
Abstract
Objective:
Impaired Theory of Mind (ToM) and insecure (adult) attachment styles have been found in persons with schizophrenia as well as in their healthy siblings. ToM refers to the ability to infer mental states of self and others including beliefs and emotions. Insecure attachment is proposed to underlie impaired ToM, and comprises avoidant (discomfort with close relationships, high value of autonomy) and anxious (separation anxiety, dependency on others) attachment. Insight into the association between attachment style and ToM is clinically relevant, as it enhances our understanding and clinical approach to social dysfunction in schizophrenia. Therefore, we studied the association between insecure attachment styles and ToM in patients with schizophrenia, their siblings, and healthy controls.
Methods:
A total of 111 patients with a diagnosis in the schizophrenia spectrum, 106 non-affected siblings and 63 controls completed the Psychosis Attachment Measure, the Conflicting Beliefs and Emotions, a subsection of the Wechsler Adult Intelligence Scale, and the Childhood Trauma Questionnaire-Short Form. Severity of symptoms was assessed with the Community Assessment of Psychic Experiences and the Positive and Negative Syndrome Scale.
Results:
After controlling for sex, intelligence, history of trauma and symptom severity, avoidant attachment was significantly associated with cognitive as well as with affective ToM, showing U-shaped associations, indicating better ToM performance for patients with lower or higher levels of avoidant attachment compared to medium levels. Anxious attachment in patients was associated with more problems in cognitive ToM.
Conclusion:
The results from this study support the idea that an anxious attachment style is associated with worse ToM performance in patients. Results also suggested a potential protective role of higher levels of avoidant attachment on ToM. These findings bear clinical relevance, as activation of (insecure) attachment mechanisms may affect interpersonal relations, as well as therapeutic working alliance. Further clarification is needed, especially on associations between ToM and avoidant attachment.
Introduction
Patients with psychotic disorders often have impairments in Theory of Mind (ToM) (Corcoran et al., 1995; Fett et al., 2011; Sprong et al., 2007). ToM encompasses the understanding and inference of mental states (beliefs, thoughts and intentions) of self and others. It is conceptually related to mentalization, which concerns the development of the self, and more affectively and interpersonally complex understandings of oneself and others (Choi-Kain and Gunderson, 2008). ToM can be divided into several components: cognitive ToM (inferences about beliefs, thoughts, or intentions), affective ToM (inferences about emotions or feelings), first-order skills (inferring the thoughts/emotions of another person) and second-order skills (inferring what one person – other than the self – thinks about another person’s thoughts/emotions) (Brothers and Ring, 1992; Shamay-Tsoory et al., 2007). ToM impairment is associated with higher paranoid ideation, worse functional outcome, less help-seeking behaviour and poorer therapeutic alliance (Davis et al., 2011; Garety et al., 2001; Lysaker et al., 2005, 2013). In high-risk samples, findings concerning ToM are inconclusive. Impairments in ToM have been found in (ultra) high-risk samples and in persons with a genetic high risk for psychosis (relatives of patients), suggesting a (partly) trait dependency (de Achával et al., 2010; Janssen et al., 2003; Yu et al., 2008). However, others found no evidence for worse ToM performance in relatives (Kelemen et al., 2004). Additionally, ToM impairments were found to worsen during acute phases in schizophrenia, suggesting that ToM deficits may also be (partly) state dependent (Pousa et al., 2008).
Fonagy and Target (1997) proposed that ToM skills are more likely to develop within secure attachment bonds. Attachment theory provides a developmental framework of interpersonal experiences that plays a role in regulating cognition, affect and (interpersonal) behaviour and is associated with resilience, interpersonal functioning, and psychological symptoms (Bentall et al., 2007; Berry et al., 2008; Rutten et al., 2013). Attachment bonds and ToM skills start to develop in childhood, and Meins and colleagues (1998) found evidence for an association between attachment and ToM in a longitudinal study in which securely attached children had superior ToM compared to insecurely attached children. Finally, childhood trauma (which may indicate insecure attachment) is associated with poorer ToM in adults (Lysaker et al., 2011; Nazarov et al., 2014). These studies indicate that (childhood) attachment and ToM may be related.
For insecure adult attachment, which guides interpersonal functioning and social life in adults, a distinction is often made between anxious and avoidant attachment styles (Berry et al., 2008). Individuals with high levels of anxious attachment need approval from others, are likely to experience separation anxiety, and engage in an interpersonal style generally marked by fixing attention on distressing stimuli. Individuals with high levels of avoidant attachment tend to feel uncomfortable with closeness to others, value their autonomy and divert attention from distressing stimuli and attachment-related thoughts and feelings (Berry et al., 2008; Fraley et al., 1998). Anxious and especially avoidant adult attachment are more prevalent in people with psychotic disorders (Gumley et al., 2014; Mickelson et al., 1997) and are associated with poorer engagement with health care services and lower therapeutic alliance, treatment adherence/compliance and social dysfunction (Gumley et al., 2014), and poorer recovery (Drayton et al., 1998).
Findings suggest, in line with the above-mentioned state-dependency of ToM performance, that ToM abilities may diminish as a function of perceived social threat which can arise in the context of therapeutic alliances when interacting activates the (insecure) attachment system (Liotti and Gilbert, 2011). Knowledge about the interplay between attachment styles and ToM may help therapists in being especially alert to ToM impairment in schizophrenia patients, as this ability can change as a function of perceived threat, which thus may indicate activation of insecure attachment systems. Findings further suggest that ToM in schizophrenia is also associated with a basal deficit (e.g. a lack of ability associated with negative symptomatology, intellectual functioning and disorganization/thinking disorders) (Brune, 2005). Impaired ToM may be improved with use of (social-) cognitive training (Kurtz and Richardson, 2012), which can help schizophrenia patients in accurately determining others’ intentions, including those of therapists, thereby facilitating therapeutic alliance and outcome. Summarizing, investigating how ToM is associated with insecure adult attachment is of interest as it may shed light on the cognitive structure underlying social dysfunction.
To investigate ToM/mentalization and attachment styles in schizophrenia, MacBeth and colleagues (2011) assessed 34 patients with a first-episode psychosis. Attachment was differentially associated with mentalization: poorer mentalizing skills were associated with avoidant attachment but not with anxious attachment. However, findings from this study are inconclusive with respect to anxious attachment due to small sample size. In another study among 32 patients with early-onset psychosis, no association was found between perspective taking – a key component of cognitive ToM – and attachment, likely as a result of assessing cognitive rather than affective ToM skills (Korver-Nieberg et al., 2013). As attachment style encompasses affect regulation, affective ToM may be more strongly associated with attachment than cognitive ToM. Studying cognitive and affective ToM, as well as first-order skills (‘first-order belief’ for cognitive ToM and ‘first-order emotion’ for affective ToM) and second-order skills (‘second-order belief’ and ‘second-order emotion’), may clarify specific ToM impairment in psychotic disorders and its relationship with attachment styles (Korver-Nieberg et al., 2013; Shamay-Tsoory et al., 2007).
The aim of the current study was to explore attachment and ToM in patients, siblings and healthy controls and to look at whether this association differed between these three groups that vary in genetic vulnerability and confounding illness-related factors. As sex, intelligence, symptom severity and a history of traumatization are associated with ToM and attachment, these variables were included as covariates (Ibanez et al., 2013; Meijer et al., 2012; Nazarov et al., 2014). We hypothesized that (a) patients would report higher levels of insecure attachment and (b) experience poorer ToM skills than siblings and controls, and that (c) ToM would be associated with attachment style, with the most pronounced associations between attachment and affective ToM.
Methods
Subjects
The present study was an add-on study of the Genetic Risk and Outcome of Psychosis (GROUP) research project, a naturalistic, longitudinal cohort study, and included samples recruited by the Amsterdam site. Inclusion criteria at baseline for patients and their siblings were the following: (a) age range of 16–50 years (extremes included); (b) a diagnosis of non-affective psychotic disorder according to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition Text Revision (DSM-IV-TR) criteria (APA, 2000); (c) good command of the Dutch language; and (d) able and willing to give written informed consent. Similar criteria applied to siblings, except that non-affective psychotic disorder was an exclusion criterion. Exclusion criteria for healthy controls were a lifetime psychotic disorder in the subject or in first-degree family (Korver et al., 2012). For this study, 111 patients, 106 siblings and 63 controls were included. Of the 111 patients, 59 had paranoid schizophrenia; 20 schizo-affective disorder; 10 a psychotic disorder not otherwise specified (NOS); eight residual, four undifferentiated, three disorganized, and two schizophreniform schizophrenia; two had a brief psychotic disorder; two a drug-induced psychotic disorder; and one had a delusional disorder.
Instruments
Attachment
Attachment was assessed with the Psychosis Attachment Measure (PAM; Berry et al., 2006), Dutch translation (Korver-Nieberg et al., 2014), which is developed to assess adult attachment style in psychosis. The Dutch PAM is a 15-item questionnaire referring to thoughts, feelings and behaviours, rated on a 4-point answer scale ranging from 0 ‘not at all’ to 3 ‘very much’. Seven items reflect avoidant attachment and eight reflect anxious attachment. Average item scores were calculated for attachment anxiety and avoidance, with higher scores reflecting higher levels of insecure attachment.
Theory of Mind
To assess cognitive and affective ToM, a shortened version of the Conflicting Beliefs and Emotions (CBE) (Shaw et al., 2004; Swart et al., 2009) was administered. This task consists of four vignettes, each concerning a short story involving a social situation featuring two actors. Each story is followed by five questions testing the subjects’ understanding of first-order and second-order belief as well as emotional states of the actors in the story. Two control questions are included to test recall of the story and the making of inferences. Each correct response is assigned 1 point; wrong answers receive no points. Average scores of first-order belief (FOB) (range 0–4), first-order emotion (FOE) (range 0–8), second-order belief (SOB) (range 0–4), second-order emotion (SOE) (range 0–4), and control questions (range 0–8) were calculated.
Intelligence
To estimate IQ, the following four subtests of the Wechsler adult intelligence scale were employed (Wechsler, 2000): Arithmetic, Digit Symbol-coding, Information and Block Design (Blyler et al., 2000).
Symptoms
The Positive and Negative Syndrome Scale (PANSS) was administered to assess the severity of positive and negative symptoms in patients and is one of the most widely used interviews to assess the symptoms of schizophrenia (Peralta and Cuestab, 1994).
The Community Assessment of Psychic Experiences (CAPE) was administered to assess subclinical positive and negative symptoms in siblings and controls. Studies using the CAPE in general population samples have shown good psychometric properties in terms of reliability and validity (Konings et al., 2006).
Trauma
The Childhood Trauma Questionnaire-Short Form (CTQ-SF) was administered to measure childhood trauma, and the total score was used (Daalder and Bogaerts, 2011).
Data analyses
Owing to the nature of the data, linear mixed models (LMM) were conducted with use of IBM SPSS 20.0 (IBM Corp., Armonk, NY, USA). As patients and siblings were part of the same family, their ToM and IQ scores may not be considered independent. A random effect for ‘family’ was therefore included in the models. This random effect represented unobserved heterogeneity between families, and therefore explicitly modelled the intra-familial correlations (Heck et al., 2010). Fit of the models was assessed by means of change in log-likelihood. To facilitate interpretation of the betas in LMM, the IQ scores were centred on the total group mean. As the precise association between attachment and ToM is not yet clear, polynomials (i.e. the squared scores on avoidant and anxious attachment) were included in the LMM model and model fit was determined. To minimize multicollinearity, centred scores were used for the attachment and squared attachment variables.
LMM were conducted as follows:
In the first model, group differences in attachment were assessed; status (control, sibling, patient) was entered as an independent variable and insecure attachment as a dependent variable. Status was treated as a fixed factor.
In the second model, group differences in ToM were assessed; status was entered as an independent variable and ToM as a dependent variable.
In the final model, analyses were performed per status group to explore the association between ToM (dependent variable; repeated for all ToM factors) and scores on attachment (both avoidant and anxious attachment in the same model) whilst including IQ, sex, positive and negative symptoms, and trauma.
Results
We refer to Table 1 for demographics and to Table 2 for a summary of results concerning models 1 and 2.
Descriptive statistics concerning demographics and illness-related variables.
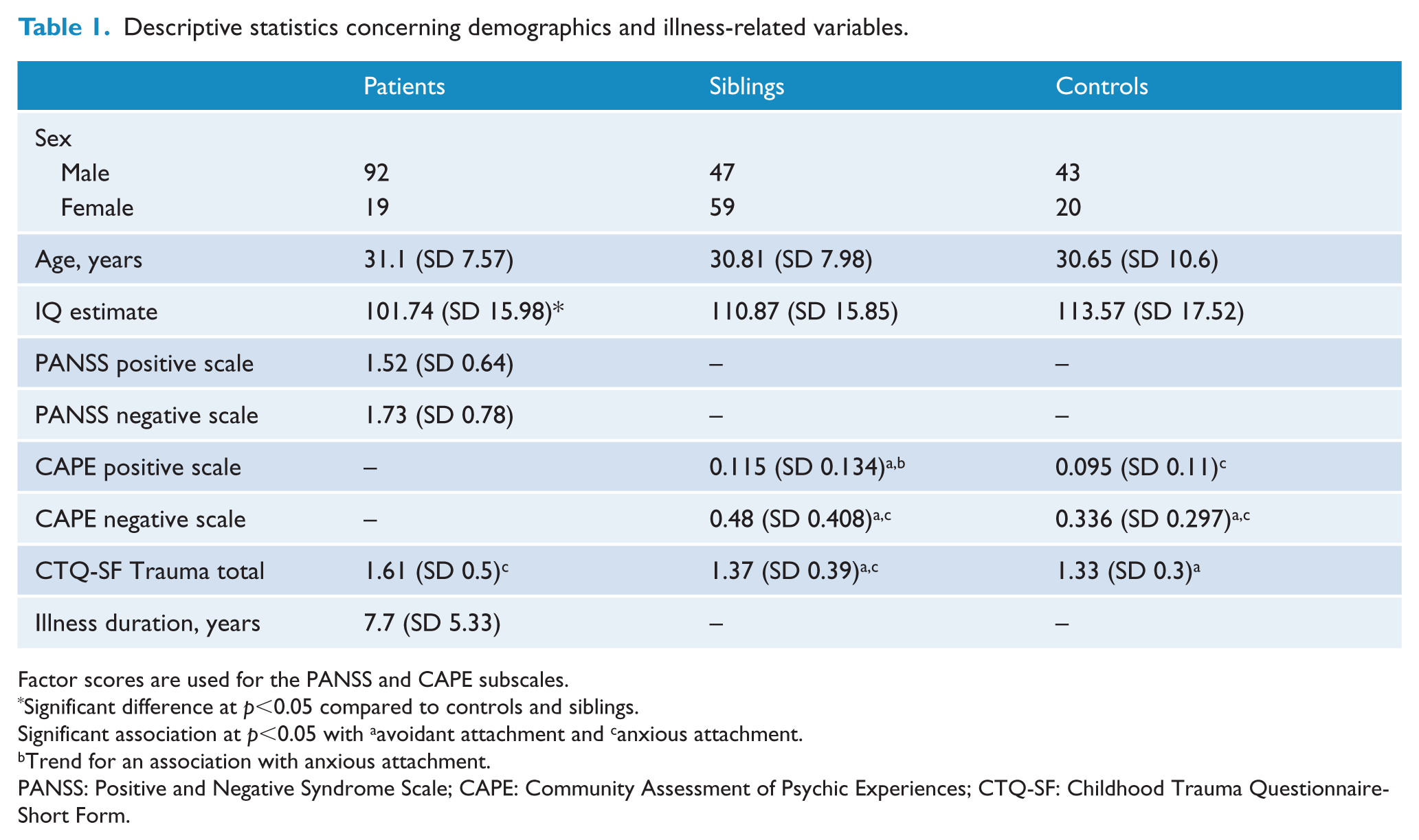
Factor scores are used for the PANSS and CAPE subscales.
Significant difference at p<0.05 compared to controls and siblings.
Significant association at p<0.05 with aavoidant attachment and canxious attachment.
Trend for an association with anxious attachment.
PANSS: Positive and Negative Syndrome Scale; CAPE: Community Assessment of Psychic Experiences; CTQ-SF: Childhood Trauma Questionnaire-Short Form.
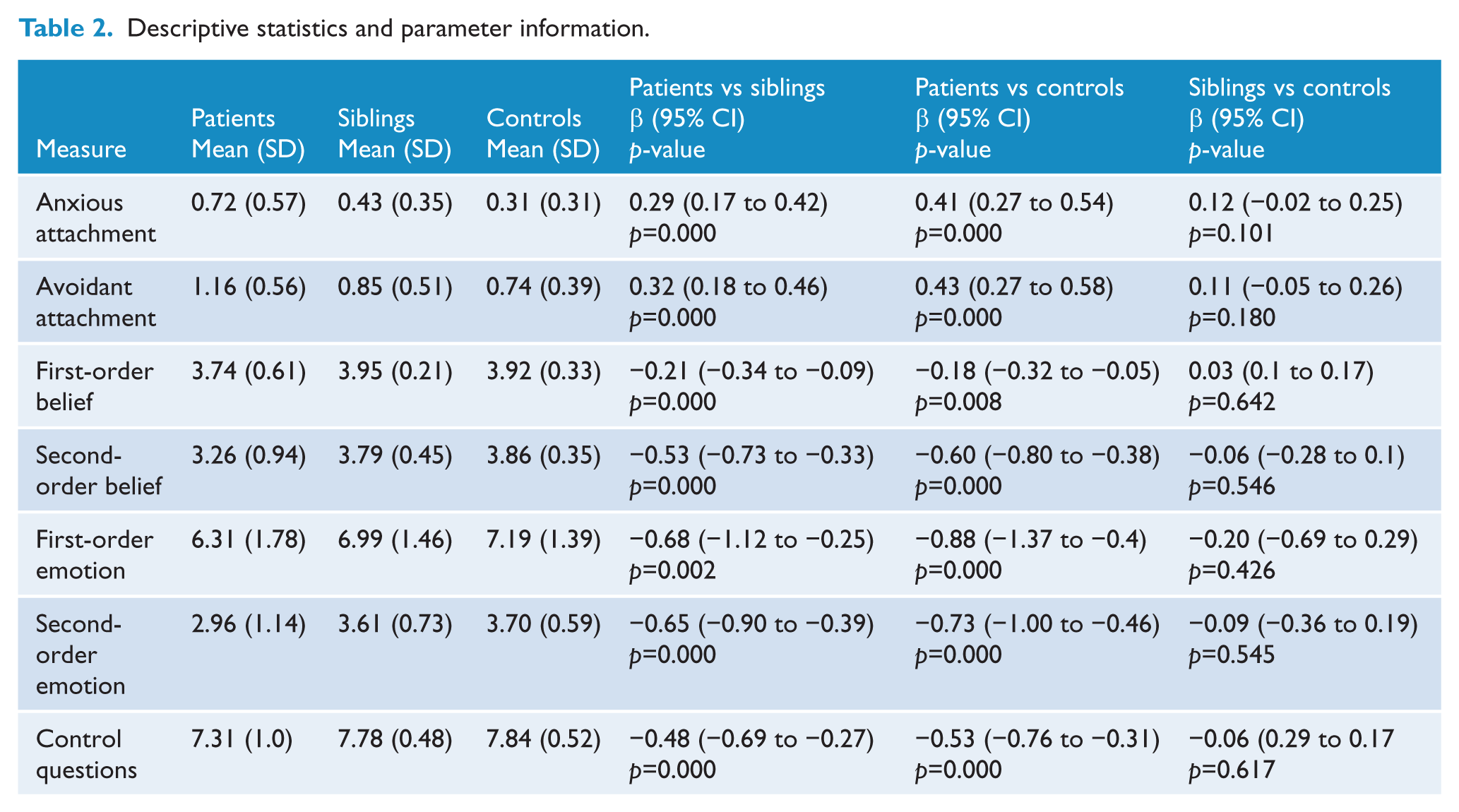
Descriptive statistics and parameter information.
First model: between-group differences in insecure attachment
Patients scored significantly higher on anxious attachment than siblings (β=0.29, p=0.000) and significantly higher than controls (β=0.41, p=0.000). The difference between siblings and controls reached trend level significance (β=0.12, p=0.101).
Patients scored significantly higher on avoidant attachment compared to siblings (β=0.32, p=0.000) and compared to controls (β=0.43, p=0.000). The difference between siblings and controls was not significant.
Second model: between-group differences in ToM
Control questions
Patients scored significantly lower on the control questions than siblings (β=−0.48, p=0.000) and controls (β=−0.53, p=0.000). The difference between siblings and controls was not significant. This indicated that patients had a poorer understanding of the stories than their siblings and controls. To adjust for these differences, the scores on the control questions were factored in the final LMM model besides IQ, sex, trauma (CTQ-SF) and (subclinical) symptoms: for patients PANSS positive and negative subscales; for siblings and controls CAPE positive and negative subscales.
First-order belief
Patients scored significantly lower on FOB than siblings (β=−0.21, p=0.000) and controls (β=−0.18, p=0.008). Differences between siblings and controls were not significant.
First-order emotion
Patients scored significantly lower on FOE than siblings (β=−0.68, p=0.002) and controls (β=−0.88, p=0.000). Differences between siblings and controls were not significant.
Second-order belief
Patients scored significantly lower on SOB than siblings (β=−0.53, p=0.000) and controls (β=−0.60, p=0.000). Differences between siblings and controls were not significant.
Second-order emotion
Patients scored significantly lower on SOE than siblings (β=−0.65, p=0.000); and controls (β=−0.73, p=0.000). Differences between siblings and controls were not significant.
Final model: within-group analysis of insecure attachment and ToM
We refer to Table 3 for a summary of results concerning the final model.
Within-group associations between insecure attachment and Theory of Mind.
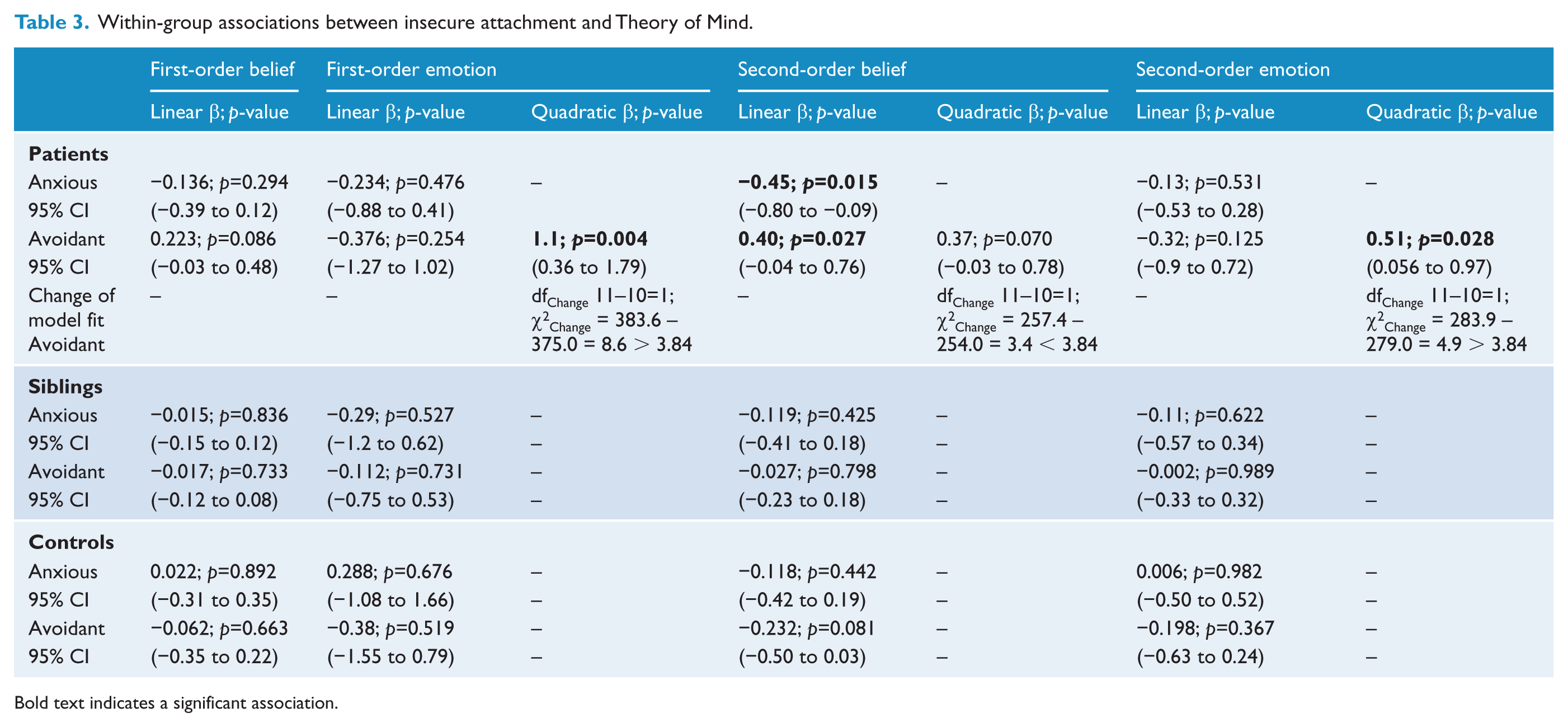
Bold text indicates a significant association.
Within-group analyses of insecure attachment and first-order belief
Further analysis revealed that avoidant attachment was trend-like associated with FOB in patients (β 0.223; p=0.086). Anxious attachment was not associated with FOB in patients. Both anxious and avoidant attachment were not associated with FOB in siblings or controls.
Within-group analyses of insecure attachment and first-order emotion
Analysis revealed that a linear association between avoidant attachment and FOE was not significant in patients. Adding the polynomial led to a significant improvement in model fit, after which a significant quadratic association between avoidant attachment and FOE was found (β=1.1; p=0.004). This indicated a u-shaped association (Figure 1). There was no association between anxious attachment and FOE in patients.
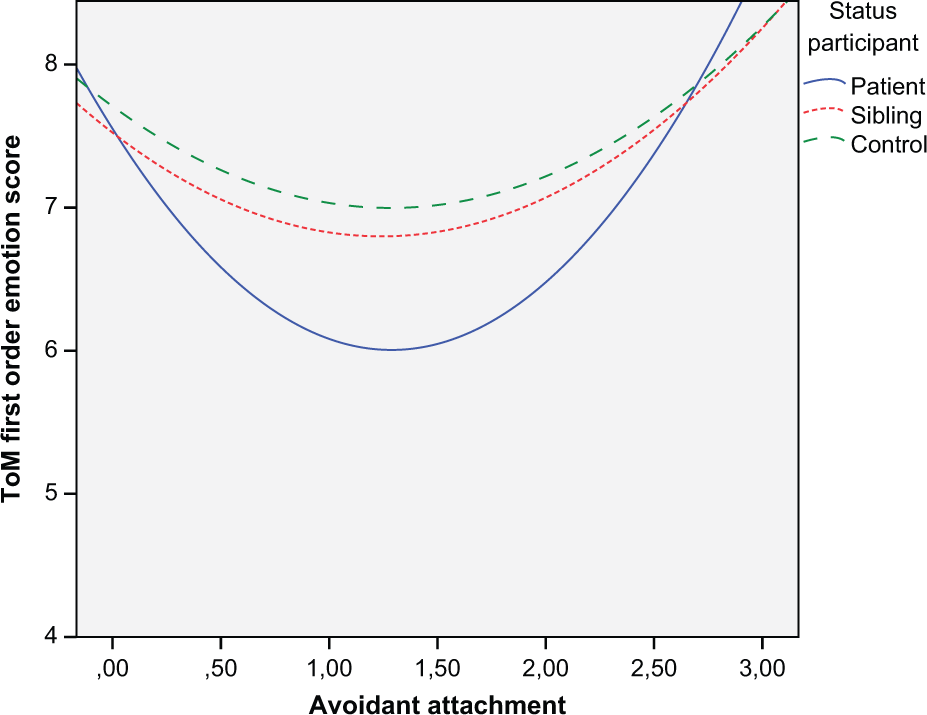
Association between first-order emotion and avoidant attachment. Significant u-shaped association for patients as measured with mixed models; lower and higher scores on avoidant attachment indicate better ToM first-order emotion compared to medium scores on avoidant attachment.
Neither anxious attachment nor avoidant attachment was associated with FOE in siblings or in controls.
Within-group analyses of insecure attachment and second-order belief
Anxious attachment was significantly linearly associated with SOB in patients (β=−0.45; p=0.015); patients with higher anxious attachment tended to have more problems with SOB compared with lower scoring patients.
Avoidant attachment was significantly linearly associated with SOB in patients (β=0.40 ; p=0.027), indicating overall better performance on SOB for patients when avoidant attachment was higher. Adding the polynomial led to a non-significant improvement in model fit. However, a quadratic association seemed to fit the data as well, and the association between SOB and avoidant attachment was trend-like quadratic (β=0.37; p=0.070), suggesting a u-shaped association with a positive slope (Figure 2) .
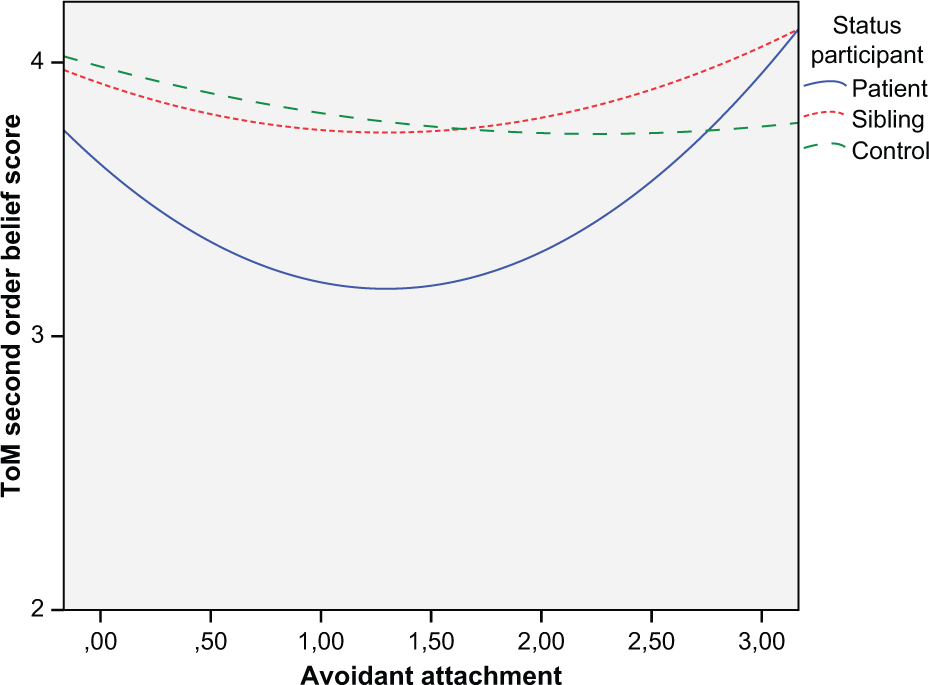
Association between second-order belief and avoidant attachment. Significant u-shaped association for patients as measured with mixed models; lower and higher scores on avoidant attachment indicate better ToM second-order belief compared to medium scores on avoidant attachment.
Avoidant attachment was trend-like associated with SOB in controls (−0.232; p=0.081), suggesting worse SOB as scores on avoidant attachment rise. Anxious attachment was not associated with SOB in controls. Neither anxious attachment nor avoidant attachment was associated with SOB in siblings.
Within-group analyses of insecure attachment and second-order emotion
A quadratic association between avoidant attachment and SOE was significant in patients (β=0.51; p=0.028). This indicated a u-shaped association (Figure 3) . Anxious attachment was not associated with SOE. Neither anxious attachment nor avoidant attachment was associated with SOE in siblings or controls.
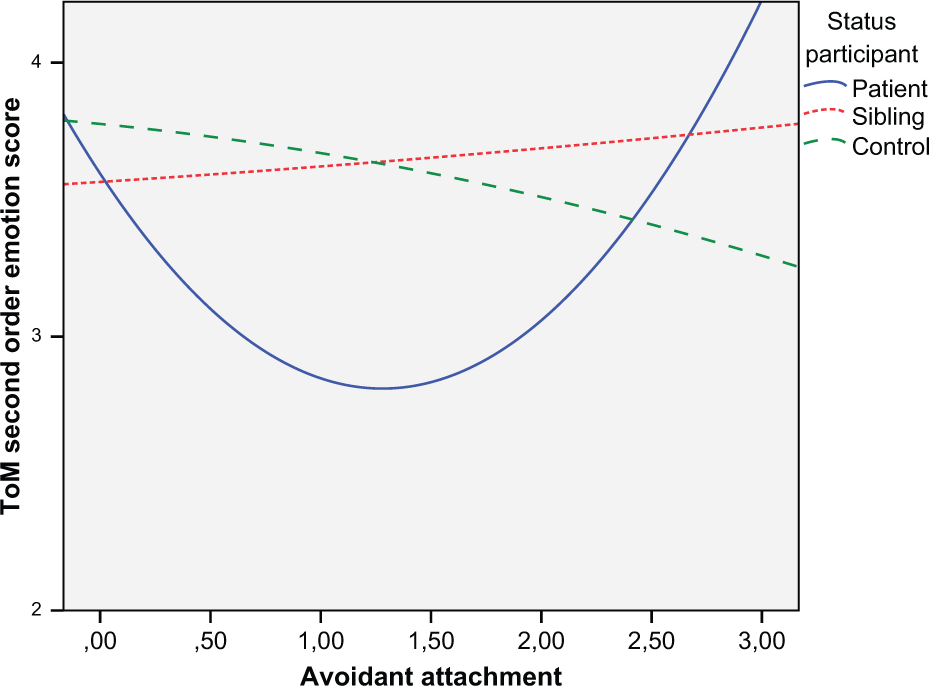
Association between second-order emotion and avoidant attachment. Significant u-shaped association for patients as measured with mixed models; lower and higher scores on avoidant attachment indicate better ToM second-order emotion compared to medium scores on avoidant attachment.
Discussion
In line with our hypotheses and earlier research findings, we found that (a) patients scored higher on avoidant and anxious attachment than their siblings and controls; and (b) patients performed worse on cognitive and affective ToM than their siblings and controls (Corcoran et al., 1995; Fett et al., 2011; Korver-Nieberg et al., 2013; MacBeth et al., 2011; Sprong et al., 2007). Differences in attachment between siblings and controls were non-significant. We also found no evidence for worse ToM in siblings compared to controls.
Association between attachment and ToM
Regarding the association between ToM and attachment (after controlling for severity of symptoms, trauma, IQ and sex), we found that (a) significant associations between ToM and attachment occurred more in affective than in cognitive ToM; (b) these associations mostly occur in the patient group; and (c) most relations are non-linear. Taken together, we found some evidence that insecure attachment style moderates ToM and that being diagnosed with psychotic disorder uniquely contributes to this association.
One explanation for the heterogeneity in these associations is that insecure attachment differentially moderates ToM. Fonagy and Luyten (2009) argue that higher anxious attachment is associated with a lowered threshold for the activation of defensive/insecure coping mechanisms (activation of insecure attachment-related behaviour) and simultaneously for ToM/mentalization deactivation; persons with higher scores on anxious attachment may be more easily overwhelmed by social information and emotionally demanding tasks, which is congruent with our finding that higher anxious attachment is indeed (strongly) associated with worse second-order belief in patients. Fonagy and Luyten (2009) further propose that avoidant attachment strategies may be associated with a more stable or persistent (e.g. less reactive to emotionally demanding tasks) functioning ToM. This is in accordance with our finding that better affective ToM performance was related with higher levels of avoidant attachment in patients.
No association between attachment and ToM in siblings was found.
In contrast to patients, controls with higher levels of avoidant attachment tend to perform worse on second-order belief (non-significant) when avoidant attachment scores rise. A possible, although speculative, explanation is that the moderating effect of avoidant attachment is level-dependent (i.e. suggesting a threshold value of avoidant attachment after which positive moderating takes effect). As scores on avoidant attachment were notably higher for patients, the positive effect of avoidant attachment on ToM may come to the fore in this group, as is found in the right-hand extreme of the u-shaped association. Medium or borderline scores on avoidant attachment, compared to a zero score on this scale, may represent a mixture of secure and insecure attachment styles and in effect an inadequate/incomplete avoidant coping/defensive mechanism (e.g. not being able to completely ignore attachment-related information). Medium scores on avoidant attachment, compared to either low or high scores, may then be related to diminished ToM as the inadequate attachment coping/defensive mechanism falls short. However, we would like to point out that results for controls should be interpreted cautiously, especially with regard to the finding of non-significant relationships in siblings.
The above-mentioned findings seem in contrast with the findings of MacBeth and colleagues (2011), who found that dysfunction in mentalization was associated with avoidant attachment. It is likely that the operationalization of mentalization in the latter study (as a more complex social skill) may account for these differential findings. As stated, Korver-Nieberg et al. (2013) were unable to find associations between ToM and attachment, probably due to (a) the relatively low sample size and (b) assessing cognitive rather than affective ToM. Our results indeed suggest that associations between ToM and attachment occurred more in affective ToM. Also, the proposed differential moderation of ToM by attachment may further complicate analyses; future research should further explore non-linear associations between these constructs, and other possible confounders/covariates.
Also, future research may clarify how psychotic symptoms, and especially paranoid ideation, as a possible expression of inadequate mentalization, may result from the interplay between rooted dysfunctional schemes that inherently operate within insecure attachment styles and impaired cognitive skills, such as afflicted ToM (MacBeth et al., 2011; Sprong et al., 2007). Also, further clarification is needed on the possible protective effect of avoidant attachment on ToM deficits, especially in relation to more complex interpersonal situations.
Summarising, the results from this study support the idea that insecure attachment style is associated with ToM function in patients. This association is clinically relevant, as different interpersonal styles (related to adult attachment) may be related to problems in ToM, which can then constitute a possible risk for therapeutic processes and other social interactions (Berry et al., 2007; Slade, 1999).
This study has several limitations. First, scores on first-order belief suggest that there was a ceiling effect, possibly explaining the failure to find significant associations. Second, measurement of ToM and attachment were conducted by single methods compromising robustness of results. However, the instrument we used to measure attachment is well validated and appeared to be reliable in earlier studies (Korver-Nieberg et al., 2014). Third, given multiple comparisons and trend findings, the results should be interpreted cautiously. Finally, due to the cross-sectional design of the study, conclusions about causality between attachment and ToM cannot be drawn.
Footnotes
Acknowledgements
We are grateful for the generosity of time and effort by the patients and their families, healthy subjects, and all researchers who make this GROUP project possible.
Contributors
The original study design was proposed by NKN and AABV, data-analysis and the writing of the first and subsequent drafts was conducted by KP. All authors contributed to and have approved the final manuscript.
Funding
The first author received no funding. The infrastructure for the GROUP study is funded through the Geestkracht programme of the Dutch Health Research Council (ZON-MW, grant number 10-000-1001), and matching funds from participating pharmaceutical companies (Lundbeck, AstraZeneca, Eli Lilly, Janssen-Cilag) and universities and mental health care organizations (Amsterdam: Academic Psychiatric Center of the Academic Medical Center and the mental health institutions GGZ Ingeest, Arkin, Dijk en Duin, GGZ Rivierduinen, Erasmus Medical Center, GGZ Noord Holland Noord; Maastricht: Maastricht University Medical Center and the mental health institutions GGZ Eindhoven en de Kempen, GGZ Breburg, GGZ Oost-Brabant, Vincent van Gogh voor Geestelijke Gezondheid, Mondriaan Zorggroep, Prins Clauscentrum Sittard, RIAGG Roermond, Universitair Centrum Sint-Jozef Kortenberg, CAPRI University of Antwerp, PC Ziekeren Sint-Truiden, PZ Sancta Maria Sint-Truiden, GGZ Overpelt, OPZ Rekem; Groningen: University Medical Center Groningen and the mental health institutions Lentis, GGZ Friesland, GGZ Drenthe, Dimence, Mediant, GGNet Warnsveld, Yulius Dordrecht and Parnassia psycho-medical center (The Hague); Utrecht: University Medical Center Utrecht and the mental health institutions Altrecht, GGZ Centraal, Riagg Amersfoort and Delta).
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.