
Abstract
Objective:
Personality has been associated with a variety of outcomes in adulthood. Most of the literature related to mental state disorder and personality is cross sectional.
Methods:
Data from more than 900 participants of the Christchurch Health and Development Study (CHDS) were examined. Extroversion and neuroticism were measured at 14 years old and social outcomes at age 30. The presence of mental state disorder between 18-30 years old was identified. Multiple potential confounders in childhood were included in the analysis.
Results:
Neuroticism at fourteen was significantly correlated with multiple environmental exposures whereas extroversion had relatively few associations. Regression analysis found that neuroticism at 14 predicted depression, anxiety, suicidality and overall mental health problems at 30 as well as poor self-esteem but not relationship quality or wellbeing. Extroversion at 14 predicted alcohol and drug dependence and overall mental health problems, but also predicted improved social wellbeing, self-esteem and relationship quality at 30.
Conclusions:
In this analysis extroversion interacts with significantly fewer environmental factors than neuroticism in predicting adult outcomes. Neuroticism at 14 years predicts poorer mental health outcomes in adulthood. Extroversion in childhood may be a protective factor in the development of mental disorder other than alcohol use disorders. Extroverted adolescents have more positive social outcomes at 30 years.
Keywords
Introduction
The importance of personality and its impact in the development and wellbeing of adults has been a subject of much research over the last three decades in non-clinical (Caspi and Roberts, 2001; Klimstra et al., 2009; Cohen et al., 2005) and clinical (Clark, 2005; Zanarini et al., 2003; Skodol et al., 2005) populations. It is increasingly apparent that personality characteristics, although changing from adolescence (Klimstra et al., 2009; Johnson et al., 2000) through early adulthood, (Roberts et al., 2001) maintain a rank-order constancy (Roberts and DelVecchio, 2000), implying a degree of stability that increases over time. What taxonomy is most accurate and the number of personality factors of greatest scientific and clinical utility is debated (Mulder et al., 2011; Larstone et al., 2002). Research across normal and abnormal personality tends to cluster into the ‘big five’ domains described by McCrea and Costa (1997). The importance of two of these domains (conscientiousness and openness) in clinical samples appears to be minor. Although a ‘big three’ model fits some data two personality factors are most commonly described as superordinate, spanning normal and abnormal personality and fitting with most accuracy (Markon et al., 2005) . These have been described as an alpha and beta factor (Digman, 1997). The alpha factor links to Agreeablness, Conscientiousness and Emotional Stability (or ‘negative neuroticism’) as described by the ‘big five’. Digman hypotheses that the alpha factor links to social desirability or socialization. Alternatively this factor may be considered to relate negatively to Eysenck’s neuroticism and to a lesser degree psychoticism (Eysenck, 1978). The link to psychoticism is not always reported (Larstone et al., 2002). The beta factor links to extroversion and openness, and Eysenck’s extroversion. Three, four and five factor models introduce increasing levels of complexity although any increase in empirical accuracy (which is uncertain) comes at the expense of clinical utility. The clinical utility of personality nosology is essential and to this end the proposed model for ICD-11 personality disorder uses a single factor as its basis (Tyrer et al., 2011a, 2011b) .
Psychopathology has also been subjected to investigation of its overarching structure. This approach has been driven largely by the problem of comorbidity in mental disorder nosology when a polythetic categorical approach (such as is present in the DSM and ICD systems) to diagnosis it taken. This comorbidity is a problem of most mental state disorders (Kessler et al., 1994) as well as between mental state disorder and personality disorder. A wide variety of models have been proposed as alternatives to this categorical structure, from a single overarching psychopathology factor (named ‘p’) (Caspi et al., 2013) to a rejection of the statistical modeling approach but favoring one that is developmental in orientation (Durbin and Hicks, 2014). This variety of models relates to both the theoretical approach taken and the statistical model used to derive it (Krueger and Markon, 2006).
Embedded within this research field are the links between personality structure and psychopathology structure. These two domains overlap and personality traits predict common mental disorder accurately (Kotov et al., 2010). Longitudinally early personality disorder is related to both later personality disorder (Johnson et al., 2000) and common mental state disorder in epidemiological samples (Cohen et al., 2005). Common mental state disorders have also been reported to fit a two factor model of psychopathology in a longitudinal sample (Krueger et al., 1998), reflecting an internalizing and externalizing factor. Both these factors have shown stability in late adolescence over a three year course. The internalizing factor has been shown to be stable in an older cohort over a ten year period (Eaton et al., 2011). Despite research being undertaking by different research groups in different domains (personality structure and psychopathology structure) similarities are clear. As Krueger and colleagues point out, “It is striking moreover, that measures of psychopathology, often developed independently of one another and with no intent to represent personality variables, manifest broad dimensions strongly resembling those observed in the personality literature.” (Krueger and Markon, 2014: 255). In psychopathology research a two factor model fits the data best, identifies these factors as internalizing and externalizing (Krueger and Markon, 2006). This is similar to the two factor structure of personality disorder. In summary, both personality and psychopathology models report two factors, one inward looking and the other outward looking.
Cross sectional research suggests personality structure is important in understanding the impact of environmental factors in childhood and the later development of adult mental state disorder (Keyes et al., 2012). Similarly childhood personality and environment predict later adult personality status (Bernstein et al., 1996). What has not been examined is the impact of adolescent personality traits on social and diagnostic outcomes in early adulthood adjusting for the common confounders using a large longitudinal sample.
It is well established that effects in childhood, when taken in isolation, tend to have only a modest effect (Fergusson et al., 1994) on adult outcomes. More detailed analysis identifies some individual factors can have proportionately greater effects than others (Fergusson et al., 2013), and that small effect sizes in individual childhood characteristics may reflect much greater effects in adulthood. Understanding individual characteristics and environmental influences that impact on life trajectory potentially provides the opportunity to improve these trajectories if the influencing factor, such as childhood personality is potentially modifiable. Further examination of the relationship between mental disorders has been identified as important (Kessler et al., 2011).
There is some evidence that personality traits, expressed as behaviors in the very young, relate to personality styles (Caspi and Silva, 1995) in adolescents but it is uncertain whether these traits lead to problems (or resilience) in adults. Studies rarely examine the superordinate personality traits of extroversion and neuroticism correlating childhood personality with later psychopathology and social outcomes. Understanding the continuity/discontinuity of personality factors that progress from childhood to adulthood allows for appropriate consideration of their impact on health and social functioning. This potentially adds to the predictive power of trait domains and the understanding of change and stability over time (Caspi and Roberts, 2001).
This study aims to examine the linkages between neuroticism and extroversion, two personality facets, in childhood and the development of a range of mental disorders and social outcomes in adulthood. By examining a longitudinal cohort the temporal connections between personality variables, mental state disorder and social wellbeing can be examined, accounting for potential psychosocial confounders.
Methods
Sample
The participants were members of the Christchurch Health and Development Study (CHDS). This is a longitudinal study of 1265 children born in a four month period in Christchurch, New Zealand, in 1977. Participants have been assessed at birth, four months, annually from 1-16 years, at 18, 21, 25 and 30 years (Fergusson and Horwood, 2013). Of the original sample 987 were interviewed at age 30 (80% of the surviving cohort). Data were collected from participant interviews, parental reports, teacher questionnaires, standardised tests and official records. Ethical approval for all phases of the study was granted by the Canterbury Regional Health and Disability Ethics Committee. After complete description of the study to the subjects, written informed consent was obtained.
Measures
Personality (age 14)
Child personality was assessed at age 14 years using the short form of the Eysenck Personality Inventory (EPI) (Eysenck, 1964). This measure comprises two subscales of neuroticism (10 items) and extroversion (10 items). Items were scored on a 3-point scale (not like me/ a bit like me/ a lot like me). Total scale scores for neuroticism and extroversion were constructed based on a sum of the items in each subscale, scored such that higher scores implied higher neuroticism or extroversion. The two scales were of moderate internal consistency (α=0.80, 0.83 respectively).
Mental health outcomes (age 18–30 years)
At ages 21, 25 and 30 years, cohort members were interviewed by trained lay interviewers on a structured mental health interview designed to assess aspects of mental health and psychosocial adjustment over the period since the previous assessment. This interview utilized selected components of the Composite International Diagnostic Interview (CIDI) (Smeets and Dingemans, 1993) to assess participants on DSM-IV symptom criteria for the following mental disorders: major depression, anxiety disorders (including generalized anxiety disorder, panic disorder, agoraphobia, social phobia, specific phobia), alcohol dependence and illicit drug dependence. Additional custom-written items were used to assess suicidal behaviors including suicidal ideation and suicide attempt (Fergusson et al., 1996). Participant responses were combined over the three interview periods to classify participants for the presence or absence of each of the above mental health problems over the period from age 18 to 30 years. In addition, to provide an overall index of the severity of mental health problems, the six dichotomous outcomes were summed to create a count measure of the total number of mental disorders (including suicidal behaviours) reported from age 18-30.
Subjective wellbeing outcomes (age 30)
In addition to measures of mental health, at age 30 participants were assessed on three measures of psychological wellbeing. (a) Adult self-esteem was assessed using the 10-item Rosenberg Self-Esteem Scale (Rosenberg, 1965). Items were scored on a 4-point scale (1= strongly agree to 4= strongly disagree). A total scale score was constructed from a sum of the items, such that higher scores indicated higher self-esteem. This scale had excellent internal consistency (α= 0.91). (b) Current life satisfaction was assessed using a custom-written questionnaire which required respondents to rate their satisfaction with each of 12 areas of their life: work, leisure time, partner relationships, relationships with people of the same sex, relationships with people of the opposite sex, social life, money, independence, daily interactions with others, family life, the future and life as a whole. Ratings were made on a 4-point scale (1= very unhappy to 4= very happy) whereby higher scores indicated greater life satisfaction. Confirmatory factor analysis of the item responses showed that these items could be scaled unidimensionally, reflecting the extent of current life satisfaction at age 30 (Swain et al., 2012). For the purposes of the present analysis, scale scores were created by summing the responses to the 12 items to create a general life satisfaction measure. This scale had high internal consistency (α= 0.89). (c) Partner relationship quality was assessed using the 25-item Scale of Intimate Relationships by Braiker and Kelley (1979). This measure comprises subscales reflecting both positive (15 items) and negative (10 items) aspects of partner relations. Both scales had good internal consistency (α=0.89, 0.84 respectively). For the purposes of the present analysis a total scale score was calculated by subtracting the negative partner relations subscale from the positive subscale. The partnership quality score was calculated only for those cohort members who were in a current partnership or who had been in a romantic partnership at some time in the past 12 months.
Covariates
A wide range of covariate factors were selected from the database of the study to control the associations between childhood personality and later mental health and wellbeing outcomes for the correlated effects of other childhood factors. These covariates were selected on the basis that they were potentially associated with either child neuroticism or extroversion, and correlated with later mental health, and wellbeing outcomes. The selected covariates broadly fell into four groups: (a) Measures of childhood family socio-demographic background including: maternal age, maternal education and family socio-economic status at the time of the cohort member’s birth, and a measure of family living standards assessed over the first 10 years of the cohort member’s life. (b) Measures of childhood family functioning including: family instability (changes of parents 0-15 years), parental history of alcohol problems, parental history of mental health problems, exposure to child abuse and inter-parental violence (0-16years). (c) Measures of the quality of parenting and parent-child relationships including: the parental care and overprotection scales of the Parental Bonding Instrument (Parker et al., 1979) and the Armsden and Greenberg parental attachment scale (Armsden and Greenberg, 1987) assessed in adolescence (age 15). These instruments provide an assessment of the attachment between child and parent examining the capacity for the child to attach and parent to allow the child to develop. (d) Measures of individual characteristics and behavior including: gender, child IQ assessed using the revised Wechsler Intelligence Scale for Children (Wechsler, 1974) at age 8-9, measures of the child’s propensity to behavioral difficulties (conduct problems, attentional problems, anxiety/withdrawal) at age 7-9 derived from parent and teacher reports obtained using the Rutter and Conners behaviour rating scales (Conners, 1969, 1970; Rutter et al., 1970), and measures of adolescent mental health problems around age 14-15 years. In total 19 covariates were considered for inclusion in the analysis. (See online Supplement for a more comprehensive description of these factors)
Statistical analysis
The association between personality at 14 years and a range of mental health and social outcomes was assessed in the following ways. To illustrate the bivariate associations between childhood personality and adult outcomes, the scales of neuroticism and extroversion were first classified into five levels reflecting approximate quintiles on the distribution of each measure. The associations between the mental health/wellbeing outcomes and the five level classification of neuroticism (Table 1) or extroversion (Table 2) were then tested for linearity using the Mantel-Haenszel chi square test of linear trend for the dichotomous mental health outcomes, Poisson regression for number of mental health problems, or one way analysis of variance with test for linear trend for the wellbeing measures.
Associations between level of neuroticism (age 14) and measures of mental health problems (age 18-30) and adult wellbeing (age 30).
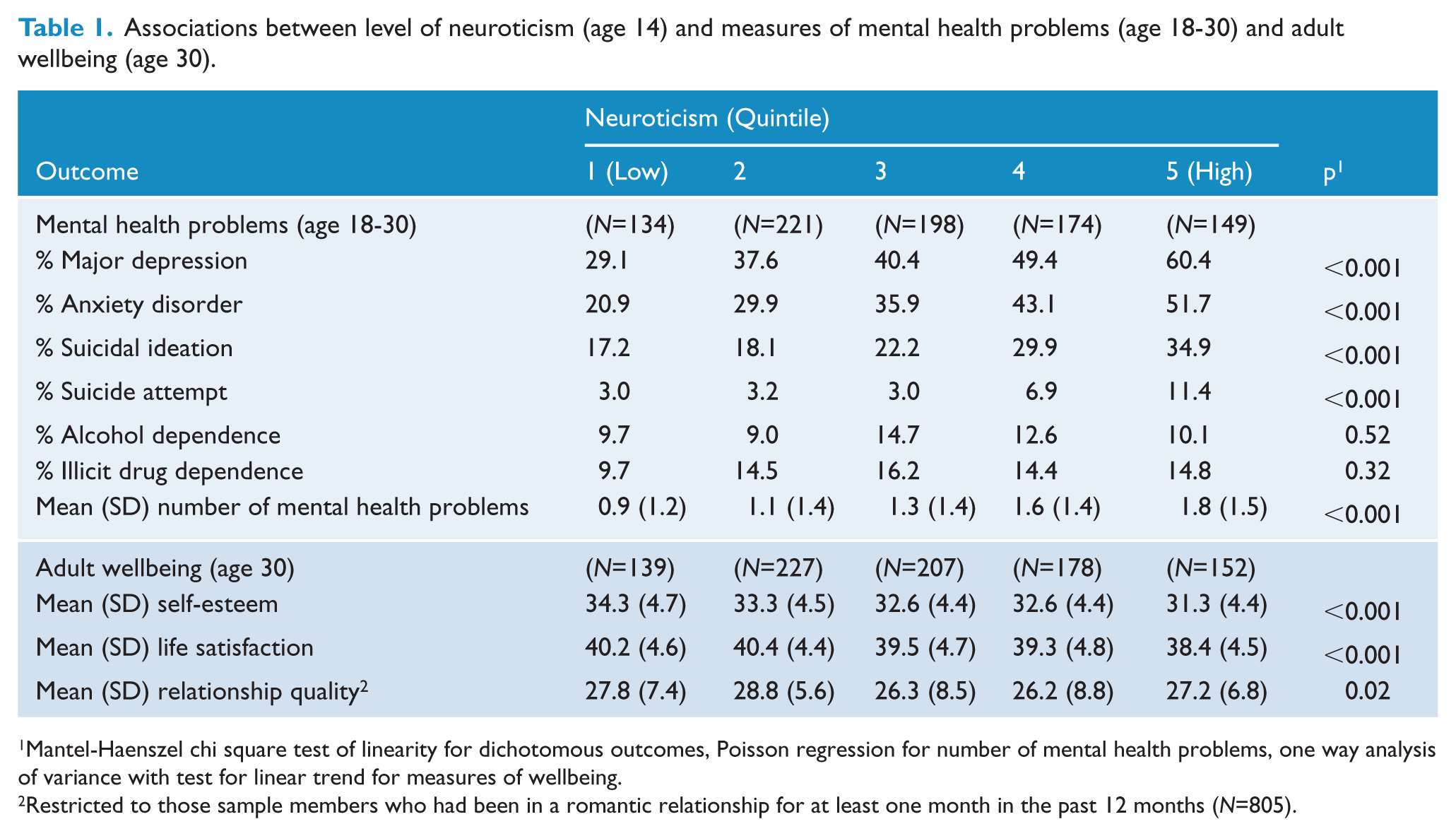
Mantel-Haenszel chi square test of linearity for dichotomous outcomes, Poisson regression for number of mental health problems, one way analysis of variance with test for linear trend for measures of wellbeing.
Restricted to those sample members who had been in a romantic relationship for at least one month in the past 12 months (N=805).
Associations between level of extroversion (age 14) and measures of mental health problems (age 18-30) and adult wellbeing (age 30).
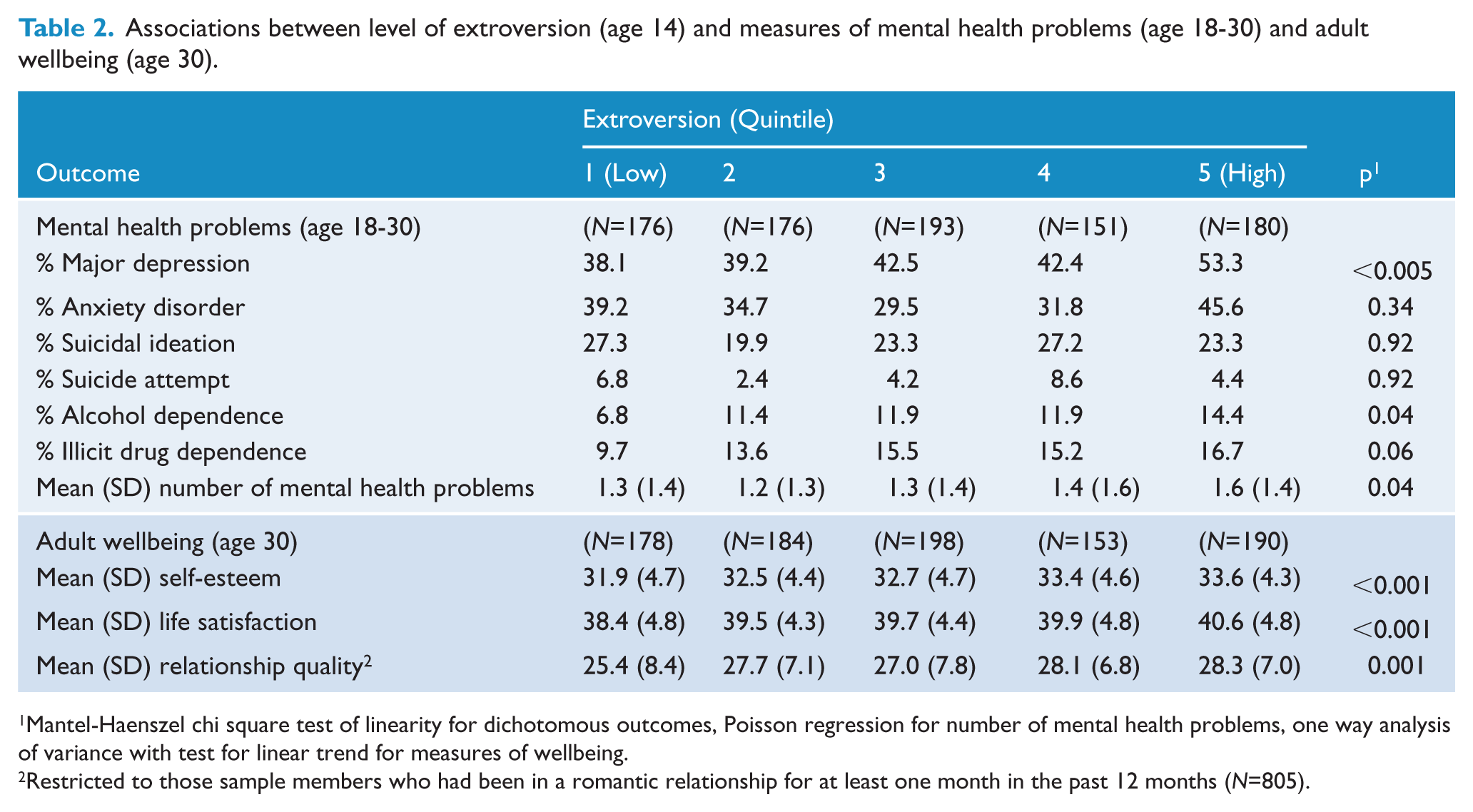
Mantel-Haenszel chi square test of linearity for dichotomous outcomes, Poisson regression for number of mental health problems, one way analysis of variance with test for linear trend for measures of wellbeing.
Restricted to those sample members who had been in a romantic relationship for at least one month in the past 12 months (N=805).
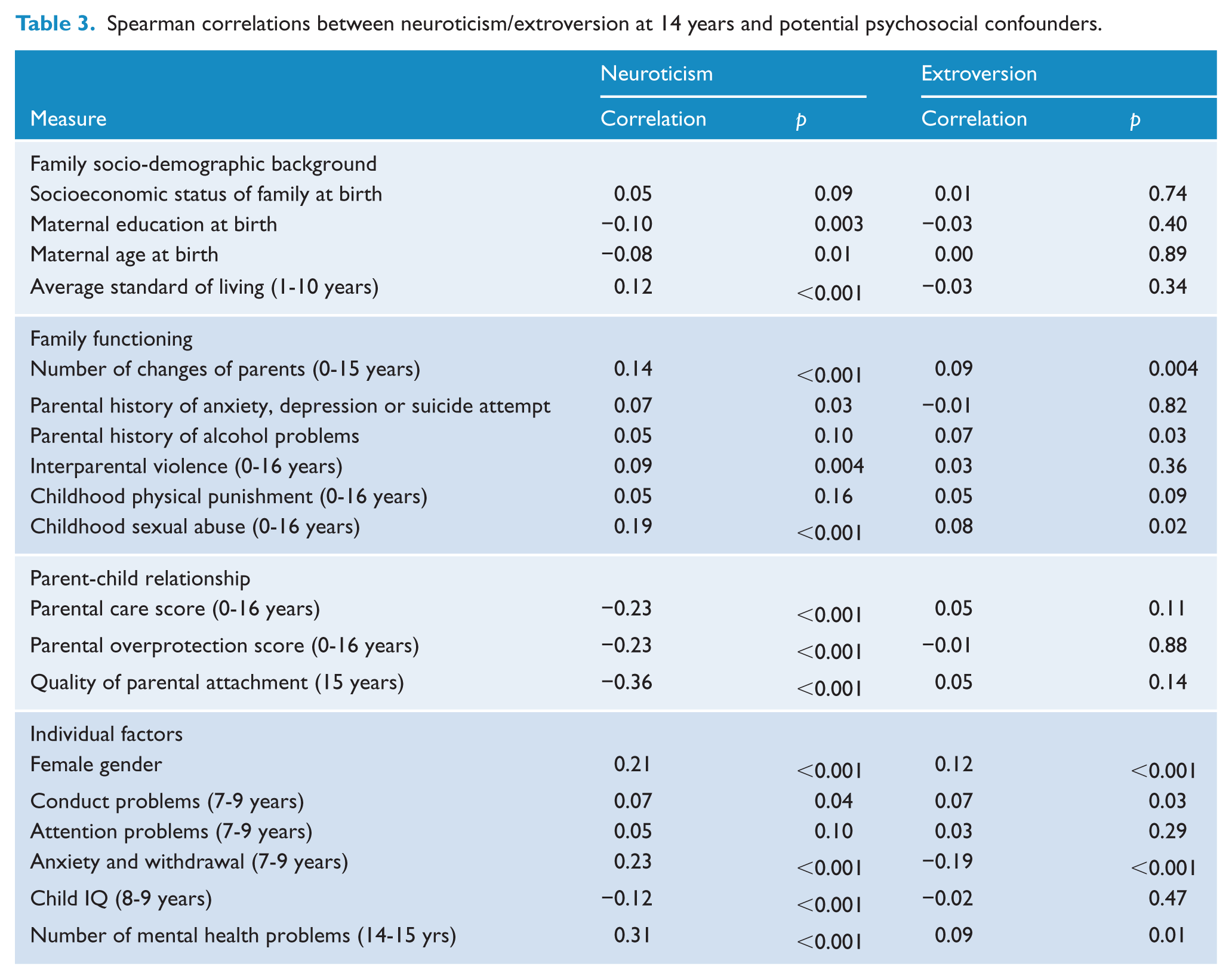
The associations between the personality measures and covariate factors were summarized using Spearman correlations and associated tests of significance (Table 3). All covariates having a significant (P<.05) or marginally significant (P<.10) correlation with either neuroticism or extroversion were considered for subsequent inclusion in regression models to control for the potential confounding effects of covariates.
Spearman correlations between neuroticism/extroversion at 14 years and potential psychosocial confounders.
A series of regression models was fitted to control the associations between neuroticism, extroversion and mental health, wellbeing outcomes for covariate factors. Logistic regression models were fitted for dichotomous mental health outcomes, Poisson regression was used for the count measure of number of mental health problems, and ordinary least squares regression for the three measures of adult wellbeing. In each case the outcome was modelled as a function of the two personality factors together with the selected covariates. In fitting these models the measures of neuroticism and extroversion were scaled in their continuous metrics rather than using the five level ordinal classifications used for displaying the bivariate associations. For each outcome, an initial model was fitted including all covariate factors. To avoid the possibility of over control and/or imprecision in the estimated effects of personality on outcomes due to the inclusion of too many covariates in the fitted models, the results for the models including all covariates were compared with the results for a similar set of models in which the covariate set had been refined down to a core set of significant or marginally significant covariates for each outcome. The estimated effects for neuroticism and extroversion on adult outcomes were virtually identical across the two series of regression models. The results reported in the paper are based on the reduced form models.
Effect size estimates were calculated from the final fitted models to summarise the covariate adjusted associations of neuroticism, extroversion with the outcome measures. For the mental health outcomes (Table 4) effect sizes were summarized by the odds ratio (OR, for dichotomous mental health measures) or the incidence rate ratio (IRR, for number of mental health problems) and 95%CI for a one standard deviation increase in the scale of neuroticism or extroversion. For the adult wellbeing outcomes (Table 5) effect sizes were summarized by the standardised regression coefficient for the effect of neuroticism or extroversion.
Associations (OR/IRR, 95% CI) between neuroticism/extroversion (age 14) and mental health outcomes (age 18-30) before and after adjustment for covariates.
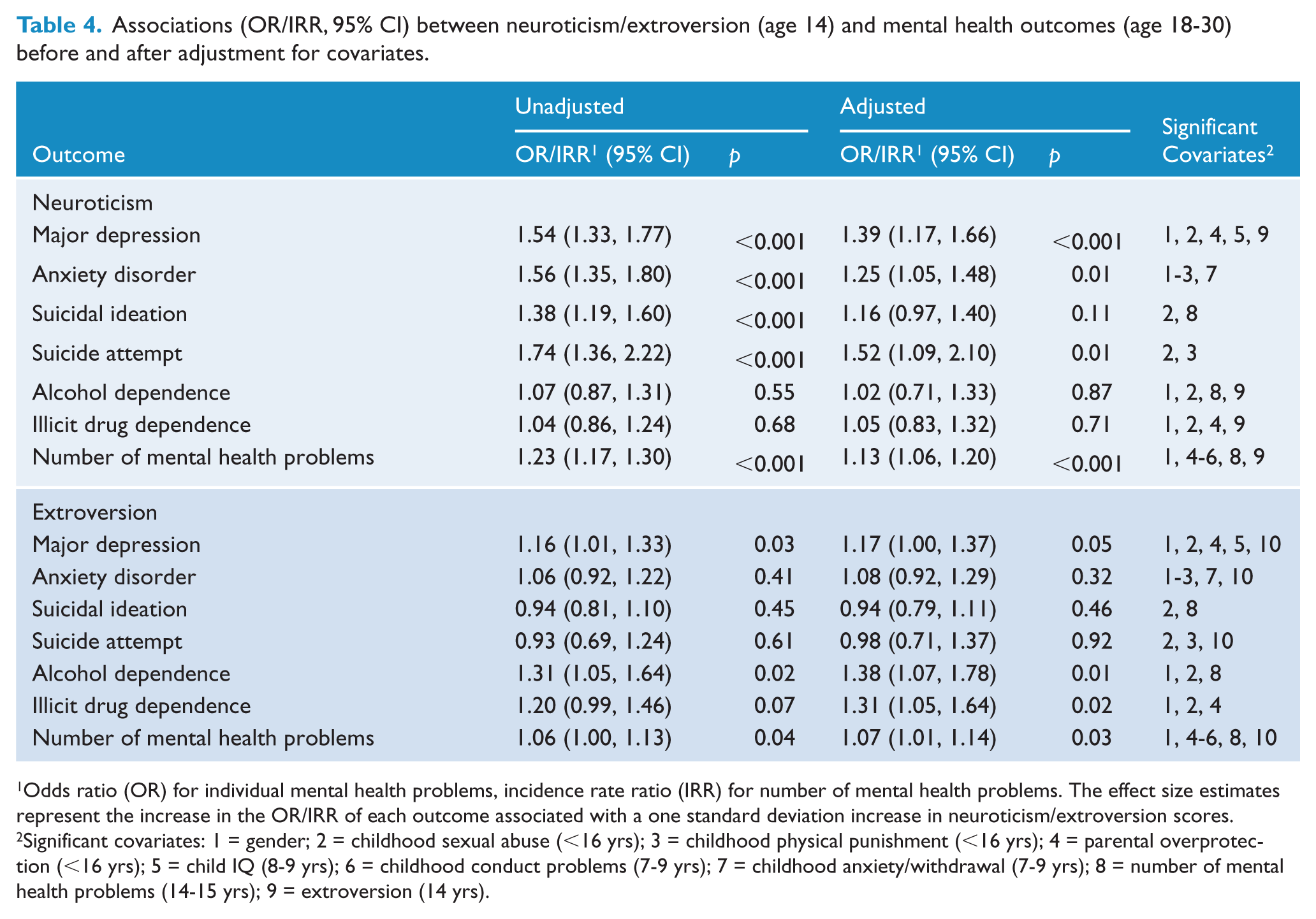
Odds ratio (OR) for individual mental health problems, incidence rate ratio (IRR) for number of mental health problems. The effect size estimates represent the increase in the OR/IRR of each outcome associated with a one standard deviation increase in neuroticism/extroversion scores.
Significant covariates: 1 = gender; 2 = childhood sexual abuse (<16 yrs); 3 = childhood physical punishment (<16 yrs); 4 = parental overprotection (<16 yrs); 5 = child IQ (8-9 yrs); 6 = childhood conduct problems (7-9 yrs); 7 = childhood anxiety/withdrawal (7-9 yrs); 8 = number of mental health problems (14-15 yrs); 9 = extroversion (14 yrs).
Associations between neuroticism/extroversion (age 14) and mental wellbeing outcomes (age 30) before and after adjustment for covariates.
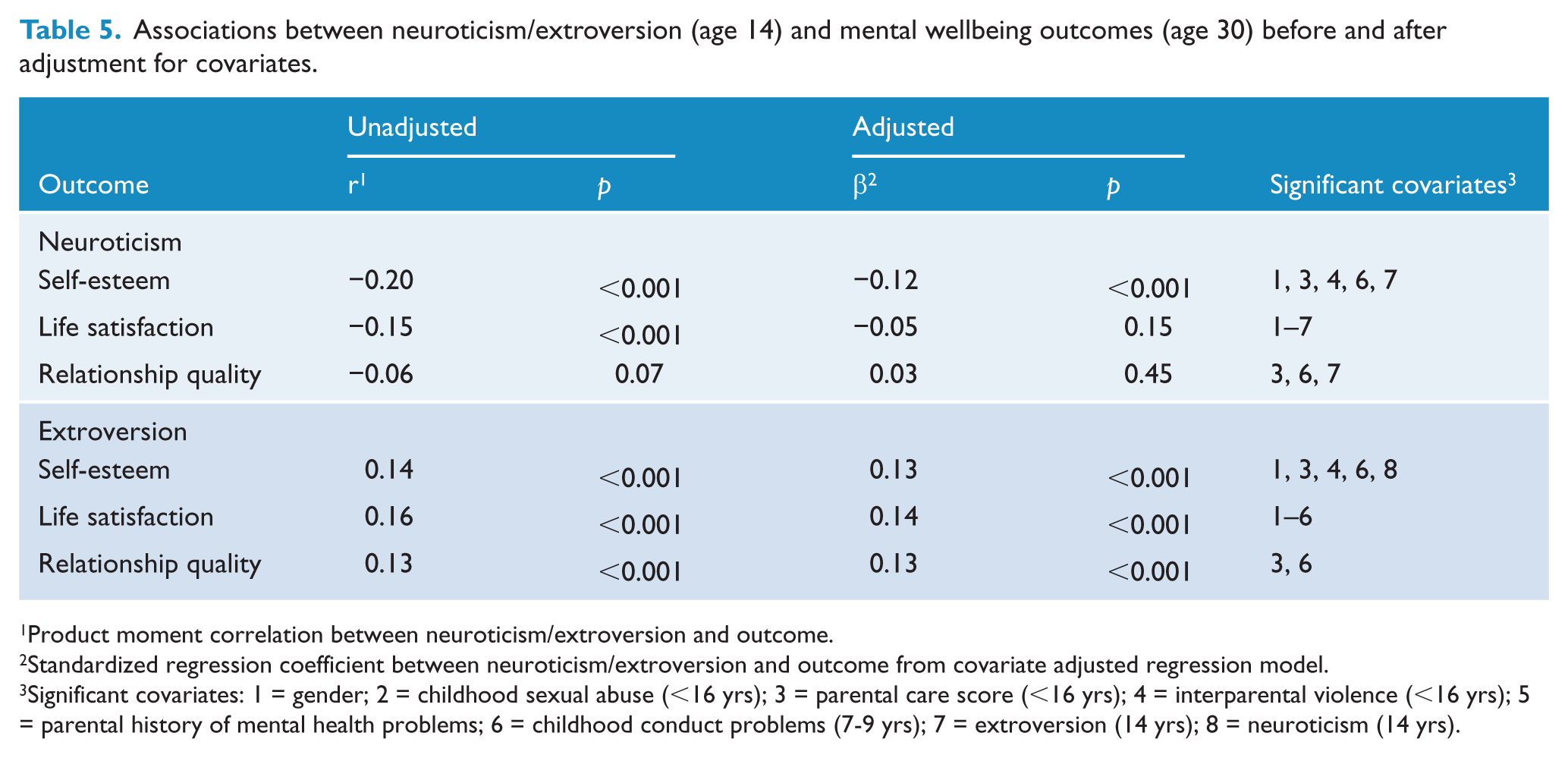
Product moment correlation between neuroticism/extroversion and outcome.
Standardized regression coefficient between neuroticism/extroversion and outcome from covariate adjusted regression model.
Significant covariates: 1 = gender; 2 = childhood sexual abuse (<16 yrs); 3 = parental care score (<16 yrs); 4 = interparental violence (<16 yrs); 5 = parental history of mental health problems; 6 = childhood conduct problems (7-9 yrs); 7 = extroversion (14 yrs); 8 = neuroticism (14 yrs).
Sample size and sample bias
The analyses are based on the samples of participants with complete data on the measures of childhood personality and outcome. Depending on the outcome these samples ranged from 876 to 903, and represented between 71% to 73% of the cohort surviving to age 30. This raises the issue of the extent to which the findings may have been influenced by selection bias attributable to processes of sample attrition and missing data. To address this issue the data were reanalyzed using both multiple imputation of missing data (Schafer, 1999) and data weighting methods (Carlin et al., 1999) to correct for potential biases. These analyses produced results that were virtually identical to those reported here, suggesting that the findings are unlikely to have been affected by sample attrition or missing data.
Results
Tables 1 and 2 show the associations between the level of neuroticism (Table 1) and extroversion (Table 2) at age 14 and a variety of mental state disorders and wellbeing measures assessed up to age 30. There were statistically significant linear associations between neuroticism and rates of depression (P<0.001), anxiety disorder (P<0.001), suicidality (P<0.001) and overall number of mental health problems (P<0.001), but no significant association with alcohol or illicit drug disorders. Increasing neuroticism associated with increasing mental health difficulties. Increasing neuroticism was also associated with lower reported self-esteem (P<0.001), life satisfaction (P<0.001) and partner relationship quality (P=0.02).
Higher rates of extroversion had significant or marginally significant associations with higher rates of depression (P<0.005), alcohol dependence (P=.04), illicit drug dependence (P=.06) and the overall rate of mental health problems (P=.04), but no association with anxiety disorder or suicidal behaviours. Increasing extroversion was positively associated with self- esteem (P<0.001), life satisfaction (P<0.001) and relationship quality (P<0.001).
Table 3 summarises the associations between the measures of neuroticism, extroversion and the covariate factors. Neuroticism was significantly associated with 15 of 19 potential psychosocial and childhood confounders. In contrast extroversion was statistically significantly associated with only seven of covariates to P=0.05.
The associations between childhood personality and mental health, wellbeing outcomes were adjusted for the potential confounding effects of covariate factors identified in Table 3 by fitting a series of regression models in which each outcome was regressed on the measures of neuroticism, extroversion and the covariates (see Statistical Methods). Table 4 summarises the covariate adjusted associations for mental health outcomes and Table 5 for the psychological wellbeing outcomes. For the mental health outcomes the effect size estimate reported is the change in odds ratio (OR) or incidence rate ratio (IRR) of disorder corresponding to a one standard deviation increase in neuroticism or extroversion after adjustment for confounding. For wellbeing outcomes the adjusted effect size estimate is based on the standardized regression coefficient (β) from the fitted regression model and thus reflects the estimated standard deviation change in outcome for a one standard deviation increase in personality score. For comparative purpose the unadjusted associations are also shown in the tables. The tables also list the significant covariate factors in the fitted regression model for each outcome.
For mental health outcomes, adjustment for confounding tended to reduce the estimated associations with neuroticism, but the associations with depression, anxiety disorder, suicide attempt and overall number of mental health problems all remained statistically significant. For extroversion, the associations with mental health outcomes were unaffected by covariate adjustment. The adjusted associations suggest that personality factors had only a modest impact on later mental health problems. The adjusted effect size estimates for total mental health problems show that a one standard deviation increase in neuroticism was associated with a 13% increase in the overall rate of disorder (IRR=1.13, 95%CI 1.06-1.20) and likewise a one standard deviation increase in extroversion with a 7% increase in the overall rate of disorder (IRR=1.07, 95%CI 1.01-1.14).
For adult wellbeing outcomes adjustment for confounding reduced the associations with neuroticism and only self-esteem was significantly associated with neuroticism after adjustment. Again the associations with extroversion were virtually unaffected by covariate adjustment. The adjusted associations for both measures were comparatively modest (β=-.12 to .03 for neuroticism, .13 to .14 for extroversion) and suggested that personality had only a small direct effect on later wellbeing outcomes when other factors were taken into account.
Discussion
This study builds on prior knowledge and confirms childhood personality factors are associated with a range of psychiatric disorders and factors indicating wellbeing in adulthood. Significant associations exist between neuroticism in early adolescence and the later development of depressive and anxiety disorders in adulthood, independent of psychosocial or environmental factors. Approximately 40% of the sample studied developed a depressive disorder by age 30 with this figure rising to almost 60% in the most neurotic quintile. These figures are higher than in other lifetime prevalence studies (Oakley Browne et al., 2006; Stein et al., 2008; Kessler et al., 2005), however the longitudinal nature of the data collection in this study may reflect actual lifetime prevalence rates more closely. Similarly increased risks for anxiety disorder, suicidal ideation and suicidal acts in early adulthood are associated with increasing neuroticism in early adolescence. The link between suicide and depression (Rihmer, 2001; Hawton et al., 2013) may be related to underlying neuroticism suggesting that screening of teenagers who are highly neurotic may help to identify those at greater risk of suicidality. The association between neuroticism, negative life events and poorer diagnostic and social outcomes is in line with a diagnostic approach that considers trait neuroticism and neurotic disorders as closely aligned. This transdiagnostic approach may more accurately underlie the empirical structure of psychopathology and is clinically relevant in considering management (McEvoy et al., 2009). Extroversion has less association with mental disorders. The strong association between extroversion and positive adult wellbeing may reflect protective qualities endowed by extroverted personality characteristics as expressed in improved self-esteem and relationship characteristics. It is notable that childhood extroversion correlates positively with later depressive disorder and this is an unexpected finding. The well-established link between neuroticism and later depressive disorder is usually independent of extroversion (Jorm et al., 2000). Similarly depression and anxiety have been associated with internalizing psychopathology, closely linked to neuroticism/negative emotionality (Krueger et al., 2001). Although these effects are modest in terms of effect size they are pervasive and extend across a 16 year time frame.
This study highlights the multiple associations between neuroticism and a variety of environmental factors. In contrast extroversion has relatively few such associations. Similar findings from other cohorts and methodologies have been reported (Farmer et al., 2002). This finding suggests that the development of neuroticism at age 14 is closely related to environmental exposure to stressful life events. Extroversion is not associated with similar environmental exposure and it may be this personality trait is more influence by heritable characteristics.
This possibility would be supported by the relative sensitivity of neuroticism to covariates in the adjusted analysis and the relative insensitivity of extroversion. Previous research support this perspective using differing methodological perspectives. Genetic studies have found links between extroversion to both COMT and DRD4 and a variety of genetic variants (Golimbet et al., 2007; Bookman et al., 2002) although this relationship is challenged (Munafò et al., 2008). Similar genetic linkages have been explored for neuroticism with less success (van den Oord et al., 2008; Willis-Owen et al., 2005), suggesting at best small effects on trait anxiety (Schinka et al., 2004). Behavioral research also supports the association between extroversion and improved wellbeing in adulthood (Eid et al., 2003; Myers and Diener, 1995) while clinical research identifies the role of environmental trauma in both psychiatric disorder and suicidality (Roy, 2002). This study links the behavioral cross sectional approach and the genetic approach, identifying both the longitudinal link between extroversion and improved wellbeing and the longitudinal link between adverse environmental conditions at 14 years, neuroticism and subsequent psychiatric disorder.
After taking account of multiple potential confounders the association between childhood personality traits and adult mental state disorder and psychological wellbeing in early adulthood remains significant. These findings support the need to pay close attention to personality factors in early life, and emphasizes the need to identify and support highly neurotic children to ameliorate the future risks of psychiatric disorder and suicidality.
Limits
These findings are limited by the study parameters of the CHDS. Personality was assessed at 14 years but has not been assessed subsequently so no comment can be made as to the stability of personality over time. The short form of the Eysenck Personality Inventory was used and so we cannot study the impact of trait psychoticism (EPI-P). The methods of obtaining diagnoses have been criticized in other settings, and although the CIDI is reliable (Andrews and Peters, 1998) its validity has been questioned. These problems with diagnosis are similar to most psychiatric research. Many of the psychosocial variables assessed as potential confounders were measured at the same time point and this raises the possibility these act as comorbid variables rather than confounders. This does not change the associations reported, but it leaves the question of interaction unanswered. The self-esteem measure may reflect ‘inverse’ neuroticism, although the repeated measures suggest at least stability over time. The analysis adjusting for comorbidity (Table 4) reports that personality traits remain associated with mental health outcomes even after adjusting for these variables. It is also of note that childhood sexual abuse (covariate 2 in Table 4) is repeatedly found to be statistically associated with poorer adult outcomes (Fergusson et al., 2013) and, although these factors are independently related to poorer adult outcomes, their interaction remains unclear.
Empirical evidence now supports the association between adolescent personality and a range of outcomes in adulthood. Neuroticism tends to lead to poorer outcomes whereas extroversion may be protective. These findings are in line with the literature to date and add to it, providing links between cross sectional analysis and retrospective data. Furthermore it links findings from childhood and adolescence into adulthood.
Footnotes
Acknowledgements
Elements of this work were presented at the BIGSPD meeting, 19th-21st February 2014 at Lincoln (England), UK.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This research was funded by grants from the Health Research Council of New Zealand, the National Child Health Research Foundation (Cure Kids), the Canterbury Medical Research Foundation and the New Zealand Lottery Grants Board.