
Abstract
Objective:
To estimate the prevalence of children in the Australian population with risk factors for adult mental illness.
Method:
Key risk factors and risk domains were identified from a 2013 review of longitudinal studies on child and adolescent determinants of adult mental illness. Data items were identified from the Longitudinal Study of Australian Children that map onto the risk domains and were used to estimate the prevalence of these key individual risk factors and the magnitude of multiple risk in children aged 3 months to 13 years.
Results:
Even by infancy, risk factors for adult mental illness are highly prevalent, with 51.7% of infants having multiple risks. In 10 infants, 1 was born to mothers who consumed daily alcohol and 1 in 8 to mothers who smoked cigarettes daily during pregnancy. Also, 10.5% of infants were in families where the parents had separated, which increased to 18% in 10–11 year-olds. Psychological problems in the clinical range (based on the Strengths and Difficulties Questionnaire total problems score) ranged from 7.8% to 9.7% across the 4–13 years age range. Risks from negative parenting behaviours were highly prevalent across age groups. Two-thirds of children aged 12–13 years had parents who displayed low warmth or exhibited high hostility/anger. Across childhood, one in seven children are in families exposed to 3+ major life stressors. By age 8–9 years, more than 18% of children are exposed to ⩾5 risk factors.
Conclusions:
We find that modifiable risk factors for adult mental illness occur at the earliest stage in the life course and at greater prevalence than is commonly recognised. Considerable capacity will be required in child and adolescent mental health services and complementary family support programmes if risk factors for adult mental illness that are already apparent in infancy and childhood are to be addressed.
Introduction
Mental illness and behavioural disorders are the leading cause of years lived with disability (YLD) worldwide (Jacobi et al., 2004; Phillips et al., 2009; Whiteford et al., 2013; Wittchen et al., 2011), and in Australia account for 22.3% of YLD, second only to musculoskeletal disorders (Institute of Health Metrics and Evaluation, 2015). An estimated one in five Australians experience mental illness in a 12-month period and an estimated 45% of the population suffer a mental illness sometime in their lifetime (Australian Bureau of Statistics [ABS], 2007). Given the large burden associated with mental disorders, it is particularly concerning that children and young people are disproportionately affected. For example, youth aged 16–24 years have the highest 12-month prevalence of mental illness at 26.0%.
The mental health community in Australia and internationally has called for prevention and early intervention to play a more central role in the delivery of mental healthcare (Furber et al., 2015; Jacka and Reavley, 2014; McGorry et al., 2007; World Health Organization, 2004). There has been some progress in this regard with the roll out of 85 Headspace Centres across Australia. The aim of Headspace is to encourage young people aged 12–25 years who are concerned about their mental health to seek help and to provide integrated primary care services to improve mental and social well-being (McGorry, 2007). In 2012, Headspace Centres provided services to 39,718 young people (headspace National Youth Mental Health Foundation, 2013) and early signs are that they are having a moderate impact in terms of reducing psychological distress and improving psychosocial functioning (Muir et al., 2009; Rickwood et al., 2014, 2015).
While these services are much needed, limiting access to young people aged 12 years and older means that a significant vulnerable population is still being overlooked. Based on the second Australian Child and Adolescent Survey of Mental Health and Wellbeing (Lawrence et al., 2015), it is estimated that 13.6% of 4- to 11-year-olds (N = 6310) experience a diagnosable mental disorder in a 12-month period. These figures indicate that mental illness is established well before adolescence and suggest that preventive interventions should target risk factors in the earliest life stage. Moreover, improved understanding of early brain development as a result of advances in neurobiological and developmental sciences underscores the role of addressing antecedents of mental illness in childhood in reducing the incidence of adult mental illness.
Importance of the early years in the prevention of mental illness
A large component of mental illness is understood as emerging from multiple cumulative and interactive effects of negative exposures that occur over the life course (Institute of Medicine, 2009; National Scientific Council on the Developing Child, 2007). It is now established that there are particularly sensitive periods of brain development during the early years of life, defined as the antenatal period to five years of age (National Scientific Council on the Developing Child, 2007; Sawyer et al., 2014). In this crucial early period, brain circuitry associated with a child’s future social, emotional and cognitive capacities is largely established, providing the foundation for functioning through the life course. There is also accumulating evidence that genes and environments are involved in ongoing interactions and that certain environmental exposures set in motion particular genetic propensities (Shonkoff et al., 2012). Other research based on ethology (the study of animal behaviours) and evolutionary theory elucidates the mechanisms whereby relational trauma disrupts development of a differentiated sense of self, potentiates shame and other constructs associated with poor mental well-being (Amos et al., 2014). Theory demonstrates how exposure to traumatic events in early childhood, such as child maltreatment can have life-long ramifications on social, emotional and cognitive well-being.
Empirical studies confirm the relationship between childhood trauma and poor mental well-being. The adverse childhood experiences (ACE) study has been particularly influential in demonstrating poor physical and mental health outcomes associated with early life adversity (Anda et al., 2006; Chapman et al., 2004; Dube et al., 2001). This accumulated knowledge provides a strong justification for intervening as early as possible in a child’s life. It has prompted widespread calls among the early childhood research and policy community to improve the quality of early life, primarily family environments (Moore and McDonald, 2013; Price-Robertson et al., 2010; Sawyer et al., 2014; Shonkoff, 2011), and address emerging mental health concerns in children in the context of a mental health preventive agenda (Furber et al., 2015; Jacka and Reavley, 2014).
The aim of this study is to advance the prevention agenda by describing the prevalence of key childhood antecedents to youth and adult mental illness. It takes a set of risk factors developed through extensive review of the literature by Fryers and Brugha (2013) that describe the childhood determinants of mental illness and applies it to the Australian population to estimate prevalence of risk. To our knowledge, this is the only research to estimate prevalence of risk for adult mental illness in Australian children. We note similarity with the work of Gubhaju et al. (2013) who used the Longitudinal Study of Australian Children (LSAC) data to develop an index of adversity to measure multiple disadvantages in Australian families. While there is overlap in the risk factors included in the two studies, our focus differs in that we use an established set of risk factors to estimate prevalence of risk specifically for adult mental illness. The scope is also limited to a crucial age group for prevention of mental illness: children aged 3 months to 13 years. These results will inform policy-makers of the number of children in Australia who likely require services to reduce their risk of developing adult mental illness.
Method
Selecting critical childhood determinants of adult mental illness
The literature on childhood determinants of adult mental illness is vast. However, there are few reviews that are comprehensive in terms of scope of risk factors and mental health conditions covered and also attempt to bring this literature together in a meaningful way (Institute of Medicine, 2009; World Health Organization, 2004), reflecting the inherent challenges of such a task. The paper by Fryers and Brugha (2013) provides the most comprehensive review and analysis of childhood determinants of mental illness that we could find. They identified, from a qualitative analysis of 450 longitudinal, primarily birth cohort studies, 10 risk domains present in childhood and adolescence that are strongly associated with negative mental health outcomes in adulthood. These domains represent opportunities for intervention across the mental health intervention spectrum (Institute of Medicine, 2009) from promotion (parenting courses) to after-care (suicide attempt by a young person).
The risk domains defined by Fryers and Brugha (2013) are listed below. We have for some categories modified the terminology and descriptors to enhance clarity and distinction between categories:
Psychological disturbances in childhood and adolescence – e.g. early symptoms of mental illness;
Genetic influences;
Neurological vulnerability in childhood – e.g. brain damage or disorder, birth complications, low intelligence and developmental delay;
Disturbed behaviours in childhood and adolescence – e.g. hyperactivity, conduct problems and bullying;
Features of personality – e.g. neuroticism or low self-esteem;
Poor school performance, poor educational achievement;
Childhood/family adversity, life events, multiple disadvantages – e.g. physical illness, extreme poverty and parental incarceration;
Child maltreatment – e.g. physical abuse, sexual abuse, neglect and witnessing domestic violence;
Parenting, parent–child relationships and parent psychological disturbance – e.g. harsh discipline;
Disrupted families – e.g. divorce and separation, parental substance misuse and family conflict.
Fryers and Brugha’s (2013) review found that some relationships are particularly well-established. For example, mental disturbance in childhood is strongly predictive of poor mental health in adolescence and mental illness in adulthood, and child abuse and neglect are potent predictors of adult mental health outcomes. In addition to attributes within the 10 listed domains being potent individual predictors, they also found significant evidence of accumulation of risk, namely that the risk of mental illness increases with the number of risk exposures. Given the recency and scope of this review, we used Fryers and Brugha’s (2013) results to inform our understanding of the priority risk factors for preventing mental illness.
To translate the domains into data items for which prevalence could be established, we cross-referenced the risks covered under nine domains described in the Fryers and Brugha’s paper with pertinent data items from the LSAC. The genetics domain is excluded given the prevention focus of this work. By limiting the analysis to a single data set, we could also construct a multiple risk index to estimate the number of children exposed to multiple risks. Since LSAC covers such a broad range of data items, it was feasible to develop prevalence estimates for adult mental illness using this single study.
LSAC
Starting in 2003, LSAC is an Australian-wide longitudinal study that aims to examine a broad range of policy-relevant questions about Australian children’s development and well-being. It involves a two age cohort cross-sequential design (Sanson et al., 2002). The ‘birth’ cohort included 5701 infants aged 3–19 months and the ‘kindergarten’ cohort included 4939 children aged 4–5 years – a total of 10,640 participants. Participants were selected from the Medicare database, which has 98% coverage of all children less than 12 months of age, according to a cluster sample design based on postcodes (Soloff et al., 2003). Postcodes were stratified by every state or territory and by capital city statistical division versus rest of state, with remote areas excluded from the study. Postcodes and children within postcodes were selected randomly. A detailed account of the LSAC study design is reported in Soloff et al. (2003).
The survey collects data from parents, children and teachers or other care providers every 2 years and is currently in its sixth wave. The most recent wave for which data were available for analysis was the fifth wave, where the oldest children were aged 12–13 years. Using the five waves and the two cohorts of LSAC, it was possible to estimate prevalence of risk factors for adult mental illness across seven age groups: 0–1 year, 2–3 years, 4–5 years, 6–7 years, 8–9 years, 10–11 years and 12–13 years.
Data items
LSAC measures an enormous range of constructs related to child well-being. Data items representing the risk factors in Fryers and Brugha’s (2013) paper were identified using two main approaches: (a) scanning the LSAC data dictionary for relevant items, taking each domain separately and (b) reviewing the LSAC literature to find examples of items used in previous studies (e.g. Bayer et al., 2011; Forrest and Edwards, 2015). When there were more than one data item that could be used to represent a risk factor, we looked to see what had been used in previous research. For example, there are several variables in the LSAC data sets concerning children’s experiences of, attitudes to and performance at school, and it was not immediately clear which were the best measures of school performance. A search for LSAC literature on school performance indicated that the ‘academic rating’ and ‘approach to learning’ scales were well used measures of school performance (Harrison et al., 2009).
Definition of risk
Most data items were derived from parent-reported questionnaires with one item reported by children and three by their teachers (literacy skills, maths skills and approach to learning). Some questionnaires had validated scoring protocols to identify children who were likely in the clinical range and in need of clinical services. In these cases, the recommended cut-off scores were used to determine presence or absence of risk. Otherwise, risk thresholds were defined by selecting a point on the response scale corresponding to frequent risk exposure and calculating the proportion of children who scored above or below this point. For example, the bullying questionnaire included five items describing different types of bullying and asked respondents to indicate how often each type occurred in the previous month on a scale of 1 = Not at all, 2 = Once or twice, 3 = About once a week and 4 = Several times a week. The threshold value was set at two, so that any child whose mean score across the five items was equal to or greater than two was considered ‘at-risk’ and would be counted as having bullying present.
Other variables had categorical response options, which logically translated into risk present or not. For example, a question regarding family drug and alcohol problems elicited a response of ‘yes’ or ‘no’ to indicate the presence or absence of these problems in the preceding year. See Table 1 below for the mapping of domains onto data items and selection of risk definitions for each data item.
Key risk domains identified by Fryers and Brugha (2013) and risk factors with description of LSAC variables and risk definitions used to estimate risk prevalence.

LSAC: Longitudinal Study of Australian Children; SEIFA: Socio-Economic Indexes for Areas; SES: socio-economic status.
5-item measure used at age 12–13 years.
There were no specific questions on child maltreatment in LSAC. We include one item from the ‘Argumentative relationship scale’ that assessed violent couple behaviour. Measures of parenting warmth and hostile/angry parenting can be considered as proxy measures of maltreatment but are included under the parenting/parent–child relationship domain.
The parental warmth distribution was skewed so that scores congregated around the high end of the response scale (i.e. 4 = ‘Often’ and 5 = ‘Always/almost always’. The original risk threshold was set at <4, however, this meant that by the time children were 12–13 years, ⩾50% were at-risk from low parental warmth. Adjusting the threshold to <3 was also unsatisfactory because it excluded almost all of the population (>98.5% across first three age groups). Thus, it was decided to apply a threshold value of 3.5, which produced estimates between the two extremes.
Except at 4–5 years and 6–7 years where only measured in birth cohort.
Data analyses
LSAC provides data from each wave and cohort in separate data files. Before conducting any data analysis, we combined cohorts on waves where children were of the same age. For example, in the first wave of the kindergarten cohort, children were aged 4–5 years and so were the children of the birth cohort in the third wave. Thus, these data files were collated so that all data on children aged 4–5 years were in a single data file. This resulted in seven separate data files containing data for the following age groups: 0–1 year, 2–3 years, 4–5 years, 6–7 years, 8–9 years, 10–11 years, and 12–13 years. Prevalence estimates were calculated separately for each age group so that in effect, the separate waves were treated as separate cohorts.
Individual risk factor prevalence
Each risk factor was rescored as a binary variable indicating either the presence (1) or absence (0) of risk. Prevalence was then estimated at each age group by calculating the percentage of children at each age for whom the risk factor was present. The process was repeated for each risk factor listed in Table 2 and across the seven age groups. Raw estimates were adjusted to derive Australian population estimates using cross-sectional population weights constructed by the LSAC team, which account for under-represented demographics (e.g. language other than English spoken at home) and sample attrition (Cusack and Defina, 2013).
Prevalence (%) of children across ages 0–13 years with defined risk factors for adult mental illness.
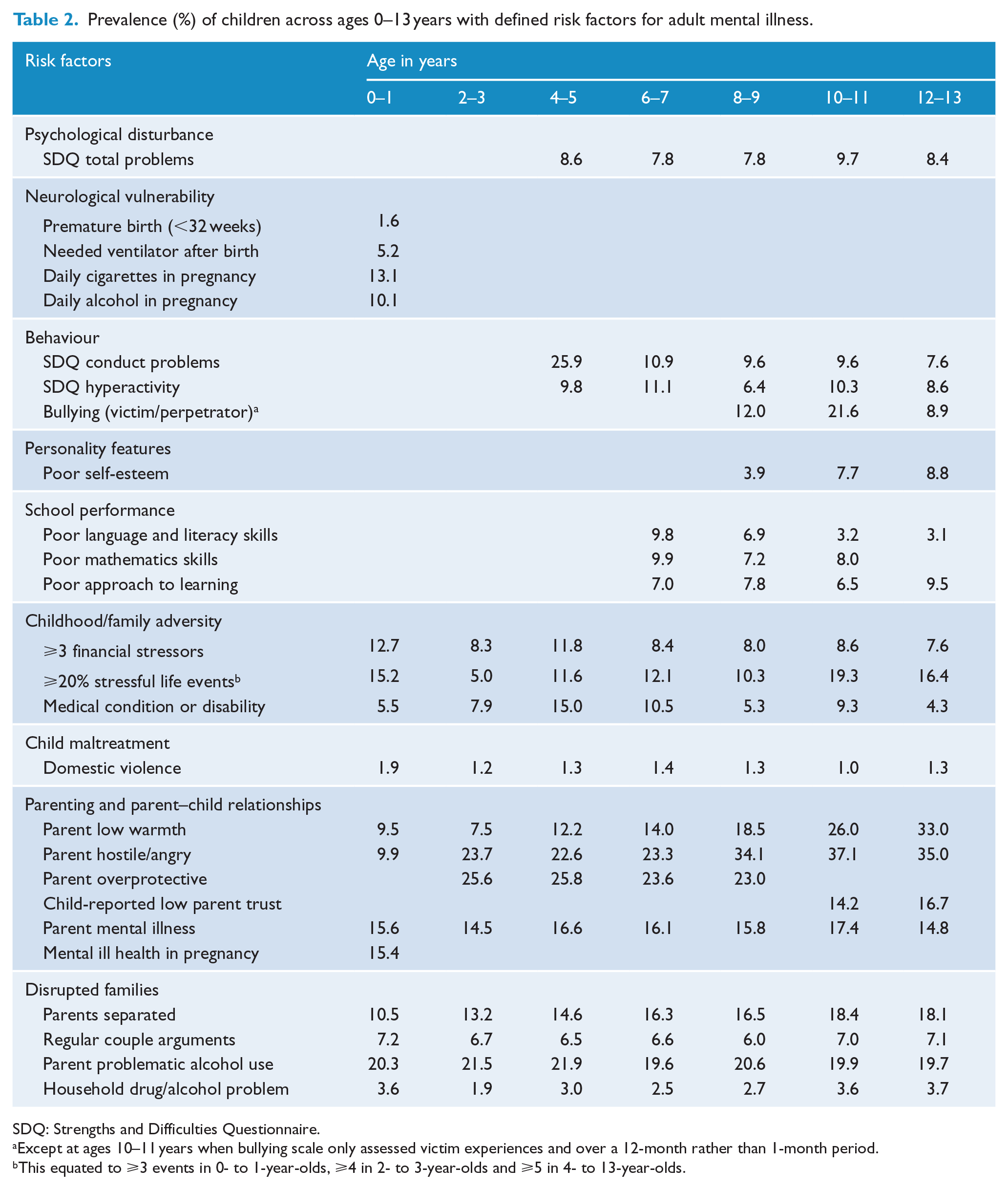
SDQ: Strengths and Difficulties Questionnaire.
Except at ages 10–11 years when bullying scale only assessed victim experiences and over a 12-month rather than 1-month period.
This equated to ⩾3 events in 0- to 1-year-olds, ⩾4 in 2- to 3-year-olds and ⩾5 in 4- to 13-year-olds.
Where two respondents provided data (e.g. two parents on problematic alcohol use, hostile parenting), children were considered ‘at-risk’ where at least one respondent’s score was over the risk threshold. If data were missing on a variable for one respondent, data from the other respondent were used where available.
Through this process, prevalence of established risk factors for mental illness was estimated for 15–23 attributes, the number varying by age group.
Missing data
On each risk factor item, all available data were used to calculate prevalence. Missing data were not imputed. Each prevalence estimate is calculated as the number meeting the risk cut-off divided by the total number of cases, which included those who did not report on that item, i.e., cases with missing data. This approach makes no assumptions about the risk status of children with missing data and results in underestimation of risk, the size of which will vary across variables depending on the amount of missing data.
Multiple risk prevalence
There are different possible approaches for calculating multiple risks and each has its merits and shortcomings (Evans et al., 2013). We decided to adopt the simpler of these approaches, consistent with the extensively published and well-known ACE study (Dube et al., 2001), which is to count and sum the presence of individual risk factors for each child. For example, a child who was born prematurely to a father who engages in risky alcohol use and a mother who scores low on warmth (and nothing else in the at-risk range) would attract a multiple risk score of three.
The multiple risk index was constructed using the ‘count’ function in SPSS. This command allows the user to specify a list of variables and a specific value to be counted within each variable. As the individual risk factors were scored as either 0 or 1, the command was set to count ‘1’ values across each child in the data set. The final score indicated the total number of risk factors present for each child. This process was repeated across each of the seven age groups. Cases were excluded where there were missing data on ⩾10 variables. Applying this criterion resulted in the percentage of missing data ranging from 0.04% to 6.8% across the age groups.
Results
Certain variables had greater rates of missing data than others and rates varied across waves. Variables with the highest rates (ranging from 10% to 25%) were those associated with parent drug and alcohol use, parents’ relationship, parenting, teacher-reported academic performance and the developmental outcome index. Children with missing data were compared to children without missing data on the SDQ total problems scale. This showed that children with missing data had greater levels of psychological disturbance than those without, suggesting that prevalence estimates associated with these variables are likely to be underestimates.
Table 2 shows the estimated prevalence of individual risk factors for adult mental illness across children aged 6–7 year-olds. Prevalence estimates varied from 1.0% of children aged 10–11 year-olds with parents who indicated domestic violence occurred between them up to 37.1% of children aged 10–11 year-olds who have at least one parent who expresses high levels of hostility/anger.
At the earliest age, risk factors for adult mental illness are highly prevalent. The prevalence of infants whose mothers smoke or drank alcohol every day for at least one trimester during pregnancy is greater than 10% and 10% of infants are in single parent households. One in eight infants was in families which experienced ⩾3 financial stressors and the same number was using prescribed medication.
Risk from negative parenting behaviours was highly prevalent across all age groups. Beyond infancy, greater than one in five children experienced hostile/angry parenting or overprotective parenting. Prevalence of children with parents low on warmth was as high as one in three by the time they were 12–13 years.
Risk from psychological disturbance as measured by the SDQ total problems scale ranged from a minimum of 7.8% among 6- to 7-year-olds to 9.7% among 10- to 11-year-olds. A quarter of Australian children were found to have parent-reported conduct problems when first assessed at age 4–5 years; however, this prevalence halves once they are in school. Hyperactivity is most prevalent (11.1%) when children are 6–7 years.
Prevalence of certain risks increased across the age groups, notably single parent households, parental low warmth and, parental hostility/anger. By the time they were 12–13 years, 18% were in single parent households, 33% experienced parenting characterised by low warmth and, 35% experienced frequent hostile/angry parenting. Although fewer data points are available, risk from low self-esteem and poor approach to learning also appear to increase across the age groups.
Prevalence of children with multiple risk factors for adult mental illness
Studies of risk factors associated with mental illness show that the likelihood of an individual developing mental illness increases as the number of risk factors experienced increases (Chapman et al., 2004; Dube et al., 2001; Prelow and Loukas, 2003; Roberts et al., 2009). We thus estimated the multiple risk profile for the Australian population.
Table 3 shows the results of the multiple risk analysis. At ages 0–1 year, 78.5% of children have ⩾1 risk factor and 8.1% have ⩾5 risk factors. By the time children are 12–13 years, 86.9% have ⩾1 risk factor and 18.0% have ⩾5 risks. Children aged 10–11 years had the greatest severity of risk for adult mental illness. Among this group, 26.6% have 3–4 risk factors and 21.1% have ⩾5 risk factors. Multiple risks appear at the youngest age, however, with 29.8% infants having ⩾3 risk factors for adult mental illness.
Prevalence (%) of children by number of risk factors for adult mental illness by age group.
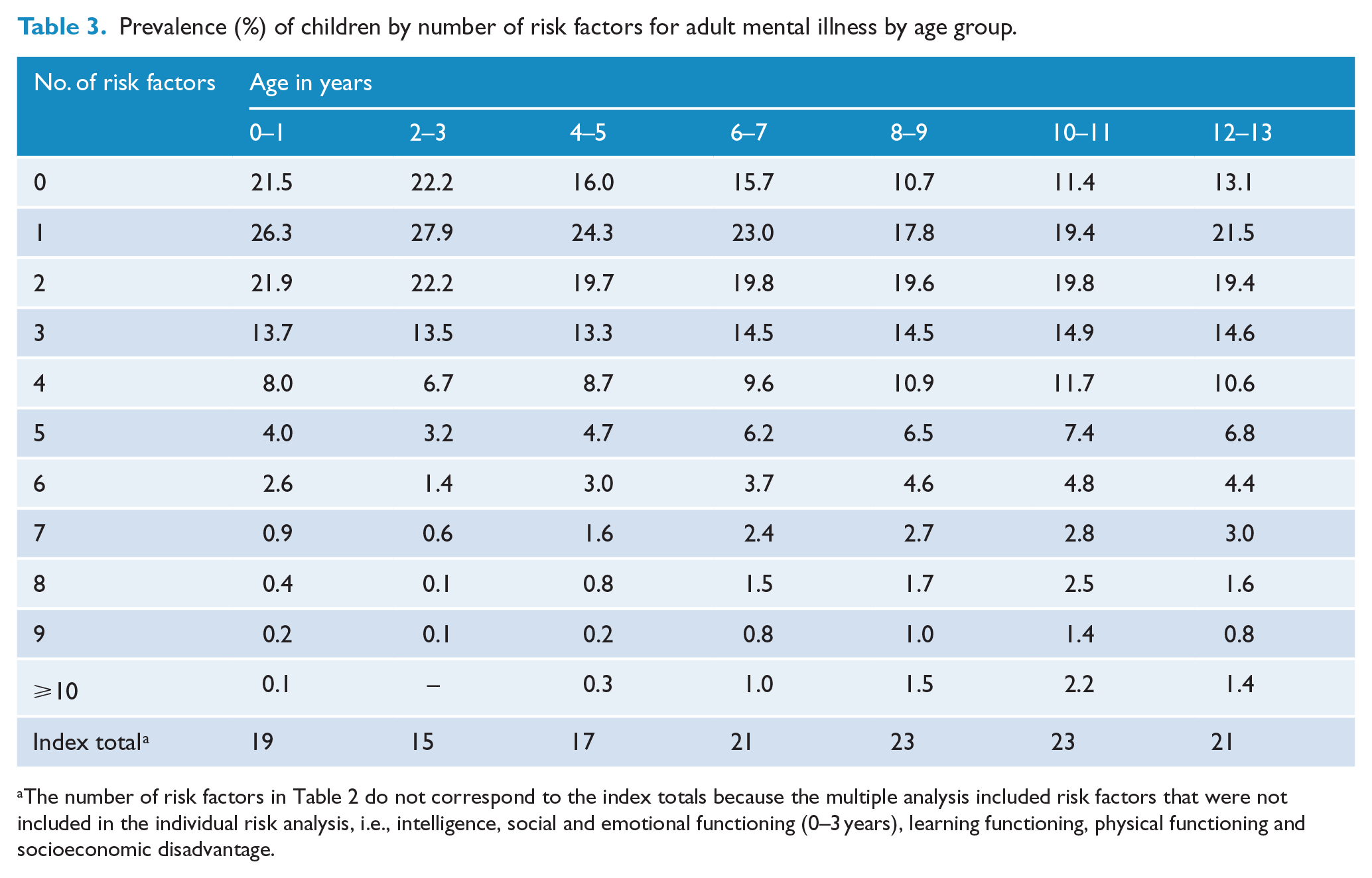
The number of risk factors in Table 2 do not correspond to the index totals because the multiple analysis included risk factors that were not included in the individual risk analysis, i.e., intelligence, social and emotional functioning (0–3 years), learning functioning, physical functioning and socioeconomic disadvantage.
Results of the multiple risk analyses are also presented in graph format (Figure 1). The prevalence of children with multiple risks increased as additional risk factors were added to the index. At ages 4–5 years, the increase in children with ⩾4 risks coincides with the inclusion of the SDQ emotional and behavioural symptoms scales. The second increase at approximately 8–9 years coincides with assessment of the learning and cognitive risk factors (i.e. language and literacy skills, intelligence) as well as bullying and self-esteem.
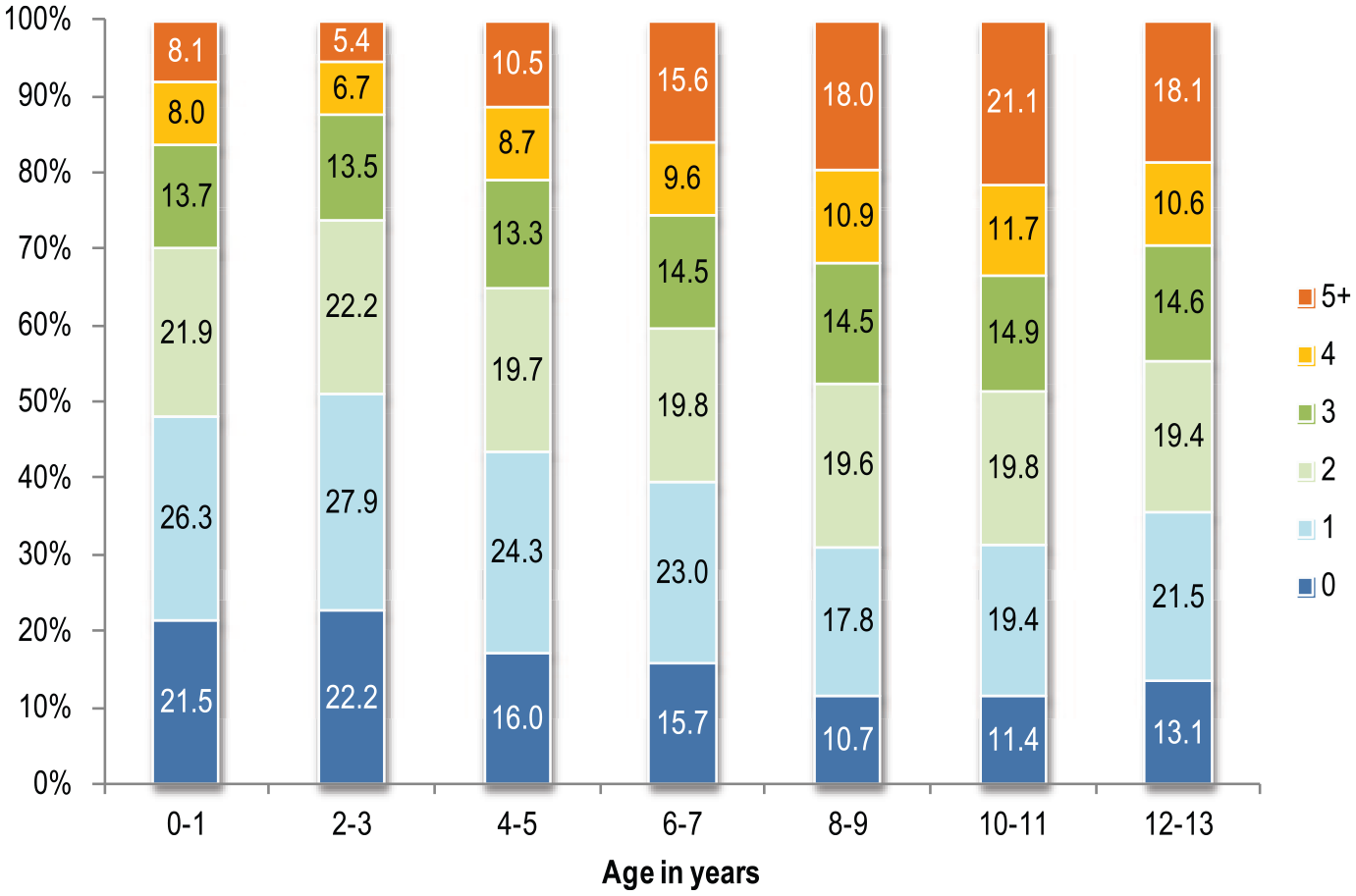
Prevalence of children aged 0–13 years with multiple risk factors for adult mental illness.
We compared children aged 10–11 years to investigate the most prevalent risks at lower and higher levels of multiple risks (Figure 2). Among high risk children, i.e. those with ⩾5 risk factors, the three most prevalent risk factors were parent anger (68.3%), bullying (45.5%) and low parent warmth (43.6%). In contrast, the three most prevalent risk factors among low risk children (⩽2 risk factors) were parental anger (18.7%), parental low warmth (14.9%) and parent problematic alcohol use (13.6%).
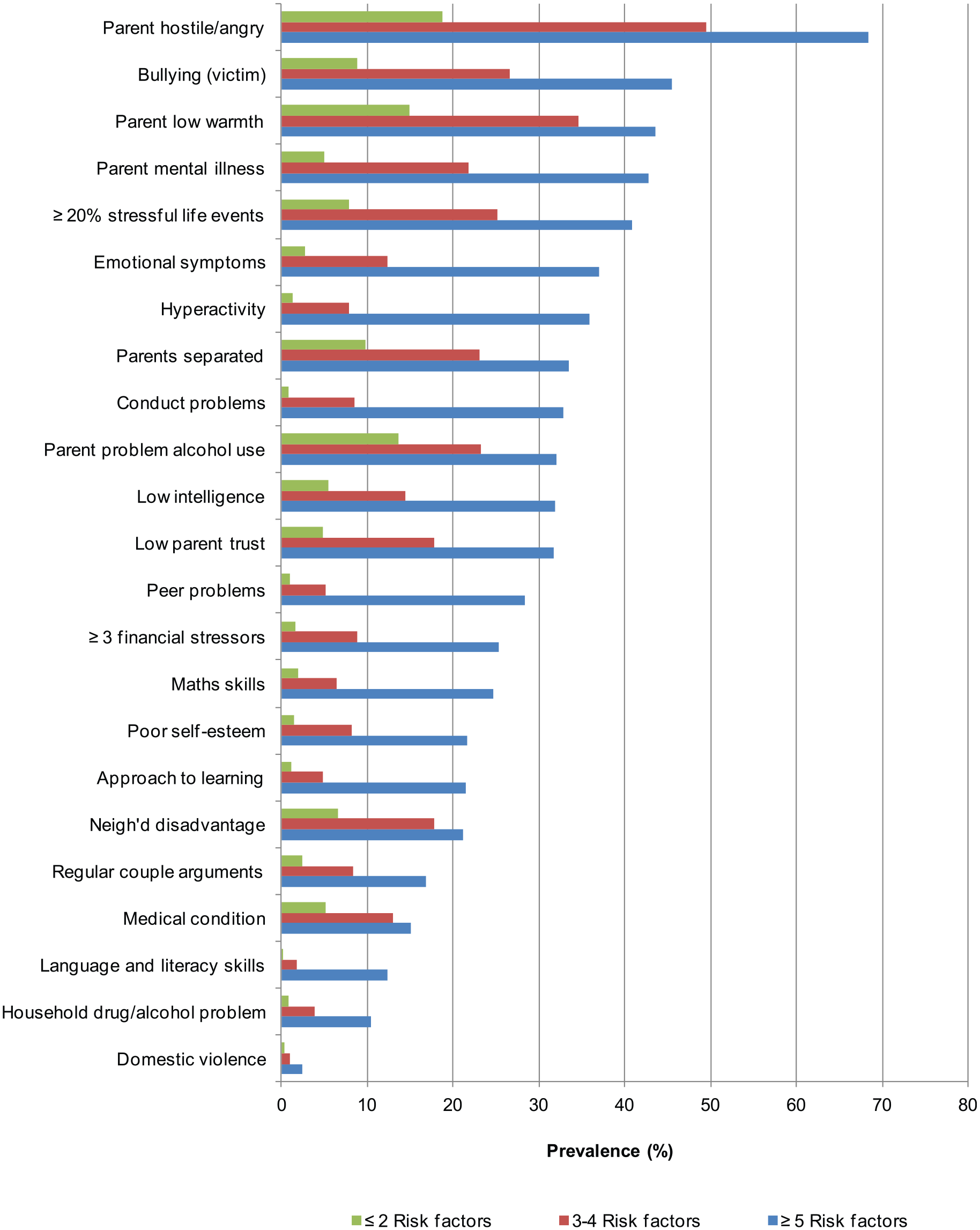
Prevalence of risk factors among 10–11 year-olds at different levels of multiple risks.
Certain risk factors were almost exclusively found in the context of multiple risk factors or at far higher rates. For example, poor language and literacy skills appeared in 12.3% of children with ⩾5 risk factors but <0.05% of children with ⩽2. Conduct problems were reported in 32.8% of children with ⩾5 risk factors but <1% of children with ⩽2 risk factors. Hyperactivity problems showed a similar pattern. Other risk factors were relatively common among all children along the multiple risk spectrum. These included parent problematic alcohol use (32.0% in children with ⩾5 risk factors vs 13.6% in children with ⩽2), parental low warmth (43.6% vs 14.9%) and medical condition/disability (15.1% vs 5.1%).
Discussion
This study describes the prevalence of key risk factors for adult mental illness among children aged 0–13 years. It builds on the work of Fryers and Brugha (2013) who synthesised the vast literature on childhood determinants of mental disorders to propose a set of 10 risk domains. Cross-referencing these domains with data from the LSAC yielded a set of 29 individual risk factors that were used to assess the extent of childhood risk for adult mental illness in Australia.
Across the number and breadth of individual risk factors, three key results stood out. First, risk factors for adult mental illness are already highly prevalent among infants (0–1 year). Second, the prevalence of children with multiple risks appeared to increase with age up to age 8–9 years and then plateau at a high of 18% of children ⩾5 risk factors. The closest precursors of adult mental illness, notably the SDQ conduct problems score and hyperactivity problems score were almost exclusively found in children with multiple risk issues. Third, negative parenting behaviours were among the most prevalent risks and common among all children regardless of where they were positioned on the multiple risk spectrum.
The three most prevalent risks among infants were parent problematic alcohol use, parent mental illness and mental ill-health during pregnancy. When multiple risks were assessed, it showed that 52.5% of 0-1 year-olds had ⩾2 risk factors and 8.1% had ⩾5 risk factors. The proportion of children with ⩾5 risk factors increased from 5.4–8.1% of 0-3 year-olds to 18.0–21.4% of 8–13 year-olds (18.1% of 12–13 year-olds). Some of this increase may reflect in small part differences in the number of risk factors assessed, varying from 15 in 2–3 year-olds to 23 in 8–11 year-olds. But it will also reflect a likely accumulation of risks over time, in part as a consequence of early adversity. It points to a large minority of children, increasing from infancy to middle childhood, at serious risk of adult mental illness.
Given the strong evidence of the compounding effect of multiple risks (Chapman et al., 2004), within a preventive mental healthcare model, children with ⩾3 risk factors would ideally have their mental health status assessed. A child with ⩾5 risks would likely require intervention by a mental health practitioner. With 1 in 12 infants having ⩾5 risk factors for adult mental illness, it is clear that services to support infant mental health within the family context are needed by a considerable proportion of the population.
Risk from negative parenting behaviours is highly prevalent in Australian families. Between 23% and 37% of children aged 2–13 years were regularly exposed to hostile/angry parenting and approximately 25% of 4–12 year-olds to overprotective parenting. Low parental warmth increased across the age groups so that by the time children were 12–13 years, one in three experienced parenting characterised by low warmth. The additional analysis of 10–11 year-olds with different levels of multiple risks showed that negative parenting behaviours were common at low and high ends of the multiple risk spectrum.
Limitations
In this study, risk measurement was limited to the set of variables available in the LSAC data set. Only some of the instruments included validated thresholds for defining objective risk, notably the SDQ and Kessler Psychological Distress Scale. Hence, it was necessary to determine our own criteria, which inevitably involved some subjectivity in the risk definitions. We note, however, that common approaches of defining risk, such as nominating × standard deviations from the mean or y% of the population as ‘at-risk’, were not considered acceptable. It in effect assumes what it is we were seeking to estimate. Instead, our definitions were informed by the inherent meaning in the response options. We have also been careful in documenting our risk cut-points. Defining risk cut-points is essentially an empirical question (the likelihood of a poor outcome), which given the richness of the LSAC data and planned long terms follow-up should be able to be established objectively, over time.
The mapping of LSAC variables to the risk factors identified by Fryers and Brugha (2013) was not perfect. The risk domains where mapping was less successful included neurological vulnerability and child maltreatment. We used two pregnancy risk factors, smoking and drinking alcohol, to indicate neurological vulnerability in addition to premature birth, need for ventilator after birth, developmental outcomes and intelligence. These variables in particular highlight intervention opportunities for preventing neurological deficits and disorder (Been et al., 2014; Flak et al., 2014). LSAC does not include direct measures of child maltreatment. We included a variable measuring intimate partner violence as an indicator of domestic violence; however, it does not identify whether children were witnesses to incidents of violence. Sexual abuse and neglect are entirely absent from LSAC, with harsh parenting an indicator of physical abuse and emotional abuse, captured under the parenting and parent–child relationships domain. Given that child maltreatment is so strongly associated with poor health and emotional well-being in adulthood (Anda et al., 2006) and has been identified elsewhere as highly prevalent (Delfabbro et al., 2010), it is unfortunate that we were unable to include it in the present study. We note questions on child maltreatment are to be included in later waves.
Missing data were not imputed and, therefore, the prevalence estimates reported here are likely underestimates. Analysis confirmed that data were unlikely to be missing at random on these variables as children with missing data had higher scores on the SDQ total problems scale than children without missing data.
Implications
This study translates an important part of the evidence base into a format that can be more readily used by policy-makers for service and workforce planning in preventive mental healthcare. We undertook a conservative approach to defining risk and managing missing data, which means that the prevalence estimates reported here indicate a minimal level of need. Based on the limited evidence that exists, it also means that the current level of service provision available to families, infants and children 12 years or younger is clearly inadequate. Only piecemeal information is available about access across the fragmented services provided to families, infants and children. For example, a study by Lucas et al. (2013) indicated that only 2% of children with mental ill-health make use of Medicare-reimbursed mental health services, although it must be noted that families access support through a range of services including paediatric, nursing, non-profit and child protection sectors. More than likely, however, the majority of children, particularly infants and toddlers, with risk factors for mental illness are not accessing any services (Australian Association for Infant Mental Health, Inc. [AAIMHI], 2015).
In reality, exposure to risk factors occurs in a complex interactive way. For example, alcohol use during pregnancy can cause developmental delay that also constitutes an independent risk, resulting in disturbed child behaviours, which combine to increase risk of poor school performance and poor school performance poses an independent risk of poor health. This example highlights how risk factors independently and cumulatively predict poor mental health. As a result, there is a need to intervene early in the child’s life and in a way that is cross-sectoral and multidisciplinary so that children and families are supported as early as possible, before risk accumulates. Government and service planning for prevention in mental health will not be successful unless such a holistic approach is applied.
A valuable next step in this line of research would be to use this set of risk factors to investigate the interactive and cumulative nature of risk exposure across childhood. It may be that there are certain risk trajectories more potent than others, which could help to identify optimal intervention opportunities and effective treatments.
Conclusion
To our knowledge, no other research has attempted to estimate the prevalence of children between ages of 0–13 years at-risk of developing adult mental illness. By identifying important risk factors and quantifying their prevalence in the Australian population, it translates an important piece of the evidence base into a more useful format for policy-makers. This research demonstrates that there are key opportunities to intervene at the earliest stage of the life course to prevent adult mental illness. In 12 infants, 1 has risk factors for adult mental illness and 1 in 40 has ⩾5 risk factors. By the time children are 10–11 years, 1 in 5 children have ⩾5 risk factors. While these numbers are alarming, they also point to an exciting opportunity to intervene in the life course of a great many children and shape a brighter and more positive future for Australia.
Footnotes
Acknowledgements
We would like to thank Prof Nicholas Proctor and Ms Catherine Turnbull for their contributions to the broader the project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Health and Medical Research Council and SA Health (Partnership Project APP1055351).