
Abstract
Objective:
Bipolar disorder is a chronic relapsing disorder associated with high rates of suicide, suicide attempts and nonsuicidal self-injury. The study aimed to prospectively identify the rates of suicide attempts and nonsuicidal self-injury in young people participating in an adjunctive randomised controlled psychotherapy for bipolar disorder and to identify differences in individuals who engaged in nonsuicidal self-injury, made suicide attempts or did both.
Method:
In all, 100 participants aged 15–36 years with bipolar disorder received 78 weeks of psychotherapy and were followed up for a further 78 weeks. Data were collected using the Longitudinal Interval Follow-up Evaluation.
Results:
Suicide attempts reduced from 11% at baseline to 1% at the end of follow-up (week 156). Similarly, self-harm reduced from 15% at baseline to 7% at the end of follow-up. Individuals who engaged in both nonsuicidal self-injury and made suicide attempts differed from those with who only made suicide attempts, engaged in nonsuicidal self-injury or did neither. They were characterised by a younger age of illness onset and higher comorbidity.
Conclusion:
Adjunctive intensive psychotherapy may be effective in reducing suicide attempts and nonsuicidal self-injury and warrants further attention. Particular attention needs to be paid to individuals with early age of onset of bipolar disorder.
Keywords
Introduction
Bipolar disorder (BD) is a chronic relapsing disorder associated with significant disability and impairment (MacQueen et al., 2001) and is also associated with high rates of suicide (Neves et al., 2009). Between 25% and 60% of individuals with BD attempt suicide at least once in their lives and between 4% and 19% complete suicide (Goodwin and Jamison, 2000) There is also some evidence that nonsuicidal self-injury (NSSI) has a particularly strong association with BD (Joyce et al., 2010; Parker et al., 2005).
The rates of suicide in individuals with BD are much higher than in the general population, with reported rates varying from 20–30 times higher (Pompili et al., 2013) to 60-fold higher (Baldessarini et al., 2006a). A large epidemiological study identified that the lifetime rate of suicide attempts (SAs) for BD was 29.2% which is twice the rate of those with unipolar depression (Chen and Dilsaver, 1996). Additionally, BD is associated with a much lower ratio of attempts: suicide (approximately 3:1) than in the general population (approximately 30:1) (Baldessarini et al., 2006b), suggesting individuals with BD have a higher level of lethality of SA.
The connection between past SA and subsequent attempt or completion is well established. Marangell et al. (2006) found that patients with BD who presented with a history of SA were over four times as likely to have a subsequent SA or completion – previous attempts were the strongest predictor of subsequent attempt. This finding was supported by Oquendo and Mann (2001) who in addition found that the presence of refractory or recurrent depression was also a strong predictor of past SAs. Other risk factors associated with SA in BD included being female, a younger age at illness onset, depressive polarity of current or recent episode, and comorbid conditions including anxiety, substance use disorder, alcohol use disorder and comorbid cluster B/borderline personality disorder (Moor et al., 2012; Schaffer et al., 2014). The presence of three or more comorbid conditions in addition to BD increased the risk of SA eightfold at baseline and greater comorbidity significantly increased the risk of having attempted suicide with high lethal intent (Moor et al., 2012).
There are limited data from prospective studies that examine suicide rates in individuals with BD. A follow-up study of adult psychiatric inpatients and outpatients with BD (mean age: 32.1 ± 11.2 years) over an 18-month period identified that 20% of patients attempted suicide with two deaths by suicide (Valtonen et al., 2006). Similar rates of 19% SA were also found in a 2-year follow-up of adult outpatients with BD (mean age: 32.1 ± 11.2 years) (Galfalvyet al., 2006) and a 5-year follow-up study on children and adolescent outpatients with BD (mean age: 12.6 ± 3.3 years) where 18% had made a SA (Goldstein et al., 2012). There was only one study, the Systematic Treatment Enhancement Programme for Bipolar Disorder (STEP-BD), that followed up SA in the context of a treatment study. This large prospective study (n = 4360) found that 182 individuals (mean age: 40.6 ± 12.7 years) made 270 suicidal acts including eight suicides over 3 years (Dennehy et al., 2011).
There has been much less focus on the association between NSSI and BD. Butler and Malone (2013) defined NSSI as the direct, deliberate destruction of one’s own body tissue in the absence of intent to die. It differs from SA with respect to intent, lethality, chronicity, methods, cognitions, reactions, aftermath, demographics and prevalence. They suggest that the person’s intent is to modify consciousness rather than terminate it. Preceding the act of NSSI is a psychological experience of increasing anger, tension, anxiety, dysphoria and general distress or depersonalisation, which the people feel they cannot escape from or control. As with suicide and SA, rates of NSSI in individuals with BD are significantly higher than in the general population. For example, Esposito-Smythers et al. (2010) found that 22% of adolescents with BD had self-harmed during the course of the most recent mood episode with a lifetime rate of 37% compared to rates of 5–9% of adolescents in Western countries.
While NSSI and SA can be regarded as distinct behaviours based on the relative intensity and clarity of the intent to die and expectation of death (Brown et al., 2002), there is considerable overlap between the two with many individuals engaging in both. In a large study of young adults (Whitlock and Knox, 2007), 24.9% of the sample reported suicidal or NSSI behaviour, with 27.4% of this group engaging in both behaviours. A small study of adolescent psychiatric inpatients identified that 55% had engaged in NSSI only and 44% had engaged in both NSSI and SA (Dougherty et al., 2009). A history of NSSI has also been associated with increased risk of suicide with the absolute risk of suicide doubling after first hospital contact for mental disorder if there was also a history of NSSI (Nordentoft et al., 2011). Furthermore, in those who have been hospitalised for NSSI, 5% had committed suicide within 9 years (Skegg, 2005). In adolescents with unipolar depression, NSSI was the strongest predictor of future SA (Wilkinson et al., 2011).
Although both SA and NSSI are associated with BD, there is limited prospective data on SA and NSSI in individuals with BD especially in the context of a treatment study. The aims of this study were to identify prospective SA and NSSI in young people with BD participating in a randomised controlled trial (RCT) and to identify the characteristics of individuals who engage in either NSSI or SA or engage in both.
Method
This study occurred in the context of a 78-week RCT which examined the efficacy of two disorder-specific psychotherapies interpersonal and social rhythm therapy (IPSRT) and specialist supportive care (SSC) in 100 young people (15–36 years) who also received pharmacological treatment. The primary outcomes for the RCT were decreased cumulative burden of depressive symptoms, improved social functioning and decreased manic/hypomanic cumulative burden outcomes over the period of 26–78 weeks. Participants were followed up for a further 78 weeks. This study focused on secondary research questions addressing impact of the intervention on rates of SA and NSSI.
Inclusion criteria were meeting criteria for Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV)-defined BD I, BD II or BD not otherwise specified (NOS). Exclusion criteria were severe substance abuse disorder as primary diagnosis and having low probability of availability over the 78-week treatment period. Ethical consent was obtained from the Canterbury Ethics Committee. For more detailed information about the study design, see Inder et al. (2015).
Psychopharmacological treatment
Participants were accepted onto the study on any medication regime. Treating psychiatrists used clinical judgement guided by a pharmacological decision tree to optimise psychopharmacological treatment consistent with the American Psychiatric Association guidelines for the treatment of patients with BD. More detailed information is outlined in Inder et al. (2015).
Interventions
IPSRT
IPSRT is a manual-based psychotherapy focusing on (1) the link between mood and life events, (2) the importance of maintaining regular daily rhythms using a Social Rhythm Matrix (SRM), (3) the identification and management of potential precipitants of rhythm dysregulation with special attention to interpersonal triggers, (4) the facilitation of mourning the loss of healthy self and (5) the identification and management of affective symptoms (Frank, 2005).
SSC
SSC is a manual-based therapy for BD disorder based on supportive psychotherapy and the American Psychiatric Association (APA, 2002) guidelines for the management of BD disorder. SSC is a structured individual psycho-education intervention that focuses on identifying and managing triggers for mood instability and developing strategies for mood management. The approach is based on a stress-vulnerability model that allows patients with BD disorder to develop a personalised understanding of the triggers to relapse and their response to these triggers.
Both therapies were delivered by five therapists (two nurses, one psychologist and one social worker) over 18 months – weekly for 10 weeks and then 2-weekly and monthly with the option of increasing sessions if necessary. The therapies were supervised by a psychiatrist experienced in the delivery of both therapies in a research environment. All therapy sessions were digitally recorded, and these recordings were randomly selected for supervision to ensure treatment integrity. Supervision was conducted fortnightly (Inder et al., 2015).
Data collection
Prospective SA and NSSI behaviour data were collected using the Longitudinal Interval Follow-up Evaluation (LIFE) (Keller et al., 1987), at baseline and at weeks 26, 52, 78, 104, 130 and 156. The LIFE is a clinician-based interview which provides a comprehensive picture of the course of a patient’s disorder on a weekly basis over the preceding 6-month period and includes questions of NSSI and SA.
Analyses
Descriptive analyses including frequencies, percentages, means and standard deviations were undertaken on demographic, clinical, lifetime SA and NSSI data. Frequencies and percentages were used to report individuals who made SA or NSSI.
To address the impact of individuals who discontinued in the study on the rates of SA and NSSI, we compared the baseline SA, NSSI, demographic and clinical characteristics on those with complete data (both baseline and week 156) with those with incomplete data using chi-square analyses, Fisher’s exact tests and independent t-tests.
Chi-square analyses and analyses of variance (ANOVAs) were conducted to test the differences between four groups: (1) those who made SA, (2) those who engaged in NSSI, (3) those who both made SA and NSSI, and (4) those who had made neither SA nor NSSI. Post hoc pairwise comparisons using least significance difference (LSD) test and Fisher’s exact tests were used to further examine the differences between the groups when the ANOVAs or chi-squared tests indicated significance (p < 0.05) between group effect.
Results
The majority of the participants were diagnosed with BD I (78%), 17% with BD II and 5% with BD (NOS). Participants were predominantly female (76%) and described themselves as New Zealand European (83%). Mean age at study entry was 26.5 (range: 15–36, standard deviation [SD] = 5.9) years. Mean age of onset of BD was 15.2 (SD = 5.0) years. Approximately half of the participants had a lifetime history of SA and NSSI. Comorbidity was common with 50% of the sample diagnosed with substance use disorder (mainly alcohol), 58% with any anxiety disorder and 18% with borderline personality disorder (Table 1).
Demographic and clinical characteristics of sample (n = 100).
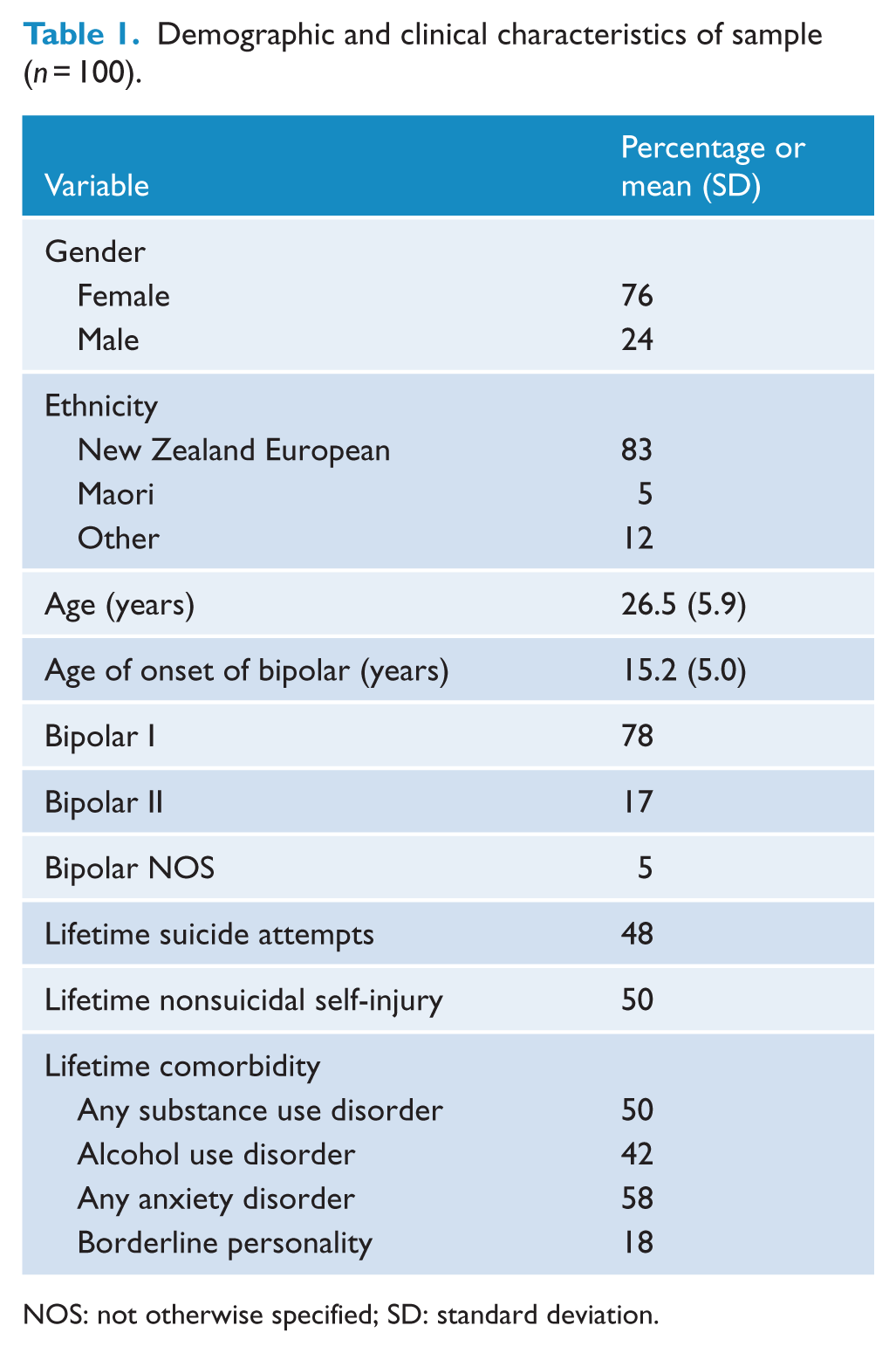
NOS: not otherwise specified; SD: standard deviation.
At baseline (6 months preceding the study), 11 individuals (all females) made a total of 18 SAs. In all, 15 individuals (2 males and 13 females) engaged in NSSI behaviour with over half (N = 8) having self-harmed three or more times. Four individuals had made SA and self-harmed. Subsequent ratings at 6-month intervals identified the individuals who had engaged in NSSI and the individuals who had made SA over the preceding 6 months. Over the 156 weeks encompassing the intervention (78 weeks) and follow-up period (78 weeks), the percentage of individuals who made SA and the percentage of individuals who engaged in NSSI reduced markedly (Figure 1). The percentage of individuals who made SA reduced from 11% at baseline to 1% at week 156. The percentage of individuals who engaged in NSSI reduced from 15% at baseline to 7% at week 156.
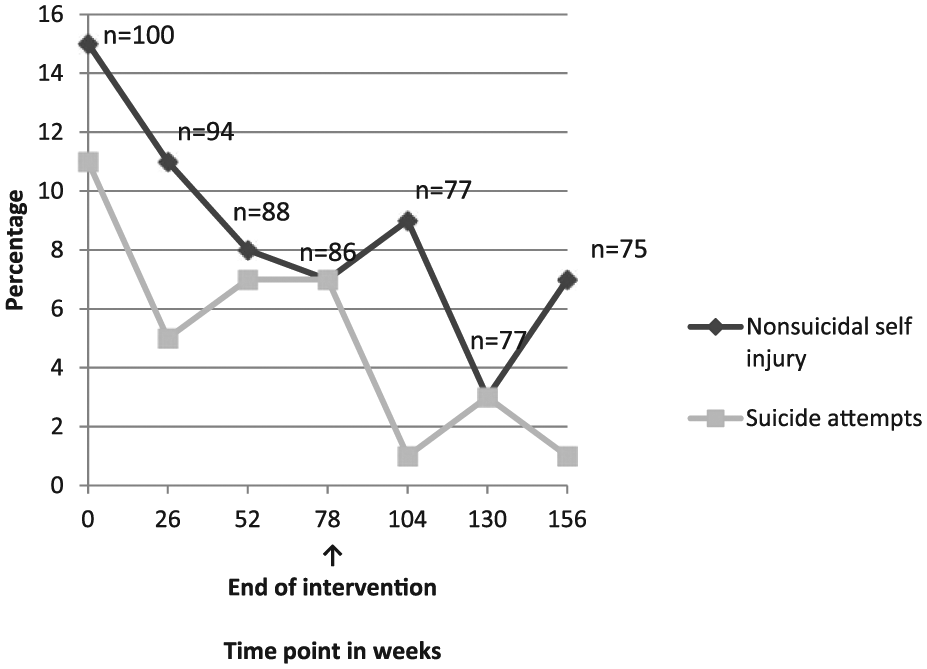
Suicide attempts and nonsuicidal self-injury from baseline to end of follow-up.
One of the confounding factors in interpreting the results from this study is the impact of the dropouts from the study as potentially this group could consist of those participants who were more likely to engage in SA or NSSI behaviours. To address this, we compared the baseline SA and NSSI of individuals where we had complete data (baseline and week 156) and those where we had incomplete data (no week 156 data). The complete data group (n = 75) consisted of individuals who had completed therapy (n = 65) and those who discontinued therapy but continued in follow-up (n = 10). The incomplete data group (n = 25) consisted of individuals who dropped out of therapy and no follow-up data (n = 11) available and those who completed the therapy phase but no follow-up data for week 156 (n = 14). There was no significant difference in baseline NSSI (p = 1.00) or SA (p = 0.14) between the complete data group and the incomplete data group. There were also no statistically significant differences in gender (p = 0.29), age (p = 0.10), age at onset of BD (0.35), having BD I (p = 0.76) or BD II (0.59). Furthermore, there were no statistically significant differences in comorbidity, specifically substance use disorder (p = 0.18), alcohol use disorder (p = 0.15), anxiety disorder (p = 0.94) and borderline personality disorder (p = 0.59). These findings suggest that the reductions in SA and NSSI are not accounted for by the impact of individuals who drop out.
During the course of the study and the follow-up period, there was one death by suicide of a 29-year-old female who died after taking an impulsive overdose. She had a diagnosis of BD I and had made six previous SAs (overdoses and cutting wrists) although none in the 6 months prior to the study. She had a history of NSSI but had not self-harmed in the 6 months prior to the study. She also had lifetime alcohol dependence and anxiety disorder comorbidity. She had completed 21 sessions of therapy at the time of her death.
Of the 100 participants, 18 individuals had made only SA, 20 had engaged in NSSI only and 30 had both made SA and NSSI. The demographic and clinical characteristics of the participants in each of these groups are presented in Table 2. There were statistically significant differences identified between the group of individuals who made both SA and NSSI and the other three groups (NSSI only, SA only and no SA or NSSI). The SA plus NSSI group had an earlier age of onset of BD, higher levels of comorbid alcohol use disorder, anxiety disorder and borderline personality disorder.
Demographic and clinical characteristics of participants with and without lifetime suicide attempts and nonsuicidal self-injury (N = 100).
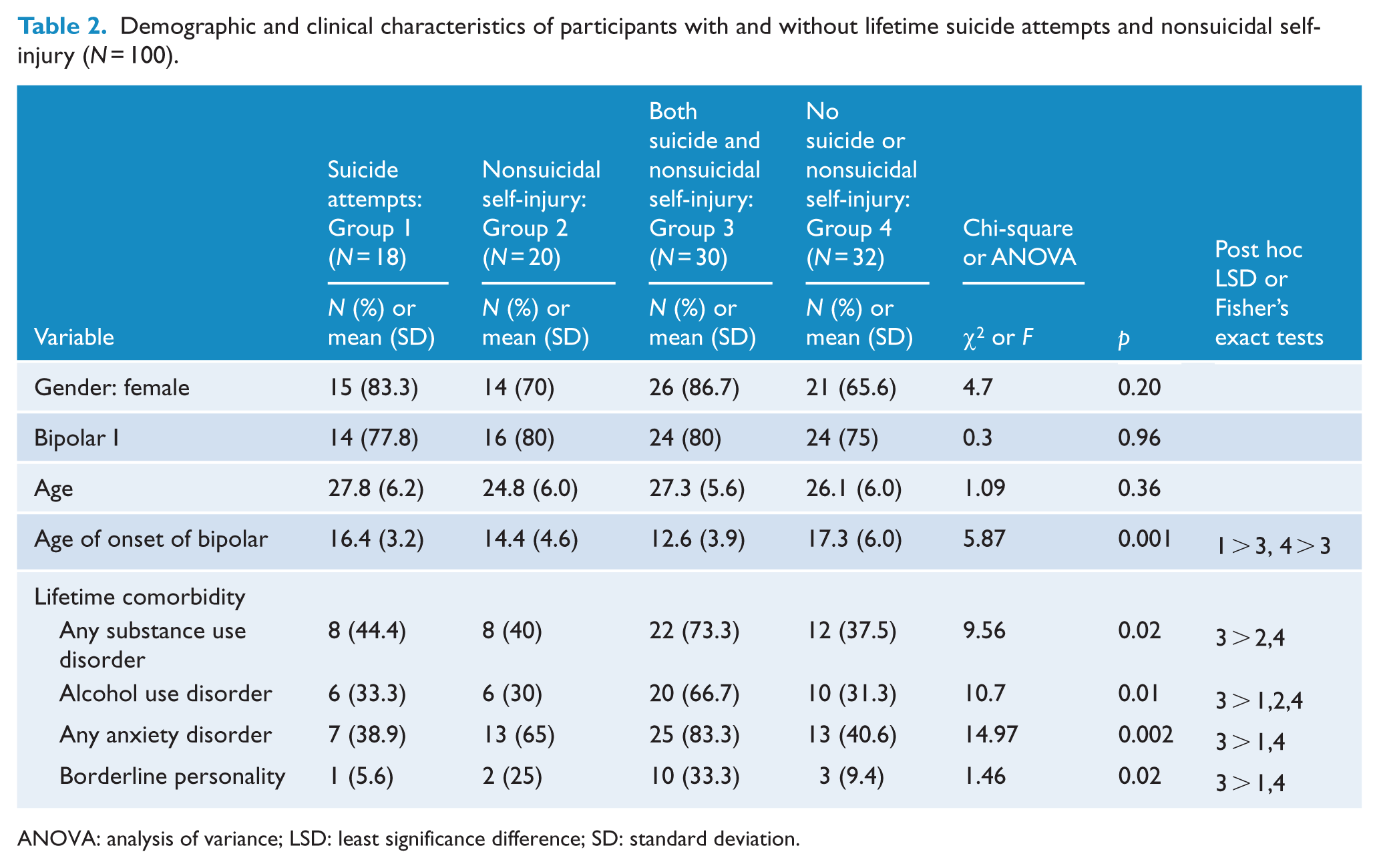
ANOVA: analysis of variance; LSD: least significance difference; SD: standard deviation.
Discussion
Our prospective 3-year study in the context of an adjunctive psychotherapy study for young people with BD (78-week intervention and a 78-week follow-up period) demonstrated a marked decline in SA and NSSI from baseline to end of follow-up. SA declined from 11% to 1% and NSSI from 15% to 5%. We also demonstrated that individuals who engaged in both NSSI and SA were different from the other three groups (NSSI only, SA only and no SA or NSSI) and had a younger age of onset of their illness and greater comorbidity.
Our rates of reduced suicide rates were similar to the STEP-BD rates (Dennehy et al., 2011) of 4%. Our rate of 1.0% for SA was markedly less than that found in other prospective studies without structured interventions who had found rates of 18–20% (Galfalvy et al., 2006; Valtonen et al., 2006). While no claim can be made that the decrease in SA and NSSI can be directly attributable to the intervention, these results add to the growing evidence that adjunctive psychosocial interventions may reduce suicide risk in BD individuals (McIntyre et al., 2008; Rucci et al., 2002). However, the beneficial effects may be also due to the optimised pharmacological treatment the participants received (Cipriani et al., 2005).
The decline in SA and NSSI may relate to the improvement in cumulative depressive symptoms found in our study (Inder et al., 2015) and lends support to the assertion that is possible to decrease the high risk of suicidal behaviour associated with BD disorder through vigorous treatment (Rucci et al., 2002). Another possible contributing factor to account for our findings was the inclusion of adolescents and young adults who may have been more responsive to treatment. Previous reports suggest treatment may be more effective if it occurs early in the course of the illness (Berk et al., 2009).
While not overstating the case for adjunctive psychotherapy, the improvement in SA and NSSI could also be related to the intensive nature of an intervention that was delivered over 18 months. While 18 months may seem long, the mean time spent with each participant who completed the intervention was 25.6 (SD = 11.5) hours (Inder et al., 2015). The delivery of therapy over a longer passage of time may be more beneficial for those with complex conditions such as BD. The delivery of the interventions over 18 months enabled the therapists and psychiatrists to develop strong therapeutic alliances and, importantly, have a long-term view of the person’s mood patterns and symptoms. This enabled a better understanding of each person’s mood patterns and potential triggers and allowed time for important mood management strategies to be developed. Ilgen et al. (2009) have suggested that even minimal increases in the extent to which the therapeutic relationship is perceived as collaborative were associated with a reduction in risk of suicidal ideation.
Other studies have also suggested that intensive intervention can make a positive impact on rates of completed suicide. In the STEP-BD study, 182 patients, out of a total cohort of 4360, made SAs while participating in the study with eight completed suicides. Overall, rates of suicide events in STEP-BD were lower than expected, suggesting that the combination of frequent clinical visits (i.e. access to care), standardised assessment and evidence-based treatment may have been helpful in this population (Dennehy et al., 2011).
It is interesting to consider our study findings in the context of explanatory model of suicidality in BD whereby ‘individuals at high risk of suicide have a tendency to interpret stressful life experiences (past, present or future) as conveying defeat, entrapment or degradation (i.e. negative situation appraisal)’ (Malhi et al., 2013: 563). The most commonly reported stressful life events for individuals with BD were relationship breakups, changes in living circumstances and family relationships, and financial and employment issues (Isometsa et al., 1995). Psychotherapy provides a forum to address the impact of these life events and potentially influence the individual’s appraisal of these events to find alternative and more positive interpretations of their experiences, thus reducing suicidality.
An important component of our study was the finding of marked differences between the group of patients who had a history of both SA and NSSI and the other groups (SA only, NSSI only, neither SA nor NSSI). The group that was engaged in both SA and NSSI was markedly different from the other three groups in that it had a much earlier age of onset of BD and higher comorbidity reflecting greater illness burden and suggestive of a more severe course of illness. The finding of an association of SA with early age of onset of BD has been found in some studies (Goldstein et al., 2012; Perlis et al., 2009) but not other studies (Hawton et al., 2013; Moor et al., 2012). While there has been less focus on NSSI, there is evidence supporting an association between NSSI and early age of onset (Hawton et al., 2013; Moor et al., 2012). However, there has been no consideration given to individuals with BD who engage in both SA and NSSI. Our findings suggest the importance of considering SA and NSSI as separate entities, and those individuals who engage in both behaviours may be a particularly vulnerable group that requires further attention.
The strengths of the study are its long-term follow-up and high retention rate (75% over 156 weeks). However, the number of participants is relatively small especially when considering the number of SA and NSSI being examined. The potential impact of number of patients who dropped out or were lost to follow-up was countered by the finding that there were no significant differences at baseline between these groups. Additionally, the study is conducted among a cohort of young persons with BD who constitute a group relatively understudied in the BD research field.
Conclusion
Our study found a marked decline in both SA and NSSI in clinically representative sample of young people participating in an adjunctive psychotherapy study involving the delivery of two intensive psychotherapies, IPSRT and SSC, over 78 weeks and with 78 weeks of follow-up. Given the high rates of SA and NSSI in BD identifying effective treatments to decrease these behaviours is important in reducing completed suicides and the distress and damage associated with SA and NSSI. Both therapies in combination with pharmacological treatment appear to be effective in reducing these behaviours, which is possibly associated with reducing depressive symptoms. Our findings suggest delivery of such interventions deserves serious consideration in clinical practice particularly targeting individuals with early-onset BD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a grant from the Health Research Council of New Zealand.