
Abstract
Objective:
Impaired Theory of Mind (ToM) is found in adults with schizophrenia and is associated with paranoid symptoms. Insecure attachment is proposed to underlie impaired ToM as well as paranoia. Insight into associations between insecure attachment and impaired ToM skills may help clinicians and patients to understand interpersonal difficulties and use this knowledge to improve recovery. This study used a visual perspective-taking task to investigate whether cognitive ToM is already impaired in adolescents with early psychosis as compared to controls. Also investigated was whether perspective-taking and paranoia are associated with insecure (adult) attachment.
Methods:
Thirty-two adolescent patients with early psychosis and 78 healthy controls participated in this cross-sectional study design and completed the level 1 perspective-taking task, psychopathology assessments (CAPE, PANSS), paranoid thoughts (GPTS), attachment style (PAM) and the WASI vocabulary.
Results:
Patients did not significantly differ in level-1 perspective-taking behaviour compared to healthy controls. No significant associations were found between perspective-taking, paranoia and attachment. Insecure attachment was significantly related to paranoid thoughts, after controlling for illness-related symptoms.
Conclusion:
No impairment of level-1 perspective-taking was found in adolescent patients with early psychosis compared to healthy controls. Results indicate that level-1 perspective-taking is not impaired during the early stages of psychotic illness. The association between paranoia and attachment support previous findings and provide further insight into the nature of psychotic symptoms. Understanding the role of attachment in paranoia may help patients and their care workers to gain insight into the reasons for the development or persistence of symptoms. Future research should compare early psychosis samples with more chronic samples to explore whether perspective-taking deteriorates during the course of the illness.
Introduction
Individuals who experience psychosis often have diminished social networks and difficulties in social functioning (Bellack et al., 1990; Berry et al., 2007a, 2007c). Therefore, factors underlying social functioning are an intensively studied topic. One of the factors influencing functional outcome in psychosis is social cognition, which is defined as the mental processes underlying social interactions (Couture et al., 2006; Fett et al., 2011). Associations between social cognition and outcome are particularly robust in the domain ‘theory of mind’ (ToM), the ability to understand mental states such as beliefs, emotions and intentions of self and others (Bailey and Henry, 2010; Dumontheil et al., 2010a). ToM is impaired in schizophrenia (Corcoran et al., 1995; Sprong et al., 2007; Versmissen et al., 2008) and this impairment was suggested to be trait- more than state-dependent, because impairments are apparent in remission samples, (ultra) high-risk groups (Chung et al., 2008; Green et al., 2012), first episode samples (Green et al., 2012; Inoue et al., 2006; Montreuil et al., 2010; Thompson et al., 2012) and in relatives of patients with psychosis (Achaval et al., 2010; Janssen et al., 2003).
However, suggestive of a state rather than a trait characteristic, Frith and colleagues found ToM performance in patients in remission to be comparable with that of healthy controls (Corcoran et al., 1995; Frith and Corcoran, 1996). Frith and Corcoran (1996) propose that ToM skill impairments develop as the disorder progresses. To date the exact nature and development of ToM impairment in psychosis remains unclear (Bertrand et al., 2007; Kettle et al., 2008). To unravel the nature of ToM impairment in schizophrenia, it is important to study whether these skills are already impaired during early stages of the illness.
A key component of cognitive ToM is the capacity of perspective-taking, which enables an individual to consider the viewpoint of another individual (Schiffman et al., 2004). Perspective-taking can be subdivided into two levels. Level 1 pertains to ‘visual perspective-taking’, the ability to understand which object another person with a different perspective can or cannot see. On average children develop these skills around the age of 2 years. Level 2 pertains to a higher-order process of perspective-taking, the understanding that when others view an object from a different (physical) viewpoint, they perceive this object in a different way. This skill typically develops around the age of 4 (Masangkay et al., 1974). Around the same age, children also develop ‘false belief understanding’, as mentioned above.
Level 2 perspective-taking has been studied intensively and was found to be impaired in psychosis (Sprong et al., 2007). However to our knowledge, level 1 perspective- taking skill has not been studied in psychosis and it remains unclear whether perspective-taking is impaired at this more basic cognitive level. In non-clinical populations level 1 perspective-taking has been studied with the ‘Director Task’ (Dumontheil et al., 2010a, 2010b; Keysar et al., 2000), an online communicative task. It was found that both adolescents and adults are prone to errors and that adolescents perform worse than adults (Dumontheil et al., 2010a). This is of particular interest to the study of psychosis, which is not only associated with deficits in perspective-taking, but also has its peak incidence in late adolescence (Paus et al., 2008).
The authors link their findings to the online character of the task given that level 1 is a skill that young children are already capable of and designate the transition from adolescence to adulthood as one of an increased social perspective-taking. The authors state that differences may be accounted for by the fact that ‘having’ the skill does not automatically mean usage of the skill, which is assessed with this task.
To understand underlying or associated factors of ToM impairment in psychosis, insights derived from attachment theory may be helpful (Berry et al., 2007b), as ToM and attachment theory are both based on mental representations about self and others and are therefore plausibly related. According to attachment theory, development of social interaction patterns stems from early experiences with significant others (Bowlby, 1973). An attachment style incorporates thoughts, feelings and beliefs about self and others and is activated for processing new social information. Two underlying dimensions, which can be explained in terms of models of self and others, are generally found when assessing attachment styles (Mikulincer and Shaver, 2007): (i) attachment anxiety, which refers to a positive view of others and a negative view of self, and (ii) attachment avoidance, which refers to a negative view of others and a positive view of self. These attachment styles, also referred to as insecure attachment, are related to social dysfunction, interpersonal difficulties and psychopathology in adult life (Berry et al., 2006, 2007a). When an individual has a positive view of self and others he or she has a secure attachment style.
The association between insecure attachment and mentalisation has previously been studied in a sample of patients with psychosis (MacBeth et al., 2011). Findings indicated that patients with higher levels of attachment avoidance had lower mentalisation skills than patients with an anxious or secure attachment style.
Both insecure attachment and impaired ToM have also been found to co-occur in patients with paranoia or persecutory ideas and have been proposed as possible underlying mechanisms of these symptoms (Randall et al., 2003; Sprong et al., 2007; Taylor and Kinderman, 2002). Garety et al. (2001) suggested a cognitive model of psychosis according to which paranoia is maintained by negative beliefs about others and social withdrawal, which are also characteristics of avoidant attachment. Indeed, previous research showed that individuals with paranoia or persecutory ideas tend to attribute negative outcome of events to others instead of situations (Bentall et al., 2001). Furthermore, associations between insecure attachment and paranoid symptoms have been found in a clinical sample, in which avoidant attachment was related to severity of paranoia. These associations remained significant, even after controlling for total symptom scores, implying that more avoidant attachment in paranoid patients could not be solely attributed to illness severity (Berry et al., 2008). Yet, other research with a clinical sample of 34 patients found no relation between attachment style and paranoia (MacBeth et al., 2011). The association between both insecure attachment dimensions and paranoia has also been found repeatedly in non-clinical samples (Berry et al., 2006; MacBeth et al., 2008; Meins et al., 2008; Pickering et al., 2008). Hence, a relationship between these two constructs and impaired ToM may also be expected during the early stages of psychotic illness. Green et al. (2008) identified two types of paranoia: social reference and persecution, in which the latter includes the belief that others have harmful intentions. Previous evidence indicates that persecution and avoidant attachment have a plausible relation (Berry et al., 2008). Furthermore, attachment anxiety involves worrying about social relations, which, in combination with a low self-image, could lead to making paranoid social references. We hypothesised that attachment avoidance would be more strongly associated with persecution paranoia, and that attachment anxiety would be more strongly associated with social reference paranoia in both samples.
The aim of this study was four-fold: first, comparing cognitive ToM level 1 visual perspective-taking in an adolescent sample with early onset of psychosis as compared to controls. Second, we assessed whether paranoia is related to impairments in level 1 perspective-taking. Third, we assessed whether insecure attachment (avoidant, anxiety) is related to impairments in level 1 perspective-taking. Fourth, we assessed whether paranoia is related to insecure attachment.
Methods
Participants
Inclusion criteria for patients consisted of (i) age between 13 and 18 years, (ii) a WASI vocabulary t-score ≥ 30 (Wechsler, 1999), (iii) experienced a psychotic episode according to ICD-10 criteria, as diagnosed by their clinician (World Health Organization, 1992), (iv) good command of the English language and (v) able and willing to give written informed consent. Inclusion criteria for the control group were (i) age between 13 and 18 years, (ii) a WASI vocabulary t-score ≥ 30, (iii) good command of the English language and (iv) able and willing to give written informed consent, and (v) no personal or family history of a psychotic illness. Patients were recruited via consultant psychiatrists and with the help of the Mental Health Research Network (MHRN) in the South London and Maudsley, North East London and South Essex Partnership University NHS Foundation Trust. Control participants were recruited from schools, the Institute of Psychiatry volunteer database ‘Mindsearch’, via colleagues and previous participants. Informed consent was obtained from all adolescents and their parents/guardians if they were under the age of 16. The study was approved by the Surrey Borders Research Ethics Committee.
Instruments
Attachment
To assess attachment dimensions the Psychosis Attachment Measure (PAM) (Berry et al., 2006) was used. A 16-item questionnaire referring to thoughts, feelings and behaviours, rated on a four-point answer scale with 0 ‘not at all’ and 3 ‘very much’. Eight items reflected avoidant attachment and the other eight reflected anxious attachment. Average item scores were calculated for attachment anxiety and avoidance, with higher scores reflecting higher levels of insecure attachment. Previous research has shown the PAM to have good reliability and validity in clinical and non-clinical samples (Berry et al., 2006, 2008).
Theory of mind: Perspective-taking task
The perspective- taking task (PTT) is a computer simulation designed by Dumontheil et al. (2010b) and based on the Keysar task (Keysar et al., 2000). The stimuli consist of 16 slot shelves, eight of which contained different objects. The task has a Director and a No-Director condition. In the first, a director standing on the opposite side of the shelves instructed the participant to move certain objects into different slots. Five slots were visible to the participant, but occluded from the director’s perspective. In experimental trials, the correct response was to select the best fitting object that was also visible to the director and to ignore a distracting object, which also fulfilled the director’s instruction but was invisible to him (see Figure 1(a) and (b)). Instructions in filler trials referred to objects that were visible to the director and the participant. The order of trial types (control (n = 8); experimental (n = 8); filler (n = 48)) was counterbalanced. The possible error range in experimental and control trials was 0 to 8. In the No-Director condition, participants were instructed to ignore objects in slots with a grey background and no director was present in the background of the picture (Figure 2(a) and (b)). Thus, both Director and No-Director conditions required participants to inhibit the pre-potent response of moving the object that best fits the instruction from their point of view. The crucial difference between conditions was that, in the Director condition, participants were instructed to take into account which objects the Director could and could not see, whereas in the No-Director condition, they were instructed to take into account the colour of the slot the object was in. Hence, the only difference between conditions was that the Director condition involved the interaction between ToM (taking into account the director’s perspective) and executive functions (inhibiting the egocentric bias).
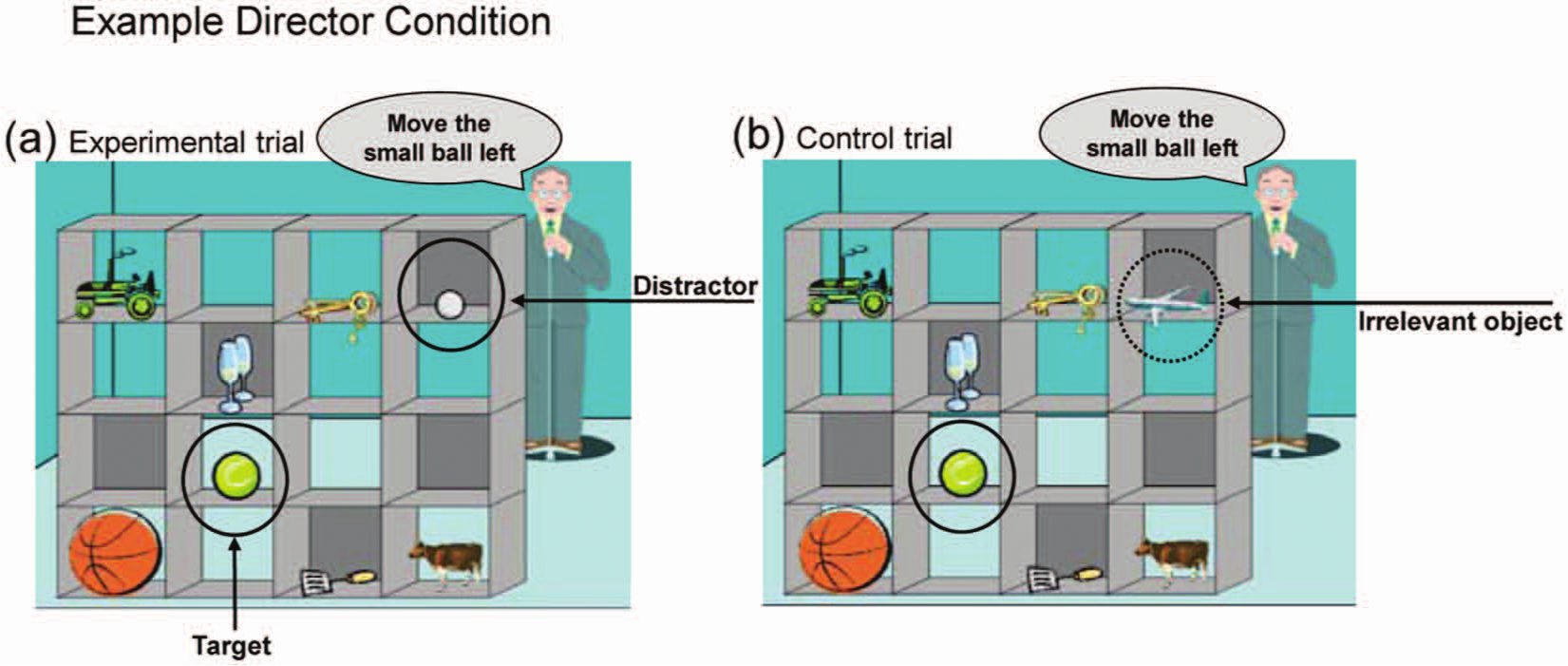
Director condition.
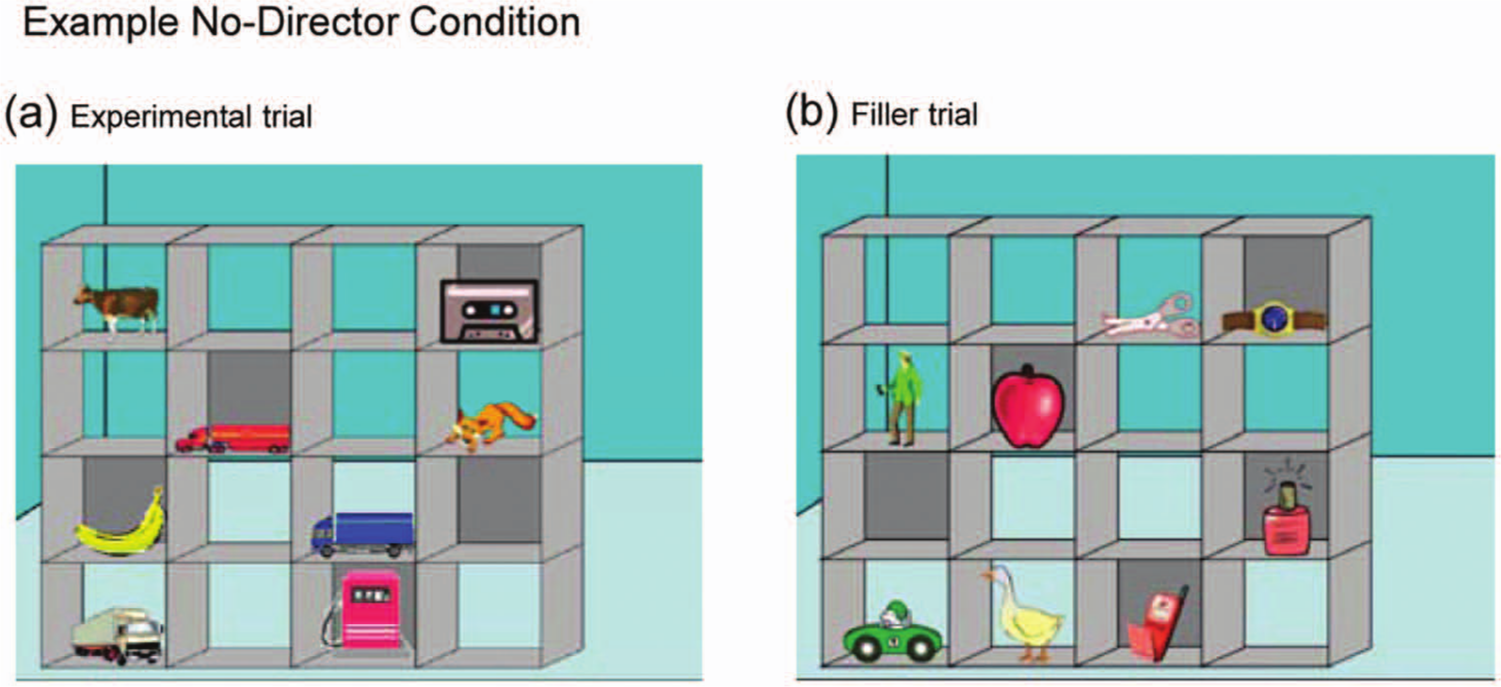
No-Director condition.
Two sets of shelf–object configurations were used and stimuli were not repeated for individual subjects. Each presented set was shown once with an occluded distracter object (experimental trial) and once with an irrelevant object (control trial). Sets were counterbalanced across subjects. See Dumontheil et al. (2010b) for a more detailed description of the PTT.
Clinical assessments
The Positive and Negative Syndrome Scale (PANSS) (Kay et al., 1987) was used to assess symptom severity in patients over the last week. For the present study, positive and negative syndrome scales were calculated according to the five-factor model (van der Gaag et al., 2006a, 2006b).
The Community Assessment of Psychic Experiences (CAPE) (Stefanis et al., 2002) was used to assess the frequency of psychotic-like experiences (PLEs) in both patients and controls. This 42-item lifetime questionnaire assesses positive, negative and depressive symptoms. For the present study only the positive and negative PLEs frequency scale was used. Overall scores range from 0 to 3, with a higher score reflecting a higher frequency of PLEs.
The Green Paranoid Thoughts Scale (GPTS) (Green et al., 2008) consists of two subscales on ‘social reference’ and ‘persecution’ paranoia and was administered to both patients and controls. The GPTS indicates the level of paranoid thoughts in the previous 4 weeks. Both subscales consist of 16 items, with answer scales ranging from 1 (‘not at all’) to 5 (‘totally’). Total scores range from 16 to 80 per subscale. Higher scores indicate higher levels of paranoid thinking. The scale has shown good internal consistency and test–retest reliability in clinical and non-clinical samples.
Neuropsychological assessments
The vocabulary subtest of the Wechsler Abbreviated Scale of Intelligence (WASI) was used as an indicator of general cognitive ability (Wechsler, 1999).
Procedure
All participants/primary care-givers read the information material and gave written informed consent before the testing procedure. Participants were tested individually in a quiet room at the Institute of Psychiatry. They were given standardised instructions for the PTT and an example stimulus of each condition was shown. It was explained that the director would tell them which object to move and where to move it and that he had a different perspective from their own, which was illustrated with an image of the director’s view of the shelves. To check whether participants understood the instructions they were asked to indicate an object that the director could not see and one that the director could see. This was meant to assess whether the participants understood that the director had a different perspective. The PTT started once instructions were understood. There were four practice trials before the Director condition. New instructions and an example stimulus were given to the participants before the No-Director condition. Again, they were asked to demonstrate what was required of them. After the PTT, the participants were assessed on the WASI vocabulary subtest, the PANSS, GPTS, CAPE and PAM.
Data analyses
Differences between the patient and control groups in social demographics, frequency of PLEs, perspective-taking errors in the Director condition and equivalent errors in the No-Director condition, attachment style and social reference paranoia and persecutory ideas were assessed with independent t-tests. The overall number of errors was calculated for each participant by condition (Director/No-Director) and trial type (Control/Experimental). The number of perspective-taking errors in the Director condition and equivalent errors in the No-Director condition was computed for the experimental trials within each condition. (i) A paired t-test was used to assess differences in perspective-taking errors in the Director condition and their equivalents in the No-Director condition. (ii) Regression analyses with group status (patient/control), age, gender and estimated cognitive ability (vocabulary t-score) as independent variables were performed on perspective-taking errors in the Director and equivalent errors in the No-Director condition as dependent variables. (iii) To assess that executive functioning would not account for possible group differences in the Director condition, we subtracted the scores of the No-Director condition from the Director condition and used this difference score as the dependent variable in a multiple regression analysis with group status (patient/ control), age, gender and estimated cognitive ability (vocabulary t-score) as independent variables. (iv) Pearson correlations were used to assess associations between the GPTS and the attachment scale scores; partial correlations were conducted to adjust these relations for the level of positive and negative PLEs, as assessed with the CAPE in both groups. (v) Finally, hierarchical multiple regression analyses were used to assess whether insecure attachment was related to the presence of paranoid thoughts and perspective-taking errors. All analyses were performed with SPSS version 18.
Results
Participant characteristics
Means and standard deviations of demographics, WASI, PAM, CAPE, GPTS and perspective-taking errors of patients and controls are presented in Table 1. A total of 32 patients who experienced a psychotic episode were included with the following diagnoses: eight schizophrenia; five acute and transient psychotic disorders; three schizoaffective disorder; six unspecified or other non-organic psychosis; five bipolar affective disorder with psychotic symptoms; two depressive disorder with psychotic symptoms; one mania with psychotic symptoms and two pervasive developmental disorder with psychotic symptoms. All but one patient took antipsychotic medication. Patients had a mean PANSS score on the positive subscale, according to the five-factor model (van der Gaag et al., 2006a, 2006b), of 13.3 (SD = 7.9) and 13.6 (SD = 8.3) on the negative subscale. Patients were significantly older than controls, t(109) = −2.4, p = 0.017. Compared to controls, patients scored significantly higher on the CAPE positive scale (frequency), t(104) = −3.9, p < 0.0001, as well as on the negative scale, t(104) = −2.8, p = 0.009. Also, patients reported higher levels of social reference paranoia t(109) = −2.4, p = 0.019 and persecution paranoia, t(109) = −2.2, p = 0.033. Finally, patients reported higher levels of attachment anxiety, t(104) = −3.9, p < 0.0001. Controls scored significantly higher than patients on the WASI vocabulary, t(108) = 3.7, p < 0.0001.
Means and standard deviations of demographics, WASI, PAM, CAPE, GPTS and perspective-taking errors of patients and controls.
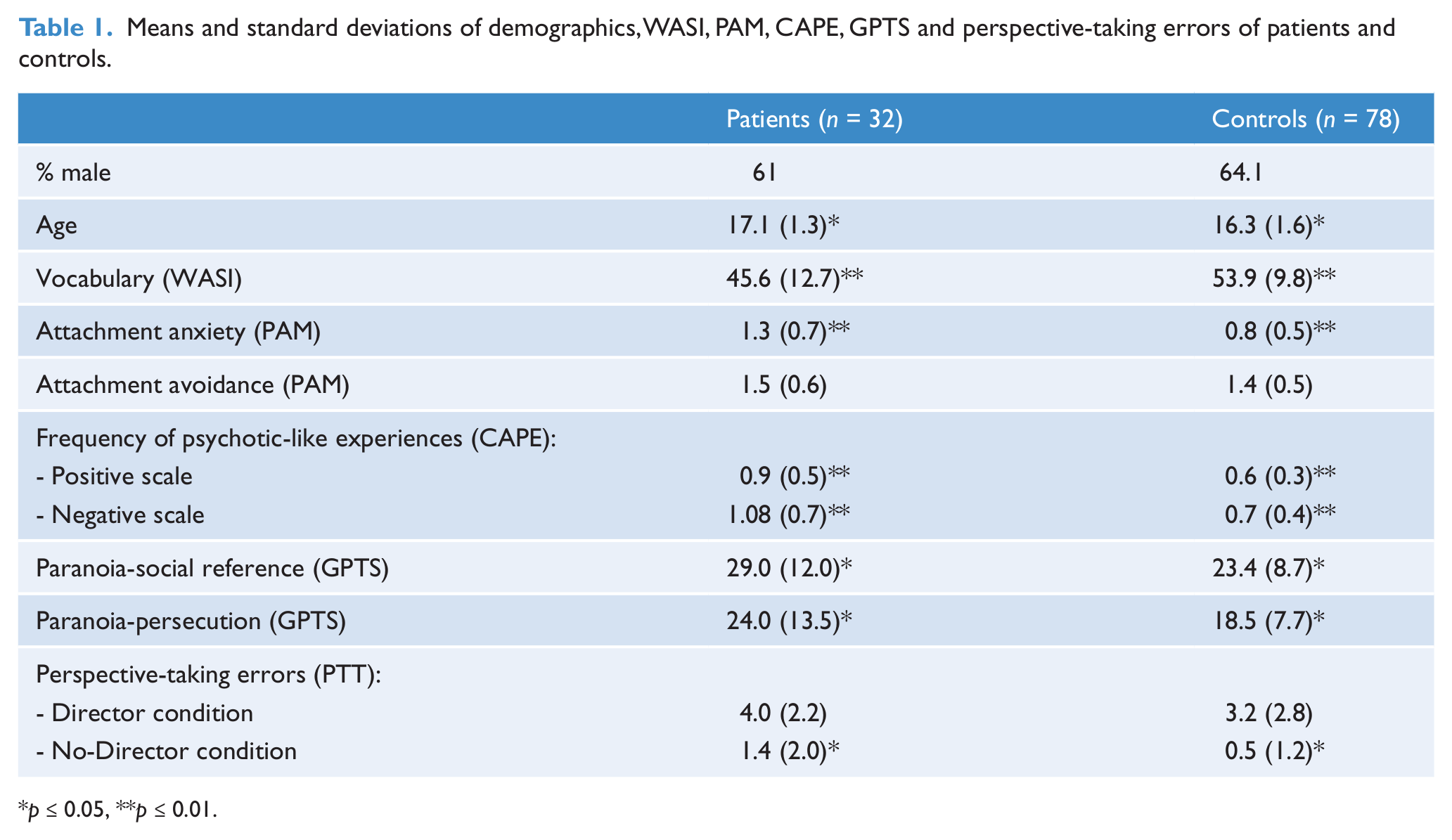
p ≤ 0.05, **p ≤ 0.01.
Perspective-taking task
Both groups made significantly more errors in the Director condition compared to the No-Director condition, patients: t(31) = 5.4, p < 0.0001, controls: t(77) = 8.0, p < 0.0001.
A regression analysis with group status (patient/control), age, gender and vocabulary t-score as independent variables showed that the number of errors (No-Director condition) was significantly related to group status (β = −0.90, p = 0.01) with patients making more errors than controls.
In the Director condition the difference between patients and controls was not statistically significant (t(108) = −1.6, p = 0.12). A regression analysis with group status (patient/control), age, gender and vocabulary as independent variables showed that the number of perspective-taking errors (Director condition) was related to WASI vocabulary score only (β = −0.06, p = 0.03).
A regression analysis with group status (patient/control), age, gender and vocabulary as independent variables showed that there was no group difference (β = 0.68, p = 0.31) in perspective-taking when controlled for executive functioning (No-Director minus Director). Also age (β = −0.24, p = 0.19), gender (β = 0.46, p = 0.42) and WASI scores (β = 0.04, p = 0.19) had no effect.
No associations were found between the number of perspective-taking errors in the Director condition and the attachment dimensions, PLEs or paranoid thoughts in the patient or control group (p-values > 0.29).
Attachment and social reference paranoia
Correlations between attachment (PAM) and paranoia scales (GPTS), controlling for positive and negative symptom scales (CAPE), are presented in Table 2. Attachment anxiety was associated with ideas of social reference in both groups, even after controlling for the frequency of positive and negative symptoms as assessed with the CAPE. Attachment avoidance was associated with ideas of social reference in the patient group; however this association was no longer significant after controlling for frequency of symptoms as indicated by the CAPE.
Correlations between PAM and GPTS scales, controlling for positive and negative CAPE scales.
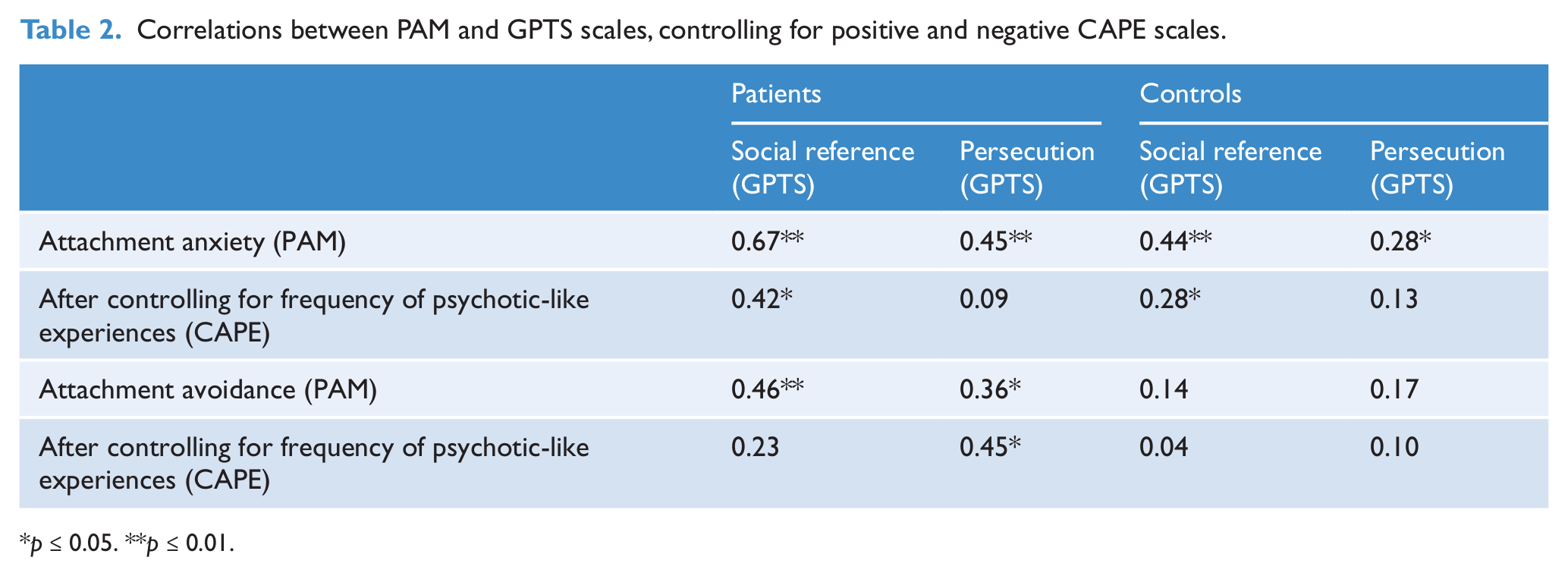
p ≤ 0.05. **p ≤ 0.01.
5. Hierarchical multiple regression analyses with group status (patient/control), age, vocabulary and positive and negative PLEs (frequency) entered in step 1, explained 37.9% of the variance in social reference paranoia. Adding attachment anxiety as well as group status by attachment anxiety interaction in step 2, resulted in an additional 6.6% explained variance (explained variance of the total model: 44.4%). Age (β = −0.2, p = 0.042), positive PLEs (frequency) (β = 0.3, p = 0.002) and attachment anxiety (β = 0.3, p = 0.013) each had a unique contribution to the final model.
Attachment and persecution ideas
Attachment anxiety was associated with persecution in both groups but this association was no longer significant after controlling for frequency of negative and positive PLEs. Attachment avoidance was significantly correlated to persecution only in the patient group; this association remained significant after controlling for the frequency of PLEs. Hierarchical multiple regression analyses with group status (patient/control), age, vocabulary and positive and negative PLEs entered in step 1, explained 34.3% of the variance in persecution paranoia. Adding attachment avoidance and group status by attachment avoidance interaction in step 2 explained an additional 6.4% of the variance, resulting in 40.7% explained variance for the final model. In the final model the interaction between group status and avoidance (β =0.7, p = 0.032) and positive PLEs (frequency) (β = 0.5, p < 0.0001) had a unique contribution.
Discussion
The aim of this paper was to investigate whether ToM, as assessed by a level 1 perspective-taking task, is impaired in adolescent patients with early psychosis as compared to controls, and how this impairment relates to attachment style and paranoia.
Perspective-taking and psychosis
To investigate whether the use of ToM is already impaired at level 1 visual perspective-taking in adolescent patients with early psychosis compared to controls we studied the differences between two experimental conditions of the PTT (i.e. the Director and the No-Director condition), in which significant differences imply reduced perspective-taking. Both patients and controls made perspective-taking errors that were not due to problems in executive functioning or inhibition. Surprisingly, although differences were in the expected direction (i.e. patients made more errors than controls), results were not statistically significant in the Director condition. This could be due to power problems, as a calculated effect size indicated a medium effect (Cohen’s d = 0.30). Nevertheless, patients with early psychosis do not seem to have severe impairments in the use of level 1 perspective-taking. Several explanations may account for the current findings. Firstly, the psychotic disorder in the early psychosis patients may not have progressed enough to impair perspective-taking. Studies in adult samples with more progressed psychosis, using a visual perspective-taking task in non-social settings did find impairments in perspective-taking (Langdon and Coltheart, 2001).
Secondly, the construct of ToM can be divided into two components. Affective ToM includes emotional empathic abilities which are needed to understand the mindset of another person, as for example required during the understanding of indirect speech. Second, there is cognitive ToM, i.e. the understanding that another person may have different beliefs about the same object, as required for the solution of ‘false belief understanding’ tasks, defined as the ability to comprehend that others’ beliefs may differ from one’s own beliefs or reality. Both components may be differentially impaired in psychosis; therefore studying both cognitive and affective ToM components may help better understand the role of specific ToM impairment in psychosis (Shamay-Tsoory et al., 2007). It has been suggested that ToM impairment in schizophrenia is specific to affective ToM. The current findings are in line with the idea that impairment may occur during the development of affective ToM rather than cognitive ToM. Thus, it is possible that level 1 perspective-taking is and (perhaps stays) unimpaired in psychosis. Alternatively, the discrepancy in the previously discussed findings could be due to the fact that the Director task requires the use of ToM, which still develops at the end of adolescence during the transition into adulthood (Dumontheil et al., 2010a). Hence, it might be possible that impairments in patients occur during this transitional stage, rather than in adolescence itself.
Furthermore, it could be possible that deficits in cognitive ToM are more specific or pronounced in non-affective than affective psychosis (Marjoram et al., 2005). Thus, the heterogeneity in the current sample could account for the fact that controls and patients didn’t differ in perspective-taking. To assess whether the heterogeneity of the diagnoses in a patient sample could be an explanation for the absence of group differences in perspective-taking, we compared the perspective-taking tendency of controls, the group of individuals with affective and the group of individuals with non-affective psychoses. The analysis did not show a significant difference between the three groups (p = 0.46). In the current sample patients with affective and non-affective psychosis had a similar ToM performance. However this may be due to the moderate sample size. It would be valuable for future research to investigate perspective-taking within larger groups of patients with affective and non-affective psychosis.
Perspective-taking, paranoia and attachment
Contrary to our expectations we did not find associations between perspective-taking errors and paranoid thoughts. This may be due to the fact that in our sample use of this specific aspect of ToM was not impaired (enough) or not yet impaired. Also, even though Bentall and colleagues found both an affective and a cognitive component, paranoia may be more associated with affective ToM rather than cognitive ToM, because emotion-related processes are associated with paranoid beliefs (Bentall et al., 2009). In addition, we did not find associations between the number of perspective-taking errors and attachment. This is in contrast with previous studies that reported a relation in clinical (MacBeth et al., 2011) and non-clinical adolescent samples (Humfress et al., 2002). The absence of a significant association could be explained by the fact that the Director task measures a more cognitive component of ToM, while attachment may rather be associated with the emotional component of ToM, in which emotions, thoughts, beliefs and intentions of self and others play a role. In contrast to the current study, previous studies focused more on emotional ToM (MacBeth et al., 2011). More research on ToM and its separate cognitive and emotional components is needed to investigate this association with attachment in samples with early psychosis.
Attachment and paranoia
Patients reported higher levels of attachment anxiety than controls and associations between attachment anxiety and both paranoid thought scales were found both in patients and in controls. These associations were controlled for positive and negative PLEs, suggesting that the associations are not confounded by (sub) clinical symptoms. Attachment anxiety had a unique contribution to social reference paranoia. Avoidant attachment was also related to ideas of social reference, but only in the patient group. Individuals with high levels of attachment anxiety tend to have a strong desire for closeness and a need to feel loved, combined with intense worry about whether others are available (Berry et al., 2007a, 2007b, 2009; Howe, 2011; Mikulincer and Shaver, 2007). It is possible that high levels of attachment anxiety can lead individuals to perceive social situations as threatening, which in combination with the typically negative view of the self may lead to paranoid social references.
Avoidant attachment was associated with persecutory ideas in the patient group, even after controlling for positive and negative PLEs, and explained a unique part of the variance. This confirms previous findings of associations between attachment avoidance and paranoia (Berry et al., 2008).
Concluding remarks
Our study has limitations: firstly the patient sample was small, which could have led to power problems, and the sample was heterogeneous with respect to clinical diagnosis. Secondly, the PAM was developed for adults and not validated in adolescents. However, because this attachment measure was developed to be easy to administer, has simple answer scales and only positively worded items, this is not likely to have affected the results. Finally, the cross- sectional design precludes evaluation of development of ToM abilities during the course of psychotic disorders. More research needs to compare early episode samples with more chronic samples (or even better, longitudinal study of ultra-high risk subjects) to investigate whether perspective-taking impairs during the course of the illness. Future research should include ToM tasks that target affective and more cognitive aspects, respectively, and include measures of attributional style in their investigation of the relationship with different attachment styles and paranoia early in psychosis, specifically the association between avoidant attachment and attributional style and their interaction with regard to paranoia.
Footnotes
Acknowledgements
We would like to thank Professor Sarah-Jayne Blakemore for providing the perspective-taking task. Also, we would like to thank all our participants and Mirjam van Driel for her help with this study.
Funding
This work was supported by a VIDI grant from The Netherlands Organization for Scientific Research (grant number MAGW 452-07-007) to Prof. Lydia Krabbendam and a Medical Research Council new investigator award (grant number 93641) to Dr. Sukhi S Shergill.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.