
Abstract
Objectives:
There is accumulating evidence about effectiveness of a number of suicide prevention interventions, and a multilevel systems approach seems promising in reducing suicide risk. This approach requires that components ranging from individual-level to public health interventions are implemented simultaneously in a localised region. This paper presents estimated reductive effects on suicide attempts and deaths that might be expected in Australia if active components of the systems approach were to be implemented.
Method:
The study estimated population preventable fractions which indicate the extent to which suicide attempts and deaths might be decreased if the each of the proposed interventions was fully implemented. The population preventable fractions were based on the best available evidence available in the literature for the risk ratio for each intervention. Prevalence estimates were assessed for each component of the proposed systems approach: reducing access to suicide means, media guidelines, public health campaigns, gatekeeper programmes, school programmes, general practitioner training, psychotherapy and co-ordinated/assertive aftercare.
Results:
There was insufficient evidence available for the impact of a number of strategies, including frontline staff gatekeeper training, on either suicide attempts or deaths. Taking prevalence of exposure to the intervention into consideration, the strategies likely to bring about the strongest reduction in suicide attempts were psychosocial treatments and co-ordinated/assertive aftercare. The greatest impact on reductions in suicide deaths was found for psychosocial treatment, general practitioner training, gatekeeper training and reducing access to means of suicide.
Conclusion:
The evidence regarding the overall efficacy of the systems approach is important in identifying what strategies should be prioritised to achieve the biggest impact. The findings of the population preventable fraction calculations indicate that the systems approach could lead to significant reduction in suicide attempts and suicide deaths in Australia. Potential synergistic effects between strategies included in the approach could further increase the impact of implemented strategies.
In 2013, 2522 people died by suicide in Australia, and an estimated 65,000 made an attempt (Australian Bureau of Statistics [ABS], 2015b; Johnston et al., 2009). Australia’s suicide rate (approximately 11 per 100,000) has remained stubbornly consistent over the last decade or more (ABS, 2015b). Moreover, it exceeds that of some European countries, including the United Kingdom, the Netherlands, Spain and Switzerland (World Health Organization [WHO], 2014).
Recently, there have been significant changes, globally, to suicide prevention by researchers and policy makers. First, evidence is accumulating about the effectiveness of a number of suicide prevention interventions (Mann et al., 2005). Second, a new idea has emerged that a multilevel, multifactorial systemic approach is needed to comprehensively reduce suicide risk (Hegerl et al., 2013; While et al., 2012). This approach requires that components ranging from public health interventions to individual-level interventions are implemented simultaneously in a localised region. While many of these suicide prevention strategies have been individually implemented in Australia, no attempt has been made to simultaneously combine these strategies using a systems approach framework.
As a systems approach to suicide prevention has not yet been implemented in Australia, the present paper attempts to estimate the reductive effects on suicide deaths and attempts that might be expected if active components of a systems approach were to be implemented. The method involves three steps. First, nine evidence-based suicide prevention strategies were identified: reducing access to lethal means, responsible media reporting, community awareness programmes, gatekeeper training, school-based suicide prevention programmes, training of general practitioners and frontline staff, psychotherapy and follow-up for individuals with a recent suicide attempts (Calear et al., 2015; Mann et al., 2005; Van der Feltz-Cornelis et al., 2011). Second, the size of the effect of each of these strategies were estimated using existing risk ratio (RR) estimates for suicide deaths and suicide attempts. Third, the extent to which each of these strategies will reach the communities so that they can have impact (the prevalence) was estimated. These two estimates were used to calculate the population preventable fractions (PPFs, analogous to Population Attributable Risk, PAR), which indicate the extent to which suicide attempts/deaths might be decreased if the each of the proposed systems-based interventions was fully implemented. The ultimate goal of the paper is to provide policy makers and community organisations with evidence-based information that will help set priorities.
Method
Existing literature was used to estimate PPF for each intervention. Using the best available estimates of risk ratio relating to either suicide deaths or suicide attempts and proportion exposed, the PPF was calculated (Rockhill et al., 1998). The PPFs were based on the best available evidence for the risk ratio (RR) for each intervention provided in the literature. The best available evidence for the RR estimate for each component was chosen from a meta-analysis when available. When no meta-analysis was available, a multicentre randomized controlled trial (RCT) or systematic review was chosen as the data source. If none of these was available, a single study with a large sample size and clear reporting of RR was selected.
Prevalence estimates were assessed uniquely for each component as follows (Table 1): Reducing access to means: the proportion of suicide attempts/deaths attributed to self-poisoning, Media Guidelines the proportion of the population exposed to media, Public Health Campaigns: the proportion of residents reached by a flyer campaign; Gatekeeper programmes: assumption that gatekeeper programmes could be established in 20% of workplaces, with 52.5% of the target population in employment; School Programmes: the proportion of residents that are school-aged combined with an assumption that 50% of schools would agree to participate in such a programme; General practitioner (GP) training: the proportion of suicidal people who receive primary care treatment; Psychotherapy: based on an increase in the proportion of suicidal people who receive mental health care from 31.6% to 50%; and Co-ordinated and assertive aftercare: the proportion of people who attempt suicide that reach an emergency department. There was insufficient evidence for frontline training as current studies only examined the effect of training on knowledge and attitudes, not on suicidal deaths or attempts. This paper rests on the requirement that data are available on the expected size of the effect to allow modelling, an assumption that was not met for a number of the strategies.
Estimated population preventable fraction for each of the strategies in the systems approach.
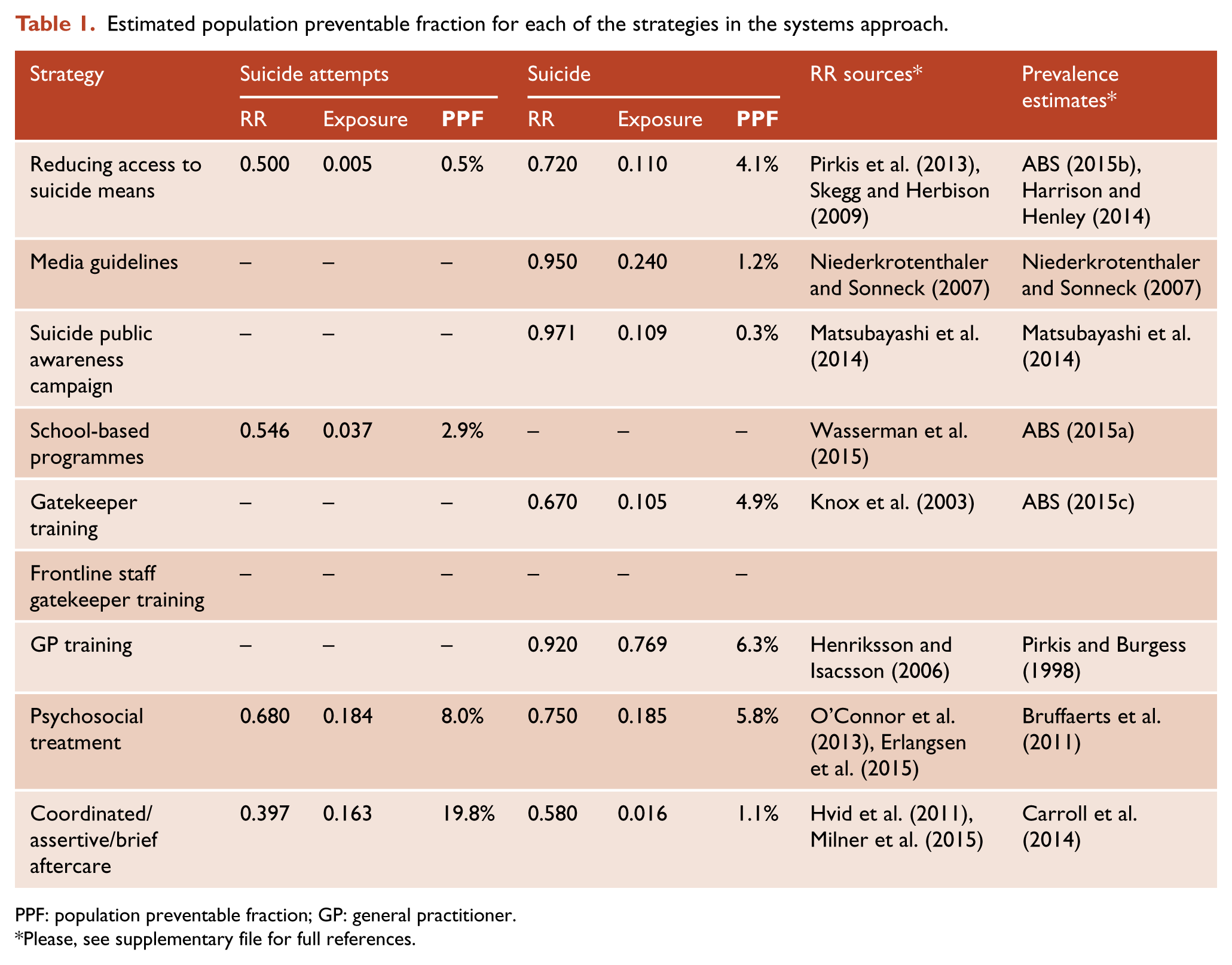
PPF: population preventable fraction; GP: general practitioner.
Please, see supplementary file for full references.
Results
Estimates of PPF are provided in Table 1, with references to the source of the RR data. Insufficient evidence was available for the impact of a number of strategies on either suicide attempts or deaths (Table 1). In respect to suicide attempts, most interventions have RRs that are not dissimilar (ranging from .397 to .680). These RRs indicate that all strategies have demonstrated effectiveness in reducing suicide attempts. Taking prevalence of exposure to the intervention into consideration, psychosocial treatments and coordinated/assertive/brief aftercare are the strategies likely to bring about the strongest reduction in suicide attempts. Similarly, for suicide deaths all interventions are associated with relatively high risk ratios (ranging from .580 to .971). Taking into account population exposure, however, psychosocial treatment, GP training, gatekeeper training and reducing access to means appear to have the greatest impact on reductions in suicide deaths.
Discussion
The findings of the PPF calculations indicate that a systems approach could lead to significant reduction in suicide attempts and suicide deaths in Australia. Two interventions with the greatest impact on suicide attempts, psychosocial treatments and coordinated/assertive/brief aftercare, could decrease the prevalence of attempts by 8.0% and 19.8%, respectively. In regards to suicide deaths, the biggest reductions can be achieved through GP training, psychosocial treatments, gatekeeper training and reducing access to means (6.3%, 5.8%, 4.9% and 4.1%, respectively). Given that, in 2013, there were 27,112 suicide attempts (Harrison and Henley, 2014) and 2522 suicide deaths (ABS, 2015b), these results suggest that up to 160 lives could be saved annually, and up to 5370 hospitalisations due to intentional self-harm could be prevented. It is possible, however, that a systems approach may have an even greater combined impact, due to potential synergistic effects between strategies (Van der Feltz-Cornelis et al., 2011).
These PPF estimates are designed to generate further planning and discussion around the best avenues for suicide prevention. The PPF calculations need to be considered in respect to a number of caveats. We have used the best available evidence for the RR estimate for each component, such as a meta-analysis, a multicentre RCT, a systematic review or a single study with a large sample size and clear reporting of RR. Using different sources might have resulted in different findings. We did not include error margins with the estimates, as many further assumptions would be required for these calculations. The PPFs may vary in response to a number of factors including regional effects, implementation challenges, the context in which the intervention is delivered and baseline variations in terms of pre-existing programmes that may already be impacting on suicide attempts or deaths. The impact of interventions may overlap, for example, the combination of brief contact and aftercare interventions would impact the same population. Combined effects from multiple interventions may be less than the sum of their individual effects, or synergise to create a stronger effect. However, partial implementation of an intervention would reduce the impact of that intervention. In addition, the studies from which the risk estimates were drawn come from various regions, where the context of the intervention may or may not reflect the Australian context, and do not include the impact of social determinants of health. Second, we were unable to source accurate estimates for a number of the effects of interest, as there is insufficient research on the effects of several of the strategies on suicide attempts or deaths.
Conclusion
Currently, there is an absence of data available to be able to calculate the potential reductive effects of a number of suicide prevention interventions on suicide deaths and attempts. The absence of appropriate data highlights the need for improved evaluation of suicide prevention interventions, especially in the Australian context. The available evidence regarding the overall efficacy of the systems approach, however, is critically important in identifying what strategies should be prioritised, and where, in order to achieve the biggest impacts.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.