
Abstract
Objective:
With the wide and rapid expansion of computers and smartphones, Internet use has become an essential part of life and an important tool that serves various purposes. Despite the advantages of Internet use, psychological and behavioral problems, including Internet addiction, have been reported. In response to growing concern, researchers have focused on the characteristics of Internet addicts. However, relatively little is known about the behavioral and neural mechanisms that underlie Internet addiction, especially with respect to risky decision making, which is an important domain frequently reported in other types of addictions.
Method:
To examine the neural characteristics of decision making in Internet addicts, Internet addicts and healthy controls were scanned while they performed a financial decision-making task.
Results:
Relative to healthy controls, Internet addicts showed (1) more frequent risky decision making; (2) greater activation in the dorsal anterior cingulate cortex and the left caudate nucleus, which are brain regions involved in conflict monitoring and reward, respectively; and (3) less activation in the ventrolateral prefrontal cortex, an area associated with cognitive control/regulation.
Conclusion:
These findings suggest that risky decision making may be an important behavioral characteristic of Internet addiction and that altered brain function in regions associated with conflict monitoring, reward and cognitive control/regulation might be critical biological risk factors for Internet addiction.
Introduction
With the development of computers and the Internet, the number of people who use the Internet excessively and who are diagnosed with Internet addiction has increased rapidly and significantly worldwide. For example, 9.8% of the total population in Germany (Beutel et al., 2011) and 10.7% of adolescents in Korea (Park et al., 2008) experience Internet addiction. Internet addiction is defined as compulsive and pathological use of the Internet (Young, 1998). In the newest Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-V), Internet addiction has been included under the terms of Internet Gaming Disorder in Section III of DSM-V (American Psychiatric Association, 2013) and is therefore recommended for further study.
Mounting evidence suggests that Internet addiction has a variety of serious public health implications, including emotional distress and health or financial problems that can lead to social disruption (Dong et al., 2011b; Shaw and Black, 2008; Young, 1998). Given the potential personal and public health problems associated with Internet addiction, it is important to examine the behavioral and neural characteristics of this disorder and to assess the clinical implications for prevention and early intervention.
It has been suggested that Internet addiction is a behavioral rather than a chemical addiction because it shares neurocognitive (i.e. risky decision making) and personality (i.e. impulsivity and sensation seeking) characteristics with other types of behavioral addictions, such as pathological gambling and compulsive buying (Charlton and Danforth, 2007; Grant et al., 2010; Potenza et al., 2003). Altered decision-making behavior is a critical behavioral characteristic of addictions (e.g. to drugs and gambling; for a review, see Bechara, 2003). Consistent with this behavior, Internet addicts are suggested to have a strong tendency to engage in risk-taking processes when making choices during gambling tasks in order to gain immediate gratification despite an increased risk of experiencing loss, while giving less consideration to the long-term consequences (Brand et al., 2014; Dong et al., 2011a, 2013a; Pawlikowski and Brand, 2011; Sun et al., 2009). In a functional magnetic resonance imaging (fMRI) study, Dong et al. (2011a, 2013a) demonstrated that the reduction in decision-making performance in Internet addicts could be related to altered brain functioning involving the executive functions. However, relatively little is known about the neural substrates of decision making in Internet addiction. This study attempted to address this gap in knowledge.
Decision making occurs in two stages before the outcome is experienced, and addicts show defects in both stages (Ernst and Paulus, 2005). The first stage of a decision-making process involves evaluating the value and usefulness of available options to form a preference (formation of preference); this is facilitated through activation of brain regions such as the insula, ventromedial prefrontal cortex, dorsolateral prefrontal cortex, dorsal anterior cingulate cortex (dACC) and caudate nucleus (Krain et al., 2006). Abnormal decision making in addicts was found to be related to alterations in the dACC (Paulus et al., 2003), which is related to conflict monitoring, and in the caudate nucleus (Leland et al., 2006), which is responsible for reward anticipation. The second stage of decision making involves the prefrontal cortex, where alternative possible actions are inhibited and one action is selected and performed (Krain et al., 2006; Ridderinkhof et al., 2004). Research on substance abusers and pathological gamblers showed that deficits in decision making were related to dysfunctions in the prefrontal cortex, an area that is mainly responsible for executive functioning/cognitive control (Cavedini et al., 2002; Volkow and Fowler, 2000).
The objectives of this study were to (1) replicate previous behavioral findings that demonstrated risky decision making in Internet addicts and (2) characterize the neural substrates of risky decision making in these addicts. Two questions were addressed. First, would Internet addicts make disadvantageous decisions (i.e. risky decision making) compared to healthy controls? Second, would Internet addicts show different activation patterns in brain regions associated with decision making (i.e. reward and control/regulation) compared to healthy controls? To answer these questions, we adopted the financial decision-making task used by De Martino et al. (2006). This task includes two-option conditions (safe vs risky). The safe option is a condition in which part of a proposed sum of money is assured; the risky option is a condition in which the entire proposed sum of money is won or lost. We hypothesized that Internet addicts are more likely to make disadvantageous decisions and that the brain regions that are responsible for conflict monitoring, reward and control/regulation would show altered activation patterns compared to healthy controls.
Methods
Participants
A total of 15 Internet addicts (young adult males, mean age = 22.20 years, standard deviation [SD] = 3.07 years) and 15 healthy individuals (young adult males, mean age = 22.47 years, SD = 2.53 years) participated in this fMRI experiment. Volunteers were recruited through on-line bulletin boards at an Internet addiction treatment center and a cyber addiction information center, and off-line at local Internet addiction recovery group meetings. The specific purposes of excessive Internet use were found to be mainly on-line gaming/gambling (73%), followed by on-line entertainment (7%), chat rooms (13%) and pornography (7%). Prospective volunteers were given a psychiatric diagnostic interview by a licensed counseling psychologist to exclude individuals with Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) Axis I disorders. In addition, the Korean translated/modified version (Kim, 2000) of the Internet Addiction Scale (IAS; Young, 1998) and the K-scale (Koh, 2007) were used. The original IAS is a self-reported 20-question assessment of pathological Internet use (i.e. preoccupation, compulsive use, behavioral problems, emotional changes, impacts on daily life). Each question is based on a 5-point scale ranging from 1 (never) to 5 (very). Individuals scoring 70 or more points comprise an Internet addiction group, for whom Internet use can cause severe problems in daily life; individuals with scores of 40–69 points are categorized as a mild Internet addiction group, and those with 39 or fewer points are considered normal users.
The K-scale is a Korean self-diagnostic scale for Internet addiction based on a survey of 146 university students. The scale consists of 20 questions and includes four subscales: disability to distinguish daily life and reality, positive expectation of the Internet, tolerance and withdrawal, and self-awareness of the Internet. Each question is rated on a 4-point scale ranging from 1 (never) to 4 (very). Individuals with scores of 54 or more points are usually classified as an Internet addiction group, whereas individuals with 53 or fewer points are classified as a normal user group.
The average IAS score of participants selected as the final Internet addict group in this experiment was 70.80 (SD = 10.31) and the average K-scale score was 60.00 (SD = 4.47), whereas the average IAS score of the control group was 28.60 (SD = 7.35) and their average K-scale score was 32.60 (SD = 7.70, p < 0.001). The demographic characteristics and background information of the participants are shown in Table 1. Participants in both groups did not experience other addictions, such as alcoholism or gambling addiction. All participants provided signed consent to voluntarily participate in the experiment after being thoroughly informed of the details of the experiment.
Demographic characteristics and background information on Internet use of study participants.

Means (standard deviations) are represented.
IAS: Internet Addiction Scale; K-scale: Korean Self-Diagnostic Scale for Internet Addiction.
p < 0.001.
Procedure and experimental paradigm
Before beginning the experiment, all participants practiced the financial decision-making task a few times to become familiar with it. Participants were informed that they would not receive immediate feedback on the outcome of their decisions during the task, but that they would be given 10% of the total amount won during the experiment upon termination of the experiment. Participants were actually compensated for their time and efforts for participating in the study by a monetary reward of more than 10% of their total winnings.
Participants performed the financial decision-making task, which consisted of 36 trials, while in an MRI scanner (De Martino et al., 2006). The task was presented using the E-prime software (Psychology Software Tools, Inc.) and was organized to enable selection of either the safe (or sure) option or the risky (or gambling) option to maximize winning. As depicted in Figure 1, each trial began with a fixation cross for 1–6 seconds, followed by a virtual initial award amount for 1 second (e.g. W25,000, W50,000, W75,000, and W100,000, which was equivalent to approximately US$25, US$50, US$75 and US$100). The choice alternatives for the safe (or sure) option and risky (or gambling) option were presented for 3 seconds, and then, participants were asked to choose from the safe or risky option for 2 seconds.
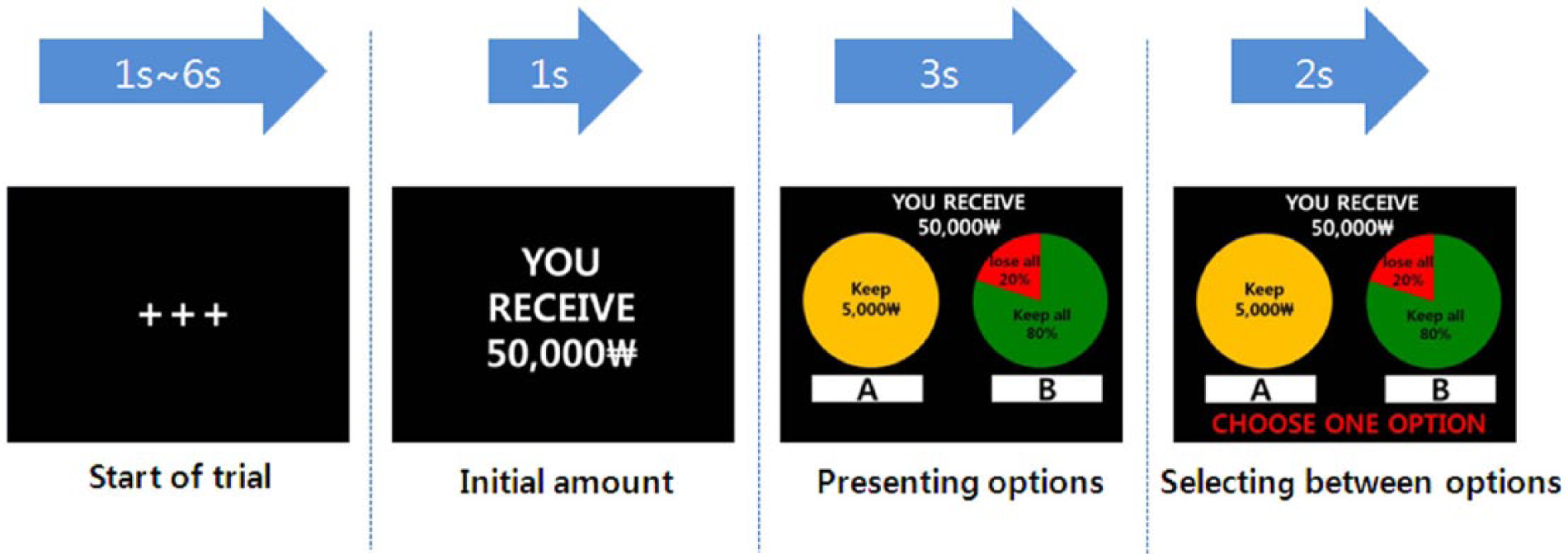
A single trial of the financial decision-making task.
The safe option was a choice in which a portion of the initial amount was assured (e.g. acquiring W10,000 out of the initial amount of W50,000), and the risky option was a gambling choice in which the entire initial amount could be won or lost. For the risky option, the winning and losing probabilities were presented in a pie chart in green and red. Five probability levels (e.g. 20%, 40%, 50%, 60% and 80% probability of winning the entire initial amount) were incorporated. The order of the four probabilities was counterbalanced. In all, 20 trials were organized, in which the expected value of the safe and risky options was equal. For example, when the initial amount of W50,000 was given, the safe option presented was that participants would ‘receive W10,000’, and the risky option shown was ‘20% chance of winning all W50,000’. The remaining 16 trials included ‘risky weighted’ options (eight trials) and ‘safe weighted’ options (eight trials), in which the probability of losing or winning was increased. For example, in the ‘gamble weighted’ option, subjects were asked to choose between the safe option of taking W10,000 of the initial W50,000 and the risky option of 80% chance of winning W50,000. In the ‘safe weighted’ option, subjects were asked to choose between taking W40,000 of the initial W50,000 and the risky option of 20% probability of winning W50,000.
Self-reporting measure
To determine whether Internet addicts were more impulsive than controls, Barratt’s Impulsiveness Scale II (BIS-II, 1983), as adapted by Lee (1992), was used. The BIS-II consists of 35 questions with dichotomized ‘yes’ (1) or ‘no’ (0) answers. The total score ranges between 0 and 35, with higher scores indicating greater levels of impulsiveness.
Imaging acquisition and preprocessing
Imaging was conducted using a 3.0 T whole-body ISOL Technology FORTE scanner (ISOL Technology, Korea) equipped with whole-body gradients and a quadrature head coil. Single-shot echo-planar fMRI scans were acquired in 35 continuous slices, parallel to the anterior commissure–posterior commissure line, with repetition time/echo time (TR/TE) = 3000/40 ms, flip angle = 80, field of view (FOV) = 240 mm, matrix = 64 × 64, slice thickness = 4 mm and in-plane resolution = 3.75 mm. Three dummy scans from the beginning of the run were excluded to reduce the effect of non-steady-state longitudinal magnetization. T1-weighted anatomical images were obtained using a three-dimensional (3D) fluid-attenuated inversion recovery (FLAIR) sequence (TR/TE = 280/14 ms, flip angle = 60, FOV = 240 mm, matrix = 256 × 256 and slice thickness = 4 mm).
The fMRI data were preprocessed and analyzed using the Statistical Parametric Mapping software (SPM8; www.fil.ion.ucl.ac.uk/spm). Slice timing correction was performed on the data to adjust for the different timing in acquisition of different slices, and motion correction was performed using six-parameter rigid body transformation to remove changes in signal intensity introduced by head motion. The realigned scans were co-registered to each participant’s anatomical images obtained in each session. Normalization was performed to identify the location of functional activation in a standardized coordinate system. To facilitate inter-subject averaging, a transformation matrix between the mean image of the realigned scans and a standardized anatomical space defined by the Montreal Neurological Institute generated with a fourth degree B-spline algorithm was applied to re-slice volumes with a 2 × 2 × 2 mm3 voxel-size. The functional map was then spatially smoothed using an 8-mm isotropic Gaussian kernel to reduce residual inter-individual anatomical variability.
Statistical analyses
Behavioral data and self-reporting measure analysis
The behavioral data were analyzed using SPSS 17 (SPSS Inc., Chicago, IL). Independent-sample t-tests were used to examine whether Internet addicts were more likely to choose risky options compared to healthy controls. Reward sensitivity was used as an additional behavioral index, as suggested by previous studies that indicated risky choices by Internet addicts are related to reward sensitivity (Vitaro et al., 1997). The reward-sensitivity index represented the expected amount for each risky choice and was calculated by dividing the total expected amount associated with the risky option by the number of risky choices. Independent-sample t-tests were used to test group differences in the reward-sensitivity index and to examine whether Internet addicts were more impulsive than healthy controls based on the BIS-II measurements.
Imaging data analysis
Data were statistically analyzed on an individual and group basis using the general linear model and the theory of Gaussian random fields implemented in SPM8. To identify specific brain regions presenting differential responses (different patterns of activity) between Internet addicts and healthy controls, a whole brain voxelwise analysis of variance (ANOVA) was conducted using option (safe vs risky) as the within-group variable and group (Internet addicts vs controls) as the between-group variable (False Discovery Rate [FDR]-corrected, p < 0.05). Activations were reported using the standardized Montreal Neurological Institute (MNI) coordinate space, and their coordinates were also converted into Talairach and Tournoux atlas space (Talairach and Tournoux, 1988).
To confirm the validity of the results acquired through SPM, the percent signal change of the functional regions of interest (ROIs) (e.g. dACC and caudate) identified from the voxelwise ANOVA was individually extracted for each subject using MarsBaR (http://www.sourceforge.net/projects/marsbar) and compared among groups using SPSS 17 with follow-up t-tests. The coordinates obtained in contrasts of the group analyses were selected for ROI analysis of peak voxels. The ROIs were functionally defined by centering spheres on the respective peak voxels with a radius of 5 mm. Analyses were performed for all activated areas in the interaction results (FDR-corrected, p < 0.05). The percent signal change for the various conditions was extracted for each subject and compared between groups using ANOVA with follow-up t-tests.
Results
Behavioral data and self-reported measurement results
As predicted, the number of risky responses differed significantly between the two groups (t28 = 2.16, p < 0.05, Cohen’s d = 0.81; Figure 2(a)). Internet addicts showed significantly more risk taking in financial decision making compared to healthy controls. Internet addicts were also more sensitive to reward, as indexed by the size of the expected value, compared to healthy controls (t28 = 2.89, p < 0.05, Cohen’s d = 1.09; Figure 2(b)). Furthermore, Internet addicts (M = 18.27, SD = 5.29) showed greater impulsiveness compared to healthy controls (M = 7.87, SD = 5.35) as measured using the BIS-II (t28 = 5.34, p < 0.001, Cohen’s d = 2.01).
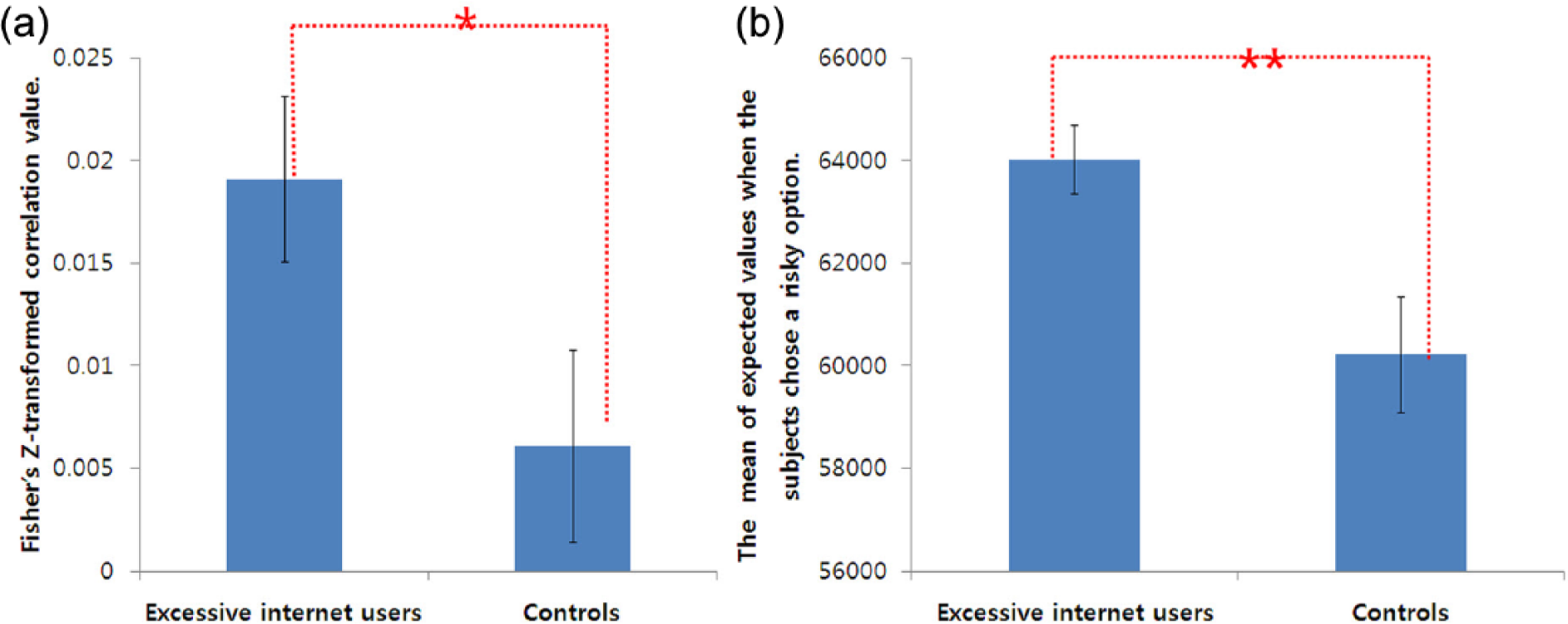
Behavioral results: (a) frequency of trials in which participants chose the risky option; (b) reward-sensitivity index.
Imaging results
A main effect of option
A main effect of option (safe vs risky) was observed in the dorsolateral prefrontal cortex, medial frontal cortex and middle temporal cortex (p < 0.05, FDR-corrected; Table 2). These regions showed greater activation under risky than under safe option conditions. However, no brain regions were more activated by the safe option than by the risky option condition.
Imaging results: main effects of option and group (p < 0.05, FDR-corrected).
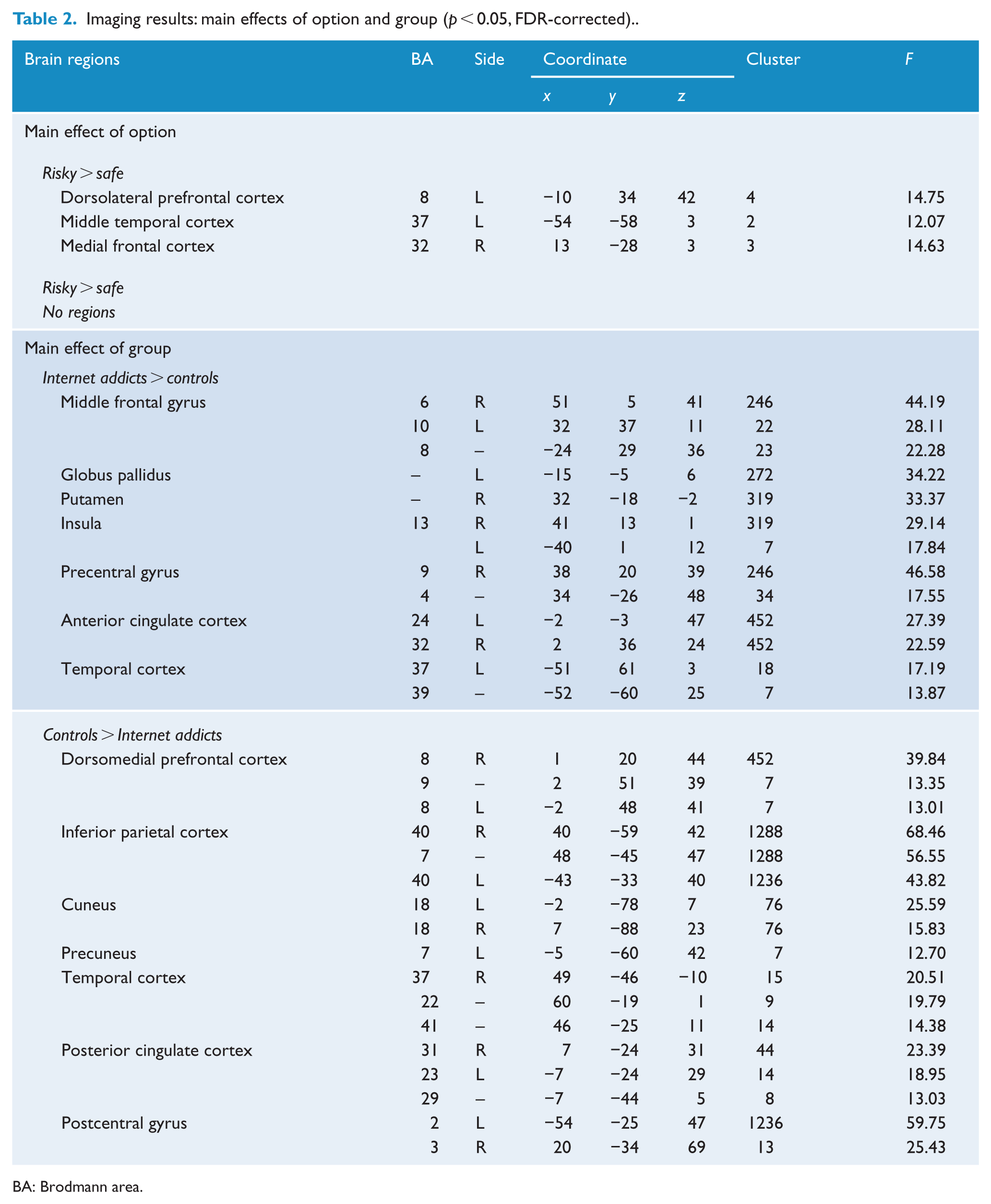
BA: Brodmann area.
A main effect of group
A main effect of group (Internet addicts vs controls; p < 0.05, FDR-corrected; Table 2) was observed in widespread brain regions, including several prefrontal (e.g. dorsomedial prefrontal cortex) and parietal areas (e.g. precentral cortex), and the temporal cortices and subcortical-limbic regions (e.g. putamen and insula). Internet addicts showed greater activation in the bilateral middle frontal gyrus, precentral gyrus, anterior cingulate cortex and left temporal cortex compared to healthy controls. In contrast, healthy controls showed higher activation in the right dorsomedial prefrontal cortex, postcentral gyrus, posterior cingulate cortex, inferior parietal cortex, precuneus, cuneus and temporal cortex compared to Internet addicts.
Option × group interaction effects
Significant option × group interactions (p < 0.05, FDR-corrected; Table 3) were identified in the left tail of the caudate nucleus, left dACC (Brodmann Area (BA) 32/24) and left ventrolateral prefrontal cortex (VLPFC; BA 47).
Imaging results: interaction effects of option × group (p < 0.05, FDR-corrected).
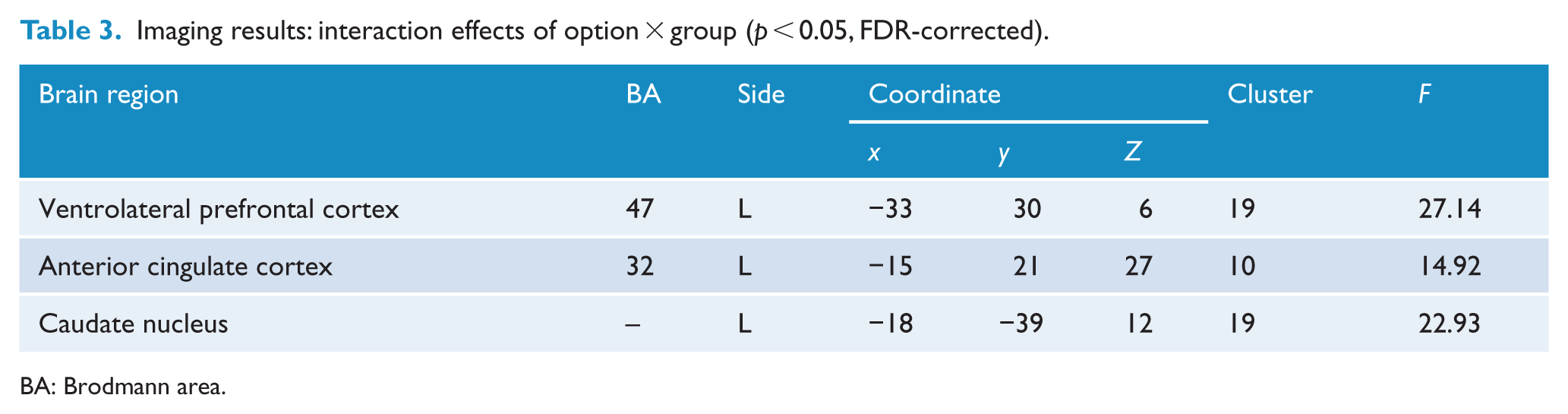
BA: Brodmann area.
In a follow-up t-test using the extracted percent signal changes of the ROIs, Internet addicts showed significantly higher caudate nucleus activation while choosing the risky option (t28 = 2.67, p < 0.05, Cohen’s d = 1.01) relative to the healthy controls, whereas less caudate nucleus activation was observed while choosing the safe option (t28 = 2.38, p < 0.05, Cohen’s d = 0.91; Figure 3(a)). A similar pattern of brain activation was found in the dACC: compared to controls, Internet addicts showed greater activation in the dACC while choosing the risky option (t28 = 2.41, p < 0.05, Cohen’s d = 0.91) but less dACC activation while choosing the safe option (t28 = 2.59, p < 0.05, Cohen’s d = 0.97; Figure 3(b)). Internet addicts also showed significantly less VLPFC activation in the risky option compared to controls (t28 = 4.25, p < 0.001, Cohen’s d = 1.61), but no significant group differences were found in the safe option (t28 = 1.75, p > 0.05, Cohen’s d = 0.66; Figure 3(c)).
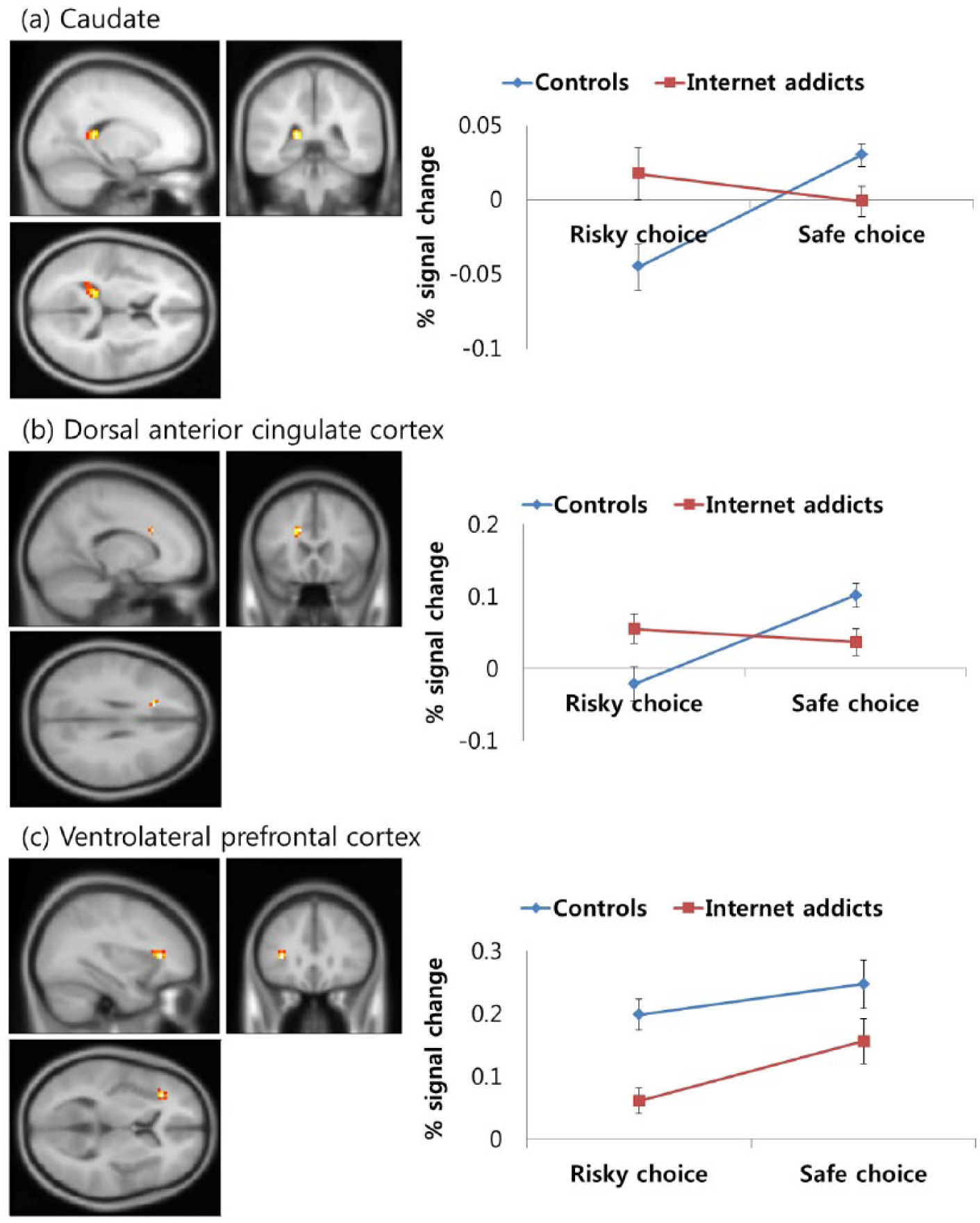
(a) Brain activation patterns in the caudate, (b) the dorsal anterior cingulate cortex and (c) the ventrolateral prefrontal cortex. The graphs depict the extracted signal change averaged across voxels from each region, displaying option × group interactions (p < 0.05, FDR-corrected).
Discussion
This study used fMRI to provide evidence of the neurobiological mechanisms that underlie impaired decision-making behavior in Internet addicts. The brain activity of Internet addicts and healthy controls was measured when subjects performed a financial decision-making task involving multiple phases of risky or safe options that led to chances of winning or losing virtual money. As hypothesized, Internet addicts showed significantly more risk-taking behavior and different patterns of brain activation in regions associated with conflict monitoring, reward and control/regulation compared to healthy controls. Specifically, Internet addicts showed greater dACC and caudate nucleus activation, yet less VLPFC activation while choosing risky options. These results suggest that altered patterns of brain activation may be related to high-risk decision-making behaviors in Internet addicts.
As predicted, Internet addicts were more likely to make inappropriate decisions because they were more prone to risk taking compared to control subjects. These decisions are referred to as ‘inappropriate’ because Internet addicts showed characteristics similar to those of gamblers, in which individuals continuously make bets despite a high chance of losing or uncertainty of outcome (Australian Productivity Commission, 1999; Devereux, 1979). This result indicates that the minds of Internet addicts function differently than those of individuals without Internet addiction. Internet addicts might find risky situations attractive, while individuals who are not addicted do not because of the negative consequences associated with inappropriate decisions. The significant differences in reward sensitivity between groups are consistent with previous findings on Internet addiction (Brand et al., 2014; Dong et al., 2013a).
These behavioral characteristics of Internet addiction might be associated with altered activation in the dACC and caudate nucleus. Internet addicts showed greater dACC and caudate nucleus activation compared to controls when they made risky decisions. Recent neuroimaging and lesion studies have shown that the dACC is related to conflict monitoring during decision making (Paulus et al., 2003; Rushworth et al., 2004), where the dACC integrates information from past behavioral results and induces action selection based on a cost–benefit analysis. Studies of individuals with other types of addictions (i.e. substance dependence and pathological gambling) proposed that conflict plays an important role in decision making (Bechara, 2003; Bechara and Damasio, 2002). In those studies, addicts appeared to experience greater conflict between primary rewards (e.g. drugs or gambling) and negative results. Therefore, the increased dACC reactions among Internet addicts observed in this study might represent increased conflict between rewards and adverse consequences during decision making. Alternatively, dACC activity may be related to error monitoring. Consistent with this, an fMRI study on Internet addiction by Dong et al. (2013b) showed Internet addicts to exhibit decreased error monitoring, which is related to greater activation in the anterior cingulated cortex (ACC).
The increased activation of the caudate nucleus observed in Internet addicts might be associated with increased sensitivity to the monetary rewards used in this study. The caudate nucleus region forms part of the ventral striatum along with the ventromedial putamen and is the area responsible for reward prediction and anticipation (Knutson and Cooper, 2005). Andrews et al. (2011) showed activation of the tail of the caudate during anticipation of monetary reward. Increased reward anticipation in Internet addicts might have significantly hindered their ability to choose the safe options, especially when the reward was a larger expected sum, despite the uncertainty of actually obtaining the reward. In summary, increased reaction in the dACC and caudate nucleus in Internet addicts suggests that the ability of Internet addicts to weigh pros and cons is impaired. This leads to greater anticipation of a larger reward, despite conflict induced by knowledge of the risks associated with unsuccessful obtainment of the reward.
Increased conflict and reward in Internet addicts might be related to failure of cognitive control/regulation, which is the second stage of decision making suggested by Ernst and Paulus (2005). Consistent with this idea, Internet addicts showed less VLPFC activation when they chose the risky options compared to healthy controls. The prefrontal cortex has been implicated in the executive function of decision making (Alvarez and Emory, 2006). The VLPFC is related to decision making that includes uncertainty or risk (Goel and Dolan, 2000; McClure et al., 2004). The VLPFC interprets cognitive and motivational information and conducts inhibitory signaling of responses that must be cancelled or blocked to facilitate decision making, leading toward goal-directed behavior (Aron et al., 2004; Manes et al., 2002; Sakagami and Pan, 2007). Therefore, decreased VLPFC activation observed in Internet addicts during the risky option could represent cognitive control or regulatory defects that are likely to be associated with addiction. This inhibitory dysfunction can be affected by environmental contingencies and cues (e.g. craving for the Internet) and consequently contributes to the maintenance of Internet abuse.
This study had some limitations and suggested topics for future research. The study participants were limited to university students, rather than a clinical group, for the purpose of collecting data from homogeneous individuals with similar cognitive ability (similar academic background or IQ); thus, it is difficult to generalize our findings to ‘patients’ from hospitals or clinics. Future research could involve similar studies with individuals who experience more serious Internet addiction. In addition, for improved precision, it will be necessary to measure differences in the executive functions of prefrontal regions based on the stages of Internet addiction. It will also be interesting to conduct research on adolescents in whom the prefrontal area is still developing and to verify whether prefrontal dysfunction has a larger impact on adolescents than on adults. Finally, to identify unique or specific features of Internet addiction, future research should make direct comparisons between Internet addicts and other types of addicts (i.e. substance abusers or gamblers).
Despite these limitations, our results are useful for characterizing the behaviors and associated neural mechanisms of Internet addicts, which goes a step beyond the descriptions of personality or behavioral characteristics presented in previous studies. Internet addicts showed increased dACC and caudate nucleus activation, indicating increased conflict and reward sensitivity when making risky choices. Internet addicts also showed low VLPFC activation, which might represent a cognitive deficiency or impaired ability to control or regulate efficiently. These results are consistent with findings from other groups with addiction and impulse-control disorders and suggest that Internet addiction, like other type of addictions, is a serious problem. These findings not only provide a neurobiological explanation for the behavior of Internet addicts but also have clinical implications for early prevention and treatment before serious brain impairment occurs. The key is not to see Internet addiction as a negative habit or behavioral problem, but to perceive it as a clear pathological issue that involves reward psychology and related cognitive dysfunction of the VLPFC. Therefore, the Internet addiction issue needs more systematic and active therapeutic interventions that incorporate understanding of, and strategies for improving, cognitive impairment.
Footnotes
Acknowledgements
The authors acknowledge, with thanks, the study participants who committed their time and whose responses form the basis of this publication.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This work was supported by the National Research Foundation of Korea Grant funded by the Korean Government (NRF-2006-2005087) and by research fund of 2014 Chungnam National University.