
Abstract
Clinicians seldom use the term Bipolar III disorder, probably because it is unclear when and how to make the diagnosis, and what it means in practice. For example, does a diagnosis of Bipolar III disorder, as opposed to another subtype (Bipolar I or II disorder), materially change the likelihood of future episodes of mania/hypomania? If so, what are its prognostic implications in terms of treatment? Furthermore, should it alter the prescription of antidepressants and, if so, how and to what extent? A paucity of evidence makes these questions difficult to answer; but for the diagnosis to be meaningful, answers are necessary and have to be sought.
Definition
Bipolar III disorder refers to the occurrence of mania/hypomania in association with antidepressant and somatic treatments. These treatment-associated ‘switches’ of mood occur against a background of recurrent depressive episodes, and typically, these periods of hypomania are brief in comparison to episodes that occur spontaneously. Neither Diagnostic and Statistical Manual of Mental Disorders–Fourth Edition (DSM-IV) nor Diagnostic and Statistical Manual of Mental Disorders–Fifth Edition (DSM-5), or indeed International Classification of Diseases–10th Revision (ICD-10), describes Bipolar III disorder, which is thought to form part of the ‘bipolar spectrum’ – a concept that originated from Dunner’s ‘bipolarity’ and was subsequently developed by Klerman and Akiskal to describe the sequential distribution of psychotic mania, Bipolar I and II disorder through to ‘softer’ forms of the illness including subsyndromal expressions such as those originating from temperament (Akiskal, 2005).
Instead, DSM-5 describes cyclothymic disorder and substance/medication-induced bipolar and related disorders, major depressive episodes with short-duration hypomanic episodes and also those that have insufficient hypomanic symptoms. It also specifies hypomanic episodes that occur in the absence of a prior depressive episode and cyclothymia that is yet to meet the 2-years duration criterion for disorder. These diagnoses capture some of the innumerable patterns of bipolar disorder that occur both spontaneously (Malhi and Porter, 2014) and because of the effects of treatments, and although Bipolar III disorder is not named, it is implicitly subsumed. Often the clinical picture is complicated further by episodes of depression and mania/hypomania being supplanted by mixed states, which are specified in DSM-5 as features. Thus, the diagnosis of bipolar disorder is complex and difficult (Malhi and Berk, 2014), and this is partly why, some years ago, the International Society of Bipolar Disorders (ISBD) created a task force to develop an agreed nomenclature for aspects of bipolar disorders (Tohen et al., 2009). The term ‘treatment-emergent affective switch’ (TEAS) was chosen because it does not attribute causality, unlike alternatives such as ‘antidepressant-induced switch’, ‘antidepressant-associated hypomania’, ‘medication-induced mania’ and ‘pharmacotherapy-emergent hypomania’. The task force considered both switching into mania/hypomania or depression and developed operational criteria (Tohen et al., 2009).
Clinical implications
Several interesting considerations and concerns arise in relation to the emergence of mania/hypomania in association with treatment. The first is the likelihood of this recurring with further exposure to an antidepressant, which depends on the diagnostic context and the type of antidepressant. The risk of a mood switch is generally greater in bipolar disorder than in major depression and, within bipolar disorder, is most likely in the context of Bipolar I disorder. Tricyclics and tetracyclics, and perhaps some serotonin–norepinephrine reuptake inhibitors (SNRIs), are more likely to precipitate a switch than other classes of antidepressants. Another interesting consideration is whether the propensity to switch spontaneously and otherwise is heightened following TEAS. This seems likely but has not been definitively shown. Similarly, the extent, if at all, to which the use of a mood stabilising agent diminishes future TEAS remains unclear. Reviewing the extant literature, another ISBD Task Force (Pacchiarotti et al., 2013) makes the following recommendations regarding antidepressant use when there is a risk of a switch to mania, hypomania or mixed states and rapid cycling:
Bipolar patients starting antidepressants should be closely monitored for signs of hypomania, mania and increased psychomotor agitation, in which case antidepressants should be discontinued (Note: mixicity and suicidal ideation are additional potential reasons for ceasing antidepressants [note added by authors]).
The use of antidepressants should be discouraged if there is a history of past mania, hypomania or mixed episodes emerging during antidepressant treatment.
Antidepressant use should be avoided in bipolar patients with high mood instability (i.e. a high number of episodes) or with a history of rapid cycling.
This advice can also be applied to major depression and to softer forms of bipolar disorder, indicating that greater awareness of maniform symptoms is necessary when treating depressive symptoms of any nature.
Research considerations
The fact that antidepressants can lead to manic symptoms when administered for the treatment of depression is intriguing. It prompts a number of questions: When administering antidepressant therapy, to what extent can TEAS be predicted? And how soon after treatment does the switch usually occur? Does the occurrence of a switch necessarily implicate the antidepressant being prescribed? And to what extent does it increase the likelihood of a subsequent switch – either spontaneous or treatment-emergent? Are individuals susceptible to TEAS fundamentally different in nature?
Clinically, up to 40% of patients with major depression experience significant hypomanic symptoms at one time or another, with a quarter of these occurring during pharmacotherapy. Rates are higher in patients with bipolar disorder, but even then, it can be difficult to establish causality. For example, common clinical problems such as insomnia can produce short-lived hypomanic/manic symptoms; the inappropriate use of stimulants can mimic hypomania. Furthermore, in the treatment of depression, antidepressants are often prescribed alongside other medications, making it difficult to identify the unique effects of a single agent. It is also worth noting that a ‘switch’ into hypomania/mania may occur spontaneously without any link to treatment. Recurrence is the defining characteristic of manic-depressive illness, and therefore, mania often ‘breaks through’ maintenance/prophylactic medication.
To better understand TEAS, we propose a schematic model for the occurrence of mania/hypomania in the context of antidepressant treatment. Figure 1 details a treatment-emergent switch into mania/hypomania from depression. It facilitates the examination of key components of the process such as the time lag between a change in treatment and the emergence of manic symptoms (treatment-emergence [TE] interval). Conventionally, a TE interval of 8–12 weeks is deemed to implicate causality (Tohen et al., 2009), but a much shorter interval may be necessary to definitively link cause and effect. To differentiate TEAS, the duration and amplitude of the affective change, specifically the time it takes to form (duration of emergence) and remain significant (period of elevation), may be of critical importance. Alternatively, it may be the characteristics of how the change resolves – for example, the time it takes (period of resolution) and whether this occurs once antidepressant treatment has been withdrawn or while treatment is continuing – that distinguishes TEAS from spontaneous episodes. Naturalistic ‘studies’ are inevitable given that bipolar disorder invariably presents with depression that is indistinguishable from major depression, resulting in bipolar patients being treated with antidepressants prior to manifesting mania/hypomania. However, in addition, controlled prospective studies that include more ‘ecological’ measures are needed to carefully dissect the effects of antidepressants on switching mood.
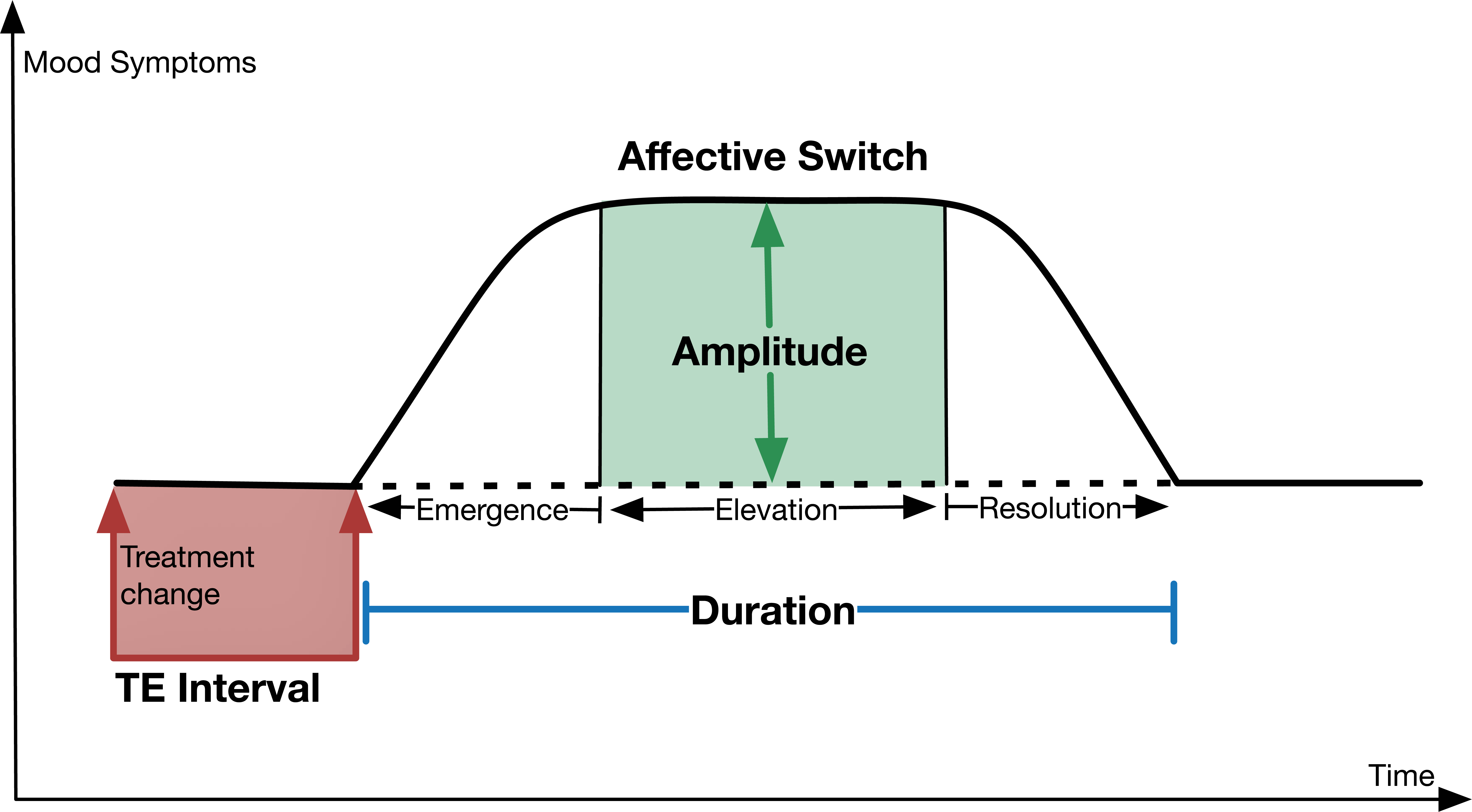
Components of a treatment-emergent affective switch (TEAS) into mania.
Conclusion
Antidepressants are often seemingly ineffective in the treatment of bipolar depression and yet, sometimes, they precipitate a significant affective switch into mania/hypomania and possibly create ongoing mood instability. Why and how such switching occurs remains unknown, but this relatively common phenomenon likely holds important clues as to the aetiology of bipolar disorder. Therefore, in addition to clinical surveillance, systematic inquiry is urgently needed to better understand TEAS and their prognostic implications.
Footnotes
Declaration of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
Gin S. Malhi is funded by a National Health and Medical Research Council (NHMRC) Program Grant (APP1073041).