
Abstract
Objective:
The risk of repetition of deliberate self-harm peaks in the first 7 days after a deliberate self-harm episode. However, thus far no studies have examined the risk factors for repeating deliberate self-harm during this short-term period. We aimed to investigate the effects of socio-demographic factors, self-harm method and mental health factors in adolescents (10–19 years old) and young adults (20–29 years old).
Methods:
We used data linkage of population-wide administrative records from hospital inpatients and emergency departments to identify all the deliberate self-harm–related episodes that occurred in adolescents and young adults in Western Australia from 2000 to 2011. Logistic regression with generalised estimating equations was used for the analyses.
Results:
The incidence of repeating deliberate self-harm within the first 7 days after an index episode was 6% (403/6,768) in adolescents and 8% (842/10,198) in young adults. Socio-demographic risk factors included female gender and socioeconomic disadvantage. Compared with non-poisoning, self-poisoning predicted increased risk of having a repeated deliberate self-harm episode in males, but not in females. Borderline personality, impulse-control and substance use disorders diagnosed within one week before and one week after an index deliberate self-harm episode conferred the highest risk, followed by depressive and anxiety disorders. Having a preceding deliberate self-harm episode up to 7 days before an index episode was a strong predictor for the future repetition of a deliberate self-harm episode.
Conclusion:
Having a repeated deliberate self-harm episode within the first 7 days was related to a wide range of factors present at an index deliberate self-harm episode including socio-demographic characteristics, deliberate self-harm method and co-existing psychiatric conditions. These factors can inform risk assessments tailored to adolescents and young adults respectively to reduce the repetition of deliberate self-harm within a short but critical period, potentially contributing to reduce the repetition of deliberate self-harm in the long term.
Keywords
Introduction
Deliberate self-harm (DSH) refers to behaviours performed directly and intentionally to cause physical or psychological destruction to oneself, regardless of suicidal intent (Hawton et al., 2012b). It is a major public health issue affecting 17% of people aged between 15–24 years (Muehlenkamp et al., 2012) and causing one in five deaths in this population (Patton et al., 2009). School-based survey studies found that approximately one in eight teenage students with DSH behaviours sought medical or emergency care (Hawton et al., 2002; Madge et al., 2008).
Studies based on medical records (e.g. hospital and emergency department) revealed that 15–16% of patients presenting for DSH had a non-fatal repeated DSH act within the first year following the initial clinical episodes, and 2% had a fatal repeated DSH act (Carroll et al., 2014; Owens et al., 2002). The repetitive nature of DSH has a strong link with subsequent suicidal death (Hawton et al., 2012b), and it also places a great burden on health and social care system (Sinclair et al., 2011). Repetition of DSH may occur more often in adolescents and young adults than people of other age groups (Zahl and Hawton, 2004).
Due to the ‘hidden’ nature of DSH behaviours, a person’s DSH behaviour usually becomes known by health professionals, when the person presents at a clinical setting such as emergency department for treatment of injuries. Therefore, clinical setting constitutes an important place where frontline services of intervention should be provided to prevent the repetition of DSH behaviours.
Previous studies that examined the risk factors for re-attendance to an emergency department or other clinical settings focussed on the repetition of a DSH episode at least 30 days after the initial DSH episode. From these studies, a range of factors have been associated with an increased risk of repeating DSH. These risk factors include socioeconomic deprivation and social fragmentation (Gunnell et al., 1995; Hawton et al., 2001), having psychiatric disorders and drug/alcohol abuse (Beghi et al., 2013; Olfson et al., 2013; Vajda and Steinbeck, 2000). Self-harm method and the degree of suicidal intent were also linked to repeating DSH (Hawton et al., 2012a). Further, having repeated DSH behaviours in the past is strongly predictive of repeating DSH in the future (Larkin et al., 2014).
Evidence based on emergency and hospital services shows that of people with a repeated DSH episode that occurred within the first year after their initial DSH episodes, more than 10% had a repeated DSH episode within the first week (Gilbody et al., 1997; Kapur et al., 2006). This incidence was found to be higher than the incidence in each subsequent week (Gunnell et al., 2002), indicating that the first 7 days after a DSH clinical episode is a critical window for interventions to be carried out to reduce the early repetition of DSH behaviours.
Further, 7 days following a discharge from an acute psychiatric unit is regarded as a vulnerable period for patients with mental health problems in Australian public mental health services (NMHWG Information Strategy Committee Performance Indicator Drafting Group, 2005). It has also been emphasised that continuity of care involving responsive community follow-up during this immediate post-discharge period plays an essential part in maintaining a patient’s clinical and functional stability and in minimising the need for early readmission.
A better understanding of the risk factors related to repeating DSH within the first 7 days can improve the capacity of community care services in delivering targeted and effective risk assessment and risk management for adolescent and young adult patients at high risk of repeating DSH. However, thus far, there has been a lack of studies with a specific focus on the risk factors for repeating DSH within the first 7 days.
In this study, we focussed on the repetition of DSH within the first 7 days following an index DSH episode in adolescents (10–19 years old) and young adults (20–29 years old). We used data linkage of population-wide administrative health records in Western Australia (WA) to examine three sets of risk factors: socio-demographic characteristics, self-harm method and mental health conditions. Because risk factors, pattern of self-harm method and suicidal intent of DSH behaviours differ between adolescents and young adults (Hjelmeland and Groholt, 2005), we conducted separated analyses for these two groups of population. Given that the risk factors for DSH vary by gender (Hawton, 2000), we also explored the gender-specific differences in the effects of each risk factor.
Methods
Linked health records
This study was based on the data linkage of population-wide administrative health records routinely collected in WA. Raw records relating to the same person were linked using probabilistic matching method by the WA Data Linkage Branch (Holman et al., 2008). Variables for linking records included name, sex, date of birth, home address and other unique identifiers such as hospital unique medical record number. Clerical checking of additional information is undertaken for possible matches that fall within a ‘grey area’ between definite matches and definite non-matches. During the linkage process, de-identified linkage keys were generated for each unique person, and we merged the records across different data collections using these linkage keys. By 1996, the proportion of invalid and missed links was both estimated at 0.11% (Holman et al., 1999; Tromp et al., 2011). More information about the data linkage in WA is on the website: www.datalinkage-wa.org/data-linkage/data-collections.
Records used for this study were sourced from the Emergency Department Data Collection (EDDC) including emergency department contacts in all hospitals under contract with the WA government, the Hospital Morbidity Data System (HMDS) including inpatient admissions (including mental health inpatients) in all hospitals in WA, the Mortality Register including all deaths registered in WA and the Mental Health Information System (MHIS) including mental health outpatients in public hospitals. Data collections date back to 2000 and earlier, except for emergency data which include records from 2002 onwards.
Study sample
We included all DSH-related records of emergency contacts, hospital inpatient admissions, and deaths that occurred among adolescents (10-19 years old) and young adults (20-29 years old) between the year 2000 and 2011 (inclusive) within WA.
Identification of valid index DSH episodes
We identified DSH-related records according to the diagnosis codes of the International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Australian Modification (ICD-10-AM). The codes are shown in the Supplementary Table 1. We followed the convention to include ‘undetermined intent’ (ICD-10-AM codes: Y10-Y34) to take into account possible misclassifications of DSH in clinical settings (Cantor et al., 2001). We referred to all the diagnostic fields in the HMDS, the EDDC, the MHIS and the Mortality Register datasets to identify DSH-related records. We also referred to two variables contained in the EDDC: ‘presenting problem’ and ‘human intent of injury’, which were coded in different systems from the ICD-10-AM. For an improved validity of the identification of DSH episodes in the EDDC data, only the episodes assigned with an injury-related ICD code (excluding injuries solely induced by assault) in addition to a DSH-related code were included in the analyses. This is because that we considered the presence of an injury as an important indicator for an actual DSH act.
The aim of this study was to explore the risk factors present at the time of a DSH episode that predicted the repetition of a DSH episode. We therefore identified the repetition of DSH within the first 7 days following a valid index episode, rather than the first episode for each unique person.
A valid index episode was defined according to the following three criteria. First, if a DSH episode occurred less than 7 days before the person’s death or the end of the study period (i.e. 31 December 2011) and this episode was not followed by any subsequent DSH episodes, such an episode was not considered as a valid index episode (removing 38 records). This criterion ensures that there were at least 7 days after each valid index episode to allow for the identification of a repeated DSH episode. Second, a death record was not considered as a valid index episode (removing 898 death records), because no subsequent DSH episodes can occur. Last, when a person was transferred from an emergency department to an inpatient care unit following the same DSH behaviour, we considered such ‘transfer-bonded’ episode pairs as one valid episode. There were a total of 1,365 transfer-bonded episode pairs, and we only used the inpatient episodes for the data analysis, because inpatient data were generally thought to have a better quality than emergency data.
In total, we identified 16,966 valid DSH episodes. Of these episodes, 13,336 (78.60%) were identified from the emergency data (i.e. EDDC), and 3,595 (21.19%) from the hospital inpatient data (i.e. HMDS). The remaining episodes were from mental health episodes (i.e. MHIS). For emergency episodes, we used the ‘presentation date’ as the starting time point to determine the 7-day window for the repetition. For hospital inpatient episodes, we used the ‘admission date’, rather than the discharge date to determine the 7-day repetition window. More information is in the Supplementary Table 2.
Identification of risk factors
Socio-demographic factors
We identified socio-demographic factors, which included sex, Aboriginality, neighbourhood socioeconomic disadvantage, and remoteness of residence recorded in each index DSH episode (Figure 1). The indices for neighbourhood socioeconomic disadvantage and remoteness of residence are developed by the Australian Bureau of Statistics (2008; The National Centre for Social Applications of GIS [GISCA], The University of Adelaide, 2004). The index score of neighbourhood socioeconomic disadvantage combines a range of factors such as household income, educational attainment and employment status of people residing in a small area that contains approximately 250 dwellings (Australian Bureau of Statistics, 2008). We used the quartiles of the score of the neighbourhood socioeconomic disadvantage, with a lower quartile representing a higher level of socioeconomic disadvantage. The remoteness of residence reflects the geographic accessibility to services in an area (unrelated to socioeconomic status, rurality and population size) (GISCA, The University of Adelaide, 2004). This index contains four levels of area, which are major cities, inner regional areas, outer regional areas and remote/very remote areas.
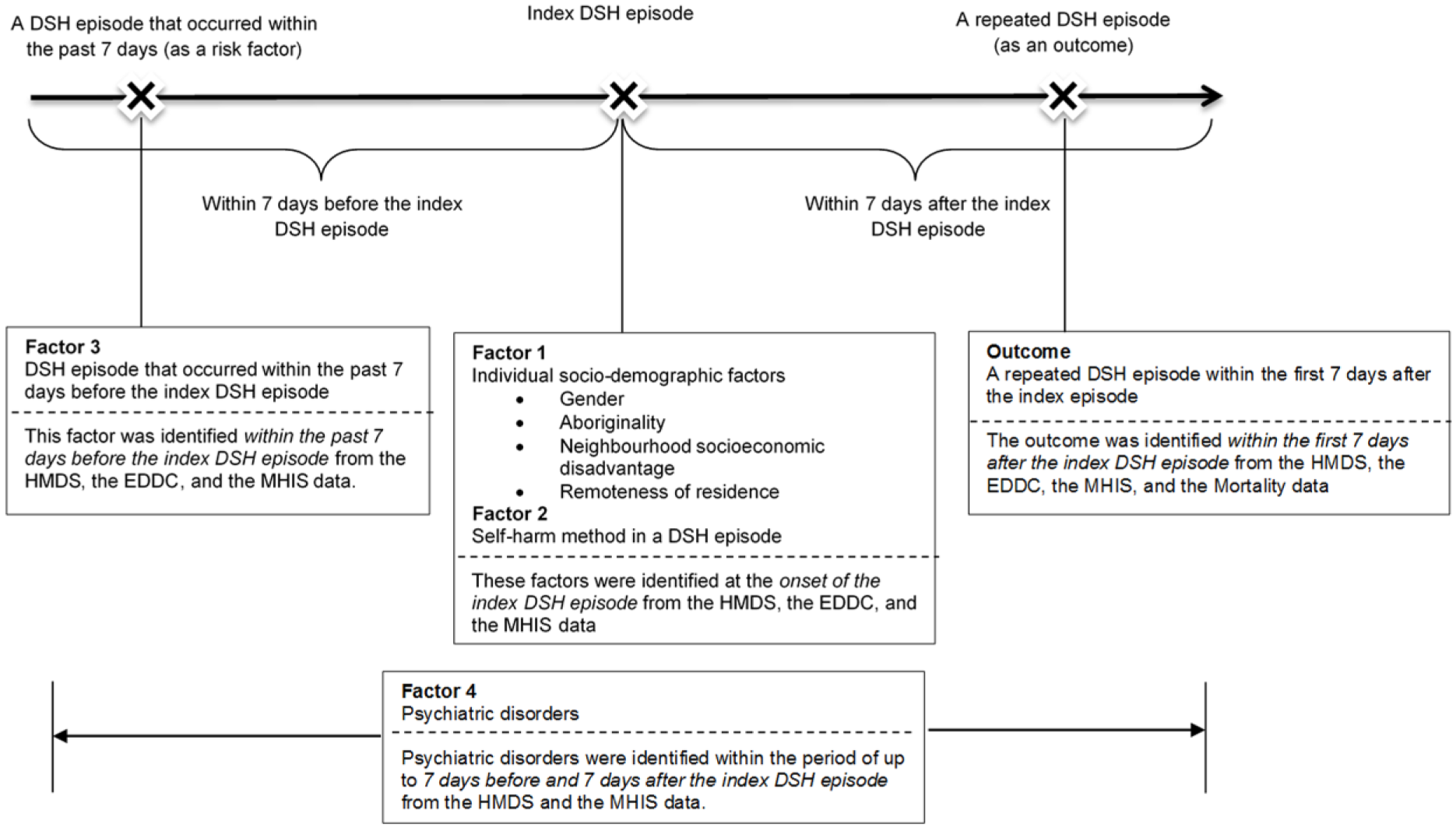
Identification of risk factors.
Self-harm method
We used the ICD-10-AM external cause codes and the presenting problem codes (EDDC) to identify self-harm method (Supplementary Table 1). First, we classified all episodes into self-poisoning vs non-poisoning episodes. For non-poisoning episodes, the predominant method was self-cutting. Second, for all self-poisoning episodes, they were further classified into three sub-categories: self-poisoning with drug/medication, with other substance and with unspecified substance. Last, all drug/medication-related self-poisoning episodes were classified into illicit drug use vs non-illicit drug use.
Mental health conditions
Co-existing psychiatric disorders
Previous studies have found that co-existence of severe psychiatric disorders at the time of DSH behaviours was a strong predictor for the future repetition of DSH behaviours (Hawton et al., 2003). Further, there was a possibility that patients’ pre-existing psychiatric disorders were discovered or diagnosed because of their presence at a clinical setting for DSH behaviours. Therefore, we identified any records of psychiatric diagnosis within 7 days before and 7 days after a valid index DSH episode as a proxy for the co-existence of psychiatric disorders. We identified co-existing psychiatric disorders from the MHIS and HMDS data according to ICD-10-AM codes (Supplementary Table 1). We also identified major types of psychiatric disorders, including substance use disorders, psychotic disorders, bipolar disorders, depressive disorders, anxiety disorders, stressor-related disorders, impulse-control disorders and borderline personality disorder (BPD).
Having a preceding DSH episode up to 7 days before an index episode
Additionally, we were interested in whether and how having a preceding DSH episode up to 7 days before an index episode may predict the future repetition up to the next 7 days following an index episode. This recent history may confer an important message for mental health crisis and hence may strongly predict repeating DSH within the next 7 days.
Data analysis
The prevalence of repeating DSH within the first 7 days following an index episode was calculated for each risk factor. Logistic regression analysis was undertaken to estimate the crude and adjusted odds ratios (ORs) for repeating DSH associated with each factor. Crude ORs were derived from univariate logistic regression models and adjusted ORs were generated from multivariate logistic models including all the factors examined in this study.
To adjust for the clustering of DSH episodes within a same person, logistic regression analyses with generalised estimating equations (GEE) were conducted. Because the association between DSH episodes may gradually decay with an increasing interval between the episodes, we specified the first-order autoregressive structure for the working correlation matrix (Fitzmaurice et al., 2004). Standard errors of regression coefficients were obtained from the empirical estimation. Zeger et al. (1988) found that the empirical estimation can yield robust standard errors even when the working correlation matrix has been mis-specified.
Furthermore, we used multivariate negative binomial regression analysis to estimate the association between having a repeated DSH episode within the first 7 days following an index episode (binary) and the total number of valid DSH episodes. We included Pearson scale parameter to address over-dispersion.
All the analyses were conducted separately for adolescents and young adults, as well as separately for males and females. We used generalised score tests for Type III GEE analysis to examine the significance of the differences in the effects of the risk factors between adolescents and young adults, as well as between males and females. P-value < 0.05 was considered as statistical significance for all the analyses. Data management and analyses were carried out using SAS® (EG) statistical software version 6.1 (SAS Institute Inc., Cary, NC, USA).
Results
Table 1 shows that a total of 6,768 valid DSH episodes in adolescents (2,123 in males, 4,645 in females) and 10,198 valid episodes in young adults (4,450 in males, 5,748 in females) were identified between the year 2000 and 2011. The prevalence of repeating DSH within the first 7 days after a DSH episode was 8.26% (842 repeated episodes) in young adults, which was significantly higher (p < 0.0001) than the prevalence of 5.95% (403 repeated episodes) in adolescents.
Gender-specific number of valid DSH episodes and percentage for having a repeated DSH episode within the first 7 days after an index DSH episode by socio-demographic factors, self-harm methods and mental health-related factors among adolescents and young adults.
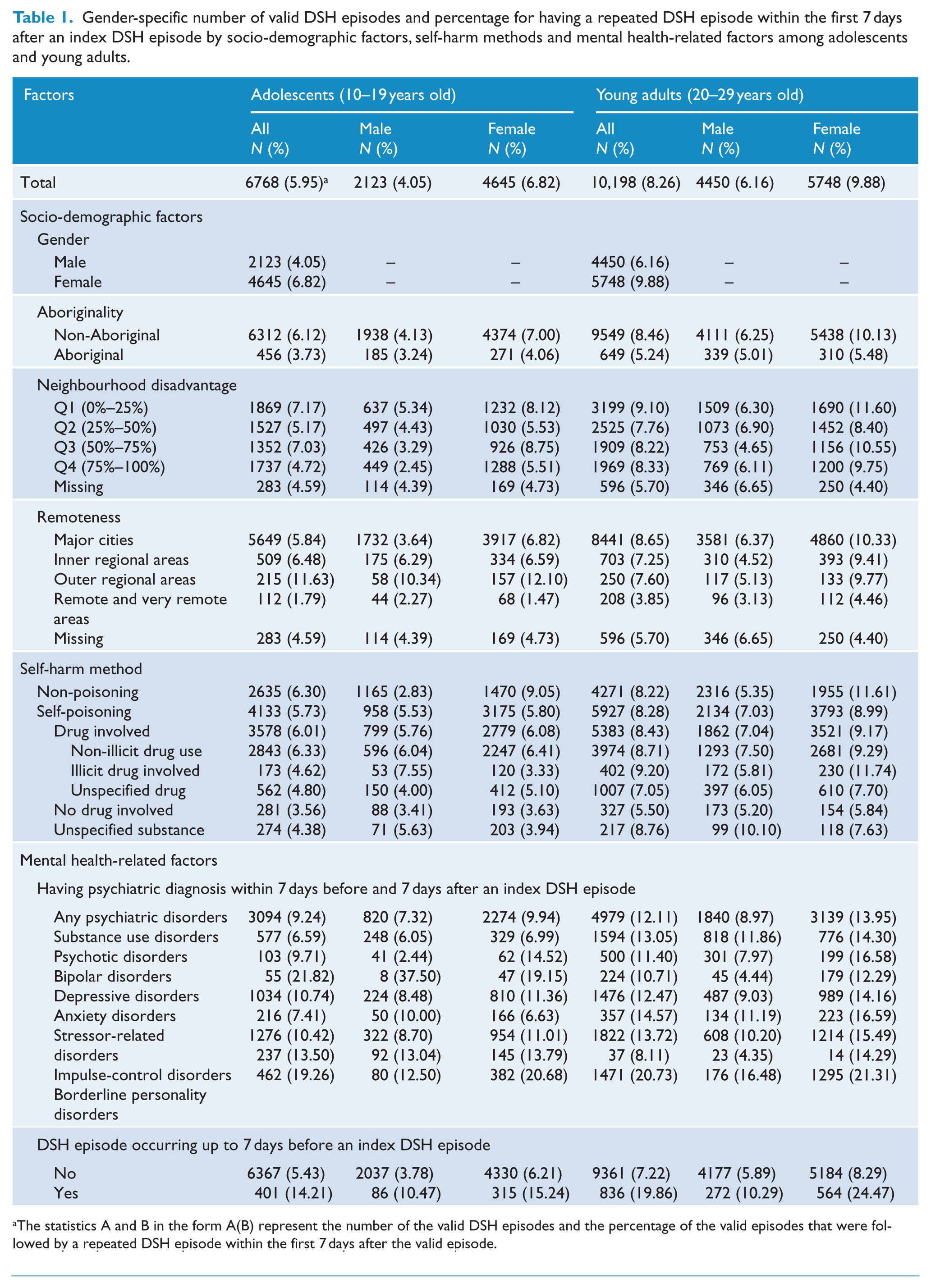
The statistics A and B in the form A(B) represent the number of the valid DSH episodes and the percentage of the valid episodes that were followed by a repeated DSH episode within the first 7 days after the valid episode.
In the following paragraphs, we showed the effects of all the factors for males and females separately in the Table 2. Because the effects of mental health-related factors were also found to differ significantly between adolescents and young adults, we further showed the effects for adolescents and young adults separately in the Table 3.
Gender-specific association between having a repeated DSH episode within the first 7 days after an index DSH episode and socio-demographic factors, self-harm method and mental health related factors in adolescents (10–19 years old) and young adults (20–29 years old).
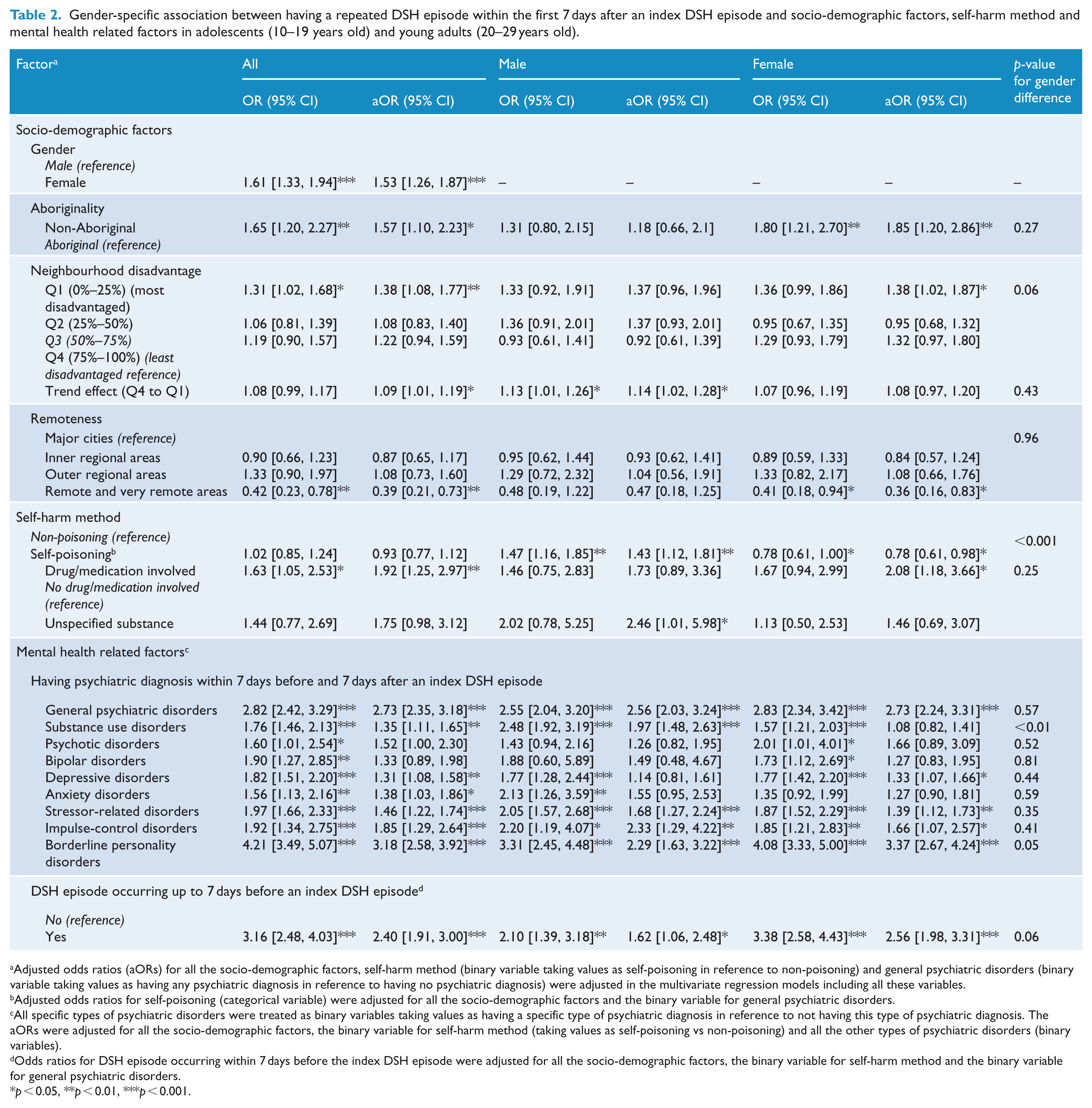
Adjusted odds ratios (aORs) for all the socio-demographic factors, self-harm method (binary variable taking values as self-poisoning in reference to non-poisoning) and general psychiatric disorders (binary variable taking values as having any psychiatric diagnosis in reference to having no psychiatric diagnosis) were adjusted in the multivariate regression models including all these variables.
Adjusted odds ratios for self-poisoning (categorical variable) were adjusted for all the socio-demographic factors and the binary variable for general psychiatric disorders.
All specific types of psychiatric disorders were treated as binary variables taking values as having a specific type of psychiatric diagnosis in reference to not having this type of psychiatric diagnosis. The aORs were adjusted for all the socio-demographic factors, the binary variable for self-harm method (taking values as self-poisoning vs non-poisoning) and all the other types of psychiatric disorders (binary variables).
Odds ratios for DSH episode occurring within 7 days before the index DSH episode were adjusted for all the socio-demographic factors, the binary variable for self-harm method and the binary variable for general psychiatric disorders.
p < 0.05, **p < 0.01, ***p < 0.001.
Gender-specific association between having a repeated DSH episode within the first 7 days after an index DSH episode and psychiatric diagnosis within 7 days before and 7 days after an index episode in adolescents (10–19 years old) and young adults (20–29 years old) respectively.
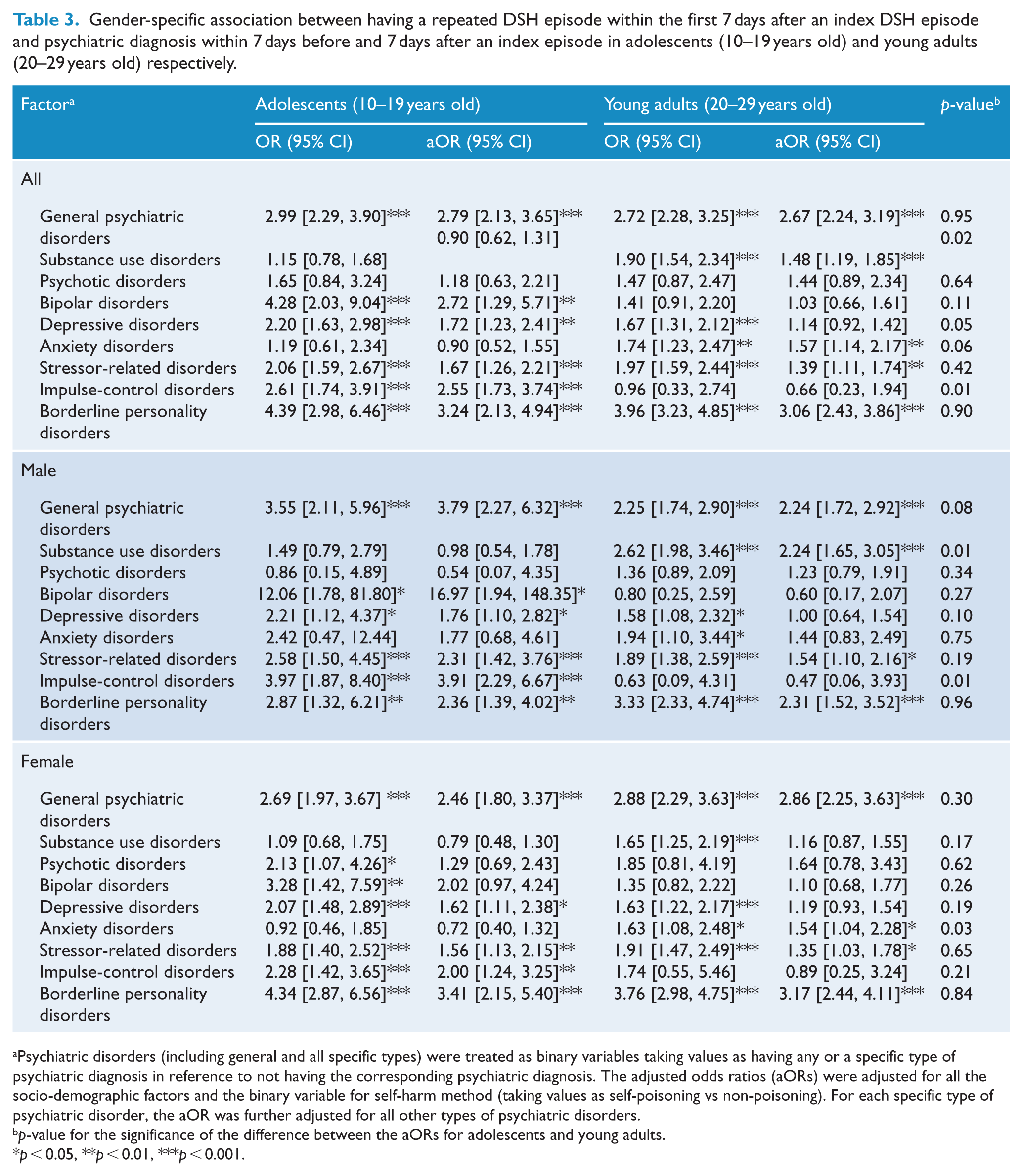
Psychiatric disorders (including general and all specific types) were treated as binary variables taking values as having any or a specific type of psychiatric diagnosis in reference to not having the corresponding psychiatric diagnosis. The adjusted odds ratios (aORs) were adjusted for all the socio-demographic factors and the binary variable for self-harm method (taking values as self-poisoning vs non-poisoning). For each specific type of psychiatric disorder, the aOR was further adjusted for all other types of psychiatric disorders.
p-value for the significance of the difference between the aORs for adolescents and young adults.
p < 0.05, **p < 0.01, ***p < 0.001.
Socio-demographic risk factors
Table 2 shows that the odds of repeating DSH within the first 7 days following a DSH episode in females were higher than males by 53% (95% CI = [26, 87]). Non-Aboriginality was a significant risk factor for females only, and the odds of repeating DSH within 7 days in non-Aboriginal females was higher than Aboriginal females by 85% (95% CI = [20, 186]).
Compared with living in the least disadvantaged areas, living in the most disadvantaged areas was associated with a 38% (95% CI = [8, 77]) increase in the odds of repeating DSH within 7 days following a DSH episode. The trend effect showed an average of 9% (95% CI = [1, 19]) increase in the odds of repeating DSH within 7 days with each increment in the quartile scale of socioeconomic disadvantage. Compared with residence in other regions, residing in remote areas was associated with a significant decrease in the odds of repeating DSH within 7 days (Table 2).
Self-harm method
Table 1 shows that self-poisoning was involved in around two-thirds of all the valid DSH episodes in females, and it was less common in males (45%). Drug/medication was ingested in nearly 90% of all self-poisoning episodes.
Table 2 shows that compared with non-poisoning episodes, self-poisoning episodes were associated with a significantly increased odds of repeating DSH within 7 days in males (aOR = 1.43, 95% CI = [1.12, 1.81]), but a significantly decreased odds in female adolescents (aOR = 0.66, 95% CI = [0.50, 0.87]), and had no significant effect in female young adults. Table 2 further shows that for self-poisoning episodes, drug/medication use was associated with a two-fold increase in the odds of repeating DSH within 7 days (aOR = 1.92, 95% CI = [1.25, 2.97]), compared with no drug/medication episodes.
For self-poisoning episodes by drug/medication, we did not find a significant difference in the effects of illicit drug use vs non-illicit drug use on repeating DSH within 7 days (aOR = 0.89, 95% CI = [0.62, 1.29]).
Mental health-related risk factors
Psychiatric disorders at the time of an index DSH episode
Table 1 shows that 45.7% of valid index DSH episodes in adolescents and 48.8% in young adults occurred with a psychiatric diagnosis recorded within 7 days before and 7 days after the DSH episodes. For both adolescents and young adults, stressor-related disorders, depressive disorders and substance use disorders were the most common psychiatric disorders. Borderline personality disorder (BPD) was common in females, particularly for female young adults. For males, impulse-control disorders were common for adolescents and psychotic disorders were common for young adults.
Table 2 shows that having co-existing psychiatric diagnosis within one week before and one week after a DSH episode was associated with a 2.73-fold (95% CI = [2.35, 3.18]) increase in the odds of repeating DSH within 7 days, compared with having no psychiatric diagnosis within this period. Table 3 shows that the magnitude of this association was highest in male adolescents.
Table 3 shows that having BPD within one week before and one week after a DSH episode was associated with a three-fold increase in the odds of repeating DSH within the first 7 days, compared with having no diagnosis of BPD. This association was equally strong in adolescents and young adults, but stronger in females (aOR = 3.37, 95% CI = [2.67, 4.24]) yet non-significantly (p = 0.05) than in males (aOR = 2.29, 95%CI = [1.63, 3.22]). The presence of stressor-related disorders also had a similar effect for adolescents (aOR = 1.67, 95% CI = [1.26, 2.21]) and young adults (aOR = 1.39, 95% CI = [1.11, 1.74]).
Table 3 shows that having impulse-control disorders was associated with a four-fold increase in the odds of repeating DSH within 7 days in male adolescents (aOR = 3.91, 95%CI = [2.29, 6.67]), which doubled the OR for female adolescents (aOR = 2.00, 95%CI = [1.24, 3.25]). However, this gender-specific difference in the effects did not reach statistical significance (p = 0.10). Having depressive disorders was related to a 1.72-fold increase in the odds of repeating DSH in adolescents (aOR = 1.72, 95%CI = [1.23, 2.41]), but not in young adults (aOR = 1.14, 95% CI = [0.92, 1.42]).
Having substance use disorders within one week before and one week after a DSH episode only had a significant effect in male young adults (aOR = 2.24, 95% CI = [1.65, 3.05]), which was significantly higher than the effects in females and male adolescents (p < 0.01).
Having psychotic disorders did not show to have a significant effect on repeating DSH within 7 days.
Having a preceding DSH episode up to 7 days before an index episode
Having a preceding DSH episode within the last 7 days prior to a DSH episode was associated with a 2.4-fold (95% CI = [1.91, 3.00]) increase in the odds of repeating DSH within the next 7 days of a DSH episode. Additionally, individuals who ever had a repeated DSH episode within the first 7 days following a DSH episode had a total number of DSH episodes, which was triple the number of DSH episodes among those who did not (p < 0.0001). This association was significantly stronger (p < 0.0001) in females (3.6-fold) than males (2.2-fold).
Discussion
To our knowledge, there were no studies with a specific focus on risk factors contributing to repeating DSH within the first 7 days following a DSH episode in adolescents and young adults. In this study, we showed that socio-demographic factors, DSH method, mental health conditions at the time of a DSH episode were all associated with the risk of repeating DSH within the first 7 days in adolescents and young adults. Our results also displayed several significant differences in the effects of these risk factors between adolescents and young adults, as well as between males and females. These findings can inform risk assessments aimed at reducing the repetition of DSH within a short but critical period, potentially contributing to reduce the repetition of DSH in the long term.
We found that young adults were at a higher risk for repetition of DSH episodes than adolescents, and females at higher risk than males. Previous studies also found that young adults and females were both at high risk of repeating DSH over the period longer than 7 days (Perry et al., 2012).
Living with socioeconomic disadvantage predisposes a person to initiate and maintain DSH behaviours (Payne et al., 2009). Our findings further showed that higher socioeconomic disadvantage was related to increased risk of repeating a DSH episode within the first 7 days following a DSH episode. This may be partially attributed to mental health issues and victimisation that accompany socioeconomic disadvantage, which hasten the recurrence of DSH episode. Further, it was suggested that people living with a higher socioeconomic disadvantage may have a lower access to mental health services and a poorer quality of care (e.g. lower volumes of services or less highly trained service providers) (Meadows et al., 2015).
In the current clinical practice, self-harm method and substance use are commonly used in the risk assessment for repeating DSH (Cooper et al., 2006; Corcoran et al., 1997; Steeg et al., 2012). Our study showed that different DSH methods may differently predict the risk of having a repeated DSH episode within the first 7 days for males and females. Most notably, compared with non-poisoning methods, self-poisoning was linked to a decreased risk in female adolescents, but an increased risk in male adolescents and young adults. Previous studies found that self-poisoning was related to a decreased risk of repeating DSH (Bilen et al., 2011; Hawton et al., 2012a); however, these findings were based on combined samples including males and females despite the majority of the DSH episodes occurring in females, thus masking a potentially important gender difference. Additionally, we did not find that illicit drug use increased the repetition of DSH within the first 7 days, although it may predict repeating DSH in a longer term (Haw et al., 2007).
A possible explanation for the decreased repetition of a DSH episode within the first 7 days related to non-poisoning vs self-poisoning method in males is that non-poisoning DSH method may very likely indicate DSH behaviours of more violent and lethal nature (e.g. cutting, exposure to gas) in males than in females (Harrison and Henley, 2014). Therefore, non-poisoning DSH methods may imply more serious resulting injuries that require critical and hence a prolonged hospitalised care in males, which may consequently delay the occurrence of a repeated DSH episode. This interpretation for the relationship between non-poisoning DSH method and reduced repetition of a DSH episode within the first 7 days may also be applied to some other findings in this study. For example, repeating DSH was significantly reduced in remote areas in Australia, where highly lethal methods were more commonly used in DSH behaviours, compared with other areas (Harrison and Henley, 2014). Similarly, this may also explain the reduced repetition of a DSH episode observed in Aboriginal females, because violent methods were more commonly used in DSH behaviours among Aboriginal people than their non-Aboriginal peers, particularly for females (Harrison and Henley, 2014).
Our results showed that co-existing psychiatric disorders within one week before and one week after a DSH episode predicted highly increased risk of repeating DSH within the first 7 days. We found that having BPD, impulse-control disorders (in adolescents) and substance use disorders (in male young adults) conferred the highest risks for repeating DSH within 7 days. These disorders are marked by an impaired self-control of emotions, which predisposes a person to impulsive and aggressive behaviours such as DSH (Evans et al., 1996). Substance use disorders only had a significant effect in male young adults, which underlines the need to provide drug and alcohol treatment services immediately after a DSH episode for a male with substance use disorders.
Additionally, psychiatric disorders with more internalising symptoms such as depressive disorders (in adolescents) and anxiety disorders (in female young adults) also carried significant risks for repeating DSH within the first 7 days. These internalising disorders, however, had a smaller effect than that of externalising disorders as discussed above, which may be because that internalising disorders have chronic than acute influence (Hawton et al., 2003; McMillan et al., 2007). We did not find strong evidence for significant gender-specific differences in the effects of psychiatric disorders such as borderline personality disorders and impulse-control disorders. This may be due to small sample size for sub-groups of population (e.g. males for BPD). More research is needed to validate these gender differences.
Finally, we found that people who had a preceding DSH episode at a clinical presentation were more likely to repeat a DSH episode in the next 7 days. Additionally, we found that for people with a DSH episode, the total number of DSH episodes (during the study period) among those who had a repeated DSH episode within the first 7 days was triple the total number of DSH episodes among those who did not. These findings may have implied that to reduce the repetition of DSH within the first 7 days is important to the prevention of repeating DSH in a longer period of time.
Strengths and limitations
The linkage of population-wide administrative health records has the following strengths. First, DSH episodes were drawn from whole population, thus a large sample size could be obtained for the examination of a rare event, such as DSH episode within 7 days. Second, administrative data enable the exploration of a wide range of risk factors. Third, the record linkage allows for longitudinal analysis, and the linkage of the records from multiple sources provides a more accurate and complete picture of the trajectory leading to the repetition of DSH. Fourth, data were collected objectively using standardised clinical diagnoses (e.g. ICD-10-AM codes) by clinical personnel, and this ensures the validity of the diagnosis of psychiatric disorders and the identification of DSH episodes and the self-harm methods.
There were also some limitations in this study. First, approximately 80% of the DSH records were sourced from emergency departments and 20% from hospital inpatient units. Pharmaceutical data and records from general practice and private clinics were unavailable in the data linkage. Therefore, our findings are specifically generalisable to adolescents and young adults who presented at an emergency department with DSH-related injuries or psychiatric conditions that were more clinically critical. Second, while suicidal intent, stressful life event and family dysfunction are important predictors for repeating DSH (Harriss et al., 2005; Keeley et al., 2003), we were unable to include these factors in this study due to the lack of such information in the data linkage. Third, although we could identify a transfer to hospital inpatient care after an emergency episode, other health service use following the discharge from an emergency unit was unknown. This warrants an important direction in future studies about the types of healthcare service (e.g. hospital inpatient care, community mental health service) that may deliver the most cost-effective interventions in reducing the re-occurrence of DSH behaviours within the first 7 days after an index episode.
Implications
A recent Danish study has demonstrated that psychosocial assessment and intervention are promising in reducing the risk of subsequent DSH behaviour and fatal outcomes of DSH both in the short-term and long-term for general population (Erlangsen et al., 2015). Our study has found that socio-demographic factors, self-harm method and mental health issues (e.g. co-existing psychiatric disorders and mental health crisis) were closely related to repeating DSH within the first 7 days after a DSH episode. Therefore, these risk factors should be carefully considered in psychosocial assessments to predict and hence intervene the repetition of DSH within an immediate post-discharge period. Our results highlighted the need to focus on different factors in the risk assessment for adolescents and young adults, as well as for males and females. Before being discharged from an emergency department or hospital inpatient unit, patients should receive a systematic psychosocial assessment, responsive follow-up involving drug and alcohol treatment if substance use problems are identified and evaluation of mental health conditions such as co-existing psychiatric disorders and mental health crisis that is present within the past week of an index DSH episode. Further, social interventions and care targeted at reducing social and economic adversities and promoting the access to health and social supports are vital for preventing the repetition of DSH in the short term.
Conclusion
In this study, we demonstrated that socio-demographic factors, DSH method and psychiatric conditions all predicted the repetition of DSH within the first week after an index DSH episode in adolescents and young adults. These factors have different impacts for adolescents and young adults, and for females and males. Our findings can inform the future development of psychosocial risk assessment that is tailored to adolescents and young adults and aimed at reducing the repetition of DSH within a relatively short but critical period, which may also have the potential to reduce repeating DSH in the long term.
Footnotes
Acknowledgements
We acknowledge the partnership of the Western Australian Government Department of Health, who provided support as well as data for this project. We also acknowledge the Western Australian Data Linkage Branch for linking the records. This article does not necessarily reflect the views of the government department. This study was supported by the Australian Research Council Linkage Project grant (LP100200507).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
This study was approved by the Human Research Ethics Committee of the Department of Health in Western Australia and the University of Western Australia Human Research Ethics Office. As part of a large study which also includes Aboriginal people in Western Australia, this study was also approved by the Western Australian Aboriginal Health Ethics Committee. Participation consent form is not required for this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Australian Research Council Linkage Project grant (LP100200507). The funders had no role in the study design, data collection, analysis, data interpretation, or writing of the report.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.