
Abstract

To the Editor
A 42-year-old gentleman (BM) with schizoaffective disorder diagnosed at age 27 was referred for neuropsychiatric assessment complaining of a decline in cognitive function associated with recurrent symptoms of peripheral paraesthesia, urinary incontinence, blurred vision, falls and heat-sensitivity. The symptoms had been present for several years, but had been attributed to BM’s schizoaffective disorder and the medications used to treat it.
On examination of the patient’s mental state there was no evidence of thought disorder, delusions or hallucinations, but BM’s affect was apathetic and conversation impoverished. On bedside cognitive testing he demonstrated poor recall, impaired visual construction, decreased verbal fluency and impaired response inhibition. Neurological examination revealed a broad-based ataxic gait, bilateral internuclear opthalmoplegia, generalised hyper-reflexia, asymmetric dystonia, generalised muscle weakness and non-habituating primitive reflexes.
MRI of the brain demonstrated extensive white matter high T2 FLAIR plaques (Figure 1(a)) with a predilection for the periventricular region. On sagittal T1 (Figure 1(b)) and coronal T1 (Figure 1(c)) they are seen as ovoid lesions radiating out from the ventricular margin. This appearance is referred to as “Dawson’s fingers” and is characteristic of multiple sclerosis (MS). The corpus callosum is also thinned with an irregular inferior callososeptal border (Figure 1(d)).
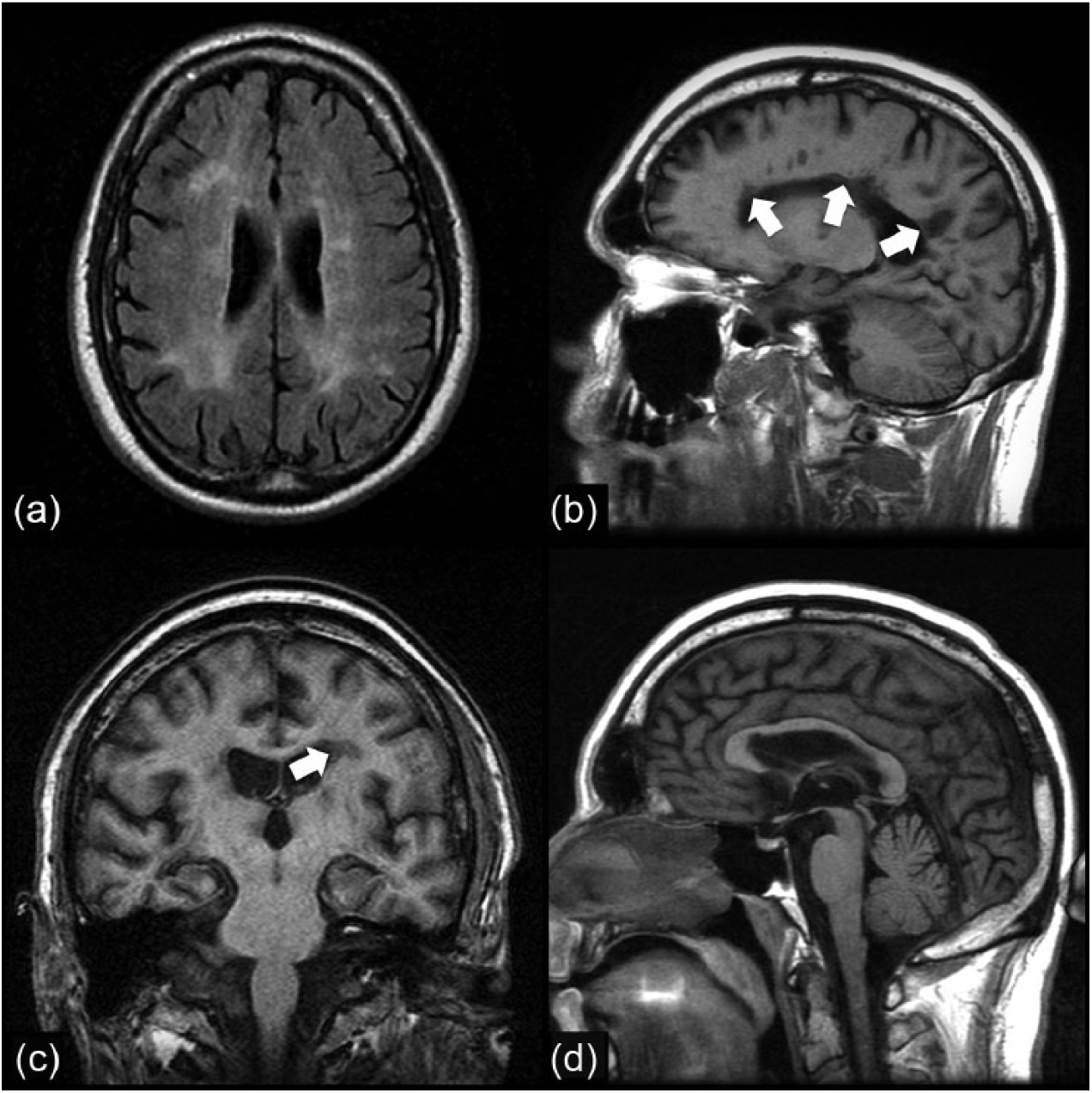
Magnetic resonance imaging findings.
MS was diagnosed, strengthened by the demonstration of oligoclonal bands in cerebrospinal fluid. White cell enzymes were found to be unremarkable, excluding metabolic leukoencephalopathies.
MS is an immune-mediated inflammatory disorder of the central nervous system that usually presents in middle age and causes disseminated axonal demyelination and dysfunction (Compston and Coles, 2008). The clinical presentation is heterogeneous and may follow a relapsing-remitting or progressive course characterised by a diverse range of central and peripheral neurological symptoms. Affective and cognitive manifestations are common (Feinstein et al., 2013) and may have contributed to BM’s diagnosis of schizoaffective disorder.
Patients with mental illness can experience long delays in the diagnosis of physical illness for a variety of reasons, including the phenomenon known as “diagnostic overshadowing”: the misattribution of physical symptoms to mental illness or its treatment (Jones et al. 2008; Lambert et al., 2003). In BM’s case, gait changes, somatic complaints and increasing functional decline were attributed to the progression of his schizoaffective disorder. Once the neurological symptoms and signs were recognised as atypical for this illness, their presence triggered further investigation and an additional diagnosis of MS.
This serves as a reminder that it is important to exclude organic illness in patients who present with atypical symptoms, even in the context of longstanding psychiatric illness. It also cautions against the explanatory complacency that may be associated with a diagnosis of schizoaffective disorder.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.