
Abstract
Objective:
In clinical settings, there is substantial evidence both clinically and empirically to suggest that approximately 50% of individuals with borderline personality disorder experience auditory verbal hallucinations. However, there is limited research investigating the phenomenology of these voices. The aim of this study was to review and compare our current understanding of auditory verbal hallucinations in borderline personality disorder with auditory verbal hallucinations in patients with a psychotic disorder, to critically analyse existing studies investigating auditory verbal hallucinations in borderline personality disorder and to identify gaps in current knowledge, which will help direct future research.
Method:
The literature was searched using the electronic database Scopus, PubMed and MEDLINE. Relevant studies were included if they were written in English, were empirical studies specifically addressing auditory verbal hallucinations and borderline personality disorder, were peer reviewed, used only adult humans and sample comprising borderline personality disorder as the primary diagnosis, and included a comparison group with a primary psychotic disorder such as schizophrenia.
Results:
Our search strategy revealed a total of 16 articles investigating the phenomenology of auditory verbal hallucinations in borderline personality disorder. Some studies provided evidence to suggest that the voice experiences in borderline personality disorder are similar to those experienced by people with schizophrenia, for example, occur inside the head, and often involved persecutory voices. Other studies revealed some differences between schizophrenia and borderline personality disorder voice experiences, with the borderline personality disorder voices sounding more derogatory and self-critical in nature and the voice-hearers’ response to the voices were more emotionally resistive. Furthermore, in one study, the schizophrenia group’s voices resulted in more disruption in daily functioning. These studies are, however, limited in number and do not provide definitive evidence of these differences.
Conclusion:
The limited research examining auditory verbal hallucinations experiences in borderline personality disorder poses a significant diagnostic and treatment challenge. A deeper understanding of the precise phenomenological characteristics will help us in terms of diagnostic distinction as well as inform treatments.
Introduction
Borderline personality disorder (BPD) is a serious mental illness marked by prolonged patterns of distinct impulsivity, instability of affect, interpersonal relationships and impaired self-image. According to the Diagnostic and Statistical Manual of Mental Disorders–Fifth Edition (DSM-5), psychotic symptoms such as auditory verbal hallucinations (AVH) and other ‘positive’ symptoms of psychosis may be present in patients with BPD, but occur ‘only for brief periods in situations of distress’ (American Psychiatric Association [APA], 2013). AVH are defined as an auditory or speech experience in the absence of an actual stimulus (David, 2004). Commonly, these experiences involve hearing one or more talking voices. Yet, experienced clinicians have recognized that a high proportion of BPD patients (50–90%) report longstanding and frequent AVH (Kingdon et al., 2010), but the extent of these experiences is not clearly recognized in the DSM. Furthermore, The International Classification of Diseases, version 10 (World Health Organization, 1992) makes no mention of psychotic symptoms in BPD. There has been only limited research as to the phenomenology of AVH in BPD patients and how mental health professionals view these symptoms in clinical practice.
AVH are a critical problem faced by clinicians who treat patients with BPD (Kingdon et al., 2010). Ongoing or persistent ‘voices’ associated with BPD often attract a clinical diagnosis of primary psychotic disorder (e.g. schizophrenia, schizoaffective disorder), which can result in incorrect treatments. The importance of clarifying whether a patient has BPD or a psychotic disorder lies in the different treatment approaches that the different disorders require. According to draft treatment guidelines developed in Australia for BPD, the best practice intervention for this disorder is psychotherapy (e.g. dialectical behavioural therapy, cognitive behavioural therapy [CBT], schema-focused psychotherapy, mentalization-based therapy) as this is the only method of treatment that has been shown to be effective for the core features of impulsivity, unstable identity and problems with emotional regulation (National Health and Medical Research Council [NHMRC], 2012). These guidelines are comparable to the UK guidelines that recommend effective treatment for BPD consisting of little or no medication, with psychotherapy being the core intervention (National Institute for Health and Clinical Excellence [NICE], 2009). However, schizophrenia is a complex disorder with substantial heterogeneity in terms of the ways in which it manifests. People with schizophrenia require a comprehensive set of interventions encompassing medication as well as psychosocial domains. Psychological therapies such as CBT in particular can be effective for helping people deal with auditory hallucinosis (Castle and Buckley, 2015).
Incorrectly diagnosing a patient with BPD who reports ‘voices’ as having a primary psychotic disorder is costly to the health system. According to Australian health statistics in terms of the cost per case, schizophrenia is the most costly mental illness to treat (Andrews and Titov, 2007). After anorexia nervosa, BPD is the third most costly disorder per case. This issue of misdiagnosis of BPD with psychotic features is made particularly difficult as recent evidence has suggested that 10% of patients initially diagnosed with BPD actually do transition to a psychotic diagnosis (Thompson et al., 2012). Offering inappropriate treatment for patients with BPD makes little impact on the core features of this disorder. When a diagnosis of a psychotic disorder is inappropriately applied, patients may be less likely to be seen as needing to take responsibility for their actions, as is necessary for patients with BPD. Self-harming behaviours often increase in this context (Paris, 2004). A recent Cochrane review of management of BPD concluded that ‘overall pharmacotherapy did not appear to be effective in altering the nature and course of the disorder. Evidence does not support the use of pharmacotherapy as first line or sole treatment for BPD [borderline personality disorder]’ (Stoffers et al., 2010). In addition, the prescription of unnecessary psychotropic medication can lead to adverse health outcomes in the form of metabolic syndromes (i.e. hypertension, diabetes and obesity), extrapyramidal side effects and tardive dyskinesia. Developing a clearer understanding of the similarities and differences of the voice experience across BPD and schizophrenia has the potential to help better understand the pathogenesis of each condition as well as inform treatment.
We argue that the clinical observation of ‘voices’ in BPD warrants further investigation and clarification so that mistreatment does not adversely affect patient treatment and cause iatrogenic harm. The language for describing ‘voices’, or AVH, has been debated since the 1850s (Berrios and Dening, 1996). Debate has continued to the present day and has resulted in distinctions being made between hallucinations that are associated with primary psychotic disorders and those that are of a lesser nature referred to as pseudohallucinations. The distinction between the two is poorly delineated, and the empirical validity is questionable (David, 2004).
In relation to psychotic disorders, David (2004) has suggested that describing AVHs is fraught with a lack of clarity in terminology. The most common form of AVH is a voice speaking to the patient directly, in the second person. These voices are personified and often occur inside subjective space. The term ‘pseudohallucination’ has been used to describe hallucinations that are isolated, that have been identified as being a production of the person’s own mind and that do not fit into primary psychotic diagnoses, such as schizophrenia (Berrios and Dening, 1996; Brewin and Patel, 2010). Research has not been able to discriminate between these two types of voices on the basis of internal location (Copolov et al., 2004).
Over the last 20 years, there has been a great deal of research in AVH in schizophrenia that has examined the cognitive mechanisms reported to be involved in the aetiology of AVH. In brief, such research has focused on a number of core possible mechanisms. First is impaired or faulty inhibition; the inhibition account suggests that patients experiencing AVH are impaired in their capacity to intentionally inhibit irrelevant representations from consciousness, which, in combination with an impaired ability to link the representation to its origin or context, leads to the experience of an external voice (McLachlan et al., 2013). Second is the suggestion that AVH are the result of fragmented, intrusive, unintentional memory retrieval. This has been supported by a number of lines of evidence, including phenomenological descriptions of the voices, neuroimaging data during voice hearing that equates to memory recall and problems with source memory (a type of episodic memory).
Although neuroimaging studies in BPD are still scarce (De Araujo et al., 2014), there have been some studies investigating the neurobiological mechanisms of BPD. Research has found that patients with BPD are typically associated with disturbed emotional processing (Scherpiet et al., 2014) and have significant morphological abnormalities in the fronto-limbic and paralimbic regions of both hemispheres (De Araujo et al., 2014) when compared to healthy controls. To date, there have been no studies specifically investigating the cognitive or neurobiological mechanisms of AVH in BPD.
Nosology and the problem of voices: are there two different kinds?
The crux of the issue is that the term ‘pseudohallucination’ has been used to refer to the symptom of voices in BPD in the 1970s and 1980s (Pope et al., 1985). However, subsequent researchers have used different terminologies, including ‘brief unsystematised’ psychotic episodes (Chopra and Beatson, 1986), ‘factitious’ (Pope et al., 1985) and ‘quasi-psychotic thought’ (Zanarini et al., 1990) to describe delusions and hallucinations in BPD. Published studies were conducted largely in direct response to the omission of any reference to psychotic symptoms in the definition of BPD in the Diagnostic and Statistical Manual of Mental Disorders–Third Edition (DSM-III) (Pope et al., 1985). Those authors, and others, successfully advocated for including psychotic-like experiences in the criteria for BPD in Diagnostic and Statistical Manual of Mental Disorders–Fourth Edition (DSM-IV) (APA, 1994). This change has been maintained in the DSM-5. The studies converge in the view that terminology such as pseudo- and quasi-psychotic/hallucinations should not be used as it trivializes the symptom and dismisses it as unimportant or as ‘not real’ (Adams and Sanders, 2011; Slotema et al., 2012; Yee et al., 2005).
In light of the issues outlined thus far, the aims of this systematic review were to summarize and compare current understanding of AVH in BPD with AVH in a psychotic disorder, to critically analyse existing studies investigating AVH and BPD and to identify gaps in current knowledge which will help direct future research.
Method
The literature was searched using the electronic database Scopus and then verified using PubMed and MEDLINE. Reference lists of sourced articles were also checked for further verification. Journals were searched from 1975 to August 2014, and the search key terms included BDP coupled with one of the following: psychosis, hallucinations or voices. The search resulted in a total number of 910 studies, but only studies meeting the following eligibility criteria were included: written in English, empirical studies specifically addressing AVH in BPD, peer reviewed, used only adult human participants and sample comprising BPD as the primary diagnosis. Studies were excluded for the following reasons: did not compare BPD and a psychotic disorder (e.g. schizophrenia and/or schizoaffective disorder) and studies investigating dissociative symptoms or affective symptoms only. A detailed flowchart of the search procedure is presented in Figure 1.
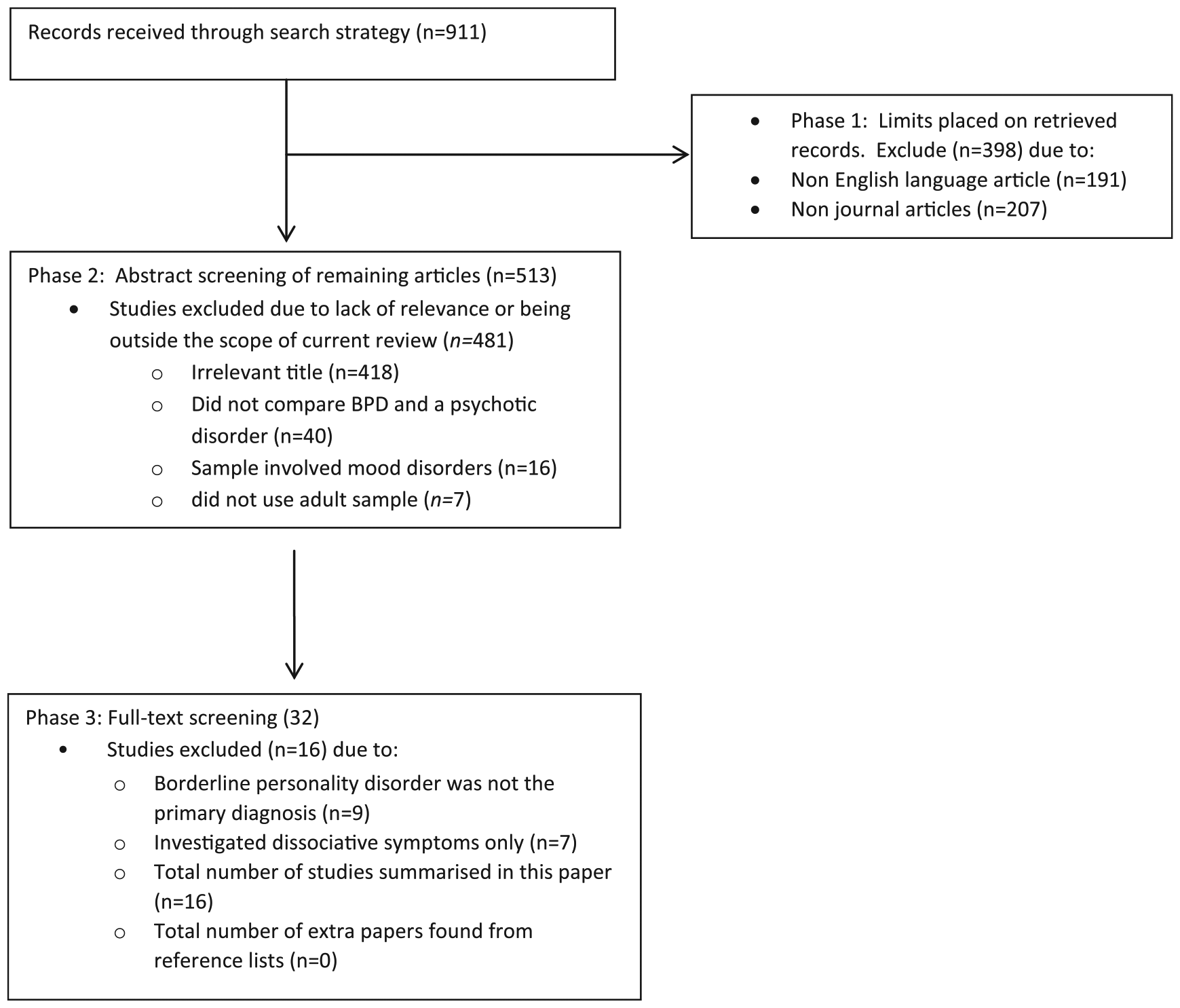
Flowchart of search procedure and number of studies included in and excluded from the analysis at each stage.
Results and discussion
Our search strategy yielded a total of 16 publications meeting the above eligibility criteria. Based on these 16 studies, we critically analyse the methodological limitations of these 16 studies and provide recommendations for future research in this area. Consequently, we summarize the nosology and implications of voice hearing in BPD and the known phenomena of voices in BPD. A summary of the results of these studies is presented in Table 1.
Summary of current studies of AVHs in BPD.

BPD: borderline personality disorder; AVH: auditory verbal hallucinations; Sz: Schizophrenia; SzAD: schizoaffective disorder; HC: healthy controls; BAVQ-R: Beliefs about Voices Questionnaire–Revised; SCID: Structured Clinical Diagnostic Interview for DSM-IV-TR; SCID-D: Structured Clinical Diagnostic Interview for DSM-IV Dissociative Disorders; DIB: Diagnostic Interview for Borderline; ESM: The experience sampling method; SADS: Schedule for Affective Disorders and Schizophrenia; RDC: Research Diagnostic Criteria; DES: Dissociative Experience Scale; MOQ: McGuffin’s Opcrit Questionnaire; BDI-II: Beck Depression Inventory-II; BAI: Beck Anxiety Inventory; PSYRATS-H: Psychotic Symptoms Rating Scale–Hallucinations; CASH: Comprehensive Assessment of Symptoms and History; PSE: Present State Examination; CTQ-SF: Childhood Trauma Questionnaire, Short Form; CTQ: Childhood Trauma Questionnaire; FDS: Fragebogen zu Dissoziativen Symptomen (German adaption of DES); PANSS: Positive and Negative Syndrome Scale.
Common assessment tools used
In the 16 studies investigating AVH experience in BPD, there are some common interview measures and questionnaires used to determine the diagnostic status and psychotic phenomenology. For diagnostic clarification, some studies (Chopra and Beatson, 1986, 1988; Links et al., 1989; Pope et al., 1985; Yee et al., 2005; Zanarini, 1990) use the Revised Diagnostic Interview for Borderline–Revised (DIB-R), whereas others (Zanarini et al., 1990) employed the Structured Clinical Interview (SCID) for DSM-III or the SCID for DSM-IV Axes 1 and 2 relevant to the diagnoses of schizophrenia and BPD (Glaser et al., 2010; Gunderson et al., 1975; Hepworth et al., 2013; Kingdon et al., 2010; Tschoeke et al., 2014). To assess current psychotic symptoms, the Brief Psychiatric Rating Scale (BPRS) and/or the Positive and Negative Syndrome Scale (PANSS) were applied (Glaser, 2010; Tschoeke et al., 2014). For investigations of the specific AVH experience in BPD, studies used qualitative interviews (Adams and Sanders, 2011; Pearse et al., 2014), the Psychotic Symptoms Rating Scale–Hallucinations (PSYRATS AVH-related items) (Kingdon et al., 2010; Slotema et al., 2012), the Present State Examination (PSE) (Pearse et al., 2014) or the Beliefs about Voices Questionnaire–Revised (BAVQ-R) (Hepworth et al., 2013; Kingdon et al., 2010) to describe the phenomenological characteristics and ensuring distress of AVH. Chopra and Beatson (1988) used the ‘psychosis’ subsection of the DIB to help elicit and categorize psychotic phenomena.
The prevalence of voices is difficult to distinguish using the questionnaires used to date. The BPRS, PANSS and PSE are general interviews that gather current psychotic symptomatology. They measure positive and negative psychotic symptoms as well as ‘general’ symptoms. A limitation, however, is that the hallucinations subsections do not measure the phenomenology in great detail and tend to emphasize those phenomena that are associated with schizophrenia, rather than taking a broader view about these phenomena.
The BAVQ and PSYRATS are thus arguably more useful when looking at the characteristics of AVH across disorders. A limitation to the BAVQ-R is that patients answer ‘yes’ or ‘no’ to all questions; hence, subtle differences and changes over time can be missed. The PSYRATS is useful to quantify the severity of delusions and hallucinations and help to gather phenomenological aspects of voices such as frequency, loudness and location. Drake et al. (2007) found the PSYRATS useful in assessing hallucinations and delusions with good reliability and validity when comparing it to other measures such as PANSS. Thus, this tool would be a useful measure to use when investigating the phenomenology of voices in BPD.
Depending on the specific investigations of each paper, other measures were also used, including Childhood Trauma Questionnaire (CTQ) (Tschoeke et al., 2014), Beck Depression Inventory-II (BDI) and Beck Anxiety Inventory (Kingdon et al., 2010), to evaluate trauma and affective experiences. Other measures used included the Dissociative Experience Scale (DES) (Tschoeke et al., 2014; Yee et al., 2005), Steinberg’s Structured Clinical Interview for DSM-IV Dissociative Disorders (SCID-D) (Tschoeke et al., 2014; Yee et al., 2005) and part of the McGuffin’s Opcrit Questionnaire (Yee et al., 2005). The McGuffin’s Opcrit Questionnaire was developed for research into psychotic illness (McGuffin et al., 1991).
Phenomenological studies of voices in BPD: what is the evidence for their existence?
Prior to and during the DSM-III, studies suggested that psychotic symptoms in BPD were questionable, transient, circumscribed and experienced as alien (Gunderson et al., 1975). The BPD group also tended to have fewer Schneidarian first rank symptoms and thought disorder than patients with schizophrenia (Gunderson et al., 1975). Other studies found that the psychotic-like experiences in patients with BPD were typically of short duration, did not have a pervasive affect on the person’s life, were not experienced like a ‘true’ psychotic episode (Zanarini et al., 1990) and appeared to be factitious, in that the voices appear to be under voluntary control and produced with the goal of assuming the ‘patient’ role (Pope et al., 1985). They were, however, associated with more psychiatric admissions (Miller et al., 1993) than BPD patients without AVH. Chopra and Beatson (1986) reported that in their BPD sample, all had some form of psychotic experience. Slightly less than half experienced AVH and these symptoms were more likely to be experienced in stressful situations. However, the majority of these studies were confounded by the failure to include patients with schizophrenia as comparison subjects and excluded patients with BPD who had enduring psychotic symptoms or co-morbid schizophrenia. Furthermore, apart from that of Zanarini, other studies used very small samples (<5 or case studies). Studies were also limited by DSM-III classification as this diagnostic system did not recognize psychotic symptoms, dissociation or paranoia as being part of BPD. Even so, it is important to emphasize that psychotic symptoms were still reported in these studies, and this provided enough evidence for the criteria for BPD to be amended in the DSM-IV (APA, 1994).
Since the publication of the DSM-IV in 1994 (APA, 1994), 10 main studies have been published concerning psychotic symptoms in BPD. When patients with BPD were compared to those with BPD and schizophrenia, and schizophrenia alone, the rates of AVH reported were 50%, 90% and 66%, respectively, in Kingdon et al. (2010). Overall, the BPD group experienced their voices as more distressing, and more negative, but the location of these voices in space did not differ from other patient groups. Patients with BPD also reported higher rates of childhood abuse.
Other studies have provided evidence to suggest that there are no clear distinctions between psychotic experiences described by patients with schizophrenia (Adams and Sanders, 2011; Pearse, 2014; Tschoeke et al., 2014) and that the voices in BPD are similar to voices in schizophrenia in their phenomenology (e.g. in distress levels and the content was predominantly negative and critical) (Hepworth et al., 2013; Pearse, 2014; Slotema et al., 2012), location (Tschoeke et al., 2014) and cognitive responses (e.g. beliefs about the power and malevolence in their dominant voice) (Hepworth et al., 2013). All these papers are more recent in their investigations, with some using schizophrenic comparison samples (Hepworth et al., 2013; Slotema et al., 2012; Tschoeke et al., 2014) and empirically proven measures (Slotema et al., 2012; Tschoeke et al., 2014). These voices may occur in the context of interpersonal relationship difficulties (Suzuki et al., 1998), and at times of increased stress (Glaser et al., 2010; Yee et al., 2005), and may be associated with past traumatic events (Tschoeke et al., 2014). Voices were sometimes identified as similar to the voice of an abuser and themes were associated with past traumatic experiences (Papadimitriou, 2007). These voices triggered by past memories of trauma were reported to be more distressing, negative, controlling and critical than what is typically reported in psychotic disorders (Yee et al., 2005). Together, these studies suggest that cumulative exposure to stressful life events, childhood abuse and neglect, and daily life stress are plausible risk factors for voices in BPD, which indeed Hepworth et al. (2013) also point out in their recent empirical study. Their conclusion was that the main difference between schizophrenia and BPD was in the affective realm, more specifically, that BPD patients had a greater emotional resistance to the voices than the schizophrenia patients.
One other difference in voices between the groups was that the voices caused more disruption to life in the schizophrenia and schizoaffective groups than those with BPD (Slotema et al., 2012). But in BPD participants, disruption to life was more significant than non-clinical participants who have voices (Slotema et al., 2012). It is important to note that the outcomes of the Slotema study do not stipulate whether the disruption to life in the schizophrenia group is solely due to AVH or merely due to other symptoms experienced in schizophrenia, for example, negative symptoms. Furthermore, the healthy controls who hear voices in this study are an interesting group to investigate given there is building evidence (i.e. Taylor and Murray, 2012) to suggest that there are non-clinical groups with no diagnosis who experience AVH but do not experience any associative distress, therefore do not seek treatment.
Conclusion on our current knowledge about voices in BPD
The voices in BPD pose a significant diagnostic and treatment challenge. Given this, it is surprising that there has been such limited research and investigation. There have been data to suggest that these ‘voices’ may be AVH similar to those reported in schizophrenia and alternative data that imply they may be different and dissociative in origin, relating to insecure disorganized attachment and subsequent childhood trauma. We acknowledge that clinicians intuitively feel that they are related to emotional phenomenon in BPD, but there is not enough empirical research to fully support these clinical findings. The lack of clarity about the diagnostic significance of voices in BPD continues to contribute to uncertainties about treatment. Phenomenological studies have been unable to provide definitive evidence for a difference between the AVH in schizophrenia and the voices reported by patients with BPD, and therefore, deeper understanding of exact phenomenological characteristics in this area is needed. In schizophrenia research, PSYRATS is the most common measure used to assess AVH, but has been rarely used to quantify the phenomenology in BPD. This particular measure should be used in future research as it provides important information on distress, preoccupation and insight and will provide the important phenomenological information we need on AVH in BPD as well as be compared to the schizophrenia literature. This will then help us make that diagnostic distinction between BPD and schizophrenia that we need in order to inform treatment.
Many studies are ambivalent about the type of terminology used to describe ‘voice hearing’ in BPD due to the unclear psychotic knowledge and understanding in BPD. There is emerging evidence that in BPD voices may be related to memories of trauma and can be exacerbated by daily stress and life events. Currently, DSM-5 criteria state that psychotic phenomena in BPD occur only at times of stress, yet our review suggests this view is too restrictive and should be revised.
It is also evident that there is only a limited neurobiological literature, with no studies investigating the cognitive mechanisms and neural networks associated with AVH in BPD. Using neuroimaging, future research should focus on this area to help better understand, from a cognitive and neurobiological perspective, why some people with borderline hear voices and some do not.
Other areas where little to no empirical studies exist include the effects of medication on AVH in BPD; how AVH in BPD relates to clinical aspects such as trauma, disassociation, attachment and other co-morbidities; papers assessing other auditory hallucinations such as music and animal sounds; and no researchers have put forward an integrative bio-psycho-social model to explain AVH in BPD. These four main areas also need to be focus of future research to help us better understand AVH in BPD. Finally, many of the papers reviewed are of small sample size; therefore, large-scale comparison studies are also needed in this area.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.