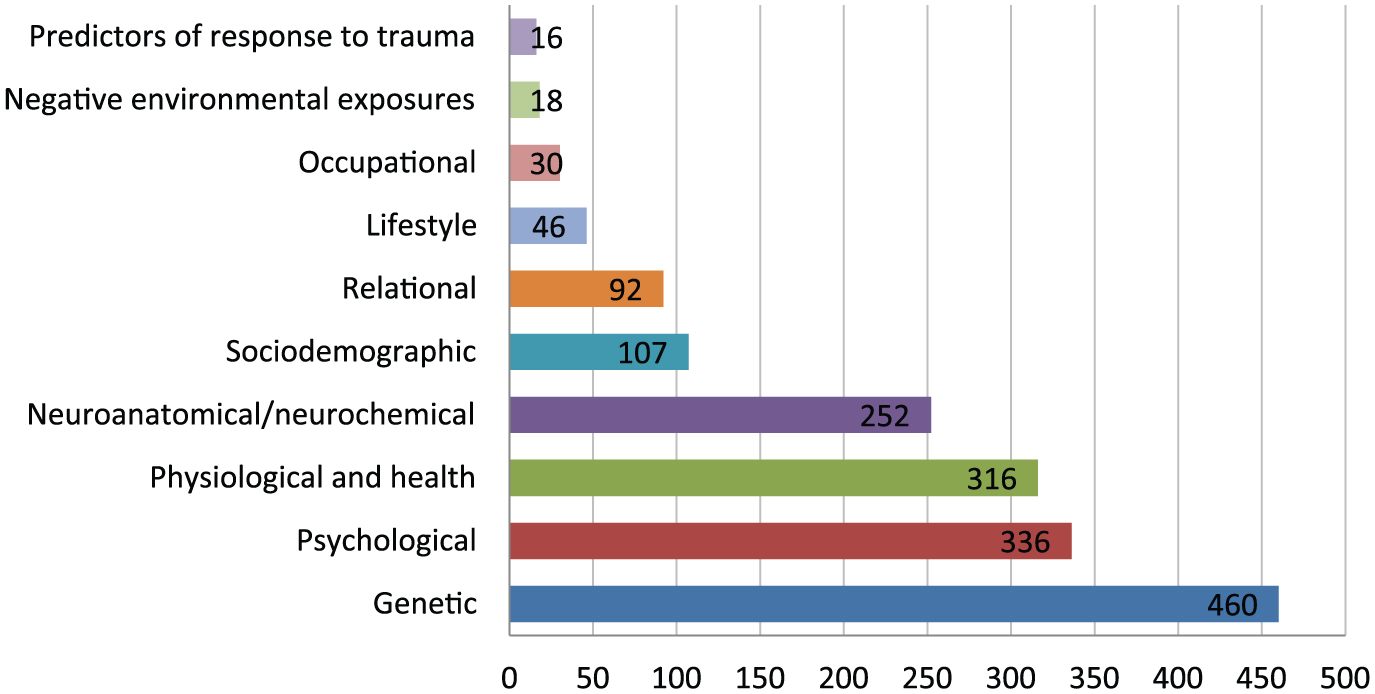
Total number of meta-analyses by primary risk factor category.
The final categorisation scheme with examples of potential risk factors is shown in Table 3. Studies of genetic, psychological, physiological and neuroanatomical factors dominated. While 9 of the 10 primary categories identified factors that distinguished people with and without mental disorders, the ‘Predictors of response to trauma’ category captured factors found to predict whether individuals exposed to traumatic events would go on to develop post-traumatic mental health disorders.
Potential risk factors for mental illness by primary and secondary categories.
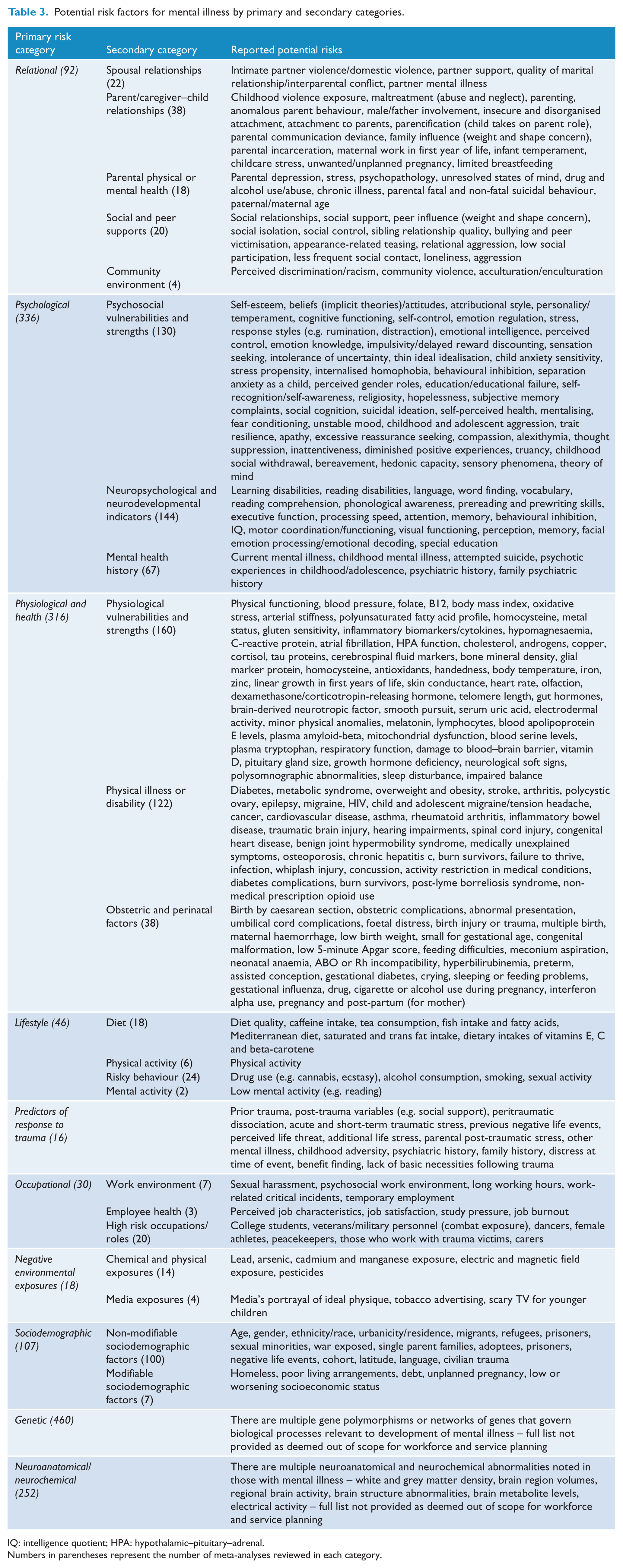
IQ: intelligence quotient; HPA: hypothalamic–pituitary–adrenal.
Numbers in parentheses represent the number of meta-analyses reviewed in each category.
Discussion
This rapid review identified 10 primary and 23 secondary categories of potential risk factors for mental illness. This categorisation scheme highlights the diversity of risk factors for mental illness, and as such, draws attention to the many ways that researchers, clinicians and policymakers might explore and potentially tackle the burden of mental illness. It is also envisaged that this work would encourage research into neglected or emerging sub-categories, such as community environment, mental activity, employee health, work environment and media exposures. As such research emerges, the authors recognise that there may be value in refining or modifying these categorisations.
The findings of this review are consistent with and inclusive of previous reviews. For example, in common with the Institute of Medicine’s (2009) report and the review by Fryers and Brugha (2013), we found evidence of many potential risk factors early in life (ages 0–25 years), including parental mental and physical illness (Goodman et al., 2011; Micco et al., 2009), child abuse and neglect (Lindert et al., 2014; Norman et al., 2012), exposure to domestic violence (Kitzmann et al., 2003), perinatal and obstetric insults (Curran et al., 2015; Su et al., 2014; Xu et al., 2014), bullying (Cunningham et al., 2016; Reijntjes et al., 2010) and mental emotional and behavioural problems in childhood/adolescence (Charach et al., 2011; Clauss and Blackford, 2012; Kossowsky et al., 2013; Sowislo and Orth, 2013). Consistent with the WHO’s ‘risks to mental health’ report (WHO, 2012), we also found evidence of risks across the lifespan, from the impact of early infections (Khandaker et al., 2012) through to negative psychosocial work environments (Nieuwenhuijsen et al., 2010; Stansfeld and Candy, 2006) and the mental health impacts of chronic illness in older adulthood (Dong et al., 2010; Xue-Mei et al., 2010). Finally, there was evidence to support a number of emerging areas of interest in mental illness prevention, particularly the role of lifestyle factors such as diet (Lai et al., 2014; Psaltopoulou et al., 2013; Singh et al., 2014) and physical activity (Aarsland et al., 2010; Gallacher et al., 2012; Sofi et al., 2011).
In the context of the large mental illness prevention workforce and service planning project in which this study was conducted (Furber et al., 2015), the findings highlight and support the idea of mental health being ‘everybody’s business’ (Ford et al., 2007; Mental Health Commission, 2012; Skeen et al., 2010). The list of potential risk factors supports a role for multiple professionals and sectors in mental illness prevention. For example, population and public health practitioners might target lifestyle, environmental exposures or occupational environments; psychologists might target early psychological vulnerabilities; child and family services may focus their efforts on important family relationships; and medical professionals might look to screen for and modify key biomedical risks. In other words, the prevention of mental illness is not just the remit of traditional mental health services.
The relative number of reviews in the different risk factor categories provides an interesting, if potentially imprecise, indicator of the volume of research in different areas, with biomedical factors (e.g. genetics, neuroanatomical and physiological) dominating over social, relational, occupational, environmental and lifestyle factors. The volume of literature, however, is not necessarily an indicator of the current value of those areas of research to prevention planning. For example, we would argue that the smaller body of literature on relational risks has considerable importance; that is, it far outweighs the much larger genetic literature in terms of providing guidance on preventive services, specifically family-based interventions targeting key early childhood adversity (Shonkoff et al., 2012).
The methodology used for this rapid review has some limitations. First, by using meta-analyses, we were limited to illness-factor relationships that have been subject to meta-analytic scrutiny. While the coverage of risks appeared comprehensive, there were areas that were almost entirely missing. For example, we found no literature on First Nations Peoples (e.g. Aboriginal and Torres Strait Islanders in Australia) or on newer research directions, like the relationship between maternal diet and infant development (Zeisel, 2009).
Second, the decision to roll all mental illnesses together for this review means that detail regarding the risks pertinent to specific disorders is lost. Specifically, it is not possible from Table 3 to discern what risk factors are relevant to which disorders. Notwithstanding, this limitation should be considered in light of the goals and target audience of the review: that is, we set out to develop an evidence-based categorisation scheme (taxonomy) for mental illness risk factors that researchers and policymakers could use as a guide for talking about prevention opportunities – one that is significantly more detailed than existing categorisation systems and can accommodate risk factors for a diverse range of mental illnesses. In this context, a broad scope was appropriate.
Third, in identifying, categorising and reviewing the studies, we relied on a single rater (G.F.) who used mostly abstracts to code the studies. The rater did double code 6 months apart, reducing risk of unchecked errors at the level of study inclusion, study categorisation or potential risk factor identification. Where the rater was uncertain, conversations were held with other authors. Ongoing work in this space may help to revise or refine the categorisation scheme.
Fourth, we did not code or sort meta-analyses in terms of the type of studies included (e.g. cross-sectional or longitudinal), quality of contained studies, risk of bias or strength of illness–risk relationship (e.g. effect sizes). Our intention was to focus broadly on what factors have been studied (and found significant), versus detailed analyses of the findings for each factor. As such, we are unable to make definitive statements about where the factors in Table 3 sit on the levels of risk described in Table 1, and the factors listed should be considered as potential risk factors until further validation. Related to this, a valuable exercise would be to draw upon additional literature to classify each of the identified potential risk factors as correlates, risk factors, variable risk factors or causal risk factors – in other words, determine how many of the identified factors are genuine modifiable antecedents of illness versus symptomatic manifestations of existing illness.
With regard to the categorisation system itself, it is acknowledged that there is room for further development. Some of the categories (e.g. genetic, physiological and psychological) are themselves worthy of further scoping given the complexity of this body of literature. Additionally, there is work to be done in separating out risk factors on a disorder-by-disorder basis and placing risk factors along the life-course.
Another interesting extension of this work would be to repeat the categorisation process for factors associated with protection from mental illness and positive mental health (e.g. positive coping style). Such a study would have to focus on original studies as well as meta-analyses given the dearth of research on protective factors, compared to risk factors. To some extent, protective factors are being picked up in this study. Although the language of risk used in this paper implies an absence of protective factors, many potential risk factors identified in this process actually represent a spectrum of functioning from risk to protective. Diet, for example, can be a risk, when it has low nutritional density, or protective, when nutritional density is optimal. Similarly, parenting can be protective when responsive to a child’s needs or damaging when responses are hostile or punitive (e.g. abuse, neglect). However, it is likely that a number of protective factors are missing from this study, thus highlighting additional avenues for mental health promotion that would complement the current risk-focused approach.
Conclusion
A diverse range of factors influence mental health from genetic and biomedical to psychological and sociocultural. Developing a more detailed taxonomy of risk factors for mental illness is a key step in highlighting where clinicians, researchers and policymakers can focus their preventive efforts, as well as highlighting that the prevention of mental illness is a multi-sectoral challenge. The method of using meta-analyses to identify potential risk factors was strong in terms of scope but limited in terms of distinguishing correlates from causal risk factors. Future work should seek to apply additional criteria to these potential risk factors to identify those most relevant to current prevention activities.
Footnotes
Acknowledgements
The authors would like to acknowledge Professor Patrick McGorry, Professor Nicholas Procter, Associate Professor Felice Jacka, Catherine Turnbull and Stephanie Miller for their contributions to the broader Mental Health Workforce Project in which this work was completed.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an NHMRC Partnership Grant (APP1055351)
Supplementary materials
Readers are welcome to contact the primary author (Dr Gareth Furber) to access the database of studies used in this paper.