
Abstract
Objective:
Mood instability levels are high in depression, but temporal precedence and potential mechanisms are unknown. Hypotheses tested were as follows: (1) mood instability is associated with depression cross-sectionally, (2) mood instability predicts new onset and maintenance of depression prospectively and (3) the mood instability and depression link are mediated by sleep problems, alcohol abuse and life events.
Method:
Data from the National Psychiatric Morbidity Survey 2000 at baseline (N = 8580) and 18-month follow-up (N = 2413) were used. Regression modeling controlling for socio-demographic factors, anxiety and hypomanic mood was conducted. Multiple mediational analyses were used to test our conceptual path model.
Results:
Mood instability was associated with depression cross-sectionally (odds ratio: 5.28; 95% confidence interval: [3.67, 7.59]; p < 0.001) and predicted depression inception (odds ratio: 2.43; 95% confidence interval: [1.03–5.76]; p = 0.042) after controlling for important confounders. Mood instability did not predict maintenance of depression. Sleep difficulties and severe problems with close friends and family significantly mediated the link between mood instability and new onset depression (23.05% and 6.19% of the link, respectively). Alcohol abuse and divorce were not important mediators in the model.
Conclusion:
Mood instability is a precursor of a depressive episode, predicting its onset. Difficulties in sleep are a significant part of the pathway. Interventions targeting mood instability and sleep problems have the potential to reduce the risk of depression.
Introduction
Of all brain disorders, major depression causes the greatest level of burden of disease (Wittchen et al., 2011), and globally is estimated to affect 350 million people and accounts for 8.2% of years lived with disability (Ferrari et al., 2013). Financial costs of major depression are also high (Olesen et al., 2012). While there are effective treatments for depression, not all those affected are able to achieve remission and recurrence rates are high (Sinyor et al., 2010). Although the core features of depression usually involve a persistent and pervasive low mood and loss of interest, a relatively neglected aspect of the syndrome is affective instability or mood instability. There are many and varied definitions of mood instability (MI) (Marwaha et al., 2014b), but generally incorporate sudden and intense mood changes in an individual over a relatively short period. The symptom is largely experienced and reported subjectively. The neurobiological underpinnings of MI remain only partly known, but current evidence suggests that abnormalities in the amygdala and its connections with the prefrontal cortex are involved (Broome et al., 2015).
It is established that MI is a core component of bipolar disorder (Bassett, 2012) and is a diagnostic criterion for borderline personality disorder (First et al., 1997). In the last decade, evidence has gradually emerged that MI is also important in depression. Levels of MI are very high in people with an established diagnosis of depression, with estimates ranging from 50%−70% (Marwaha et al., 2013a). Furthermore, MI, depression and anxiety are significantly linked (Marwaha et al., 2013b). In an experimental study of those with major depressive disorder (MDD) and those without MDD, MI was significantly associated with having a lifetime history of MDD (Thompson et al., 2011). In an associated study, affect variability (but not intensity) at baseline predicted anhedonic depression after 3 months, even after the depressive symptoms at baseline were controlled for in the analysis (Thompson et al., 2011).
While suggestive, the current limited literature does not allow firm conclusions regarding the temporal precedence of MI over depression as most studies are cross-sectional, or have measured MI concomitantly with depression. Therefore, it remains unclear as to whether MI is solely an under-recognized aspect of the depression construct, or an early indicator or trait vulnerability factor which predisposes the individual to subsequent depressive illness. Another unanswered question is whether MI could act to maintain depression, thereby worsening its course. Prospective analyses of MI-depression associations could therefore advance our theoretical understanding of the development of depression, informing early intervention and the further refinement of prognostic risk scales. Furthermore, this approach may facilitate the identification of potential mediating factors in the pathways towards depression, highlighting novel targets for intervention and prevention.
There are a number of mechanisms that could potentially underpin the link between MI and depression. First, MI and sleep difficulties are linked independent of depression (Bowen et al., 2013a), and sleep problems and depression are associated in prospective studies (Batterham et al., 2012). Therefore, MI could increase the subsequent risk of depression by increasing the risk of sleeping difficulties. Second, MI could increase depression risk via increased likelihood of alcohol consumption, that is, those with an unstable mood might abuse alcohol in an attempt to control symptoms. Indeed, cyclothymia is significantly more common in those with a propensity towards alcohol abuse, and this is not explicable by the effects of alcohol consumption or withdrawal (Pacini et al., 2009). Alcohol abuse is highly comorbid with depression (Regier et al., 1990), and US National Epidemiological Survey data suggest that there is a reciprocal relationship between alcohol abuse and new onset affective disorders (Grant et al., 2008). Finally, MI has been associated with greater levels of interpersonal impairment within romantic relationships (Miller and Pilkonis, 2006), and in turn, life events are prospectively associated with new onset depression (Singleton and Lewis, 2003).
We used baseline and follow-up data from the National Psychiatric Morbidity Survey (NPMS) of Great Britain 2000 to examine the association between MI and depression and the influence of potential underlying mediators. We tested specific hypotheses that (1) MI will be associated with a diagnosis of depression cross-sectionally, (2) MI will predict new onset and maintenance of depression prospectively and (3) the association between MI and depression will be mediated by sleep problems, alcohol abuse and life events.
Methods
Setting and design
Full details of the survey methods are available in the main survey report (Singleton and Lewis, 2003). In brief, the sampling frame was the English Small Area Postcode Address. Adults living in private households were selected using population-based multi-phase probability sampling. Experienced survey interviewers identified private households containing at least one person. They used the Kish grid method to select at random one person in each household, ensuring that all eligible household members had the same chance of being selected.
In order to render the results representative of the household population in the chosen age range, primary sampling units were stratified by region and socioeconomic characteristics. Thus, in each case, data were weighted to take account of survey design and non-response. Survey interviewers carried out Phase 1 assessments using a detailed questionnaire that established socio-demographic characteristics, and covered a range of topics.
Those interviewed at 18-month follow-up represented one of three groups from the baseline 2000 cross-sectional survey. All those with a mental disorder as defined by the Clinical Interview Schedule–Revised (CIS-R) (Lewis et al., 1992) and those who had sub-threshold symptoms of mental disorder were offered an interview. In addition, 1 in 5 people with no mental disorder were randomly sampled for follow-up interview. Ethical approval for the survey was given by the Multicentre Research Ethics Committees in England. Participants gave informed consent before enrollment into the study.
Measures
Dependent variable
Presence of a depressive episode according to the International Classification of Diseases–10th Revision (ICD-10) was assessed at baseline and at the 18-month follow-up using the CIS-R (Lewis et al., 1992). This is an interviewer-administered structured schedule covering non-psychotic symptoms. The CIS-R includes initial questions about symptoms experienced in the last month, with those meeting this threshold being asked further detailed questions about more recent experiences. The CIS-R has a reliability between 0.74 and 0.91 (Lewis et al., 1992) and can be used to derive ICD-10 diagnoses by an algorithm.
Independent variable
An item from the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders–Fourth Edition (DSM-IV) Axis II personality disorders (SCID-II) (First et al., 1997) was used as the measure of MI. The item asks ‘do you have a lot of sudden mood changes?’ with the timescale for this symptom being ‘suffered this over the last several years’. This item in the SCID-II is designed to elicit the MI component of the DSM-IV borderline personality disorder criteria. Respondents can answer yes or no. This item has been used in a number of other studies to measure MI in a range of disorders (Marwaha et al., 2013a, 2014a), and a directly comparable question has previously been found to predict transition in people who are at risk of bipolar disorder (Angst et al., 2003).
Confounders
Because of the comorbidity between anxiety and depression as well as the fact that anxiety disorders may predate a depressive episode by some time (Moffitt et al., 2007), we controlled for anxiety symptoms using the CIS-R anxiety score.
To verify that MI was not simply a reflection of hypomania alternating with depression, we adjusted for hypomanic mood in the modeling. Hypomanic mood was assessed in relation to the past year in the first section of the Psychosis Screening Questionnaire (PSQ) (Bebbington and Nayani, 1995).
In addition, we controlled for age, gender, employment status, marital status and ethnic grouping since all of these have been associated with depression (Singleton and Lewis, 2003).
Potential mediators
Sleep at baseline was measured using components of the CIS-R, which includes five questions on problems related to the quality of sleep. These are as follows: having had problems with sleep for four nights or more in last 7 days, spent at least ¼ hour trying to get to sleep on the night with least sleep in the past week, number of nights spending >3 hours trying to get to sleep in the last week, sleeping for at least ¼ hour longer than usual on the night that the person slept the longest in the last week and number of nights sleeping for more than 3 hours longer than usual in the past week. We used the CIS-R total sleep score given both insomnia and hypersomnia, whether individually or co-occuring, are associated with depression (Soehner et al., 2014).
Alcohol misuse was measured using the Alcohol Use Disorders Identification Test (AUDIT) (Saunders et al., 1993) which uses the last year as the period of reference. As is usual, a threshold of 8 or more (representing hazardous and harmful drinking) between baseline and follow-up was used to indicate alcohol misuse.
Life events relating to interpersonal relationships were assessed at 18 months and referred to the previous 6 months. Divorce or separation and serious problems with a close relative or friend were coded (yes/no). We chose life events occurring closely with the 18-month time point as opposed to assessment at baseline given that the more recent the life event, the greater the risk of developing depression (Kendler et al., 1999).
Analytic strategy
To assess the association of MI with a diagnosis of ICD-10 depression (any severity), we used binary logistic regression. We first conducted the analysis on the cross-sectional dataset and then followed this with the same analysis on the 18-month follow-up data. In order to investigate whether MI at baseline was associated with new inception of depression at follow-up, we restricted the sample to those without depression at baseline. Conversely, to examine the effect of MI on maintenance of depression, we included those with baseline depression only. We did not exclude those with comorbid personality disorders in any analysis. Mediating variables are those hypothesized to be in the causal pathway while confounders are those outside of it.
Modeling proceeded in three stages. After producing unadjusted odds ratios (ORs), we next adjusted for socio-demographic characteristics (age, sex, marital status, employment status and ethnicity). Finally, we adjusted for hypomanic mood and anxiety.
We applied the –khb– (Karlson Holm Breen) command in Stata to complete multiple mediational analyses. This method implements a decomposition of the total effect of a variable into direct and indirect (i.e. mediational) effects (Breen et al., 2013) and can be used in logit models. In these analyses, the effects of socio-demographic confounders on the decomposition were controlled for.
A diagram of the conceptual model under test is displayed in Figure 1. Consistent with the analytic approach of other research completing multiple mediational analyses (Fisher et al., 2013), we initially inserted all mediators into the model to understand their combined effect. We then entered the mediators separately modeling if they were still significant. If they were not, we dropped them in further modeling, inserting only significant individual mediators into the final model explaining new onset depression.
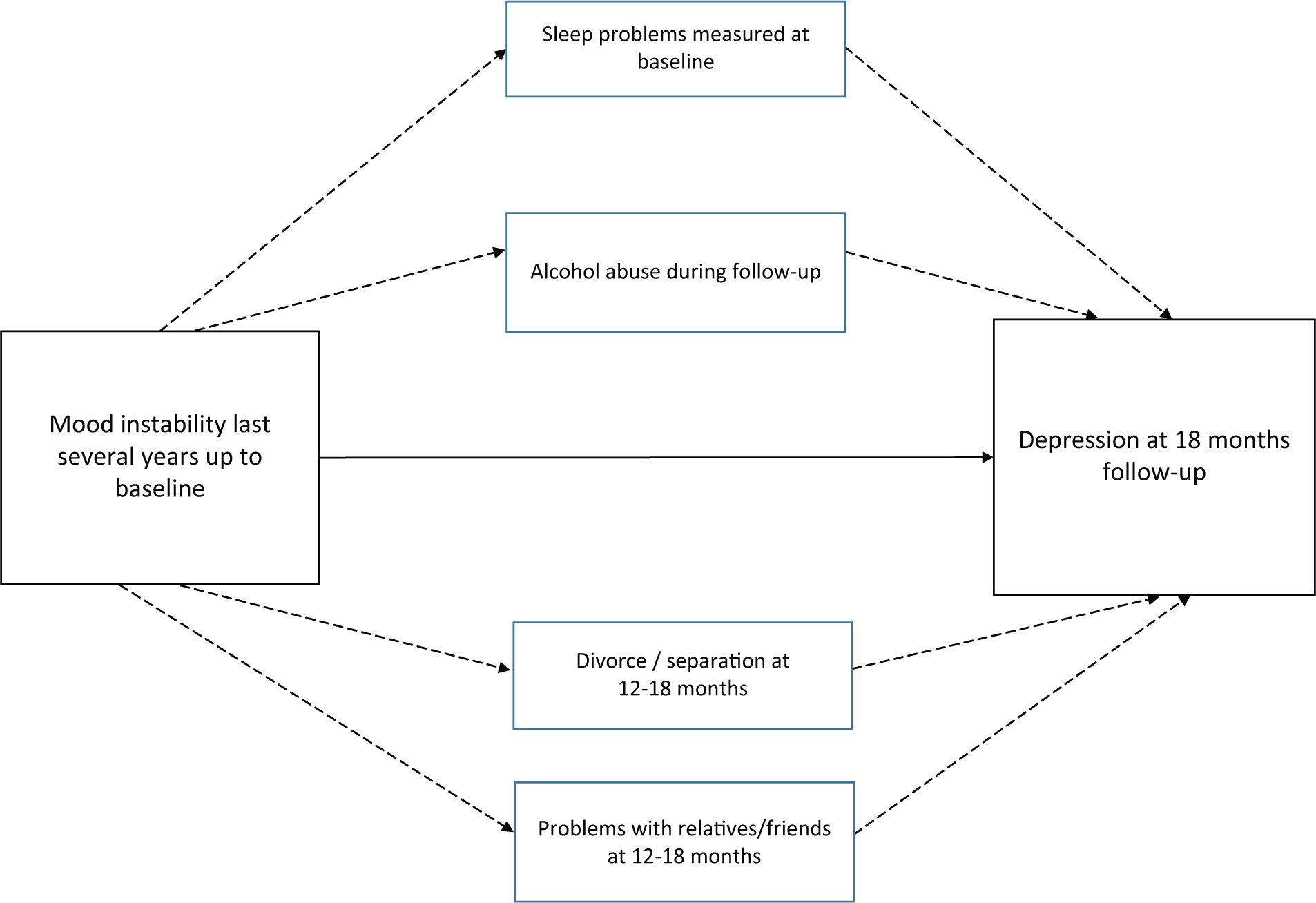
Conceptual mediation model under test. Solid arrow represents the direct effect. Dashed arrows represent the indirect effect.
In all analyses, data were weighted to take account of survey design and non-response, and full details are available in the main survey report (Singleton and Lewis, 2003). Regression and mediation analyses were carried out in Stata 13 for Windows.
Results
In the initial 2000 survey, 8580 persons were interviewed. At follow-up, 3536 persons were selected for follow-up, and 3045 were successfully contacted. In all, 79% (n = 2413) completed the follow-up interview. There were no significant differences in the CIS-R scores at baseline of responders and non-responders (Singleton and Lewis, 2003). The number/rate of ICD-10 depression (all severity) at baseline was 133 (2.6%). At follow-up, the number who continued to be depressed were 28 (22%), and new cases of depression were 74 (1.9%). All proportions are weighted.
Using the cross-sectional data, MI was associated with depression after adjusting for all confounding variables (OR: 5.28, confidence interval [CI]: [3.67, 7.59], p < 0.001). MI significantly predicted new onset depression at 18 months in the unadjusted analysis, and this association persisted after controlling for socio-demographic variables. While the effect was moderated by adjustment for anxiety and hypomanic mood at baseline, MI continued to significantly predict new inception of depression (OR: 2.43, CI: [1.07, 5.99], p = 0.042). MI at baseline was not associated with persistence of depression at 18 months in unadjusted analysis, so further analysis was not completed. The results of the regression modeling are summarized in Table 1.
The cross-sectional and prospective link between mood instability and depression.
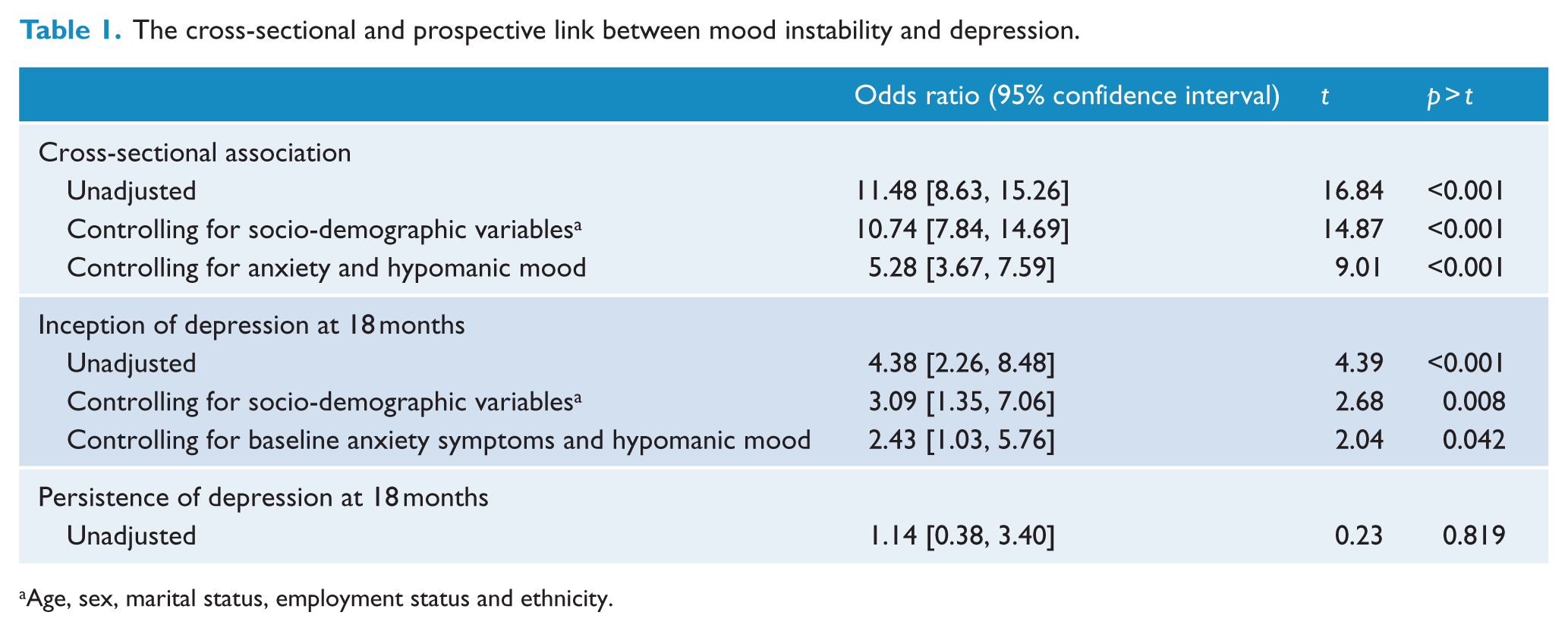
Age, sex, marital status, employment status and ethnicity.
The path analysis in which all potential mediators were incorporated into the model demonstrated a significant indirect effect (p < 0.001) and explained 33.12% of the link between MI and depression inception. In the mediation model in which only sleep was entered as a mediator, the direct effect of MI on depression and the indirect effect mediated by sleep were significant, as well as the total effect. Similarly, this was the case when assessing the influence of problems with close family or friends. When both sleep and interpersonal conflict was entered into the model, then their combined effect made the direct effect of MI non-significant. In individual analyses, divorce/separation and onset of alcohol abuse were not significant mediators, and thus were dropped from the final model. The final model indicates that poorer sleep and problems with close friends and family mediate 29.12% (p < 0.001) of the link between MI and a new episode of depression. Table 2 shows this three-staged mediational analysis.
Mediators of the association between mood instability and new onset depression.
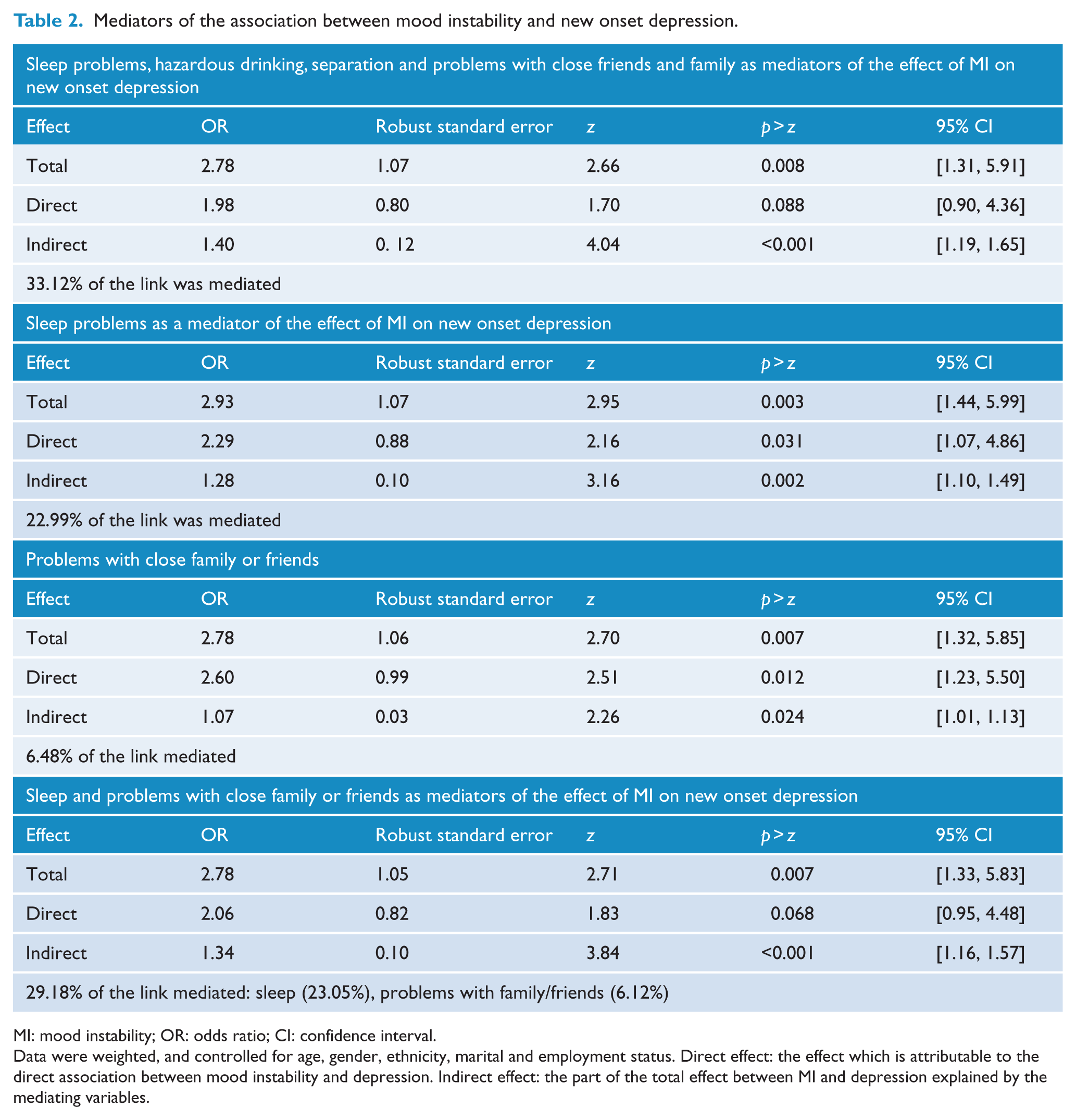
MI: mood instability; OR: odds ratio; CI: confidence interval.
Data were weighted, and controlled for age, gender, ethnicity, marital and employment status. Direct effect: the effect which is attributable to the direct association between mood instability and depression. Indirect effect: the part of the total effect between MI and depression explained by the mediating variables.
Discussion
Main findings
This study examines the association between MI and depression, both cross-sectionally and prospectively in a large population survey. Consistent with findings of a later cross-sectional survey in England (Marwaha et al., 2013a), MI was strongly associated with concurrent depression. As far as the authors are aware, MI has not been investigated previously as a predictor of depression using prospective epidemiological data. By doing so, part of our second hypothesis was confirmed in that MI is a significant precursor of a diagnosis of depression, after suitable adjustments for important confounds such as socio-demographic variables, anxiety and hypomanic mood at baseline. MI does not appear to predict persistence of a diagnosis of depression over 18 months. However, we may have had too small a sample size to detect this. A number of mediators were also explored in order to understand possible mechanisms in the pathway from MI to depression. Poor sleep as well as problems with close friends and family significantly mediated this relationship, whereas new onset alcohol problems and separation/divorce did not.
Theoretical and clinical implications
MI occurs in both children and adults. Significant difficulty in mood regulation (mood repair) is a feature experienced by children and adolescents who later go on to develop major depression in adulthood (Kovacs and Lopez-Duran, 2010). Our findings show that MI experienced in adulthood is also a significant factor in the inception of depression.
There are two possible ways to conceptualize this finding. First, MI might be a vulnerability trait for depression. Temperament is known to modify the response to stressful events possibly acting through differences in coping styles (Mezulis et al., 2004). Negative emotionality, a tendency for people to get angry, distressed and insecure easily after an unpleasant event, has been shown to predict increased depressive symptoms over time (Elovainio et al., 2014) mediated through increased exposure to adversity (Kendler et al., 2003). Problems with mood repair in childhood could be embedded into an emotionally unstable temperament of which MI forms one part, and this then acts to predispose to developing a multi-finality of outcomes including that of depression (Crowell et al., 2009). It is of course possible that there is a common neurobiological vulnerability to MI and depression. For example, both emotional dysregulation as well as major depression are associated with changes in the hypothalamic–pituitary–adrenal axis characterized by an increased cortisol response (Wingenfeld et al., 2010).
Second, MI rather than a trait predisposition could represent an early precursor symptom. Indeed, mood changeability has been identified to be part of the prodrome of depression (Jackson et al., 2003). It is likely many mechanisms are associated with the onset and maintenance of depression. Fluctuations in mood could be perceived subjectively as frequent, perplexing and distressing, leading to feelings of vulnerability, helplessness and eventually a more pervasive depressive syndrome (Bowen et al., 2013b).
With regards to indirect effects, our investigation of mechanistic factors revealed that sleep disturbance mediates a relatively large amount of the association between MI and depression, suggesting that MI may increase risk of subsequent depression via an increased likelihood of sleep disturbance. Sleep problems and depression are highly comorbid (Staner, 2010), and sleep problems have been found to be early symptoms of major depression (Batterham et al., 2012). Furthermore, evidence from a large epidemiological study suggests both insomnia and hypersomnia (as was coded in the current study) are strongly associated with depression (Soehner et al., 2014).
MI results in, or is coexistent with, a delayed return to emotional baseline (Marwaha et al., 2014b). This lack of an ability to attenuate a strong emotional state means that cognitive arousal may spill over into the night time upsetting sleep patterns (Selby et al., 2013). Poor sleep quality itself may produce or exacerbate MI (Bowen et al., 2013a), setting in motion a circular cascade of dysregulation. In turn, sleep problems (i.e. hypersomnia and insomnia) either coinciding with or subsequent to MI may increase risk of depression. In combination with the effects of problems with family and friend, sleep difficulties were more powerful than the direct effect of MI in the genesis of depression. Further research is required in order to fully elucidate and understand the reciprocal associations between MI and sleep disturbance, and their link to new onset depression.
The effects of MI and sleep are likely to be linked to shared abnormalities in biological substrates, notably central serotonin and noradrenergic transmission (Adrien, 2002). Serotonin has multiple functions in the central nervous system (CNS) including in the regulation of affect and the sleep–wake cycle by modification of rapid eye movement (REM) sleep or wakefulness (Monti, 2011). The link between sleep abnormalities, depression and MI is provided by the finding that variation in the 5-HT transporter gene has been linked with neuroticism (Canli and Lesch, 2007), a core part of which is MI (Bowen et al., 2012). Prospective cohort studies are needed to help further delineate the temporal associations between mood dysregulation, sleep disturbance and depression (Winsper and Tang, 2014).
Interpersonal problems with relatives and friends mediated the association between MI and depression. Our findings confirm the previously suggested specific association between MI and interpersonal problems (Miller and Pilkonis, 2006) and in part may relate to findings that a fluctuating mood state is also linked with interpersonal sensitivity and impulsiveness (Perugi et al., 2003). It is likely that this pattern of emotional functioning will lead to interpersonal problems within close relationships and that these can then act as a trigger for depression.
Onset of alcohol abuse over the follow-up period was not an important mediator of the association between MI and new onset depression. Our hypothesis that people with MI may try to self-medicate with alcohol and this could lead to depression was not supported. It was surprising that divorce was not a significant mediator. It may be that a major life event such as divorce encompasses such a complex array of psychological and social processes that our marker of MI was not powerful enough to exert an effect.
Our findings indicate identification and modification of MI and sleep problems have the potential to reduce the incidence of depressive episodes. However, there are considerable challenges to effecting change. MI is poorly assessed and managed by mental health professionals with needs often not being met (Bilderbeck et al., 2014). The reasons for this may be manifold, including an under-appreciation of the significance of MI, lack of a settled method to clinically assess it and the issue of when, why and how to offer intervention.
Currently, then, the science around measurement of MI and when to treat is underdeveloped. In such a situation, interventions targeting MI need to be low risk and high benefit. One such example is to consider the place of regular exercise. As well as its general health benefits, physical activity reduces MI (Bowen et al., 2013a), and there is evidence for its treatment effect in depression and a range of mental health problems (Rosenbaum et al., 2014). In those who have recovered from previous episodes of depression, now presenting with MI and sleep problems, there is a rationale for the further investigation of the usefulness of social rhythm therapy, already found to be effective in reducing relapse in bipolar disorder (Frank et al., 2005). It is also of interest that effective mindfulness based therapies for depression may operate through reducing affective reactivity (Kuyken et al., 2010). Given the connection between sleep disturbance and MI, another method is to target sleep. Innovative approaches using Internet-based cognitive behavioral therapy (CBT) for insomnia are under investigation and may prove helpful in preventing the onset of depression (Gosling et al., 2014).
Limitations
The study had a number of limitations. Although MI has an objectively observable behavioral component, it is primarily subjectively perceived. Therefore, our use of a self-report item to measure MI was appropriate in the context of a large epidemiological survey. It is also acceptable to participants as very few (n = 25) people refused to answer it in the cross-sectional survey, and its use in studies of a variety of disorders (Marwaha et al., 2013a, 2014a) supports the construct validity of the question. While practical for a longitudinal epidemiological study, our results are limited by the use of a single-item question to assess MI. The question from the SCID used to elicit MI uses a reference timeframe of ‘the last several years’; therefore, we cannot be sure that MI was being experienced currently when assessed at baseline. The measure of MI used emphasizes mood variability as opposed to intensity. It has been suggested that MI should be fully specified as intensity, variability and level of control (Marwaha et al., 2014b), and further studies using this more comprehensive measurement paradigm are an important next step. Furthermore, MI was not assessed at follow-up, so we were unable to examine whether it accompanied incipient and persistent depression.
We did not find that MI was associated with maintenance of depression. It may be that we had low power to detect this association given that only 22 people continued to be depressed from baseline to follow-up. Further studies with a larger sample of people with persistent depression are required in order to corroborate our findings. It is, however, unlikely that this negative finding is explained by the absence of MI in the context of a depressive episode, given that they are commonly associated. There was a degree of temporal overlap between the assessment of the mediator variables and MI and depression, meaning that we cannot be sure that mediators such as sleep problems always followed MI. Finally, sleep may have an effect on the likelihood of interpersonal problems with close family and friends and vice versa (Bernert et al., 2007), but our mediational analyses could not take account of this.
Conclusion
In conclusion, MI is a precursor to depression, and its effect is mediated by sleep problems as well as interpersonal problems with close friends and family. The findings are highly relevant to the prevention and treatment of this mental disorder. Even with optimized care and delivery of services, it has been estimated that only up to 30% of the burden of disease attributable to mental disorders can be prevented (Andrews et al., 2004). This makes a powerful argument for a switch of research and clinical attention to prevention and early intervention targeting factors such as sleep and MI.
Footnotes
Acknowledgements
We would like to acknowledge the UK Data Archive and the National Centre for Social Research as the data collectors and depositors of the study. The National Centre for Social Research and the University of Leicester were the Principal Investigators of the Adult Psychiatric Morbidity Survey. They bear no responsibility for this further analysis or interpretation of this public dataset.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.