
Abstract
It is argued that not intervening at an early stage could lead sufferers of a psychotic illness towards greater social isolation causing decompensation and subsequent hospital admissions. A number of authors have suggested early intervention programs that can be delivered to patients experiencing their first episode of psychosis as a way of minimising hospitalisation and improving the patients' functioning within the community [1–3]. These programs have stressed the importance of ‘best practice’ treatment which include cognitive–behaviour therapy, individual and group psychotherapy, social and life skills development, low dose atypical neuroleptic medication and family therapy and psychoeducation. In order for treatment to be effective, the delivery of services has to be intense and multimodal.
A great deal of attention has been paid to factors which may predict outcomes for patients who have schizophrenia. Predictors such as patient's educational level, gender, age of onset and length of illness have been used to predict patient outcome. Previous research has demonstrated that premorbid levels of functioning, including social and psychological factors as well as biographical variables such as age and gender have been associated with poorer patient outcome [4,5]. One such predictor that has demonstrated a relationship with treatment outcome and hospital admissions is the length of duration of untreated illness defined as the time of interval between symptom onset and formal psychiatric treatment [6]. Studies have demonstrated that patients with longer untreated illness have higher relapse rates [7] and shorter community survival [8]. Though this may be the case within early psychosis populations, none of these studies have sought to investigate whether these predictors of survival are equivalent in other populations of patients who have more established psychotic illness and who have received similar intervention treatment.
This study has two purposes. First, to identify whether community survival functions are equivalent among patients with their first episode of psychosis and those with chronic schizophrenia after intensive community-based case management intervention. Though the programs are designed specifically for their respective populations, both employ similar assertive community case management treatment and medical management regimens (i.e. the emergence of atypical antipsychotic medication as a treatment for both early psychosis and chronic populations). Although both populations are similar in typology, the concern is whether clients with early psychosis mimic similar community survival trajectories when provided equivalent assertive community treatment.
The second purpose is to identify what demographic variables and factors of social and life skill functioning at the initial stages of treatment contribute to community survival between the two populations. Such information can shed some light on whether community survival is essentially a function of treatment or a function of patient characteristics.
Method
The study compared the survival within the community of 42 schizophrenia subjects with 49 early psychosis subjects after receiving intensive community-based case management. Both groups were placed within their respective programs: one for long-term chronic mentally ill, the other an early psychosis system of care. In this study both the early psychosis program and the program for those with chronic schizophrenia use comparable elements of assertive intensive community case management defined by Kanter [9]. The early psychosis program had a half-time consultant psychiatrist and psychiatric registrar, as well as a clinical psychologist, social worker and two community mental health nurses. Subjects treated with intensive case management for chronic schizophrenia had a similar team structure without direct assistance of a clinical psychologist and with one additional social worker. Each subject in the study was assigned a case manager who was primarily responsible for the overall clinical management of the patient. Caseloads for each case manager were capped at 10 patients with assertive community treatment including home visits, accommodation support, vocational assessment, supportive counselling, family psychoeducation, social and living skills development and recreation and leisure activities. Once to twice weekly home visits were common to both treatment programs. Within 4 weeks of receiving a patient within the program, case managers were asked to provide information on what treatment was being delivered to the patient out of a possible 15 options. Each case manager was given an operational definition of each treatment type to reduce rater variability. A sum of all 15 treatments were calculated to give an overall number of treatments received. The 15 treatments were then divided into 5 treatment types including (i) individual therapy, which included specific focused individual work, cognitive–behavioural focused therapy, and supportive counselling, (ii) group therapy, which included group work, family therapy and psychoeducational groups, (iii) medical treatment involving medical consultation, drug therapy and inpatient treatment, (iv) assessment work involving accommodation assistance, legal advocacy and vocational training, and (v) social skills development such as recreation and living skills. Each subject could receive a maximum of three treatments in each treatment type. Overall treatment intensity was evaluated using an analysis of variance (ANOVA) between the two intensive community treatment programs and total number of treatments received.
Kaplan–Meier survival analysis was used to compare the programs by estimating the risk of relapse after receiving intensive community case management. Relapse was defined as any subsequent admission into the Alma Street Centre, Fremantle Hospital, an approved psychiatric hospital where the subjects received treatment. All non-psychiatric admissions to hospital were ignored in the survival function. The survival function was generated using the actuarial method by dividing the time period into 36 months. Censored cases were defined as those subjects who did not require psychiatric hospital admission during the course of the study. Readmission periods were calculated in monthly observations from the patient's entry point into their respective intensive case management program. Comparison of the survival curves was performed using the log-rank test.
Life table analysis was performed on both groups to evaluate the percentage of subjects who required readmission throughout the 36-month period. The number and percentages of subjects hospitalised at each monthly interval from among those remaining in the study at that month were computed.
A Cox-regression analysis was used to investigate whether sex, age, social and occupational functioning measured by the social and occupational functional assessment score (SOFAS) [10], living skills measured by the life skills profile score (LSP) [11] and overall role functioning measured by the role functioning scale (RFS) [12] predicted community survival. An increase in scores denotes an improvement in functioning for all instruments. All predictors were entered simultaneously into the survival equation. Assessments of each functioning predictor was made by the case manager assigned to each subject within the first 4 weeks of commencing intensive case management. These scores were subsequently used to identify which variables contributed to community survival.
Patients classified in the schizophrenia group had to meet the DSM-III-R diagnostic criteria for schizophrenia and required at least three hospital admissions in the 12 months prior to receiving intensive case management. All diagnoses were prescribed by the treating consultant psychiatrists from each program and derived from case notes and clinical interviews.
Results
Patient characteristics
As in most early psychosis populations, diagnosis was heterogeneous [13,14], however, subjects had to meet the requirement of presenting psychotic features or a subsequent admission for a psychotic episode before being accepted into the early psychosis program. Of the 49 early psychosis subjects 18.4% were diagnosed with schizophrenia, 12.2% with schizophreniform psychosis, 8.2% with delusional disorder, 8.2% with schizoaffective disorder, 12.2% with substance-induced psychosis, 10.2% with bipolar affective disorder with psychotic features, and the remainder with depressive related illnesses. Chi-squared analysis and analysis of variance (ANOVA) was performed to observe population difference in gender, age and functioning on the predictor variables. As shown in Table 1, no gender differences were observed between the two groups. As expected however, significant differences were observed with age (F = 7.21, df = 1, 89, p = 0.009), and duration of illness (F = 73.42, df = 1, 89, p = 0.000) indicating that subjects with schizophrenia were significantly older and had an average length of illness 10 years more than their early psychosis counterparts.
Patient characteristics and predictor variables
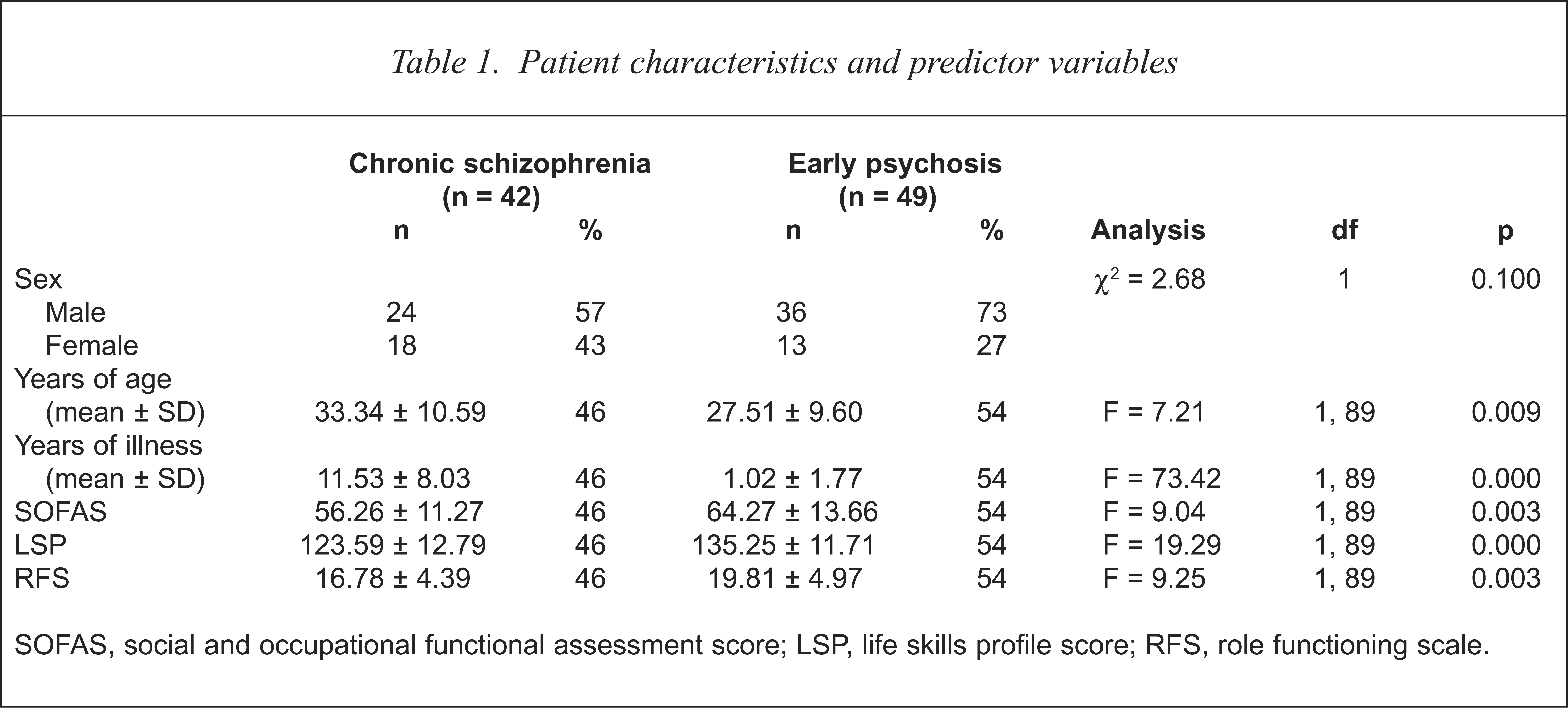
SOFAS, social and occupational functional assessment score; LSP, life skills profile score; RFS, role functioning scale.
Initial scores on the SOFAS (F = 9.04, df = 1, 89, p = 0.000), LSP (F = 19.29, df = 1, 89, p = 0.000) and RFS (F = 9.25, df = 1, 89, p = 0.000) were significantly lower for subjects with schizophrenia, indicating that these subject had significantly lower levels of role functioning and life skills, than those with first episode psychosis.
Treatment characteristics
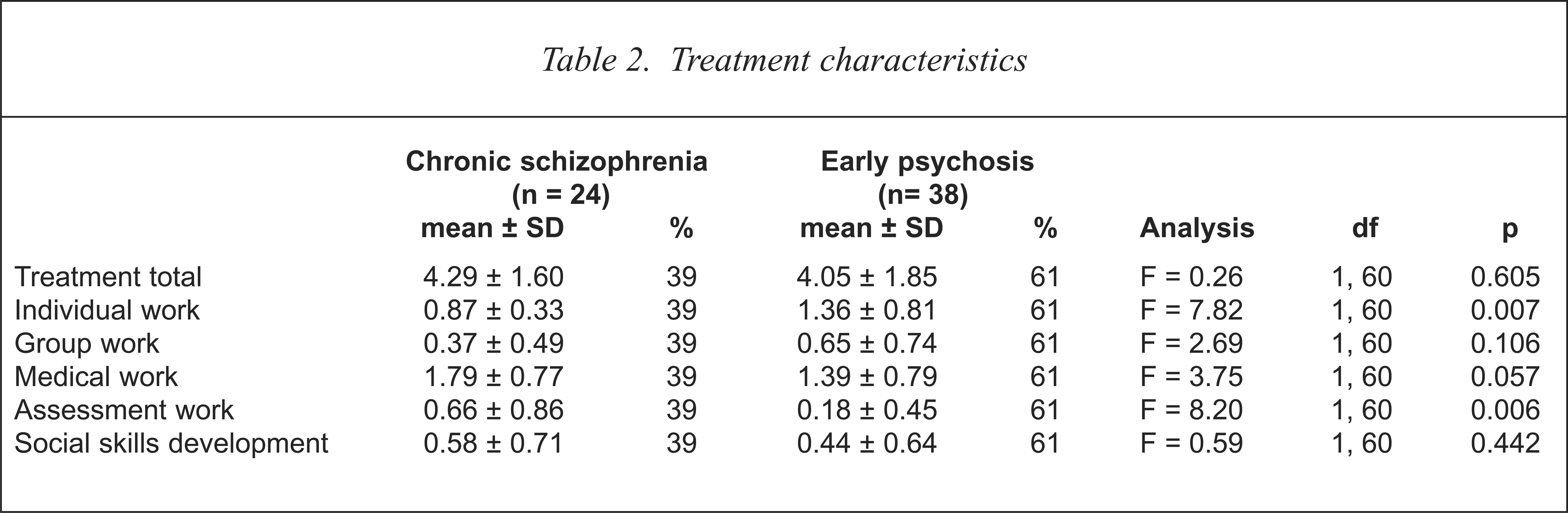
The total number of treatments received by the two groups was not significantly different (Table 2). However, early psychosis subjects received significantly more individual therapy treatment (F = 7.82, df = 1, 60, p = 0.007) and those in the chronic group more assessment work (F = 8.20, df = 1, 60, p = 0.006) including legal advocacy and accommodation assistance. The amount of medical treatment, group therapy and social skill development interventions were equivalent between the groups.
Treatment characteristics
Kaplan–Meier survival analysis
Figure 1 illustrates the Kaplan–Meier survival curves indicating time to rehospitalisation between subjects with schizophrenia and early episode psychosis. The estimated risk of remaining in the community for the two groups within the 3 year time period was 49% for subjects with early psychosis and 33% for those with schizophrenia. When the survival functions were compared over the time period the log-rank Chi-squared test did not reach significance (log-rank χ2 = 1.31, p = 0.252) indicating the survival function to be equivalent between the groups. Observation of Figure 1 illustrates that the survival curves have equivalent trajectories up to the first 12 months of treatment with the curves splitting after this point with survival rates remaining approximately 50% for early psychosis subjects up to the 36-month period. The survival rates within the community for subjects with chronic schizophrenia continue to fall past the 12-month period with only a third of the population remaining in the community at the end of the study period.
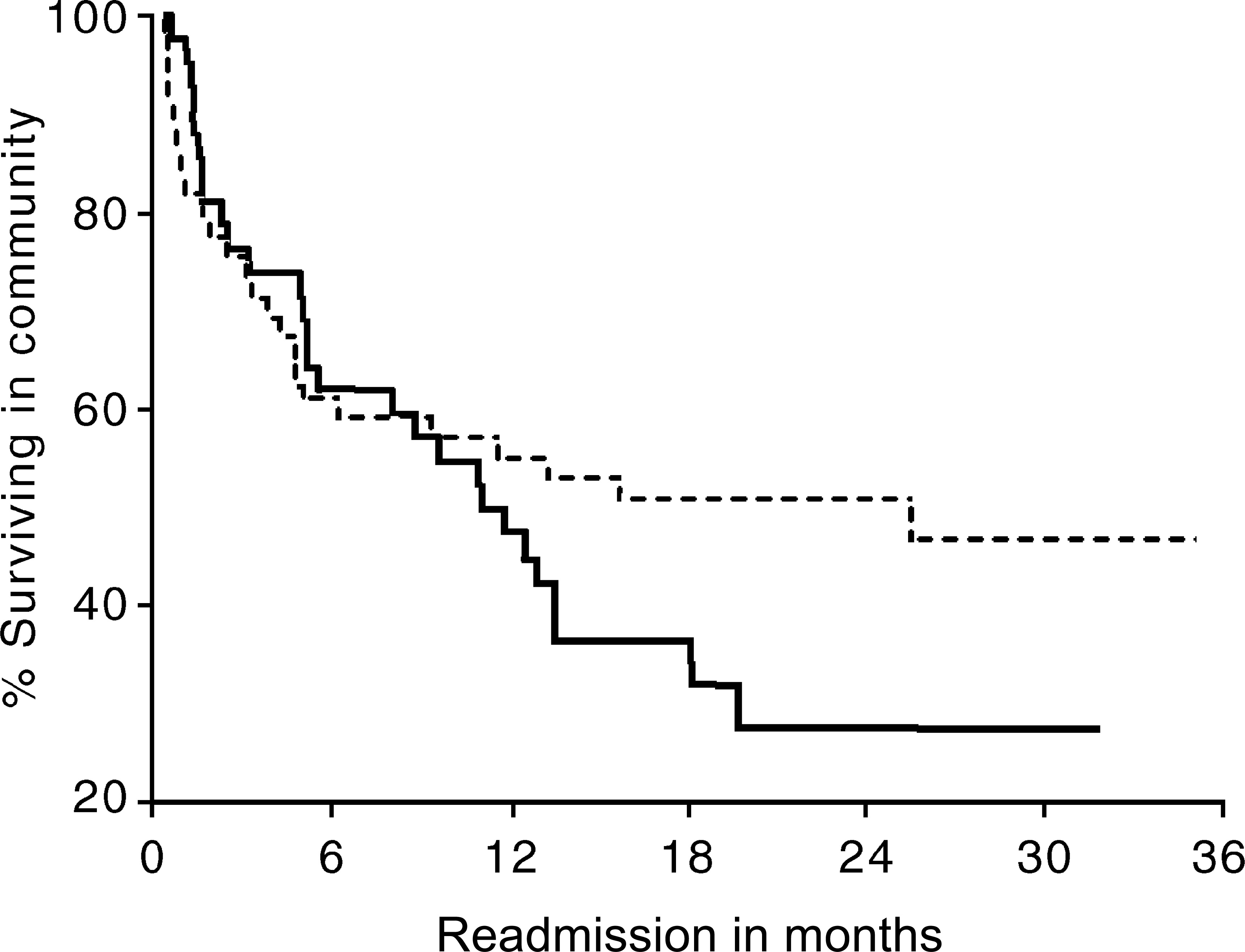
Community survival functions of early psychosis (—-) and schizophrenia (——)
Life table analysis
Fewer relapses were observed among subjects with early onset psychosis, the median survival time was 25 months compared with 11 months for the schizophrenia group. Of the 49 cases in the early psychosis group, 24 (48.98%) were censored in the study period while of the 42 subjects with schizophrenia, 14 (33.33%) remained censored.
Cox regression analysis
Age, gender, SOFAS, RFS and LSP scores were simultaneously entered into the Cox regression model. The change in the partial likelihood function was significant (χ2 = 11.46, df = 5, p = 0.049) indicating the model to be significant in predicting survival. Observation of the predictor variables (see Table 3) indicated that living skills measured by the LSP predicted community survival. The coefficient for the LSP score indicated that increased scores in the LSP (denoting increased living skills) improved community survival. The confidence intervals of the LSP fell below 1 for both upper and lower limits (Lower, 95% CI = 0.9395; Upper, 95% CI = 0.9859) indicating that the LSP variable is related to survival [15].
Results of Cox regression analyses for association between social functioning predictor variables and time to remission for subjects with early episode psychosis and schizophrenia
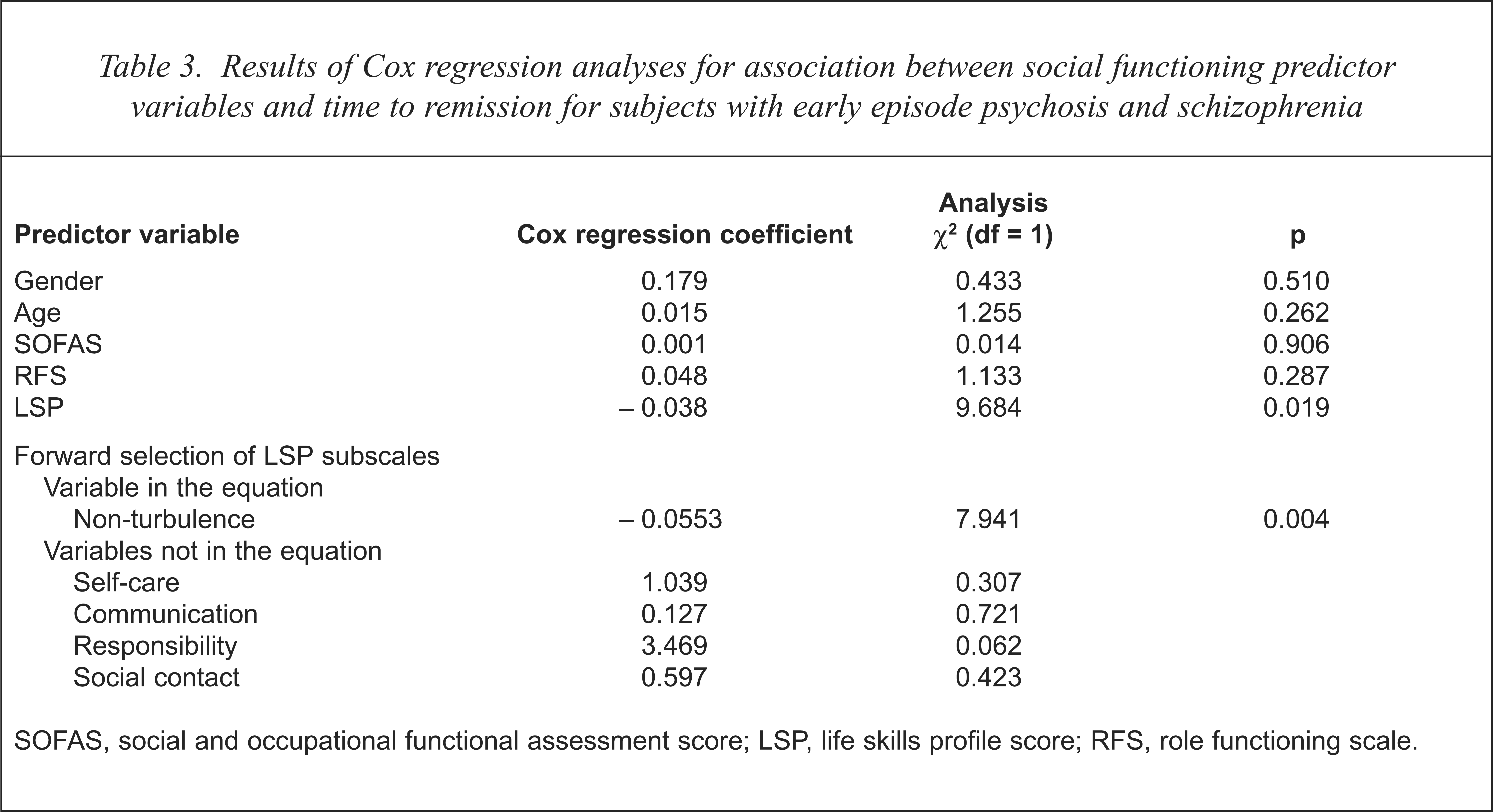
SOFAS, social and occupational functional assessment score; LSP, life skills profile score; RFS, role functioning scale.
A further Cox regression analysis was performed on the four subscales of the LSP suggested by Parker [16] including self-care, communication, non-turbulence, responsibility and social contact. The forward selection method was chosen to observe the unique contribution of each predictor with community survival. The residual Chi-squared for the model was accepted (χ2 = 13.43, df = 5, p = 0.019) indicating that the model was related to survival. The subscale of non-turbulence observed the smallest significance level and hence was entered in first (see Table 3). The direction of the coefficient of non-turbulence to time in the community indicated low turbulence predicted longer community survival. When the second step was entered accounting for the variance already explained by non-turbulence the residual Chi-squared did not reach significance consequently rejecting the other subscales as predictors of community survival. Observation of items within the non-turbulence subscale included violence to others, violence to themselves, irresponsible behaviour and the like. This subscale could be interpreted to be related to antisocial behaviour [17]. This subscale denotes the extent to which subjects interact with others within the community in a non-threatening or social manner. A Pearson correlation matrix revealed that, among the subscales, non-turbulence was the only subscale that displayed a strong correlation to time spent in the community (r = 0.30, P = 0.004, n = 89) apart from the LSP global score (r = 0.21, p = 0.049, n = 83). The direction of the correlation indicates that improved non-turbulence scores are associated with longer survival in the community. An analysis of covariance (
Discussion
The study attempted to identify whether patients with an early episode of psychosis survived longer or equivalent in the community when receiving comparative intensive community case management compared with subjects with chronic schizophrenia. Levels of social and life skills functioning were recorded at commencement of treatment to identify whether these aspects of functioning predicted community survival. The study demonstrated that subjects with early psychosis received more individual therapy than subjects with schizophrenia, while schizophrenia patients received more advocacy and assessment work. These differences are expected when one investigates the main emphasis of treatment with the different populations. When overall treatment numbers were analysed there was no difference between the groups. The survival analysis demonstrated that although survival functions were equivalent between the two programs, half the early psychosis subjects survived in the community for 19 months while half of the schizophrenia subjects survived for 11 months before requiring rehospitalisation. The survival function also demonstrated equivalent survival trajectories up to 12 months with just under a half of the early psychosis subjects surviving in the community up to the 36-month period. For the equivalent time period only one-third of clients with schizophrenia remained in the community. The survival functions indicated that if an intensive case management treatment program can manage to keep patients with early psychosis out of hospital for 12–18 months they are likely to keep them out for a further 18 months. By 18 months, one-half of the early psychosis subjects remain in the community while three-quarters of subjects with long-term schizophrenia within the same time period required hospitalisation during the study period.
In order to investigate predictors of community survival, measures of social and occupational functioning (i.e. SOFAS and RFS) and living skills (LSP) were entered into a Cox-regression model. The results indicated that the life skill profile score and in particular the subscale of non-turbulence predicted survival. Non-turbulence can be best described as the factor within the life skill profile instrument which measures antisocial behaviour [17]. The regression model revealed that those clients with high antisocial behaviour were more likely to require hospitalisation.
There have been many discussions in the literature which argue that early intervention and treatment of emerging psychosis can reduce the risk of relapse and subsequent readmissions to hospital [1,13,18]. This study attempts to investigate this claim comparing equivalent intensive community-based treatments both of early psychosis subjects and of subjects with long-term schizophrenia. The present study demonstrates that the trajectory of relapse is equivalent between both groups up to the 12 month time period. Subjects with early psychosis show superior community survival after this 12 month time frame (see Fig. 1).
The difficulty is to identify whether this continued community survival is attributable to intensive treatment or to the social and life skills of clients prior to entering intensive community treatment. Indeed, the study demonstrated that at the initial stages of intensive community case management subjects with early episode psychosis displayed superior life skills and social and role functioning than those with schizophrenia. The regression analysis demonstrated that community survival is related to the degree of antisocial and disruptive behaviour displayed by patients at early stages of intensive community case management. It is quite possible that the level of life skills possessed prior to treatment predict relapse, regardless of a patient's diagnosis or length of mental illness, as an
The life tables indicated that treatment gains can be observed if patients who suffer from early psychosis are kept within the community with intensive case management past the first 12 months of treatment. Half of the early psychosis sample were able to stay within the community for up to 18 months with only one other subject requiring hospitalisation in the remaining 18 months. A previous 3 year prospective survival analysis study demonstrated that the mean duration before initial treatment among 70 patients with early psychosis was 52 weeks [6]. Prolonged community survival is improved considerably if patients remain in the community within the first 12–18 months of receiving treatment. The window period appears to be the first 12 months, as Figure 1 illustrates survival trajectories are equivalent for both subjects with early psychosis and schizophrenia up to this point, then the survival trajectories start to divide. The object of continued study should be whether these gains continue past the 3-year period. One such study that calculated the survival function for 5 years demonstrated that 80% of 51 early psychosis subjects required hospitalisation within this time [19]. If one is to look at life skills as a predictor for relapse then the evidence indicates that antisocial behaviour contributes to relapse among both subjects with early psychosis and schizophrenia.
The limitations of the study are pronounced when one considers whether changes to medication regimes and other predictors other than social functioning and living skills contribute to community survival. Other limitations may lie also in the size of each group within the Cox Regression. It is possible that with greater numbers in each group, differences in survival function between chronic schizophrenia and early psychosis populations may have been detected. Larger group membership would allow for more sophisticated regression models to identify the contribution of these factors to community survival. Further research is required in this area by employing more sophisticated prediction models that include variables other than sociodemographic, social functioning and living skills variables as predictors of community survival. This would require tracking treatment type, treatment intensity, changes to medication regimes and the like throughout the course of intensive community treatment as predictors of community survival. This study demonstrates that techniques like survival analysis and Cox-regression, which are under-utilised in psychiatric research, can be useful in determining the predictors of prolonged community living among psychiatric populations receiving intensive community treatment, and can go some way in identifying treatment fidelity.