
Abstract
Purpose:
Although patients demonstrate a range of problematic health-related lifestyle behaviours preceding suicidal behaviour, there is little research that routinely measure these behaviours. This paper seeks to establish the utility of health-related lifestyle measure (Fantastic Lifestyle Checklist) in people presenting to a major inner city Emergency Department with a range of suicidal behaviours.
Methods:
From 2007–2014, data from the 366 patients who had completed the Fantastic Lifestyle Checklist, after referral by the Emergency Department to a service for people with deliberate self-harm or suicidal ideation, were included in the analysis study. A Maximum Likelihood factor analysis was performed to assess the factor structure of the Fantastic Lifestyle Checklist and the resultant factors were explored in relation to measures of health; namely the Depression, Anxiety and Stress Scale and the 12-item Short-Form Health Survey.
Results:
A three-component factor structure emerged comprising Component 1 ‘positive life investments’, Component 2 ‘poor emotional regulation’ and Component 3 ‘poor health behaviours’. There was a significant negative correlation between ‘positive life investments’ and each of the Depression, Anxiety and Stress scales subscales and significant positive associations with ‘poor emotional regulation’ and Short Form Health Survey-12 mental health scores. Only the Short Form Health Survey-12 physical health subscale was weakly correlated with ‘poor health behaviours’, in females.
Conclusion:
Our findings support the construct and concurrent validity of the Fantastic Lifestyle Checklist measure. The three factors obtained for the Fantastic Lifestyle Checklist were coherent and seem useful for research and clinical practice.
Introduction
A recent review of suicide and suicidal behaviour provides a comprehensive overview of high- and low-income countries, noting that Australia has relatively high rates of suicidal ideation and attempts in line with other high-income countries (Tricky and Brent, 2015). In Australia, deliberate self-harm and suicidal behaviour account for 0.5% of all hospital presentations and clinical practice guidelines available (Boyce et al., 2003). A recent systematic review and meta-analysis of 177 studies reported estimates with reported repetition of non-fatal deliberate self-harm of 16.3% after 1 year and suicide rates of 1.6% after 1 year and 3.9% after 5 years (Carroll et al., 2014). They also stated that annual rates of repetition were 13.7% based on hospital reports and 21.9% based on patient self-report.
However, people with suicidal behaviours are a heterogeneous group, differing in intent and underlying mental health conditions and precipitating factors (Kapur and Gask, 2009). Most studies use outcome measures identifying mental health symptoms, present and past suicidal behaviours, substance use and assessing risk assessment. Although these people have clinical presentations of patients reflecting a range of lifestyle problems preceding depression and suicidal behaviour, these concerns are not generally measured in relation to self-harm, but should be assessed (Tricky and Brent, 2015).
The significance of considering the lifestyle behaviours is highlighted by a long-term follow-up study of over 11,000 patients presenting with deliberate self-harm to an Emergency Department (ED) in a hospital in the United Kingdom (Hawton et al., 2006). In addition to a significantly greater risk of later death by suicide, these patients were found to have a higher mortality rates from causes related to poor lifestyle, including accidents other than poisoning (such as motor vehicle accidents), homicide and most natural causes including respiratory disease, circulatory, neurological, endocrine (generally diabetes), digestive, skin, musculoskeletal and connective tissue disorders (Hawton et al., 2006).
There is considerable literature demonstrating the relationship between depression and lifestyle factors (including diet, substance use, exercise, social support, meaningful life roles) that is too extensive to summarise here (Jacka and Berk, 2012). There is also an increasing appreciation of the relationship between smoking, substance use and suicidal ideation and behaviours (Berlin et al., 2015; Bronisch, 2008). For example, a large German population-based cohort study (Schneider et al., 2014) of risk factors for suicide reported that while depression and being male were strongly associated with suicide risk, lifestyle factors (obesity, smoking and living alone) were associated with increased risk. The researchers concluded that suicide prevention measures pay attention to lifestyle factors as well as mental disorders. A clinical review of alcoholism and suicidal behaviour (Sher, 2006) also concluded that alcohol use is associated with a considerable increase in the likelihood of attempted or completed suicide, particularly when alcohol use co-occurs with depression, stressful life events (including interpersonal difficulties and partner-relationship problems) and poor social support. The authors recommended that assessments of those displaying high alcohol use and/or suicidal behaviours include this range of lifestyle and interpersonal factors.
The focus of this paper is on the assessment of health-related lifestyle factors in a group of people presenting to a major inner city ED with a range of suicidal behaviours. The Fantastic Lifestyle Checklist (FLC; Wilson and Ciliska, 1984) is a brief and accessible measure, designed to assist general practitioners in a holistic assessment of a patient’s health-related behaviours. The FLC has been part of the brief battery of measures used at the Green Card Clinic, a three-session intervention service for suicidal behaviours at St Vincent’s Hospital, Sydney for over a decade (Wilhelm et al., 2000, 2007). The name is derived from groupings of items with the acronym ‘FANTASTIC’, along with the question, ‘How fantastic is your lifestyle?’ The measure allows clinicians to gain a broad range of information regarding a patient’s lifestyle behaviours, both physical (sleep, exercise, diet) and emotional (social connections, experiences of anger, depression). It assesses alcohol and drug use, smoking, risk-taking behaviours likely to lead to accidental death, and potential risk factors for illness and early morbidity due to poor health, such as junk food consumption, exercise and aggression. It also screens for key mental health vulnerabilities (depression, anxiety and anger) and assesses protective factors (role satisfaction and social support). Its simplicity and practicality has led to widespread use, particularly in Canada and South America.
Following the papers on its initial development (Kason and Ylanko, 1984; Simpson et al., 1984; Wilson and Ciliska, 1984; Wilson et al., 1984), the FLC has been used as part of the assessment process for a number of organisations including the Canadian Armed Forces (Melancon, 2004) and paramedics (Justice Institute of British Columbia, 2013). Research using the FLC has been published from Brazil (Rodriguez Añez et al., 2008), Korea (Kim et al., 2006), Australia (Kamien and Power, 1996; Wilhelm et al., 2000, 2007) and Canada (Decina et al., 1990; Dennis et al., 2013). These studies have included samples in primary care or with physical health conditions, including hypertension (López-Carmona et al., 2000), diabetes (Rodríguez Moctezuma et al., 2003) and metabolic syndrome (Triviño Quintero et al., 2009), while multiple studies have also evaluated the measure in general population samples (Ramírez-Vélez and Agredo, 2012; Ramírez-Vélez et al., 2015; Rodriguez Añez et al., 2008).The measure as yet has not been explored in a sample with hospital presentations for mental health concerns or deliberate self-harm.
Previous evaluations of the scales’ psychometric properties have generally been positive, with a high test-retest reliability consistently reported (e.g. 0.91 [López-Carmona et al., 2000]; 0.92 [Rodriguez Añez et al., 2008]; 0.84 [Rodríguez Moctezuma et al., 2003]). However, previous attempts to break the scale into domains have had mixed results. The most common approach is to classify the scale into the nine domains suggested by its title (F = Family & Friends; A = Activity; N = Nutrition; T = Tobacco & Toxics; A = Alcohol; S = Sleep, Stress; T = Type of personality; I = Insight; C = Career). One study using this approach in a sample with diabetes (Rodríguez Moctezuma et al., 2003) found that while the internal consistency of the scale overall was high (Cronbach’s alpha 0.80), the nine subscales varied considerably, with Cronbach’s alpha ranging from 0.08 to 0.80, and five of the nine domains having a Cronbach’s alpha lower than 0.60, which has been suggested as the minimum threshold for acceptability of a scale (Hair et al., 1998). Similarly, a more recent study in a general population sample found that while the overall internal consistency was 0.69 [Rodriguez Añez et al., 2008], the range for the nine domains was 0.53–0.65, with Cronbach’s alpha for seven of the domains falling beneath 0.60. These findings are indicative of low homogeneity between items and suggest that implementing the scale in this way may have limited utility. As these domains are conceptual rather than based on statistical evidence, it is possible that more meaningful subscales may be determined using statistical methods.
The Green Card Clinic (GCC) at St Vincent’s Hospital Sydney is a specialist clinic for Consultation Liaison Psychiatry for patients who present at ED with deliberate self-harm and suicidal behaviours. From 2007, the GCC used the FLC and Depression, Anxiety and Stress Scales (DASS; Lovibond and Lovibond, 1995) and collected data on health status and quality of life via the 12-item Short-Form Health Survey (SF-12; Ware et al., 1996).
This study aimed to build on the existing psychometric literature on the construct validity of the FLC, and to examine internal consistency of items by assessing its factor structure when determined by statistical means, compared with the conceptual domains utilised in previous studies. The study also seeks to explore the concurrent validity of the FLC by examining its association with the 12-item Short-Form Health Survey (SF-12; Ware et al., 1996) and the DASS (DASS; Lovibond and Lovibond, 1995) and its utility in a mental health setting. The study looked at possible gender differences, as there had not been considered in the previous studies. We used data from the GCC at St Vincent’s Hospital Sydney, a specialist clinic for in Consultation Liaison Psychiatry for patients who present at ED with deliberate self-harm and suicidal behaviours.
Method
Procedure
All patients attending the ED with deliberate self-harm or suicidal ideation had a routine psychiatric examination, including a risk assessment, undertaken by psychiatry registrars. Those deemed appropriate for the GCC were given a ‘green card’ with an appointment time for the next working day and telephone crisis contact numbers. This referral process excluded people (1) admitted directly to the psychiatry unit; (2) already under care of the community mental health team or their own psychiatrist/psychologist; (3) demonstrating long-term cognitive impairment or (4) unable to speak English. Prior to clinic referral, a full medical examination had been performed in the ED. Full details of the clinic processes have been described previously (Wilhelm et al., 2000, 2007). Patients were asked to complete the study measures by the clinic receptionist on arrival to their first appointment. Participation was voluntary, and patients were provided with information forms regarding the study before consent was obtained. The study was approved by the St Vincent’s Human Research Ethics Committee.
Participants
From 2007 to 2014, of the 563 patients who attended their first appointment at the GCC (‘attenders’), a total FLC score was available for 366 participants. Demographic and clinical variables collected included age, sex, marital status, method of deliberate self-harm and psychiatric diagnosis, as well as the DASS and SF-12.
Measures
The FLC Wilson and Ciliska, 1984) is a 25-item instrument assessing 11 lifestyle domains using the acronym FANTASTIC (family, friends, activity, nutrition, toxins, alcohol, stress, sleep, personality type, insight and career). Each item is scored on a 3-point Likert scale from 0 (hardly ever), 1 (some of the time), to 2 (almost always). There is some variation in wording depending on the item and some items are reverse scored. The sum of the items yields a total score that categorises participants into four categories, where a higher score indicates more control over one’s lifestyle: 0–29 (you need to take more control over your lifestyle behaviours), 30–34 (fair), 35–41, (good) and 42–50 (you’re in control). The authors report a high test-retest correlation coefficient of 0.88 (Wilson and Ciliska, 1984) and a reasonably high internal reliability coefficient (Cronbach’s alpha) of 0.75 (Simpson et al., 1984). Within the current service, responses to the tobacco item were modified to reflect changes in smoking habits; scores now correspond to ‘daily use’, ‘occasional use’ and ‘none’, instead of ‘pipe’, ‘cigarette’ and ‘none’. The item on wearing a seatbelt was not included in the analyses as seatbelt wearing is mandatory in Australia and there was little variation in responses to this item.
The Short-Form Health Survey (SF-12; Ware et al., 1996) is a 12-item measure of health-related quality of life. It yields two-component scores; a Mental Component Score (MCS) and a Physical Component Score (PCS), which comprise eight key aspects of health status and quality of life (PCS: physical functioning, role-physical, bodily pain, general health; MCS: vitality, social functioning, role-emotional and mental health). Low scores indicate that physical or mental health problems are interfering with social and occupational functioning: 40–49 (mild level of disability), 30–39 (moderate level of disability) and <30 (severe level of disability). Together with the longer 36-item version, MCS and PCS have been shown to distinguish groups differing in the presence and severity of psychiatric and physical disorders, respectively, with median relative validity estimates at 0.97 for the MCS and 0.67 for the PCS. High test-retest (two week) correlations of 0.76 and 0.89 have been reported for the MCS and PCS respectively (Ware et al., 1996).
The Depression Anxiety and Stress Scales-21 Item Version (DASS-21; Lovibond and Lovibond, 1995) measures three negative emotional states (depression, anxiety and stress). The depression scale assesses dysphoria, hopelessness, devaluation of life, self-deprecation, lack of interest, anhedonia and inertia. The anxiety scale assesses autonomic arousal, muscle tension, situational anxiety and subjective experience of anxiety. The stress scale assesses difficulty relaxing, nervous arousal and being easily agitated, over-reactive and impatient. Respondents rate the extent to which they have experienced each state over the past week on a 4-point Likert-type scale ranging from 0 (never), 1 (sometimes), 2 (often) to 3 (almost always). The DASS has high convergent validity with other measures of depression and anxiety and a factor structure consistent with the manner in which items are allocated to subscales (Henry and Crawford, 2005).
Results
Demographics
All statistical analyses were conducted using IBM SPSS Version 21.0. The majority of the 366 participants were female (57.4%) and the mean age was 31.7 years (SD = 10.6 years, range: 17–69). Participants were predominantly single (73.5%). The most common methods of self-harm were self-poisoning/overdose (44.0%) and cutting (10.7%); other less frequent methods included hanging, gassing and jumping. Forty percent of patients presented with suicidal ideation without self-harm. The most common psychiatric diagnosis at presentation was depression (33.0%), followed by substance disorder (20.3%), adjustment disorder (14.6%) and anxiety disorder (12.6%).
Maximum Likelihood analysis
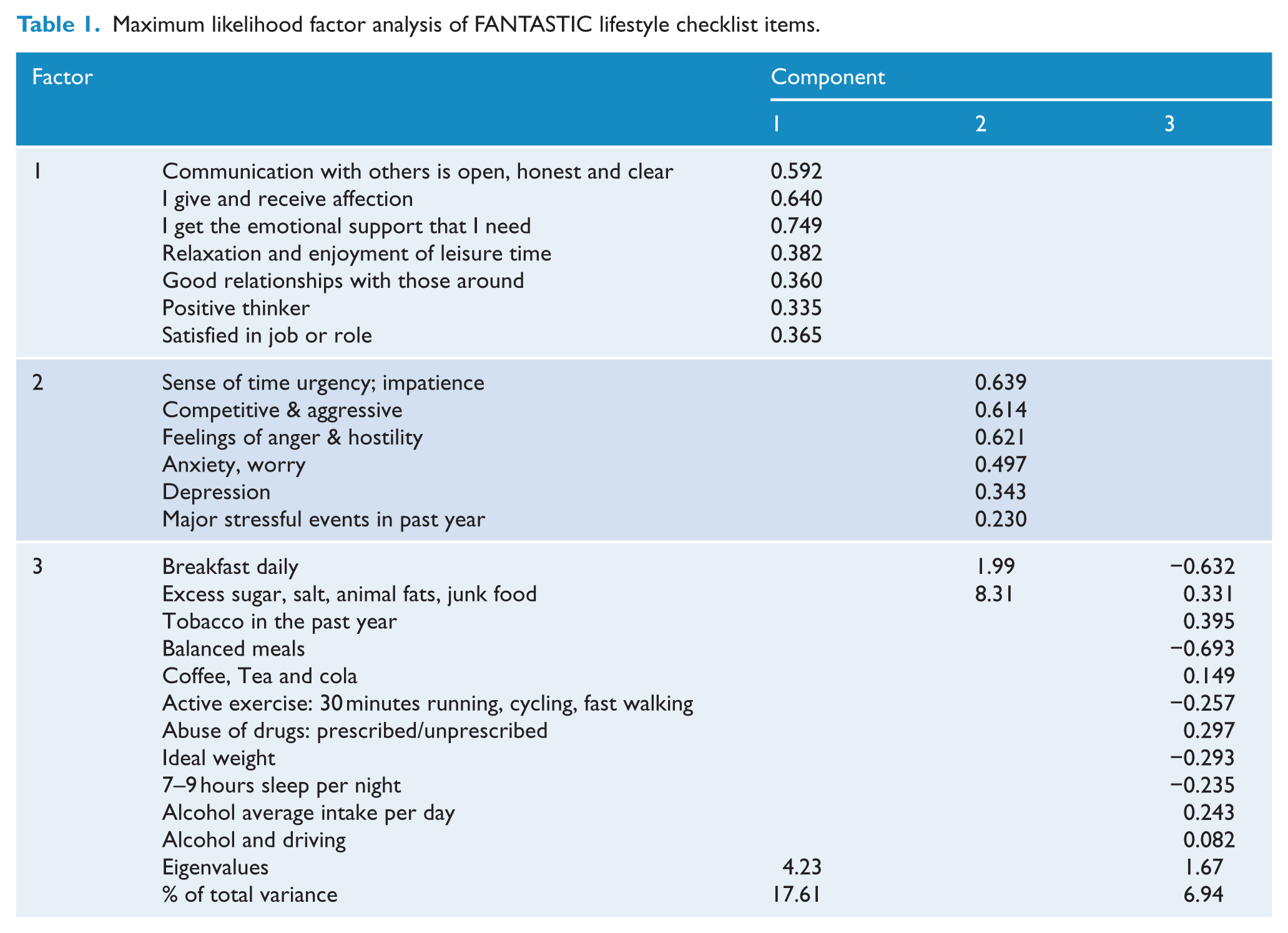
A Maximum Likelihood factor analysis was carried out on responses to the 24 FLC items to assess the factor structure (see Table 1). The Kaiser–Meyer–Oklin value (0.8) exceeded the recommended value of 0.6 and Bartlett’s Test of Sphericity reached statistical significance, supporting the factorability of the correlation matrix. The analysis revealed eight components with eigenvalues greater than 1, which together accounted for 57.3% of the variance in the scale (17.6%, 8.3%, 6.9%, 5.6%, 5.3%, 4.8%, 4.4% and 4.3% respectively). The scree plot indicated a significant loading on the first component, followed by a clear break and smaller demarcations. A forced two-component solution led to a relatively even split of the number of items loading on each factor; however, there was no discernible meaning for either factor (i.e. each factor contained both positive and negative physical and emotional behaviours). A forced four-component solution led to approximately half of items loading onto a single factor that appeared to be related to physical wellbeing, with the remaining items loading roughly evenly onto the remaining three factors; however, again the dispersion of items onto each factor appeared arbitrary. Interpretation of a three-component solution was most logical and straightforward, hence this was imposed. There was a moderate correlation between the factors produced (r = 0.4), thus an oblique rotation method (oblimin) was used to aid in interpretation of the item loadings. This solution is shown in Table 2. Component 1 was interpreted as ‘positive life investments’, Component 2 as ‘poor emotional regulation’ and Component 3 as ‘poor health behaviours’. The three components explained 17.6%, 8.3% and 6.9% of the total variance respectively.
Maximum likelihood factor analysis of FANTASTIC lifestyle checklist items.
Relationship between FANTASTIC lifestyle checklist factors and markers of mental health and wellbeing.
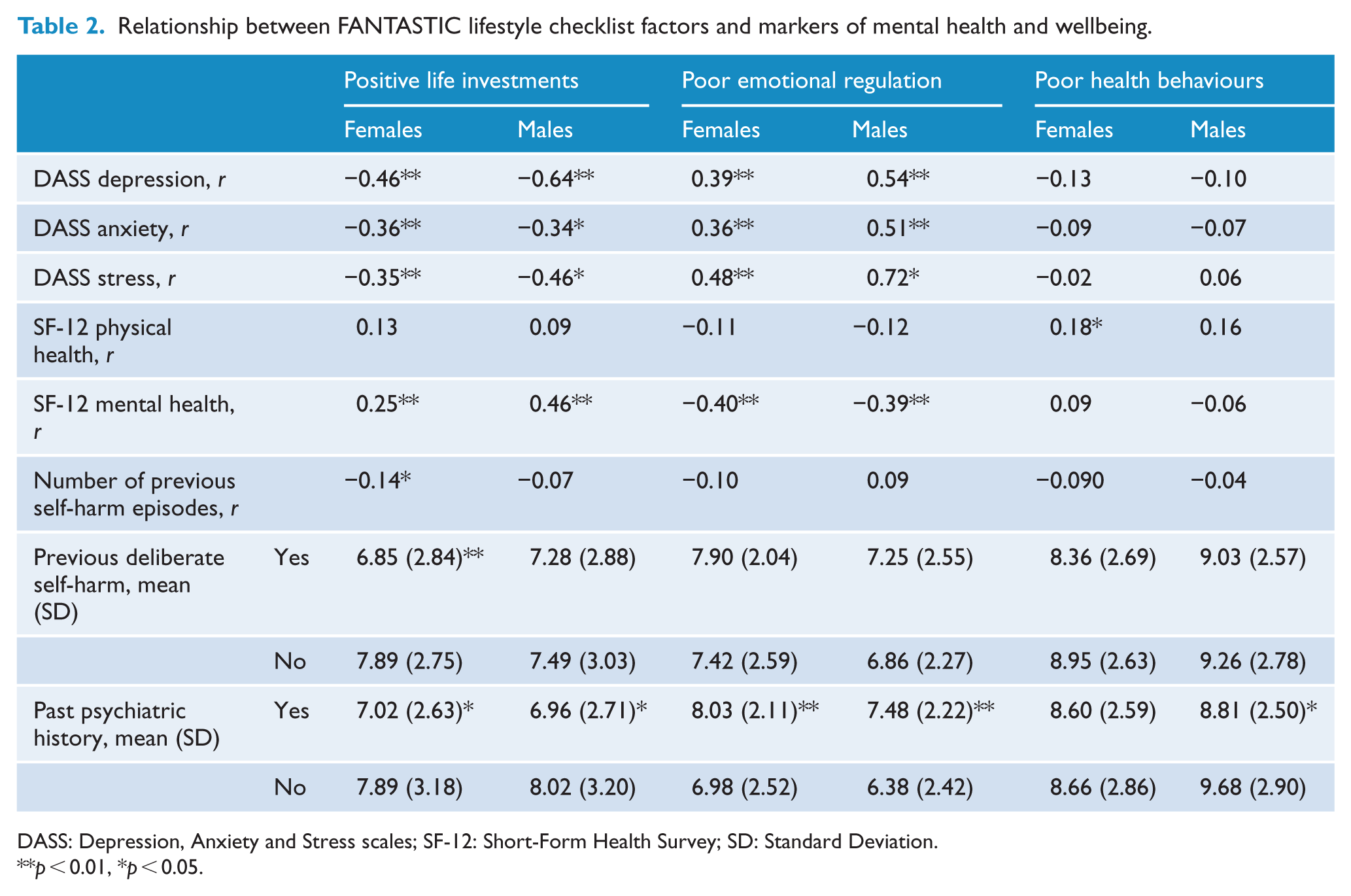
DASS: Depression, Anxiety and Stress scales; SF-12: Short-Form Health Survey; SD: Standard Deviation.
p < 0.01, *p < 0.05.
Overall, the mean score on ‘positive life investments’ was 7.36 (±2.89; range 1–14). This factor had good internal consistency (Cronbach’s alpha 0.72). ‘Poor emotional regulation’ had a mean overall score of 7.38 (±2.36; range 1–12) and good internal consistency (Cronbach’s alpha 0.70). The mean score on ‘poor health behaviours’ was 8.85 (±2.70; range 2–19); this factor also had acceptable internal consistency (Cronbach’s alpha 0.63). Although the factor loadings for some items were low, the ‘Cronbach’s alpha if item deleted’ output from SPSS showed that none of the three scales would improve in their reliability if low-loading items were removed from the scale. When the scale was analysed by the nine FANTASTIC domains used in previous research, there was high variation in the internal consistency for each domain. Cronbach’s alpha ranged from 0.08 to 0.70, with the highest internal consistency observed for ‘Family and friends’ (0.70), ‘Type of personality’ (0.69) and ‘Insight’ (0.67), while the lowest were for ‘Sleep & stress’ (0.08) and ‘Alcohol’ (0.24).
There was a weak positive correlation between age and ‘positive life investments’ (r = 0.13, p = 0.010) only. Gender had a significant relationship with both ‘poor emotional regulation’ and ‘poor health behaviours’; females reported significantly higher scores on ‘poor emotional regulation’ than males (7.67±2.31 vs. 6.99±2.37; p < 0.007), and females reported significantly lower scores on ‘poor health behaviours’ than males (8.61±2.67 vs. 9.18±2.70; p = 0.043).
Relationship with mental health variables
In light of the gender differences described above and the lack of previous studies on gender differences, further analyses were split by gender. For both males and females, there was a significant negative correlation between ‘positive life investments’ and each of the three DASS subscales, with a stronger association for males in relation to depression and stress (see Table 2). Scores for both genders on the SF-12 mental health subscales were also positively associated with ‘positive life investments’ scores, again with a stronger association for males. Females with a past history of deliberate self-harm and those with a past psychiatric history, scored lower on ‘positive life investments’ overall. This was also true for males with a past psychiatric history. There was a weak correlation between ‘positive life investments’ and the number of previous deliberate self-harm attempts for females only.
Each of the three DASS subscales was positively associated with ‘poor emotional regulation’, for both genders. Again, the magnitude of these effects was stronger for males than females. For both males and females, there was a negative correlation between ‘poor emotional regulation’ and SF-12 mental health subscale scores, with a moderate effect size. Both males and females with a past psychiatric history scored significantly higher on ‘poor emotional regulation’.
There was a weak positive correlation between ‘poor health behaviours’ and the SF-12 physical health subscale for females; no other measures were significantly associated with ‘poor health behaviours’.
Discussion
The FLC is a brief and accessible measure of lifestyle factors, initially designed to assist general practitioners in a holistic assessment of a patient’s health-related behaviours. Its simplicity and practicality has led to more widespread use but, as yet, its psychometric properties have not been assessed among patients presenting to ED with deliberate self-harm and suicidal behaviours. While the name ‘Fantastic’ is an acronym of domains covered, it may be perceived as seeming to trivialise the content of the measure, particularly in distressed populations. We therefore refer to it simply as a Lifestyle Checklist when administering to participants.
This study aimed to add to existing data on the concurrent and construct validity of the FLC by assessing its factor structure in a sample where lifestyle factors are potentially important, as well as its correlation with markers of mental health including the SF-12 and DASS. We also explored the possibility of gender differences in responses.
The data for this study were provided by people presenting to ED with suicidal behaviours or ideation and the profile of presenters was consistent with the presentation rates to hospital noted in previous research (Carroll et al., 2014). A limitation is that FLC data were cross-sectional and involved people while they were distressed and/or depressed, but not repeated on recovery. We note that all the negative affect items fell onto one factor, with health-related behaviours falling onto other separate factors. This was consistent with our clinical impression that the reported lifestyle behaviours were longer standing, rather than brought on by current distress. Participants in the clinic were easily able to complete the measure, even while in a distressed state, and usually found the measure helpful in enabling them to consider their current situation and identify areas for potential change.
The first of the three factors, positive life investment covers areas related to social support and positive life roles. All the items loaded in a positive direction and the factor had an inverse relationship to scores on self-reported negative affect. This factor was more highly endorsed by those with no previous psychiatric history or deliberate self-harm attempts. The other two factors, poor emotional regulation and poor health behaviours, showed the reverse pattern and were more likely to be endorsed by those with previous attempts and psychiatric history. This is consistent with a report from our previous sample (Wilhelm et al., 2007) where people presenting with a second or subsequent deliberate self-harm episode (repeat episode) had lower total FLC scores than those with suicidal ideation or first deliberate self-harm episode and showed significant differences in scores in relationships, activity and leisure, nutrition and alcohol use domains and were more likely to elect problem areas concerning relationships, anger/impulsivity, negative thinking patterns and the need to make life changes, which demonstrated some insight and change potential.
The items in the poor health behaviours factor relate to diet, substance use and exercise, which is relevant given the growing awareness of the effects of such lifestyle fact on mood and onset of common non-communicable conditions such as diabetes, obesity and heart disease. Most GCC attenders are in the 20–40 age range, which could be too early in life for there to be a highly significant association with these chronic diseases, but this does point to a possible pathway for early effects of lifestyle on later ill-health, as well as the potential for lifestyle-based interventions in this group.
The relationship between self-reported mental health measures and FLC factors was generally stronger for men, the only exception being the relationship between positive life investment and SF-12 mental health. There was a weak association between SF-12 physical health subscale and poor health behaviours for women only, with a similar non-significant trend for men. As this was the only factor associated with the measure of physical health, the association added to the validity of the poor health behaviours factor.
In conclusion, our findings support the construct and concurrent validity of the FLC measure. The three factors obtained were coherent and more internally consistent than the original domains and seem useful for further research and in clinical practice.
Turecki and Brent’s (2015) review noted the importance of regular follow-up of people who attempt suicide to prevent future suicidal behaviour by providing effective interventions. This will often include the need for clinicians to enable people to make positive lifestyle changes. With this in mind, the FLC seems to be a useful measure to include in routine assessments by hospitals and mental health services. The items and identified factors can enable people at a low point in their lives to make changes in their health-related behaviours with the potential to substantially improve their physical and mental health into the future.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.