
Abstract
Objective:
To assess, from a health sector perspective, the incremental cost-effectiveness of three treatment recommendations in the most recent Australian Clinical Practice Guidelines for posttraumatic stress disorder (PTSD). The interventions assessed are trauma-focused cognitive behavioural therapy (TF-CBT) and selective serotonin reuptake inhibitors (SSRIs) for the treatment of PTSD in adults and TF-CBT in children, compared to current practice in Australia.
Method:
Economic modelling, using existing databases and published information, was used to assess cost-effectiveness. A cost-utility framework using both quality-adjusted life-years (QALYs) gained and disability-adjusted life-years (DALYs) averted was used. Costs were tracked for the duration of the respective interventions and applied to the estimated 12 months prevalent cases of PTSD in the Australian population of 2012. Simulation modelling was used to provide 95% uncertainty around the incremental cost-effectiveness ratios. Consideration was also given to factors not considered in the quantitative analysis but could determine the likely uptake of the proposed intervention guidelines.
Results:
TF-CBT is highly cost-effective compared to current practice at $19,000/QALY, $16,000/DALY in adults and $8900/QALY, $8000/DALY in children. In adults, 100% of uncertainty iterations fell beneath the $50,000/QALY or DALY value-for-money threshold. Using SSRIs in people already on medications is cost-effective at $200/QALY, but has considerable uncertainty around the costs and benefits. While there is a 13% chance of health loss there is a 27% chance of the intervention dominating current practice by both saving dollars and improving health in adults.
Conclusion:
The three Guideline recommended interventions evaluated in this study are likely to have a positive impact on the economic efficiency of the treatment of PTSD if adopted in full. While there are gaps in the evidence base, policy-makers can have considerable confidence that the recommendations assessed in the current study are likely to improve the efficiency of the mental health care sector.
Introduction
In August 2013, the new Australian Guidelines for the Treatment of Acute Stress Disorder & Posttraumatic Stress Disorder were released (Australian Centre for Posttraumatic Mental Health (ACPMH), 2013). Posttraumatic stress disorder (PTSD) is a common psychiatric disorder, with a 12-month prevalence rate in Australia of 4.4% (McEvoy et al., 2011). PTSD is characterised by four types of symptoms: re-experiencing symptoms such as intrusive memories or dreams; avoidance symptoms such as avoiding thoughts, feelings, and places associated with the traumatic event; numbing symptoms such as feeling detached from others; and increased arousal symptoms such as poor sleep, irritability and hypervigilance. Left untreated, PTSD tends to have a chronic course and high comorbidity with other mental health disorders (ACPMH, 2013). The Guidelines were developed in accord with the National Health and Medical Research Council guideline development requirements. The Guidelines were informed by a working party comprising key national experts and a broad range of relevant stakeholders (including service users) and were underpinned by a systematic review of the literature along with consensus expert opinion where there was an insufficient evidence base. The Guidelines provide recommendations for practice spanning the entire treatment pathway, including the broad categories of screening, assessment and treatment planning.
The Guidelines are mainly based on evidence of effectiveness rather than cost-effectiveness as very few economic evaluations of interventions for PTSD have been published. In 2004, Issakidis et al. (2004) evaluated the cost-effectiveness of moving from current practice to evidence-based practice (defined as cognitive behavioural therapy (CBT) and pharmacotherapy) for anxiety disorders (including PTSD) within the Australian context. Another Australian economic evaluation recently evaluated the impacts of treatments (CBT and pharmacotherapy) for PTSD in children who were sexually abused (Gospodarevskaya and Segal, 2012). Both these studies have concluded that evidence-based treatments for PTSD are likely to be very cost-effective. However, the results of these studies are not comparable owing to important methodological differences, including the methods by which outcomes are defined and the breadth of costs included.
An important question for any change in clinical practice is whether changes to the interventions advocated within new treatment guidelines are cost-effective. This is a significant policy question since it is widely recognized that clinical adherence to treatment guideline publications is not necessarily a linear process and a multifactorial approach to guideline implementation is required (Grimshaw et al., 2004). The knowledge of whether effective interventions are also cost-effective is an important part of the decision-making, dissemination and implementation process. Ideally, the cost-effectiveness of interventions should be evaluated alongside well-conducted clinical trials, set within the context in which they will be routinely delivered (defined as translational effectiveness trials). Such information is not always readily available to guide decision-making. Even when such information exists, the cost-effectiveness of interventions is usually context specific and evidence from international contexts may not have local applicability since health care systems vary in design and cost.
Therefore, there are very few existing economic evaluations of treatments for PTSD in the literature and the few existing studies do not answer the question of whether a practice shift to the treatments advocated within the new Guidelines is cost-effective. The term ‘cost-effective’ in the current context is defined as providing good value for money compared to commonly used Australian value-for-money thresholds (such as $50,000 per quality-adjusted life year) (Carter et al., 2008). The current study aims to answer the question of whether a practice switch to the following three Guideline treatment recommendations for people seeking care for PTSD provides value for money compared to current practice in Australia from a health sector perspective. The three interventions evaluated by the current study, include:
Trauma-focused cognitive behavioural therapy (TF-CBT) as the first-line treatment for PTSD in adults.
TF-CBT as the first-line treatment of PTSD in children and adolescents.
Selective serotonin reuptake inhibitors (SSRIs) as the pharmacological intervention of choice in adults with PTSD who are currently prescribed medication.
Notably, these three Guideline recommendations are underpinned by the strongest levels of evidence of effect. Establishing their cost-effectiveness is another important perspective to support their implementation.
Methods
The economic evaluation methods used in the current study are grounded in an economics-based priority-setting methodology developed in Australia since 2001 called the Assessing Cost-Effectiveness (ACE) approach (Carter et al., 2008). This approach has been used extensively in the Australian context, including the mental health context (Mihalopoulos et al., 2011a, 2011b; Vos et al., 2005b) and has been found to be acceptable to Australian decision-makers. The perspective of the economic evaluation is the health sector, which incorporates government (Commonwealth and State) and patients’ (out-of-pocket) costs. This perspective was chosen for consistency with the other ACE studies, plus evidence of intervention impacts in other economic sectors (such as productivity) is not available for the interventions under consideration. All costs are reported in 2012 Australian dollars. Economic modelling, using existing databases and published information, was used to determine the population cost-effectiveness of the interventions (described further below).
Consideration was also given to factors not considered in the quantitative analysis but which are likely to determine the uptake of the proposed intervention guidelines, including: an evaluation of the strength of the evidence (which impacts on the confidence in the reported incremental cost-effectiveness ratios (ICERs)); potential impacts on equity; acceptability to stakeholders; and sustainability and/or implementation issues. Such considerations are termed ‘second stage filter considerations’ in the ACE methodology (Carter et al., 2008).
The interventions
Trauma-focused CBT
As the interventions were based on the Guideline recommendation, the literature which informed each of the three Guideline recommendations was used to characterise the evaluated interventions (Newton et al., 2012). As such, 8–12 individual weekly sessions of TF-CBT in adults and 8–10 sessions in children were modelled. The analysis assumed that all sessions were delivered by a psychologist funded through Australia’s public insurance scheme, Medicare. In addition to these sessions, an initial visit to a GP for a mental health plan and referral, and a follow-up GP visit at completion of the TF-CBT sessions were also included in the intervention pathway.
SSRIs
Pharmacotherapy using SSRIs (from the current mix of available SSRIs in 2011/2012) was modelled for 9 months of treatment, as per trial-based evidence included in the systematic review (Newton et al., 2012). The modelled intervention replaced other currently prescribed anti-depressants with an SSRI and added an SSRI to the current medication regime in eligible adults where anti-depressants were not a component of the regime. The number of medical visits and mix of providers from current practice were not altered in this analysis since eligible adults currently on medications were assumed to be appropriately medically managed. The dose/form of any particular SSRI prescribed was not specified but rather determined by the mix of SSRIs currently prescribed to Australian adults, as reported for the 2011/2012 financial year (Australian Government, 2012) (published online at www.medicareaustralia.gov.au/provider/pbs/stats.jsp).
Eligible population for the interventions
Prevalent cases (12-month prevalence) of PTSD estimated for the Australian population of 2012 (adults and children under 16 years) were deemed eligible for the interventions, if they were currently seeking care and had consulted any health professional for a mental health problem during the previous 12 months, but did not receive evidence-based medicine (EBM). The 2007 National Survey of Mental Health and Wellbeing (NSMHWB) (Australian Bureau of Statistics, 2009) was used to determine the 12-month prevalence of PTSD and treatment consulting patterns for adults diagnosed at interview with PTSD (DSM-IV criteria) in the last 12 months. Those adults seeking care in the past 12 months for a mental health problem from any health professional were defined as ‘consulting’ (51% of males; 41% of females).
For the TF-CBT intervention, EBM (or practice consistent with the Guidelines) was defined as including three components: care provider type; treatment type; and quantity of resource use. Consistent with previous health economic analyses (Sanderson et al., 2003; Vos et al., 2005a), it was assumed CBT EBM occurred if adults were consulting with a GP, psychologist or psychiatrist, were receiving counselling or CBT, and did so on more than nine occasions in the last 12 months. In the absence of more specific data reflecting the content of the counselling or CBT item, this categorisation is the closest approximation to EBM available. Adults were eligible for the TF-CBT intervention if they were consulting but did not receive CBT EBM, as defined here. It was found that 33% of adult 12-month prevalent PTSD cases met the criteria of receiving non-EBM care. This proportion was then modelled as shifted to TF-CBT in the current analysis.
For children, the methods of defining and estimating the eligible population differed since the Child Component of the NSMHWB conducted in 1998 (Australian Bureau of Statistics, 1999) did not include PTSD. Prevalent cases of PTSD in children were therefore necessarily estimated from the published international literature (Copeland et al., 2007). In order to identify current practice, the study by Haby et al. (2004), which evaluated CBT and SSRIs for depression in children and adolescents, was agreed by the project expert advisory panel to be used as a proxy for current practice of PTSD. Both the proportion of children seeking treatment and the proportion of those who sought treatment receiving CBT EBM were estimated at 35%.
EBM with respect to prescribed medications was defined at the level of drug class (i.e. taking anti-depressant SSRIs). Of consulting adults with PTSD during 12 months, 53% of males and 69% of females were prescribed medications (derived from the 2007 NSMHWB). Only 65% and 58%, respectively, of the males and females prescribed medications were taking anti-depressants. Of those males and females prescribed anti-depressants, only 65% and 70%, respectively, were taking SSRIs. Adults were eligible for the SSRI intervention if they were consulting, were prescribed medications but were prescribed either no anti-depressant (35% of males and 42% of females prescribed medications) or were prescribed a non-SSRI anti-depressant (35% and 30% of those males and females prescribed anti-depressants). The other medications (e.g. anti-psychotics, anxiolytics, sedatives) were not evaluated further as they were not expected to change with the intervention under consideration. The panel of PTSD experts and industry representatives who comprised the advisory panel for this project endorsed these assumptions.
New cases to treatment are not included in the current analysis as the recommended interventions examined here do not include a screening and case-finding component.
Assessment of health gain
A cost-utility design was used as the economic evaluation framework with the health benefits modelled as quality-adjusted life-years (QALYs) gained (using utility-weights from the Assessment of Quality of Life (AQoL-4D) instrument included in the 2007 NSMHWB) and disability-adjusted life-years (DALYs) averted (using disability-weights from the Australian Burden of Disease Study) (Mathers et al., 2000). We used QALYs as they are the most commonly used outcome metric in international economic evaluation studies. However, DALYs have been used extensively in Australian priority-setting studies; therefore, our current results are comparable to other Australian studies which have used DALYs (e.g. Mihalopoulos et al., 2011b; Vos et al., 2005b). The inclusion of both QALYs and DALYs also increased the robustness of the analyses as it could be determined whether choice of outcome metric alters the conclusions of the analyses.
We used the estimates of effectiveness from a meta-analysis of all TF-CBT interventions (Newton et al., 2012). This meta-analysis reported the relative risk (RR) of PTSD diagnosis in adults following TF-CBT intervention as 0.52 (95% CI 0.43 to 0.62) and as 0.14 in children (95% CI 0.02 to 0.99). The systematic review of trials comparing SSRIs to other anti-depressants reported equivocal evidence of benefit, using mostly symptomatic outcome measures such as self-reported severity of PTSD symptoms or improvements on clinician-rated scales.
The trials included in the TF-CBT meta-analyses taken together also enabled estimation of the proportions of adults and children eligible for CBT (i.e. able to participate), likely to agree to participate and likely to comply/adhere with CBT under trial conditions. These proportional values were used in the economic model to estimate the size of the Australian population likely to be eligible for the intervention, likely to agree to participate and rates of likely compliance. As we also included uncertainty in the economic model (refer to later section on uncertainty measurement), a lower limit of 50% was introduced to the eligibility, participation and compliance proportions to account for real-world routine health service conditions which may differ from those found in clinical trials. The relevant RR of PTSD diagnosis following treatment was applied only to the proportion of adults and children expected to comply fully with the TF-CBT intervention.
QALYs
QALYs are a generic health outcome measure developed to combine both mortality and morbidity components of health gain. They are simply the length of life lived in a particular health state multiplied by a ‘utility (or preference)-weight’ associated with that health state (Drummond et al., 2005). Utility-weights are normally scaled on a 0–1 scale, where 0 represents death and 1 represents perfect health. The NSMHWB included the AQoL-4D, which is a 12-item, health-related quality of life multi-attribute utility instrument allowing the calculation of QALYs (Hawthorne et al., 1999). In order to derive the utilities of NSMHWB participant responses to the AQoL-4D questionnaire, responses were scored with SPSS syntax downloaded from the AQoL website and a utility score was assigned to each survey respondent. This utility score was interpreted as baseline quality of life assessment incorporating all health-related factors that impact on the individual as assessed within the domains included in the questionnaire. We assumed that the negative impacts of comorbidities, in addition to PTSD, as well as any benefits from current treatments, were reflected in these baseline utilities. The survey allowed us to categorise people into those with or without a current diagnosis of PTSD and whether or not they had received EBM treatments in the last 12 months. The absolute differences in the utilities of these different groups were used to estimate the QALY gains due to the TF-CBT interventions.
Only the adults and children who no longer had a PTSD diagnosis following full compliance with the TF-CBT intervention were assigned the incremental utility gain that was derived from the 2007 NSMHWB as the differential utility between those adults who have 12 months’ PTSD and receive CBT EBM and do not have 30-day PTSD (utility = 0.63 males; 0.64 females) and those who have 12 months’ PTSD and do not receive CBT EBM (but do receive some care) (utility = 0.54 males; 0.57 females). We also applied a longer-lasting CBT benefit over the 4 years following treatment at an annual decay rate of 50%, meaning that no QALY benefit was included beyond 5 years (Vos et al., 2005a). In sensitivity analysis we reduced the utility gain from 0.08 to 0.04 and lower to assess its impact on the cost-effectiveness results, and determine the value of the QALY gain where the intervention would be no longer cost-effective. Parameter values contributing to this element of the analysis are provided in Table 1.
Critical parameter values, sources and uncertainty distributions current practice and the trauma-focused CBT intervention.
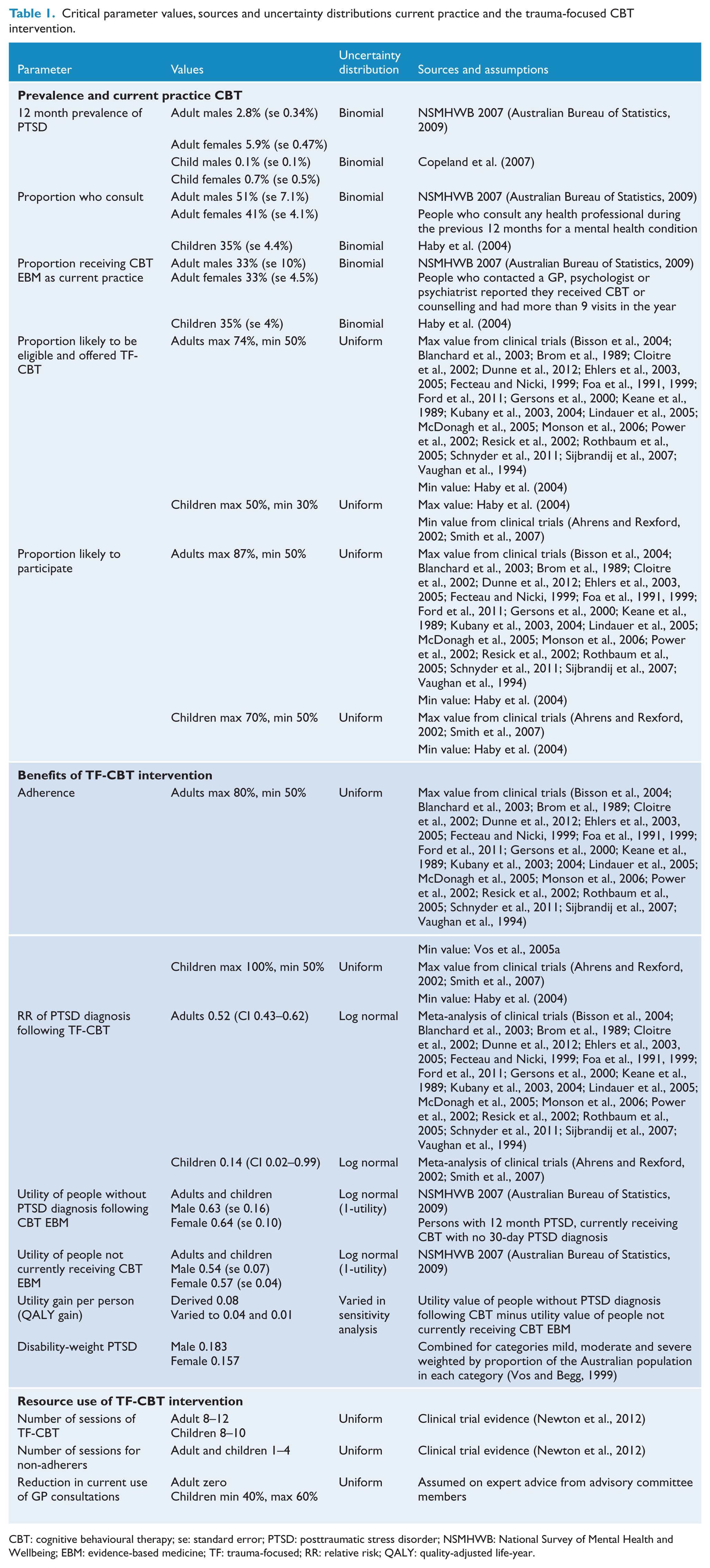
CBT: cognitive behavioural therapy; se: standard error; PTSD: posttraumatic stress disorder; NSMHWB: National Survey of Mental Health and Wellbeing; EBM: evidence-based medicine; TF: trauma-focused; RR: relative risk; QALY: quality-adjusted life-year.
The utility increment due to taking SSRIs was estimated as the difference between those persons taking SSRIs (0.51, n=40) and those persons taking non-SSRI anti-depressants (0.42, n=27). Therefore the incremental utility gain of switching to an SSRI was assumed to be 0.09.(0.51-0.42).
Parameter values contributing to this element of the analysis are provided in Table 2. The small numbers of raw survey observations from which these SSRI utilities were obtained, prevented gender-based analysis and the appropriate jackknife population weighting, which we approximated by adopting, for the two gender subgroups, the relationships between mean utility and confidence intervals available in the larger population group of persons taking anti-depressants (n=67).
Critical parameter values, sources and uncertainty distributions current practice and the SSRI intervention.
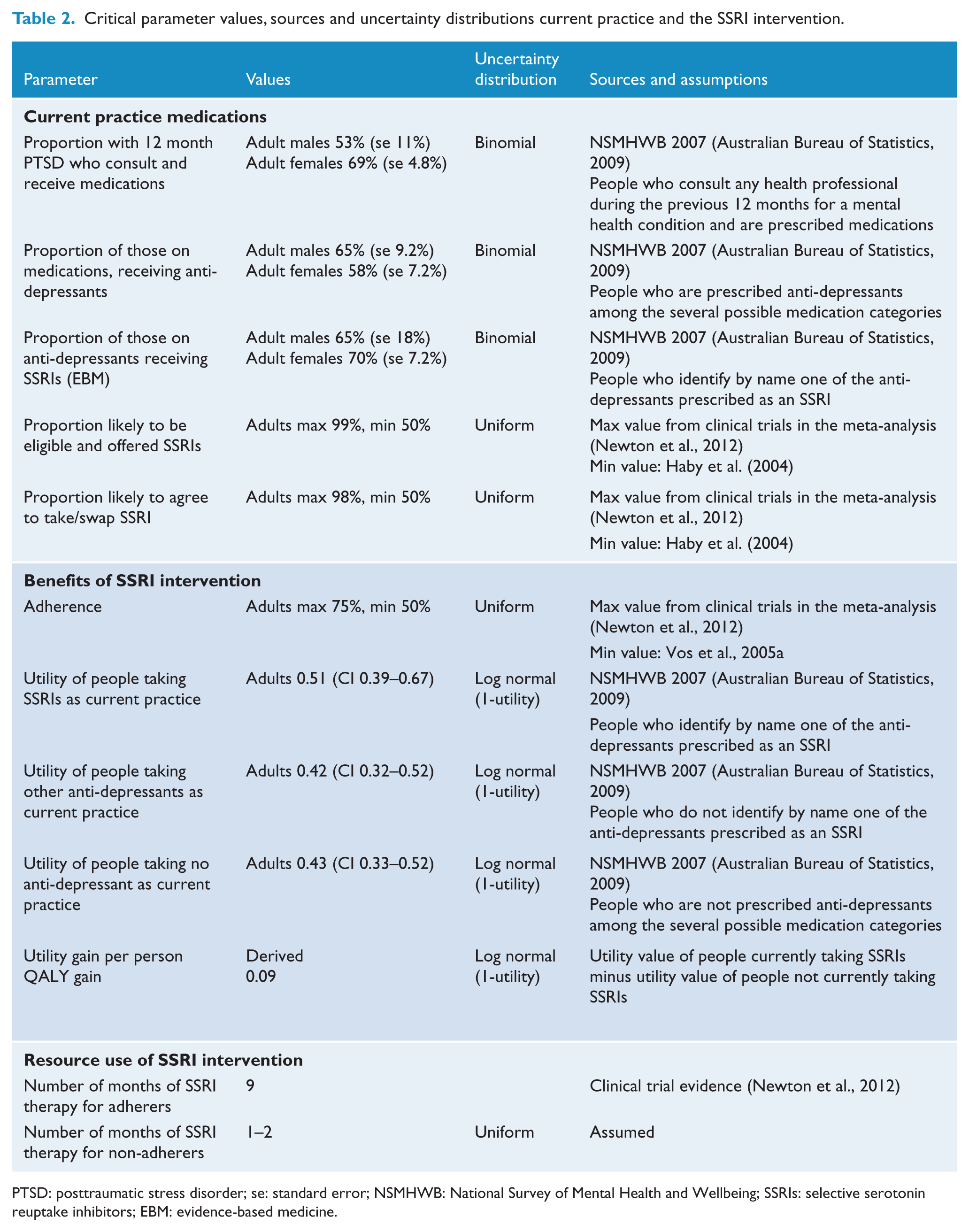
PTSD: posttraumatic stress disorder; se: standard error; NSMHWB: National Survey of Mental Health and Wellbeing; SSRIs: selective serotonin reuptake inhibitors; EBM: evidence-based medicine.
DALYs
DALYs are a summary measure of population health which captures the impact of premature deaths and years of healthy life lost to disability. Conceptually they are not dissimilar to QALYs. DALYs are derived by summing the years of life lived with a disability (YLDs) and years of life lost (YLLS) due to premature mortality, for each disease/injury category. The disability-weight (dw) assigned to PTSD in adults and children was first used in the 1999 Australian Burden of Disease study (Mathers et al., 1999) and was assumed to apply to the proportion of time a person was experiencing symptoms (51–56% of a year on average). The symptoms could be either mild, moderate (dw=0.13 for both) or severe (dw=0.51). A composite dw (0.183 in males and 0.157 in females) has been estimated using the proportions of the Australian population surveyed in the 1997 NSMHWB in each of the three PTSD health severity states (spreadsheets were formally available from Australian Institute of Health and Welfare (1999), but have now been withdrawn. Details are available from authors). DALYs averted by the TF-CBT intervention in adults and children is the product of the gender-based composite disability-weight, the percentage of time spent over a year symptomatic and the number of adults and children who are estimated to no longer have a PTSD diagnosis following full compliance with the TF-CBT intervention, identified as outlined above. We similarly quantified a longer-lasting CBT benefit over the 4 years following treatment at an annual decay rate of 50%, meaning that no DALY benefit was included beyond 5 years (Mihalopoulos et al., 2011b; Resick et al., 2012).
The DALY could not be used to model the health gain in the SSRI intervention since no change of PTSD diagnosis was available from the trial evidence, nor were there useful measures of PTSD severity in the 2007 NSMHWB to be altered in accordance with trial evidence.
The likely adherence rate was incorporated into the modelling for both QALYs and DALYs since persons not complying with more than four TF-CBT sessions were not expected to derive any health benefits, but they incurred treatment costs. No lag to treatment effect in the assessment of benefits was applied.
Assessment of costs
Costs were tracked for the duration of the respective interventions and applied to the estimated 12 months’ prevalent cases of PTSD in the Australian population of 2012.
TF-CBT intervention
There were two components of costs which were included in the current study. The first were the additional costs of the EBM interventions modelled. The second were the ‘cost-offsets’ associated with the replacement of costs of non-EBM treatments with the cost of EBM treatments. Therefore, in both adults and children we replaced the current mix of psychologist and psychiatrist consults with a specified number of sessions of TF-CBT offered by a psychologist which matched the benefit evidence in the trials, plus we incorporated the cost of a visit to a GP for development of a mental health plan and referral to the psychologist for TF-CBT and a follow-up GP visit to review plan progress. On expert advice, based on the experience of other Medicare initiatives, we did not reduce the number of other GP sessions attended by adults each year (i.e. 37% consulting a GP one to three times, 15% consulting a GP four to six times, 5% consulting a GP more than seven times), while the number of other GP sessions attended by children was reduced by 40–60%. The use of alternative medical therapies (e.g. myotherapist, acupuncture), other medical specialists, and current medication costs (if applicable) of the eligible population for the TF-CBT intervention was not varied (due to lack of evidence from the trials).
The current mix of services, which was replaced in the analysis because they did not meet our multidimensional definition of CBT EBM, included: 7% of people with PTSD who consulted a psychiatrist one to four times, 5% who consulted a psychiatrist five or more times; and 8% who consulted a psychologist one to two times, 15% who consulted a psychologist three to five times, 4% who consulted a psychologist six or more times. The cost applied to the TF-CBT sessions, lasting at least 50 minutes, was taken from the average cost in the 2011/2012 year of the two Medicare Benefits Schedule (MBS) item numbers (80010 and 80110), weighted by the proportions of services, provided by clinical and non-clinical psychologists at the applicable cost rates (these items were used to reflect the longer duration of consultations as consistent with the trials).
Since current practice for CBT in children was less well known, a separate intervention was modelled as a sensitivity analysis. This intervention comprised the addition of TF-CBT to whatever the current mix of care options/therapies may be for children in Australia, and compared the benefits to the costs without replacement of any other therapies and their associated costs. In the same sensitivity analysis, the adult TF-CBT intervention as a complete addition to current practice was also modelled in order to examine the impact on the cost-effectiveness conclusions.
Actual out-of-pocket costs by Medicare item for the 2011/2012 year were provided for analysis from Medicare and have been aggregated and averaged over total services by professional groupings and service types. The unit costs used in all analyses are detailed in Table 3.
Resource unit costs, sources and assumptions.
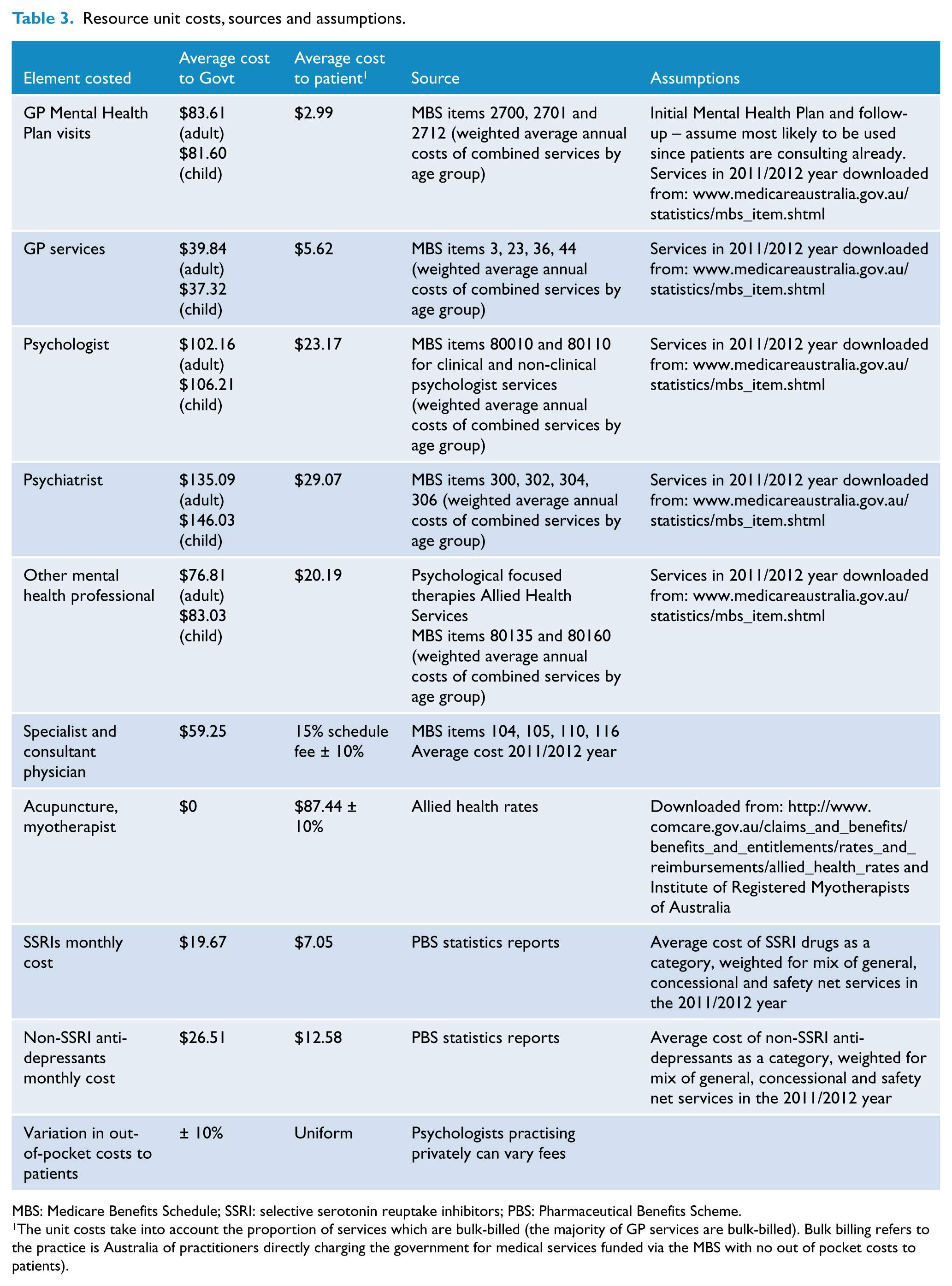
MBS: Medicare Benefits Schedule; SSRI: selective serotonin reuptake inhibitors; PBS: Pharmaceutical Benefits Scheme.
The unit costs take into account the proportion of services which are bulk-billed (the majority of GP services are bulk-billed). Bulk billing refers to the practice is Australia of practitioners directly charging the government for medical services funded via the MBS with no out of pocket costs to patients).
SSRI intervention
For compliers to therapy, among those people taking other anti-depressants, the average monthly cost of the non-SSRI anti-depressant drugs as a class was calculated for the 2011/2012 year. The 9-month non-EBM drug costs were replaced with the average costs of SSRIs for 9 months. In contrast, we added the average cost of taking SSRIs for 9 months to those people expected to comply with treatment, who were not currently taking anti-depressants as part of their drug regime. For non-compliers, only 1–2 months of SSRI drug costs were included as medication costs.
Modelling framework
A simulated population cohort decision-tree model was constructed in Excel which captured the intervention and comparator parameters and provided 95% uncertainty around the incremental cost-effectiveness ratios (refer to Supplementary Figures 1 and 2, available online). Micro-simulation-type models were not considered appropriate in the current context because there was no evidence of heterogeneity of effect across meaningful subgroups and the data requirements of such models are considerable. A 3% discount rate was applied for costs and consequences incurred in years 2–5 of the model.
While there may be some impacts on mortality, in reality these are very small compared to the morbidity impacts of such interventions (Mihalopoulos et al., 2011a; Vos et al., 2005a). Furthermore, there is no evidence from the available trial data that the guideline interventions impact mortality.
Uncertainty and sensitivity analyses
To incorporate the uncertainty associated with all costs and outcomes, Monte Carlo simulation modelling was used (which is a form of multivariate probabilistic uncertainty analysis) and we present uncertainty ranges as well as point estimates for benefits, costs, cost offsets and cost-effectiveness ratios. Details of the parameters varied in the uncertainty analysis are presented in Table 1. The results from these 4000 iterations of the model analyses are presented as scatterplots on a cost-effectiveness plane (Figures 1 –3).
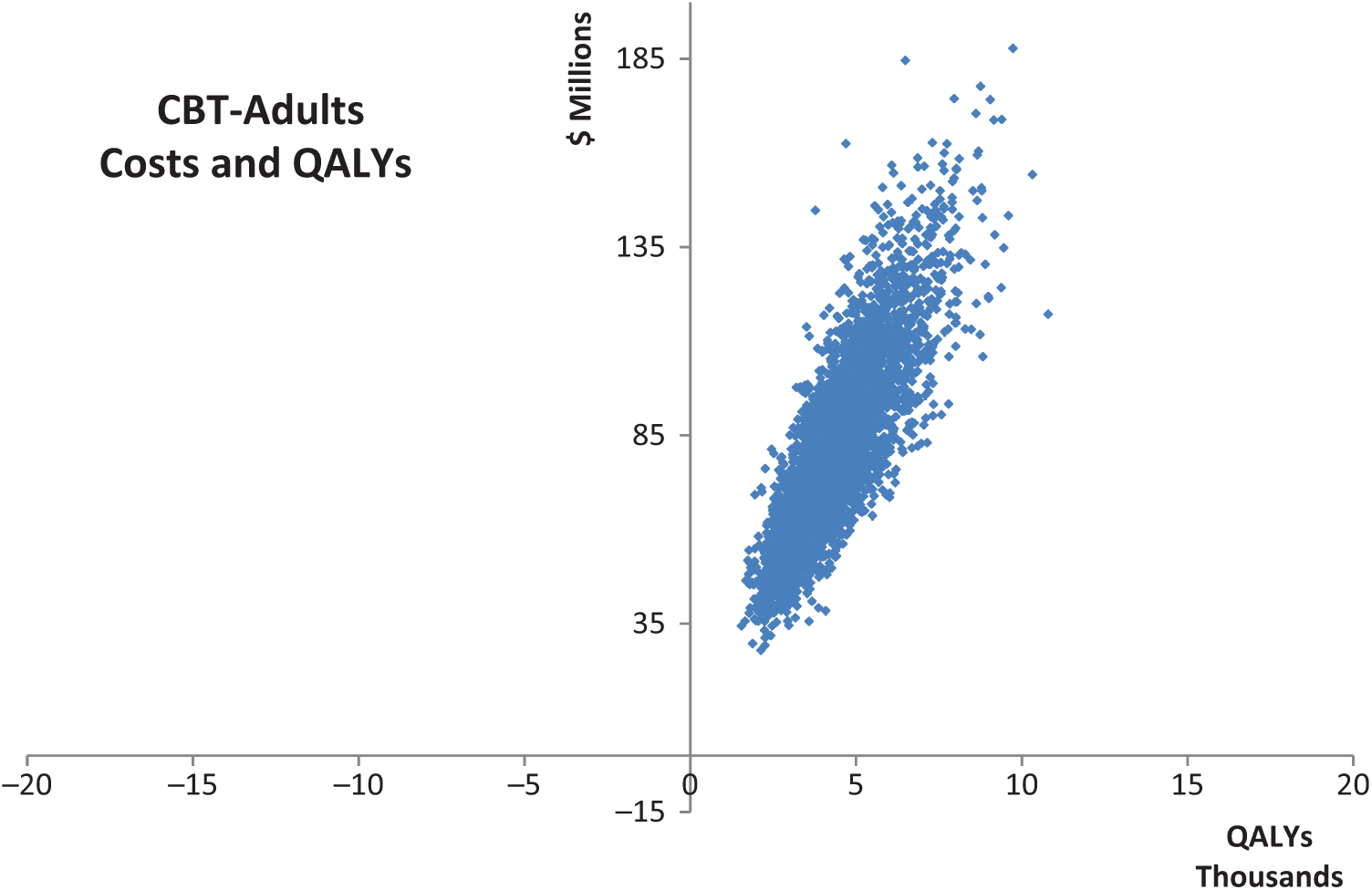
Cost-effectiveness planes – TF-CBT adults.
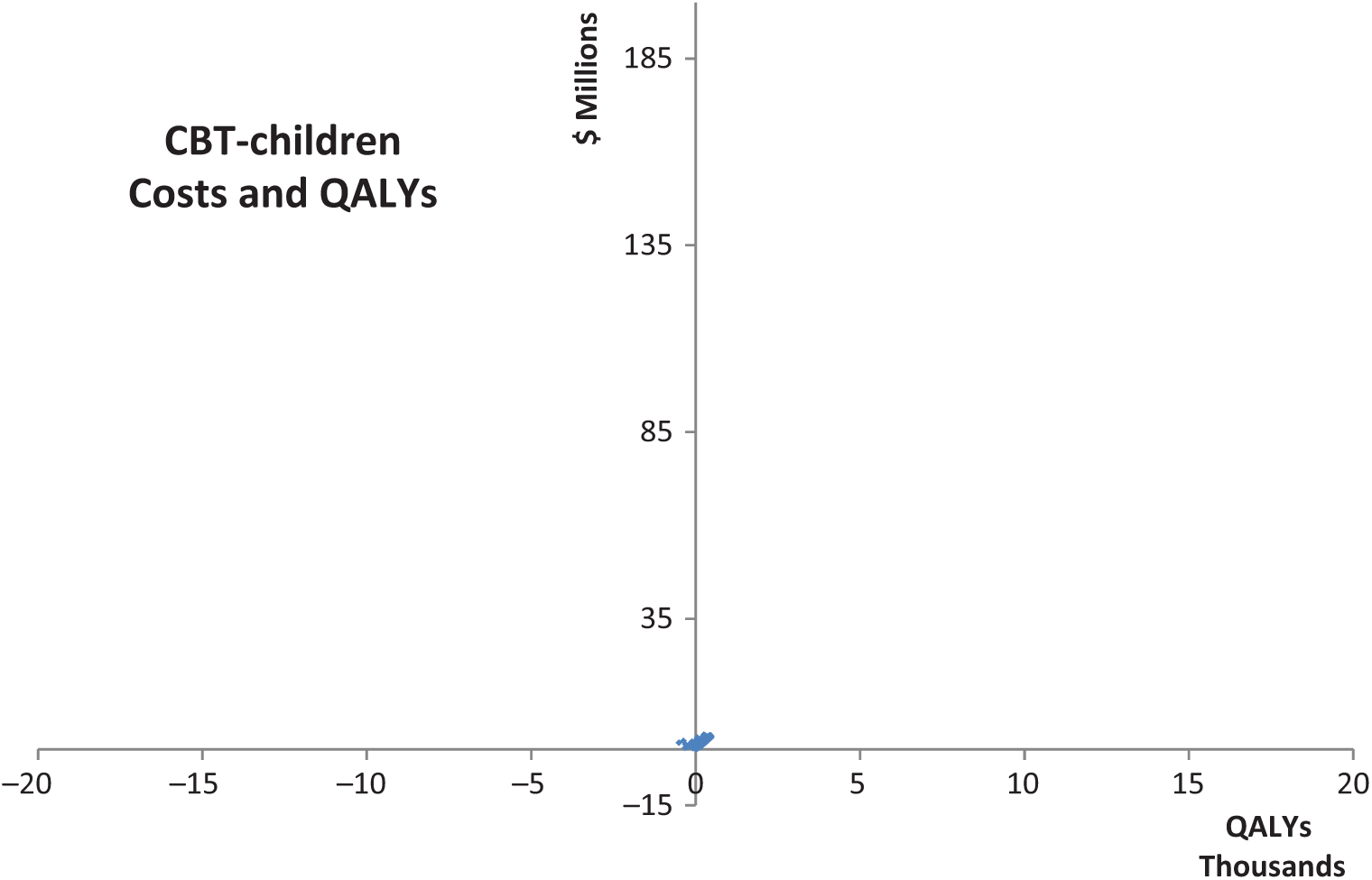
Cost-effectiveness planes – TF-CBT children.
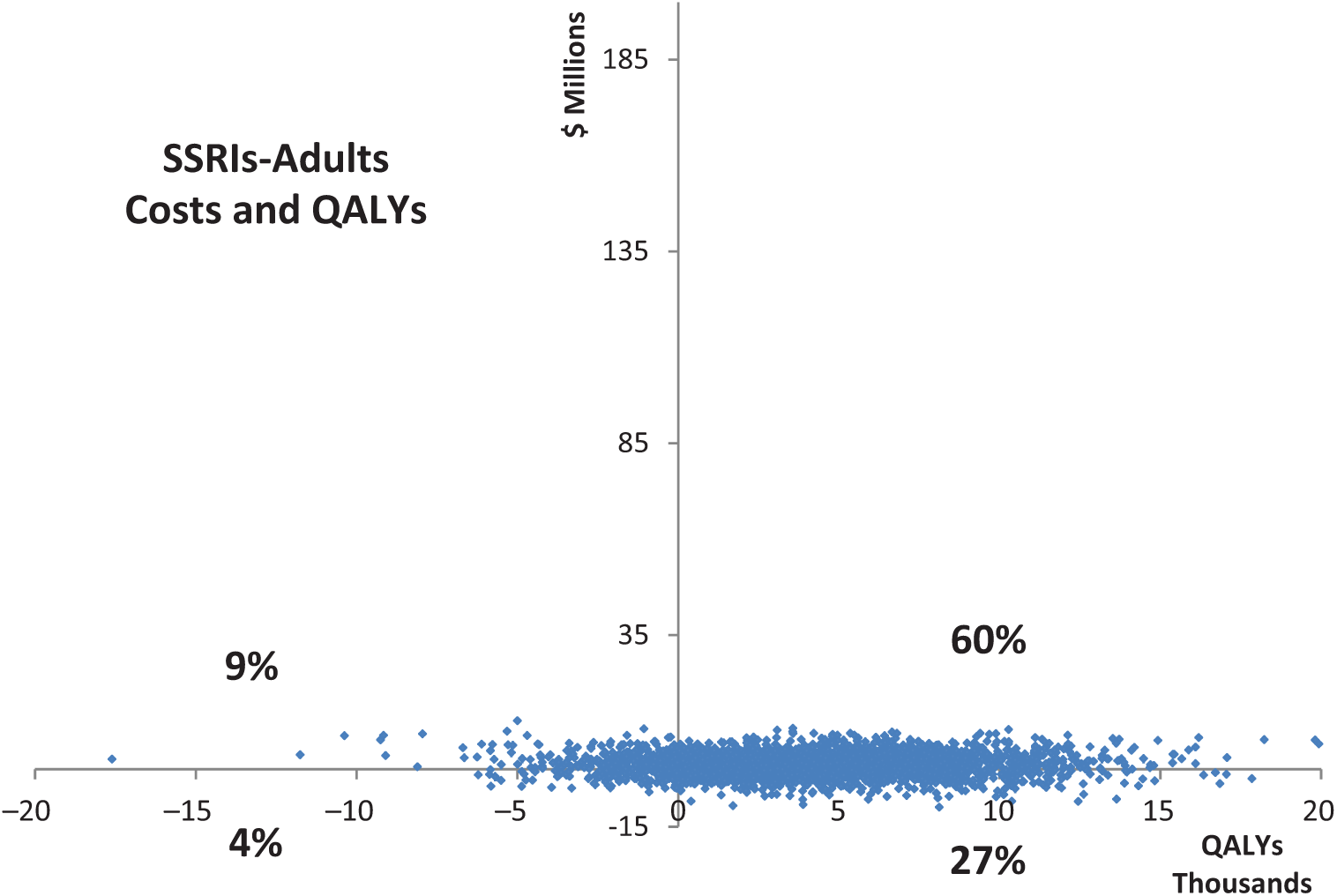
Cost-effectiveness plane – SSRIs to adults.
Sensitivity analysis is a useful addition to probabilistic uncertainty analysis, as it allows the impact of individual assumptions or key design features of an intervention to be examined. As stated above, we also perform a series of sensitivity analyses to test the impact of important structural assumptions in the model (e.g. size of utility gain).
We are also able to report the input variables that contributed most to the uncertainty around the outputs of interest and for which better data are needed to be more confident in results.
Value-for-money threshold
A $50,000 per DALY averted or per QALY gained ‘value-for-money’ threshold has been adopted in this study. Interventions whose ICERs fall below this threshold are considered ‘good’ value for money and interventions whose ICERs fall above this threshold are considered ‘poor’ value for money. This threshold has been used in previous Australian economic evaluation studies and is a ‘rule of thumb’ within the Australian context (Carter et al., 2008).
Results
Trauma-focused CBT
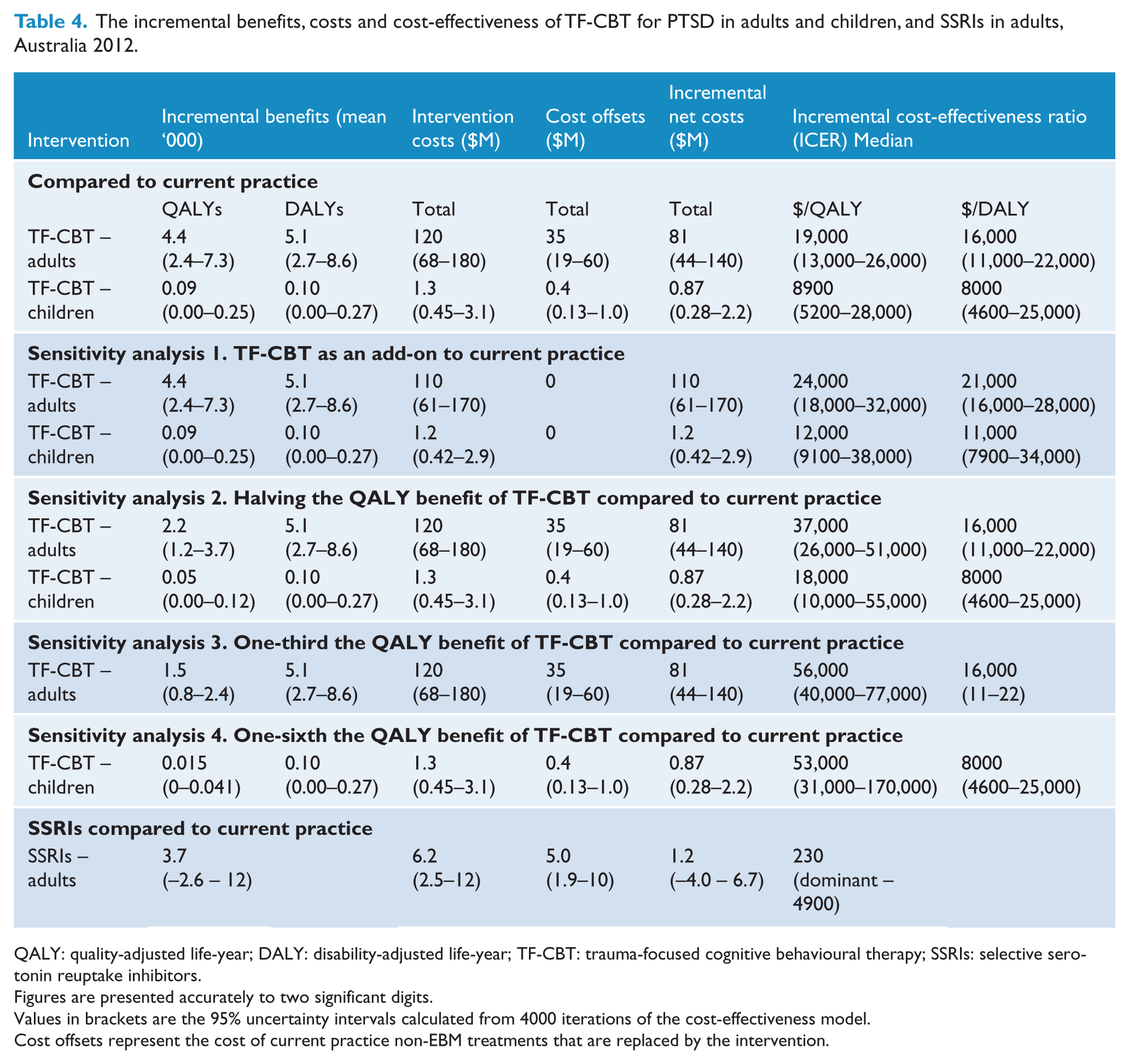
The TF-CBT intervention in adults and children is highly cost-effective. This conclusion holds regardless of whether QALYs or DALYs are used or whether it is modelled as a replacement or add-on to current practice. Results are detailed in Table 4. These ICERs represent good value for money since they are well below the value-for-money threshold of $50,000.
The incremental benefits, costs and cost-effectiveness of TF-CBT for PTSD in adults and children, and SSRIs in adults, Australia 2012.
QALY: quality-adjusted life-year; DALY: disability-adjusted life-year; TF-CBT: trauma-focused cognitive behavioural therapy; SSRIs: selective serotonin reuptake inhibitors.
Figures are presented accurately to two significant digits.
Values in brackets are the 95% uncertainty intervals calculated from 4000 iterations of the cost-effectiveness model.
Cost offsets represent the cost of current practice non-EBM treatments that are replaced by the intervention.
Cost-effectiveness planes are provided in Figures 1 and 2. These plots show that in 100% of the adult model iterations the ICER remains below the $50,000/QALY averted threshold and the same is true in 99% of the children model iterations.
In the sensitivity analysis, when TF-CBT was evaluated as an addition to current practice for both adults and children, the ICERs for both adults and children increased, but remained well below the value-for-money threshold. Details are presented in Table 4.
In a separate sensitivity analysis, reducing the adult QALY utility gain from 0.08 to 0.04 per complier halved the QALYs and the ICER/QALY doubled as expected. When the QALY benefit was reduced in adults to one-third of its original size modelled, the intervention became not cost-effective, passing the threshold to $56,000 per QALY gained. In children, halving the QALY benefit similarly doubled the ICER/QALY. The intervention for children remains cost-effective until the QALY gain is reduced to one-sixth the original size modelled.
The four input variables which were most influential in the degree of uncertainty around QALYs and DALYs gained in adults were the likely participation rates, adherence to treatment, the likelihood of being offered the CBT intervention and the RR of PTSD diagnosis following treatment effect.
The four variables which were most influential in the degree of uncertainty around QALYs and DALYs gained in children were the 12 month prevalence estimate for children, the RR of effect, the likely adherence rates and the likelihood of being considered eligible for CBT treatment.
SSRI intervention
Swapping other antidepressants for SSRIs coupled with prescribing SSRIs to adults on medications but not already taking an antidepressant, has an 87% probability of leading to health gain and a 13% chance of health loss. The intervention has a 69% probability of costing the health sector additional resources and a 31% chance of saving health sector dollars. Owing to this variability in incremental costs and benefits, the intervention has a very cost-effective ICER but with the chance of being either dominant (i.e. saving more resources than what it cost) or dominated (costing more but with no health gain). A cost-effectiveness plane is provided in Figure 3.
The four input variables which were most influential in the degree of uncertainty around QALYs gained in adults were the utility-weights of persons taking either SSRIs, no antidepressants or taking other anti-depressants (where numbers of observations were too small to evaluate by gender or to obtain statistical jackknife population weighting), followed by the likely participation rate taken from the relevant trial evidence. Total intervention costs to the health sector are detailed by payor (Table 5), which highlights the importance of the government as primary payor in these interventions.
Distribution of intervention costs over government funders and patients within the health sector.
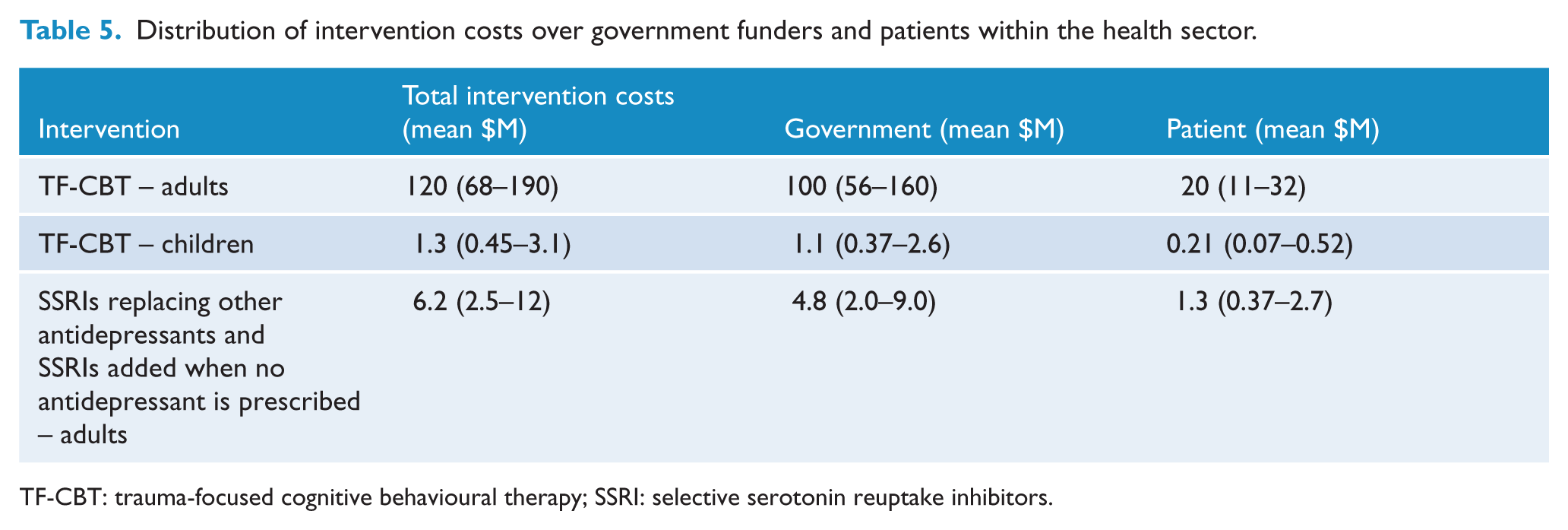
TF-CBT: trauma-focused cognitive behavioural therapy; SSRI: selective serotonin reuptake inhibitors.
Second stage filter criteria
There are a number of issues that are relevant for further consideration in addition to the quantitative analysis – these are detailed in Table 6. The largest issues would appear to be workforce considerations, including reluctant attitudes towards TF-CBT coupled with the ongoing needs for appropriate training and supervision of practitioners. There are difficulties providing TF-CBT to all the children who would benefit, due to the need to engage parents in decision-making. It is also clear that there is potential for greater benefits to families and other sectors (e.g. education) which have not been captured in this health sector-based analysis.
Second stage filter criteria issues.
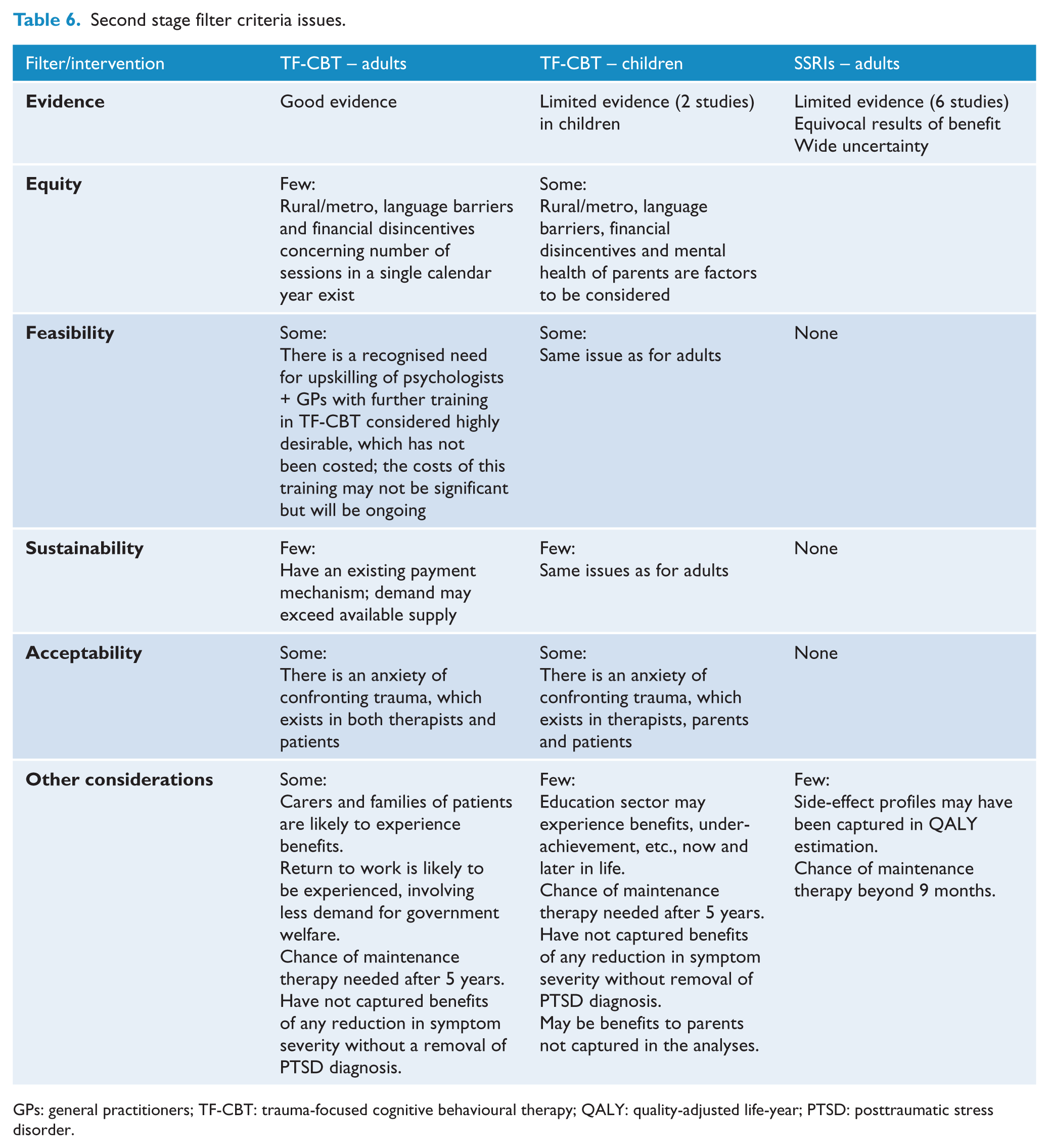
GPs: general practitioners; TF-CBT: trauma-focused cognitive behavioural therapy; QALY: quality-adjusted life-year; PTSD: posttraumatic stress disorder.
Discussion
TF-CBT in adults and children is highly cost-effective in the Australian setting. Prescribing SSRIs to adults currently receiving non-SSRI medications may be cost-effective but there is considerable uncertainty around the benefit and costs. Therefore, the answer to the question of whether a practice shift to these three interventions advocated in the new Guideline recommendations is that there is a very high likelihood that this shift will be highly cost-effective. While the practice shift will not necessarily save resources, it will result in sufficient health gains which are deemed to be ‘worth’ the extra cost.
The results of the current study are largely in the same vicinity as Gospodarevskaya and Segal (2012), which reported an ICER of under $7000/QALY for children with PTSD who were sexually abused. The results for adults in the current study are also similar to those reported by Issakidis et al. (2005) of $15,728/YLD (95% CI $12,550 – $24,311).
While the current study has employed modelling techniques, which are always subject to some uncertainty (Briggs et al., 2008), we have tried to remain as close to the published literature as possible in terms of populating key model parameters. The 2007 NSMHWB has been a valuable source of nationally representative data upon which many of the model parameters were based (e.g. prevalence rates, health-related quality of life and resource use, following intervention changes to current practice evaluated). In this regard the results of the model can be deemed to be fairly representative of the Australian situation. We have separately analysed adults from children and under alternative scenarios, again with consistent findings regarding the cost-effectiveness of the proposed interventions.
Another strength of the study, and a useful addition to the economic evaluation literature more generally, is the use of both QALYs and DALYs to evaluate the health outcome of the interventions. DALYs have gained international prominence as an accepted measure of disease burden in both global and local Australian burden of disease studies (Begg et al., 2007; Murray et al., 2012). However, their use in economic evaluation has been limited outside the WHO Generalised Cost-Effectiveness Analysis studies (WHO-GCEA) (Chisholm, 2005) and the Australian ACE studies in priority-setting (Carter et al., 2008). Both the ACE studies and WHO-GCEA studies are large priority-setting projects which have the requirements of methodological comparability; therefore, the disability-weight used in the derivation of DALYs provides a consistently derived set of disease weights across multiple disorders and diseases. However, the usefulness of DALYs for economic evaluation has been challenged. This is largely because it has been argued that the disability-weights used in quantification of the DALYs are ‘different’ to the utility-weights used in QALYs (Meunnig, 2007; Sassi, 2006). Since the first 1999 Australian burden of disease study, PTSD has been aggregated with all anxiety disorders, which may limit the application of the appropriate disability-weight in the DALY estimation when measuring changes in this disorder following intervention, especially in children. Furthermore, the same disability-weight for both adults and children has been used in these studies.
While the arguments between QALYs and DALYs and the deficiencies of each of these weights remains, it is important to show pragmatically whether the choice of metric dramatically alters the conclusion of the analysis. The current study has demonstrated that regardless of whether QALYs or DALYs are used as the outcome metric, the resulting cost-effectiveness ratios do not dramatically alter and hence the conclusions of the analyses are consistent. This is an important finding and can give some confidence to decision-makers that the cost-effectiveness credentials of these interventions are realistic regardless of whether QALYs or DALYs are used. However, it must be acknowledged that the trials upon which the current analyses are based did not express outcomes in QALYs or DALYs and assumptions regarding each of these generic outcomes had to be made for the current analyses. While the assumptions we used have some face validity among expert advisors, it must be acknowledged that these are only an estimate.
A further strength of the current study is that a conservative approach to modelling potential cost-offsets associated with a switch from current practice to the evidence-based guidelines has been adopted. This pragmatically means that we have ensured that we do not overinflate any likely cost-savings associated with the interventions and hence do not incorrectly decrease the ICER so that it appears to be more favourable.
Of course, as with all modelling studies, there are a number of weaknesses or assumptions associated with the current analysis. Most of these are related to the sources of key model parameters. For example, the standard errors of proportion estimates and utilities increased as smaller numbers of survey-based observations in subgroups were analysed. This led to the wider uncertainty intervals around key results. In any case, the conclusions for the cost-effectiveness of TF-CBT in adults, in particular, were still robust within this context. This means that the majority of model scenarios fell well below the value-for-money thresholds adopted in this incremental analysis. Another weakness, for the child analysis in particular, is the fact that the prevalence and treatment of PTSD in Australian children has never been measured in a nationally representative survey. Similar to other Australian modelled economic evaluations (e.g. Vos et al., 2005a), we have adopted a range of uncertainty around out-of-pocket costs which may not be reflective of the true out-of-pocket costs for this particular population. Finally, while the pooled effectiveness measure for adult TF-CBT was based on 24 randomised trials, only two trials informed the child measure. Therefore, it is not surprising that the uncertainty associated with the effectiveness and cost-effectiveness of TF-CBT in children is higher than that for adults.
The current study did not explicitly track which cases of PTSD should or should not be treated, rather it focused on evaluating evidence-based treatments to those people who are seeking care and not provided such treatment. In reality, not all cases of PTSD will necessarily require care; however, as it is currently impossible to know which cases will self-remit and which will not, the Guidelines recommend that treatment be provided to all whose distress persists such that they meet criteria for PTSD. It is also incumbent that future trials of all PTSD interventions include high-quality economic evaluations so that there is less reliance upon modelling to translate largely clinical-efficacy studies into economic evaluations. Importantly such studies should also include multi-attribute utility measures capable of determining QALYs so that actual individual-level QALY gains can be assessed. While modelling may still be required for population-level impact or longer time horizon modelling, it is imperative that at least the cost-effectiveness of interventions within trials be evaluated at an individual level.
Finally, while the technical results of the current analysis are largely very positive, the analysis did raise a number of issues which need to be addressed in the second stage filter criteria. Notably, the acceptability of TF-CBT to clinicians and clients is an important issue and one which requires appropriate education, support and supervision. In addition, the shortage of suitably qualified therapists and the cost of training and supervising new therapists to provide TF-CBT is acknowledged, but not costed in the current analysis. Finally, in clinical practice, a small number of additional sessions at the commencement of therapy are often required in order to introduce and engage the patient in trauma-focused treatment. It should also be noted that Medicare funds up to 10 psychology treatment sessions per calendar year, while the Guidelines stipulate that 8–12 treatment sessions are generally required. In circumstances where treatment spans across 2 calendar years, the full 12 sessions can be funded through Medicare, but in other cases additional sessions will be at the clients’ expense. Extending the Medicare rebate to cover 12 sessions for the treatment of PTSD would support the implementation of evidence-based treatment.
Conclusion
The three recommended interventions evaluated within the current study which have the strongest evidence base in the new PTSD and ASD (acute stress disorder) treatment guidelines are expected to have a positive impact on the economic efficiency of the treatment of PTSD if adopted in full. While there are gaps in the evidence base which are highlighted in this analysis, policy-makers can have considerable confidence that the three Guideline interventions evaluated in the current analyses and, in particular, TF-CBT, represent a good use of health sector resources. However, in order for adoption of these Guideline recommendations to occur, ongoing training/supervision needs for therapists must be systematically and successfully addressed.
Footnotes
Acknowledgements
We would like to thank the following members of the advisory panel for the economic evaluation: Richard Bartlett, First Assistant Secretary, Medical Benefits Division, Department of Health and Ageing; Jan Coles, Academic and General Practitioner specialising in trauma treatment in general practice, Monash University; Mark Creamer, expert trauma clinician – adult, University of Melbourne; Judy Daniel, First Assistant Secretary, Health and Community Services, Department of Veterans’ Affairs; David Davies, Executive Director Mental Health and Substance Abuse, Department of Health, SA, Representing Mental Health Standing Committee Chair and state and territory Mental Health Directors; Brett McDermott, expert trauma clinician – child and adolescent, Director, Mater Child and Youth Mental Health Service; James McKenzie, Director Health Services, ComCare; David Morton, Director General, Mental Health, Psychology and Rehabilitation, Department of Defence.
The advisory panel members gave time and expert opinion to guide the analysis, and enumerate and assess the impact of the relevant second stage filter issues. We would also like to thank the Australian Centre for Posttraumatic Mental Health who provided us the recent meta-analysis upon which we have relied for evidence of health benefit and who funded this study. Finally, we would like to acknowledge and thank the Australian Bureau of Statistics for the release of the Confidentialised Unit Record File of the 2007 NSMHWB and Medicare Australia who provided service and benefit details of Medicare item numbers (including out-of-pocket expenses) used in the current study.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
The Australian Guidelines for the Treatment of Acute Stress Disorder & Posttraumatic Stress Disorder and the cost-effectiveness analysis of the Guidelines were both funded by Department of Veterans’ Affairs, Department of Defence and beyondblue. The Australian Centre for Posttraumatic Mental Health led the development of the Guidelines and the cost-effectiveness analysis was undertaken independently by Deakin Health Economics. CM is a recipient of a NHMRC Early Career Researcher Fellowship (grant number: 1035887).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.