
Abstract

It is a critical time for the field of traumatic stress. Table 1 summarises the recent and proposed changes to the diagnostic criteria for post-traumatic stress disorder (PTSD) across the two most influential diagnostic systems, the Diagnostic and Statistical Manual of Mental Disorders (DSM) and the International Classification of Diseases (ICD). These may have unintended consequences which are particularly relevant in the Australian context.
Overview of the post-traumatic stress disorder diagnostic criteria for DSM-5 and ICD-11. ICD-11 criteria for PTSD adapted from Morina et al., 2014.
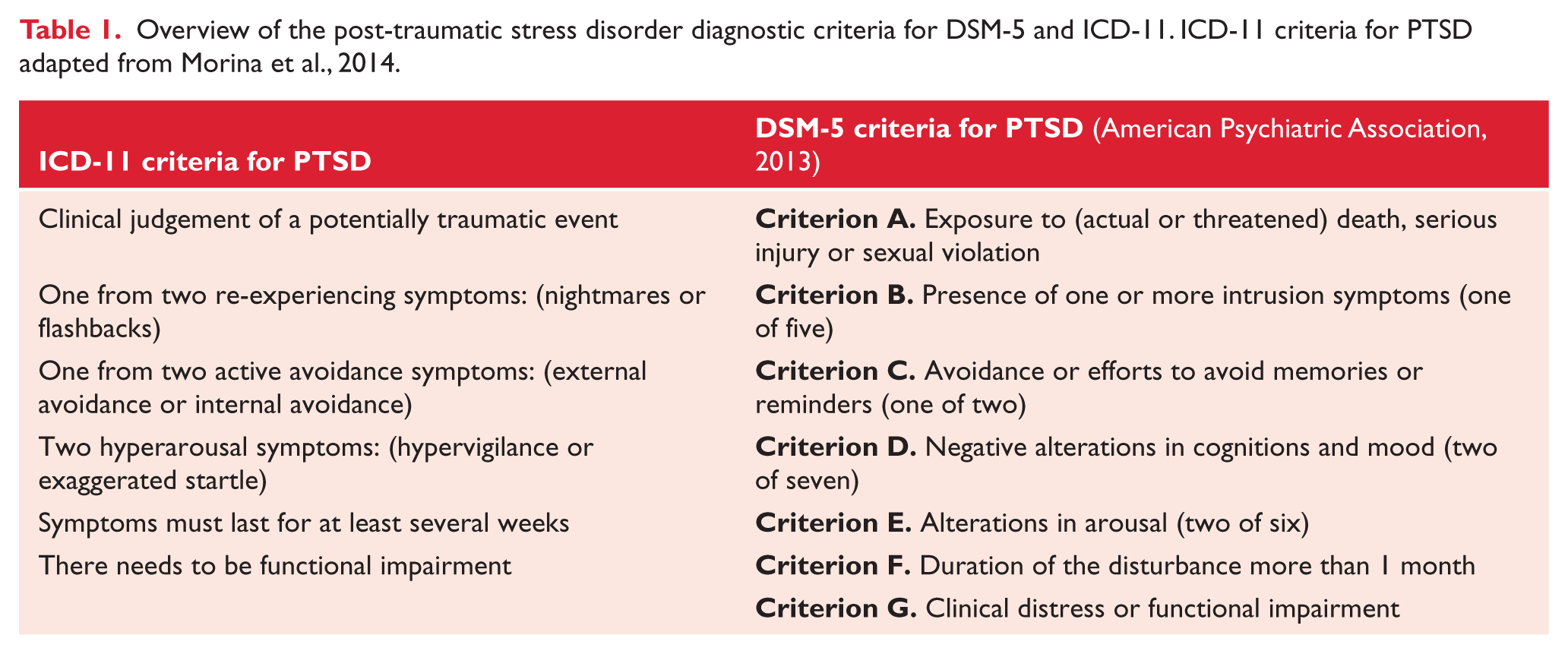
These two key nosological entities are taking markedly different directions leading to a divergence of the PTSD construct across systems. The modifications to the diagnostic criteria for PTSD in DSM-5 were motivated by intent to capture a more comprehensive clinical profile of traumatic stress responses. As such DSM has modified the wording of certain criteria and increased the number of symptoms available to the diagnosis, from 17 to 20 (American Psychiatric Association, 2013). Alternatively, the proposed changes in ICD-11 aim to refocus the diagnosis of PTSD to its essential features, and to increase its ease of use for clinicians. It has therefore reduced its available symptom criteria from 14 symptoms to six (Morina et al., 2014).
There are two key considerations by which to assess the potential impact of the changes to diagnostic criteria: what does this mean for prevalence rates within each system?, and what does this mean for comparability across systems? First, research investigating prevalence rates comparing DSM-IV and DSM-5 suggest they are generally similar. In our study of a large severe injury sample we found no difference in prevalence rates using DSM-IV or DSM-5 criteria (O’Donnell et al., 2014). However, in our study and those of others (e.g. Hoge et al., 2014) a moderate/large proportion of those meeting PTSD criteria under DSM-IV failed to meet criteria under DSM-5, and vice versa. This suggests the PTSD phenotype being assessed may have changed with the latest DSM iteration.
Prevalence rates between ICD-10 and ICD-11 may be somewhat different. There is early evidence to suggest that prevalence rates may drop significantly under the ICD-11 criteria relative to ICD-10 (e.g. O’Donnell et al., 2014). This is in contrast to the early commentary around ICD-11 suggesting that PTSD prevalence rates associated with ICD- 11 would remain constant (Morina et al., 2014). It is still early days in terms of research examining prevalence rates using ICD-11 criteria, but it may be that simplifying the PTSD diagnosis will have unintended consequences.
The second issue to consider is what the difference in criteria (between DSM-5 and ICD-11) means regarding the PTSD phenotype being assessed. The finding from our study, with ICD-11 prevalence rates being only one-third the rate of DSM-5 prevalence rates (O’Donnell et al., 2014) suggests variation in phenotypes across classification systems. Our study suggests that ICD-11 sits primarily as a subset of DSM-5 with only 11% of those who met ICD-11 criteria failing to meet DSM-5 criteria. However a large multinational study by Stein et al. (2014) found approximately 30% of those who met ICD-11 criteria failed to meet DSM-5 diagnosis, which raised the question as to whether the systems are looking for the same phenotype.
Initially the differences between the two systems may appear unimportant as the USA generally utilises DSM while Europe/UK tends to use ICD. However difficulties arise in countries like Australia where, for example, the hospital systems tend to adopt ICD, while most domestic research tends to follow DSM. While this dichotomy was also true for previous iterations of both classification systems, the intentional divergence in direction between the two nosologies increases the difficulty in synchronising information across them. For example, will PTSD treatment protocols developed under ICD-11 be as efficacious for those diagnosed using DSM-5 criteria? Further research that clarifies the similarity or difference between PTSD phenotypes across classification systems is necessary to fully understand the impact of using treatment research from one system for a person diagnosed under the alternative criteria.
Similarly, differences in diagnostic criteria may impact compensation systems within Australia. The requirements within a number of compensation systems (e.g. Workcover, Transport Accident Compensation, Victims of Crime, Military Rehabilitation and Compensation) where PTSD is an important issue are not consistent or clear on the criteria necessary to be eligible for compensation. Veterans who apply for healthcare based on mental health conditions can be diagnosed under DSM-IV and DSM-5 criteria. Others such as the Victorian Workcover Authority ‘Certificate of Capacity’ provide no clear instructions on the diagnosis of PTSD. With emerging evidence suggesting marked difference in PTSD prevalence rates based on diagnostic classification systems, the decision to prefer one over the other may have considerable financial, legal and personal implications for those seeking compensation under various schemes.
Finally the divergence between the ICD and DSM diagnoses will complicate comparing North American research, which predominantly applies DSM criteria, with that from UK/Europe, which generally follow ICD. While an argument could be made for the benefit of structuring competing constructs to facilitate uncoveringthe true nature of PTSD, it may infact muddy the empirical waters. Importantly, the clinical, compensatory and research ramifications for places like Australia, which utilise both diagnostic systems, need to be considered.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.