
Abstract

Introduction
In April 2015, the National Mental Health Commission (NMHC) Report recommended that the federal government should transfer AUD$1 billion from acute hospitals to community programmes (NMHC, 2015). This would cut mental health fundingfor acute hospitals by at least 10% from 2017 to 2022, necessitating the closure of recently mainstreamed beds.
The acute hospital funding was to be transferred to a mix of early intervention and recovery programmes including step-up/step-down sub-acute beds (Figure 1). This ‘optimal’ treatment was predicted to improve patient outcomes and decrease demand on downstream services such as acute care. It was also predicted to reduce Medicare benefits schedule (MBS) payments, pharmaceutical benefits scheme (PBS) costs, disability support pensions and carer benefits.

The NMHC model transfers resources from acute care in hospitals to fund community programmes and sub-acute care (reproduced with permission of the NMHC).
It is arguable whether these predictions were evidence-based. The NMHC Report relied on KPMG modelling of optimal treatment (NMHC, 2015: Summary page 13), which was based on seven case studies with expert opinion informing the key assumptions. As population-based data were unavailable, KPMG cautioned the NMHC (2015) that ‘scaling down from a population based study to a clinical case study approach may limit the ability to extrapolate results to system wide policy decisions’ (KPMG Commissioned Report, p. 36). This data limitation needs to be taken into account when considering the system-wide recommendations made by the NMHC Report.
Given the gap in the evidence for the NMHC Report, this article examines the real-world effect of a 10% cut in acute hospital funding. We ask whether Australia has already reached the safe minimum number of acute beds and whether further cuts could have negative impacts on patient care.
Does Australia have too many beds?
The community psychiatry movement has been remarkably successful in Australia. The nation has gone from 313 to 39 psychiatric beds per 100,000 over the last 50 years (Organisation for Economic Co-operation and Development [OECD], 2014). Australia is ranked 26th out of 34 OECD countries on hospital psychiatric care beds (Figure 2). By comparison, the United Kingdom has 54 beds per 100,000; in fact, wealthy European nations generally have many more beds than Australia with Italy being the most notable exception.
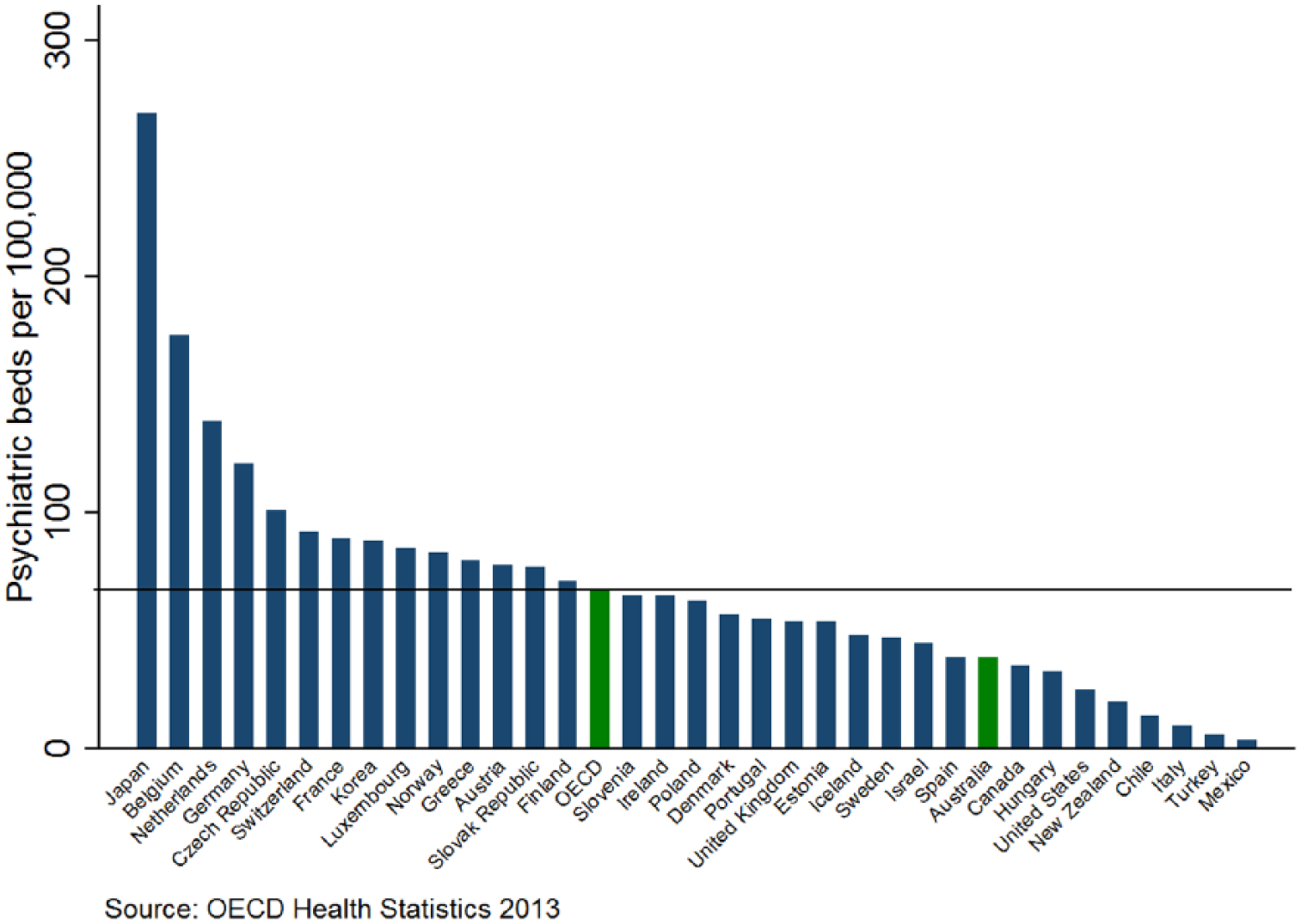
Hospital psychiatric care beds per 100,000 population, 2013 (reproduced with permission of the OECD).
While acknowledging Australia’s innovative community programmes, the OECD (2014) warned ‘with low inpatient psychiatric bed numbers, patients with severe mental illness risk worsening symptoms, more stays in emergency settings, and more hospital readmissions’ (p. 1). They concluded, ‘Australia should pay attention to getting the tricky balance of care provision right’.
As the OECD suggested, Australia’s low bed numbers may limit access to inpatient care, and this could result in higher thresholds for suicide risk and aggression at either admission or discharge. Indeed, a review of deinstitutionalisation and suicide included the observation that suicide was one of the ‘hazards on the fast lane to community care’ (Goldney, 2003).
Clinically, the authors share the OECD’s concerns. Acute wards are effectively full. This creates problems as bed occupancy rates above 85% reduce access to acute care and undermine a hospital’s ability to safely meet emergency demand (Bagust et al., 1999). The relevant benchmark is the national emergency access target (NEAT). The mandatory NEAT requires 90% of all patients to leave the emergency department (ED) within 4 hours (discharged or admitted).
South Australia’s acute bed closures
South Australia (SA) provides a real-world example of the potential impact of the NMHC Report’s recommendation to transfer 10% of the acute hospital funding to community and sub-acute programmes (Figure 1). In July 2011, SA began decommissioning 10% of their acute hospital beds to fund community (sub-acute) beds.
At the time, SA was the only state closing acute beds, and by 2014, SA was 20% below the national average for non-veteran general adult acute hospital beds and had double the average number of community beds. As a result, average ED waiting times were longer during 2014 than inprevious years. The 4-hour NEAT performance for mental health was 44% compared with 59% for other hospital divisions; on average, non-mental health patients waited 9 hours for admission, while mental health patients waited 33 hours (Ministerial Clinical Advisory Group [MCAG], 2014).
Longer ED stays meant thatmental health patients needed more ED cubicle space; mental health patients represented only 4% of the ED presentations but required 10% of the ED cubicle space (MCAG, 2014). This contributed significantly tooverall ED block and created major challenges for safe and effective patient care across the SA health system.
In response to the worsening clinical situation and community concerns, in December 2014, the SA Health Minister informed parliament that the government was determined to improve ED waiting times; they set performance targets, initially for no mental health patient to wait more than 24 hours in ED by January 2016 and 75% of the mental health patients to wait no more than 4 hours in ED by July 2018.
To improve patient care by meeting these ED targets, an additional 30 acute hospital beds were commissioned during 2014–2015. This initiative returned SA to the national average for non-veteran general adult acute inpatient beds. As a result of this significant policy change, there was an immediate and sustained reduction in ED waiting times for mental health patients.
Safe minimum numbers of acute beds
The recent SA experience reinforces the OECD’s warning about Australia’s low number of hospital psychiatric care beds. Australia may have reached the safe minimum number of acute beds, and further cuts could jeopardise patient care during acute illness when the risks of suicide and aggression are higher.
We suggest a data-driven approach to funding acute beds based on the careful monitoring of hospital demand. This requires collating national hospital activity data for acute bed occupancy rates, inpatient lengths of stay and the mandatory 4-hour NEAT. While Australia collects extensive mental health data, there remain many issues with data quality and access to large data sets as the NMHC Report clearly demonstrates.
Mental health performance should be benchmarked against other hospital divisions such as medicine and surgery as described in the SA example. Longer ED waiting times would support the case for increasing rather than decreasing Commonwealth investment in acute beds through national activity–based funding.
Australia’s acute bed numbers should be an important consideration for the National Mental Health Plans. In particular, we await the release of the National Mental Health Service Planning Framework commissioned by the Commonwealth as a population-based planning model that aimed to quantify packages of care required by people living with mental illness.
Summary
The terms of reference for theNMHC Report focused mainly on Commonwealth programmes and were restricted to existing levels of spending. Disappointingly, this limited the NMHC’s ability to argue for greater investment, and instead, the NMHC Report recommended cutting hospital funding, which would take Australia’s already low psychiatry bed numbers further below the OECD average.
Given the increasing burden of mental illness (NMHC, 2015), there is scope to invest much more in mental health; Australia spends only 7% of its total health budget on mental health compared with the United Kingdom’s 13%, which allows the United Kingdom to have 15 more beds per 100,000 than Australia along with more community options.
Conclusion
Over recent decades, psychiatric bed closures have helped fund community care; we argue that this policy alternative is no longer available within the Australian health-care system.
Footnotes
Declaration of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.