
Abstract
Injury is a leading global cause of morbidity [1], an important component of which is psychological distress and mental disorder [2–4]. The psychological sequelae of serious injury, usually manifest in post-traumatic and depressive symptomatology, may emerge from the experience of a traumatic event or the physical and functional consequences of the injury. The advent of this morbidity after a recognizable event makes it theoretically amenable to early preventative intervention. To date the focus of preventative intervention has been directed at reducing post-traumatic symptoms using debriefing, with the balance of evidence yet to support its efficacy [5]. An alternative approach of addressing the physical and functional consequences of injury has not been explored. This paper describes a randomized controlled trial of interpersonal counselling (IPC) applied as a universal preventative intervention after major physical trauma.
New cases of major depression and post-traumatic stress disorder (PTSD) occur in approximately one in 10 cases after major injury [2, 4, 6, 7]. In a 12 month follow up of 363 admissions to a trauma centre O'Donnell et al. reported major depression or PTSD alone in 4% of cases, while both diagnoses were present in 6% of cases [2]. Significant psychological distress, represented by subsyndromal disorder or self-reported symptoms to a level of caseness, occur in at least 20% of patients in the first year after injury [8–10]. In a minority of cases adverse symptoms will become chronic. In the case of post-traumatic symptoms this is more likely to occur when they persist beyond 6 months [11]. Less is known about the natural history of depressive symptoms after serious injury, although major depression is known to be a recurrent disorder in the general population [12].
Persistent physical disability is common after major physical trauma and may underpin persistent adverse psychological symptoms. Holbrook et al. found that 18 months after admission to a trauma centre, 80% of patients scored below the functional health norms [13]. The mean physical role score, assessed using the Short Form 36 (SF-36) [14], in 247 people 12 months after admission to a trauma centre was 35% less than the norm [15]. More severe injuries [16] and multiple extremity injuries [17] are more likely to lead to persistent physical disability. Although on a population level, physical disability and depression have been linked [18], in injured populations the relationship has not been well explored.
Preventative approaches can reduce the emergence of new cases of disorder and be cost-effective [19–21]. An important decision in prevention research is between adopting universal approach or targeted approach [22]. A universal intervention has the advantages of not requiring screening and triage, but at the cost of diluting its potential effect size by intervening in individuals who will not otherwise manifest significant psychological distress. A targeted approach is built around a method of identifying high-risk individuals, and although more efficient, carries the potential to miss cases. In the case of serious injury, to date, no predictive tool has been developed with adequate sensitivity and specificity to fulfil this role [23, 24]. An alternative strategy using a stepped care approach in which injury survivors are monitored and triaged to specific therapies as symptoms emerge, has been shown to be of benefit [25], albeit requiring significant resources.
In light of the high levels of persistent disability after serious injury and a relationship between disability and depression, the hypotheses may be raised that a brief universal psychological intervention aimed at addressing the physical and functional consequences of serious injury may be effective in reducing long-term psychological morbidity. In order to test this hypothesis we conducted a randomized controlled trial of IPC in a population of patients after major physical trauma. IPC was chosen as the specific therapy because its aims in promoting adaptation to role change and loss appeared well matched to the challenges described by injury survivors [26]. In addition IPC has been shown to reduce depressive symptoms in patients with medical comorbidity [27, 28], is brief, standardized, can be tested for adherence and is able to be administered by a range of practitioners [29]. The aim of the intervention was to promote adaptation to injury, reduce depressive and post-traumatic symptoms and prevent the emergence of new episodes of psychiatric disorder.
Methods
Participants
All patients admitted to the two level 1 trauma centres in Melbourne, Australia over an 18 month period were screened for eligibility. Patients were eligible if they were aged ≥18, had experienced major physical trauma, had not sustained a major head injury or injury due to self-harm and did not currently have a psychotic illness. The criteria for major trauma applied was one or more of: Injury Severity Score (ISS) >15 [30]; serious injury to two or more body systems; urgent surgery for non-limb injuries; or injuries requiring mechanical ventilation for >24 h. Patients were deemed not to have a major head injury if post-traumatic amnesia lasted <24 h, there were no lesions on computed tomography and patients scored ≥27 at assessment on the Mini-Mental State Examination [31]. The study was approved by the Research and Ethics Committees of the participating hospitals.
Measures
Subjects who agreed to take part in the study provided informed consent and underwent a baseline assessment within 2 weeks of their accident and after parenteral narcotic medication had been discontinued. Baseline assessment consisted of collection of demographic data, Structured Clinical Interview for DSM-IV (SCID) [32] to determine past and current (taken to mean at the time of the accident) psychiatric diagnoses, completion of questionnaires assessing current depression (Beck Depression Inventory, BDI [33]), anxiety (Hospital Anxiety and Depression Scale, HADS [34]), post-traumatic symptoms (Post-Traumatic Checklist [35]), alcohol use (Alcohol Use Disorders Identification Test [36]) and a 10-point visual analogue scale for pain (anchored from none to severe). Assessments at 3 and 6 months consisted of a repeat of the baseline questionnaires. At 6 months a repeat SCID was conducted by an assessor blinded to the treatment condition and the previous assessment results. The SF-36 was completed as a measure of health-related function [14].
Randomization
Subjects were randomized to IPC or treatment as usual. The process of randomization involved the initial assessor contacting a research officer who made a blinded selection from a box of mixed envelopes. The active intervention was allocated at a ratio of 5:4 in expectation of a proportion of therapy patients not completing the full course of treatment.
Intervention
IPC was delivered to subjects in the first 3 months after their injury. The therapists were clinical psychologists registered with the state psychology board who had received at least 20 h of seminar training in IPC, supervision of at least two cases by an experienced IPT (interpersonal therapy) practitioner and ongoing peer review using videotaped sessions. The IPC manual developed for the study of IPC in primary care settings [27] was adapted to the patient population over six pilot cases in order to improve relevance and acceptance. As part of the therapy, the impact of the injury on interpersonal issues pre-dating the injury were identified and explored. Interpersonal issues arising after the trauma that were addressed included the degree to which needs were communicated with and responded to by family, health professionals and, in some cases, insurers. The domain of role transition was expanded to include the transition from health to injury. Issues of grief and loss arising from the injury were explored and related to pre-injury issues where appropriate. Strategies to enhance adaptation to theses issues were outlined in therapy and practised by the patient between sessions.
Psychotherapy adherence was measured using the Collaborative Study Psychotherapy Rating Scale (CSPRS) [37]. Two assessors, blinded to details of the case, scored three videotaped sessions from each completed therapy, one randomly chosen from each of the first two, middle two or final two sessions. The interrater reliability of the assessors was 0.94 using interclass correlation. The mean difference between IPT and cognitive behavioural therapy (CBT; IPT-CBT diff) subscale scores was 0.56 (SD = 0.35), which was significantly different from a mean score zero (t = 10.9, p = 0.001). Therapy acceptance was measured by asking subjects who completed the IPC to provide a written answer to the question ‘what were the positive and negative aspects of your therapy’ after completion of their final session.
Treatment as usual
Subjects allocated to treatment as usual were informed following randomization that they would not be receiving the IPC and would be reassessed at 3 and 6 months. In the case of psychological distress they were recommended to seek assessment through their primary practitioner, but were also able to contact the study coordinator.
Statistical analysis
Data screening was conducted using a number of techniques including visual inspection of histograms and boxplots and examination of statistics for skewness, kurtosis and normality (Kolmogorov–Smirnov). Skewed data underwent logarithmic transformation.
An analysis of covariance was used to determine if there was a difference in symptom measures between subjects completing IPC and those receiving treatment as usual. The dependent variables used in separate analyses were the BDI, HADS and Posttrauma Stress Disorder Checklist (PCL) scores at 3 and 6 months. The baseline scores for the symptom being measured, age and gender, were entered as covariates. The study was designed to detect a moderate effect size (0.5) in symptom scores with a power of 0.7. The χ2 statistic or Fisher's exact test were used to analyse differences between the number of cases of psychiatric disorder in each group at 6 months.
Results
Sample
A total of 964 cases of major trauma were assessed, of which 146 were eligible (Figure 1). The thirty two patients who refused to participate in the study did not differ from participants in terms of age, gender, injury severity or length of stay.
Flow diagram of enrolment, randomization and follow up. IPC, interpersonal counselling.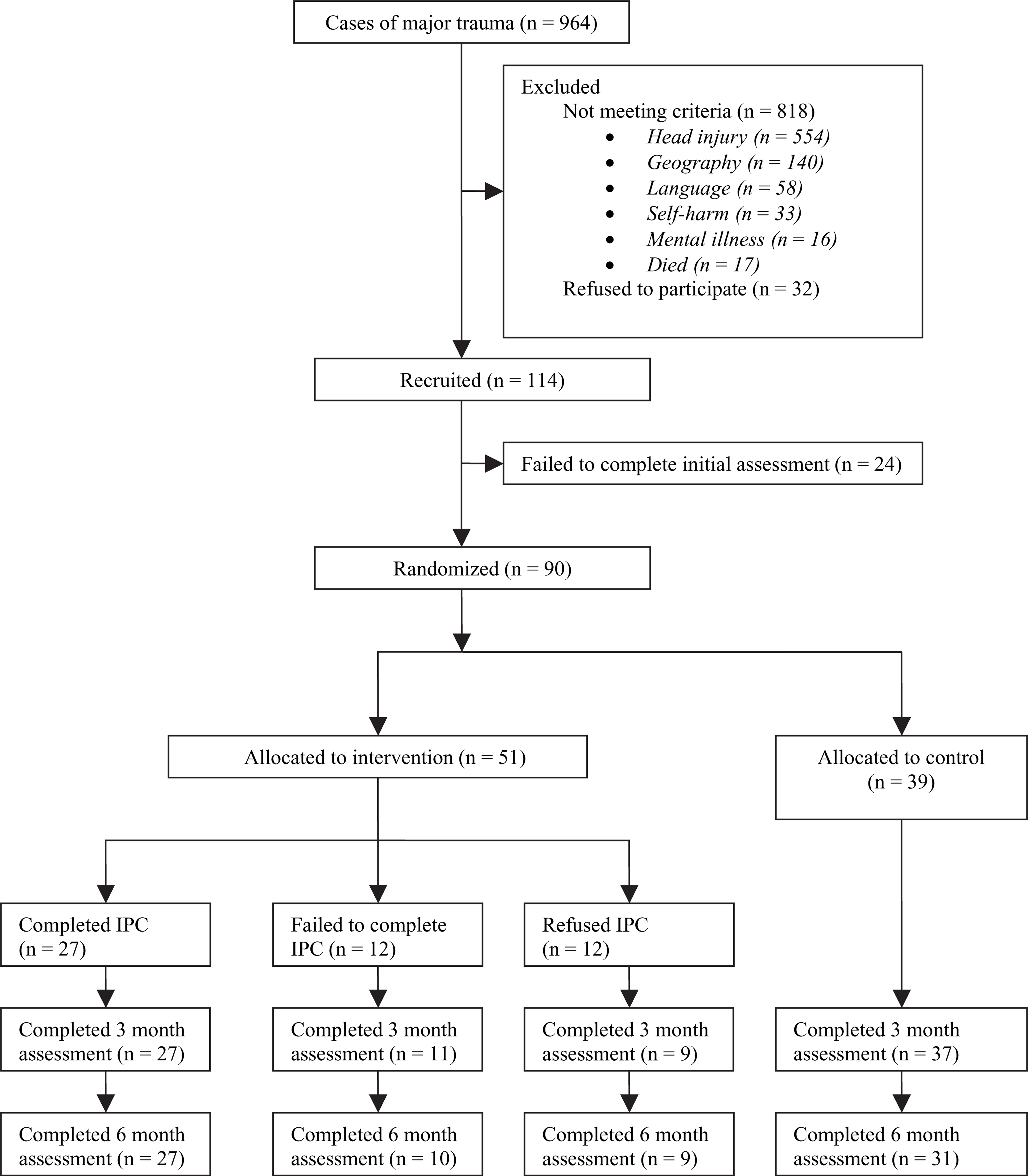
The mean age of the 114 subjects recruited was 37.0 years (SD = 14.7). The majority were male (69.2%). The mean ISS was 17.0 (SD = 8.1). Approximately two-thirds of patients (n = 50, 62.5%) had received their injuries in road traffic accidents, 17.5% (n = 14) in falls or collisions and 13.8% (n = 11) through non-accidental injury. When compared with the population of major trauma patients admitted during the time period, recruited patients were younger (37.0 vs 42.2 years, p = 0.006), had a lower ISS (16.7 vs 22.1, p < 0.001), and a longer length of stay (13.8 days vs 11.0 days, p = 0.019).
Patient compliance
Eighty-four patients completed the 3 months assessment and 77 patients the 6 month assessment. The patients who dropped out were no different from those completing the study in terms of age, gender, injury severity or length of stay.
Fifty-one patients were randomized to IPC (Table 1). Of these 24 failed to complete the intervention. Twelve patients declined to commence therapy and a further 12 failed to complete therapy, receiving a mean of 1.5 sessions (SD = 1.0). Those who declined and those who failed to complete did not differ significantly in terms of age, gender, injury severity or length of stay from completers.
Subject characteristics
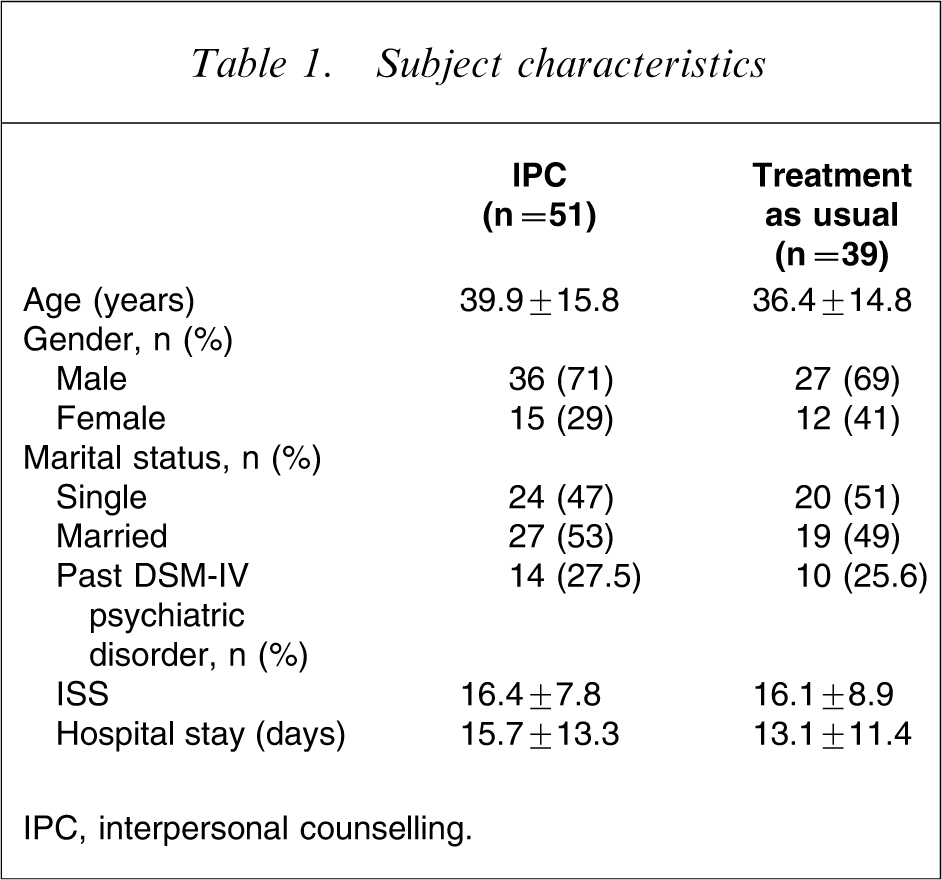
IPC, interpersonal counselling.
Twenty-seven patients completed a course of IPC. Those who completed the IPC did not differ in age, gender or injury severity from those who did not complete therapy. Subjects who commenced, but failed to complete therapy had higher alcohol use as compared with those who completed the IPC (p = 0.035). While none of the completers had current substance or alcohol abuse/dependence, the prevalence in the non-completers was 25% (χ2=7.65; p = 0.007).
Intervention
The mean number of sessions for those completing therapy was of 5.9 (SD = 1.1). The mean psychotherapy adherence scores derived from the CSPRS for interpersonal therapy items (mean score = 1.69, SD = 0.44) was significantly greater than for the CBT items (mean score = 1.16, SD = 0.14; p < 0.001). All patients who completed the IPC completed the acceptance question on the therapy termination form. Those who did not complete the therapy did not complete the form. Eighty-two per cent of comments were positive, with the most common themes relating to the opportunity that therapy provided to express fears and distress about their injuries and to adapt to injury.
Treatment as usual
Patients in the treatment-as-usual group received on average 22.6 h (SD = 44) of non-specific psychological support (physical and occupational) and saw a psychologist or psychiatrist for a mean of 0.8 h (SD = 3.1).
Confounding factors
The mean hours of specific psychological intervention (other than the IPC) and non-specific therapy did not differ between the intervention and treatment-as-usual groups. Physical disability and pain at 6 months did not differ between the two groups.
Intervention outcomes
Psychiatric diagnoses
At 6 months the prevalence of major depression, PTSD, alcohol or substance use/dependence in the intervention group did not differ as compared with the treatment-as-usual group (Table 2). The rate of major depression in the intervention group was 14.8% (n = 4) as compared with 19.3% (n = 6) in the control group (p = 0.45).
DSM psychiatric diagnoses
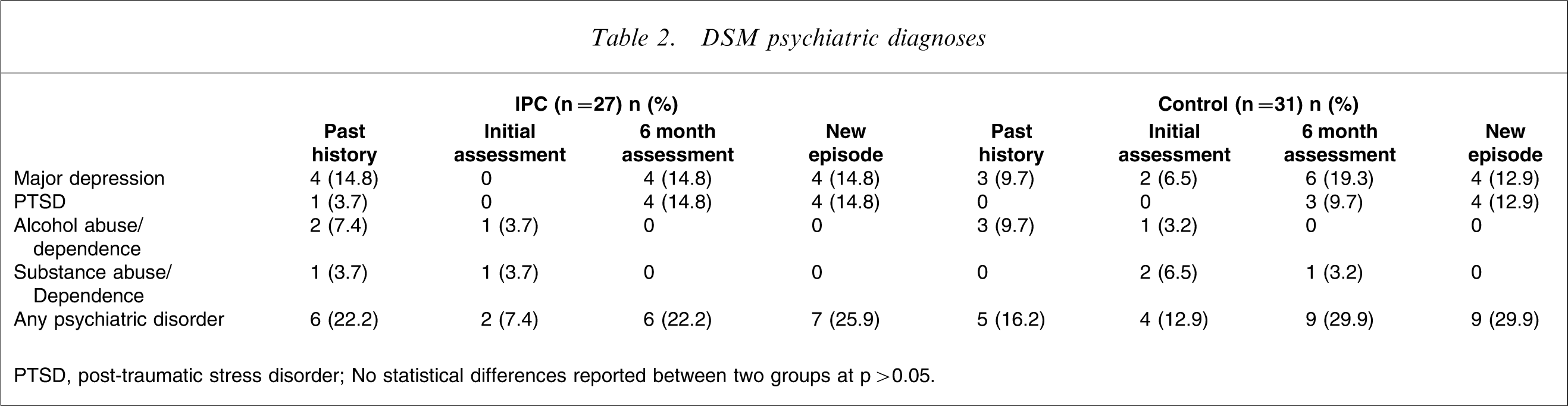
PTSD, post-traumatic stress disorder; No statistical differences reported between two groups at p > 0.05.
Psychological symptoms
No intergroup differences were detected in any of the symptoms scores at any time point (Table 3). An analysis of symptom clusters derived from the PCL indicated no significant differences.
Psychopathology scores (mean±SD)
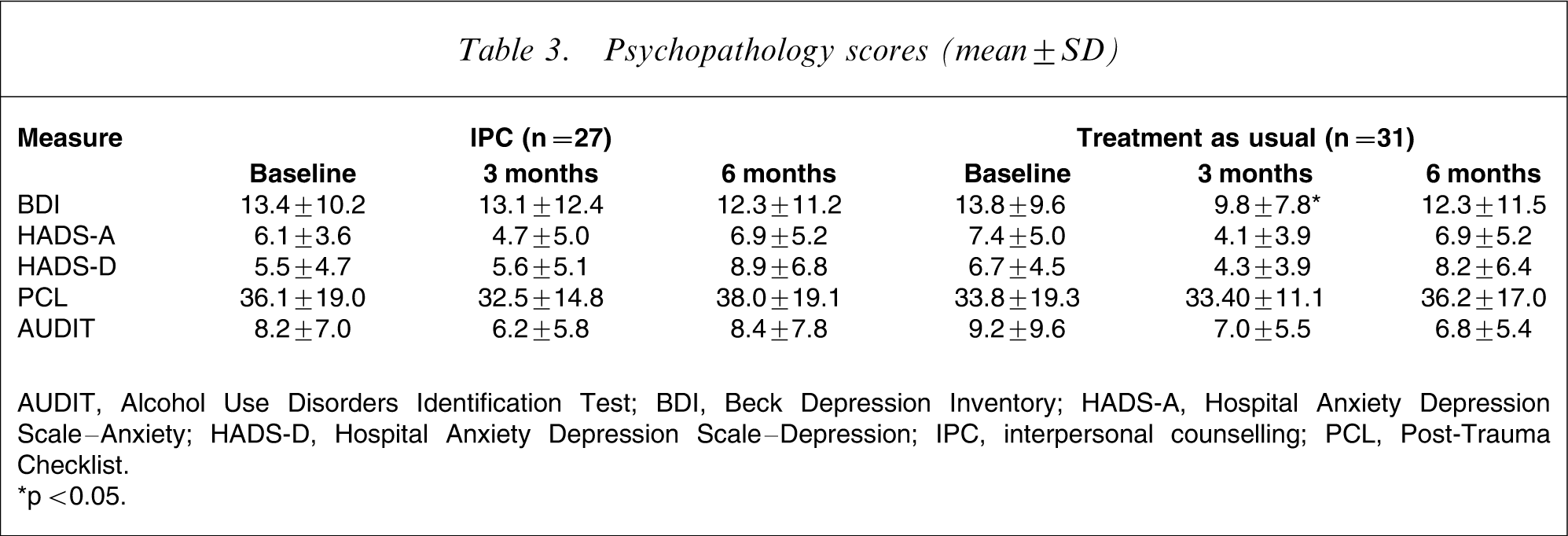
AUDIT, Alcohol Use Disorders Identification Test; BDI, Beck Depression Inventory; HADS-A, Hospital Anxiety Depression Scale–Anxiety; HADS-D, Hospital Anxiety Depression Scale–Depression; IPC, interpersonal counselling; PCL, Post-Trauma Checklist.
∗p < 0.05.
Health-related function
No intergroup differences were detected in any domain of the SF-36.
Post-hoc analysis
Linear regression modelling was used to determine if there was any interaction between treatment effect and past psychiatric disorder in the present sample. In the first step potential risk factors for post-injury psychiatric morbidity (age, gender, past psychiatric history, initial symptoms, and impaired physical function) were tested for bivariate association. Parameters with bivariate association significance p < 0.05 (past psychiatric history, initial symptoms, impaired physical function), along with a measure of injury severity and the treatment condition, were entered simultaneously into linear regression models. The dependent variables were depressive and post-traumatic symptoms scores. Factors that did not retain their significance were removed stepwise. For depressive symptoms at 6 months, initial depressive symptoms (F = 9.4, p = 0.0001), and the interaction of past major depression and IPC (F = 4.7, p = 0.018) were found to be independent predictors. For post-traumatic symptoms at 6 months, initial post-traumatic symptoms (F = 78, p = 0.0001), any past psychiatric diagnosis (F = 8.2, p = 0.006) and the interaction of any past psychiatric diagnosis and IPC (F = 7.7, p = 0.007) were found to be independent predictors.
Discussion
Despite being valued by patients who completed the IPC, the present study provided no evidence that IPC reduced psychiatric disorder or psychological symptoms after major physical trauma. Furthermore, the high rate of therapy dropout challenges the practicality of universal multi-session interventions in this group and complicates the interpretation of the results. The finding a past history×IPC interaction may be interpreted as evidence that the IPC had an adverse effect in a subgroup of vulnerable individuals, raising further concerns about the application of a universal preventative approach after serious injury.
A number of hypotheses may explain the high rate of therapy dropout. Incomplete compliance occurs with a wide range of preventative interventions [38]. Dropout has not been highlighted as a problem with single-session debriefing, but this is probably due to the short timeline between event, engagement and therapy completion. In the present study the balance between a potential, but not proven benefit and the work required to complete the IPC weighed against completion in a group initially committed to the process. In individuals seeking help, motivation is commonly driven by distress. Motivation is a factor strongly associated with therapy outcome [39]. In the case of preventative interventions distress may be absent and hence motivation and compliance impaired. Overall, the fact that dropout occurred despite extensive measures aimed at maintaining engagement, including the choice of therapy, may been seen to support the conclusion that universal multi-session interventions are unlikely to be ever truly universal.
Completing a course of IPC did not ameliorate psychological distress after serious injury. This finding suggests that facilitating adaptation to change and loss is not an effective strategy in this group. The strength of this result may be questioned in the light of the high rate of therapy dropout, although imputation using the data from non-completers did not suggest that symptom scores would have improved had completion rates been greater. The efficacy of IPC may also have been reduced by the ongoing physical consequences injury. This hypothesis is supported by the multivariate models for psychological symptoms at 6 months that showed that impaired physical function was independently associated with higher depressive and post-traumatic symptoms. Persistently impaired physical function may constitute a psychological burden that is better addressed by ongoing management than a brief early intervention.
The combination of IPC and a past psychiatric history was an independent predictor of adverse psychological symptoms at 6 months. The simplest explanation for this finding is that the IPC ‘unravelled’ vulnerable patients after injury rather than protected them. The identification of loss, change and interpersonal problems after injury, rather than leading to adaptive solutions, constituted an additional stress that precipitated a worsening of symptoms. This finding has some similarities to the studies of debriefing [40, 41], which demonstrated adverse results, and raises the possibility that past psychiatric history may differentiate outcome in those studies.
Future research should be based on a targeted approach. The degree to which a targeted approach can be successful will depend on the development of predictive tools for use in this population. That said, even using a tool with excellent specificity (e.g. 0.8) and sensitivity (e.g. 0.8) in a group of 100 injury survivors, three out of 14 cases would be missed and intervention would be conducted in approximately 30 individuals. An alternative strategy, one currently being trialled, is to apply a stepwise approach as modelled by Zatzick et al. [25], guided by the identification of high-risk individuals. Using this approach a subgroup of vulnerable individuals is re-assessed 1 month after their injury and symptomatic individuals triaged to the appropriate psychological therapy.
Conclusion
Psychological distress and psychiatric disorder is common after major physical trauma. IPC, although well-attuned to the challenges of physical trauma, does not reduce the emergence of adverse psychological sequelae and may even increase symptoms in vulnerable patients. The weight of evidence is increasingly against a universal approach after major physical trauma, suggesting that the monitoring of high-risk patients followed by early symptom-specific intervention is a better strategy.
Footnotes
Acknowledgements
The authors would like to thank Dr Myrna Weissman for allowing us use of her manual for the administration of IPC and Associate Professor Scott Stuart for his support with IPC training. We also acknowledge the support of the Victorian Trauma Foundation in providing the financial support for the present study.