
Abstract
Objective:
Past traumatic events have been associated with poorer clinical outcomes in people with bipolar disorder. However, the impact of these events in the early stages of the illness remains unclear. The aim of this study was to investigate whether prior traumatic events were related to poorer outcomes 12 months following a first episode of psychotic mania.
Methods:
Traumatic events were retrospectively evaluated from patient files in a sample of 65 participants who had experienced first episode psychotic mania. Participants were aged between 15 and 28 years and were treated at a specialised early psychosis service. Clinical outcomes were measured by a variety of symptomatic and functioning scales at the 12-month time-point.
Results:
Direct-personal traumatic experiences prior to the onset of psychotic mania were reported by 48% of the sample. Participants with past direct-personal trauma had significantly higher symptoms of mania (p=0.02), depression (p=0.03) and psychopathology (p=0.01) 12 months following their first episode compared to participants without past direct-personal trauma, with medium to large effects observed. After adjusting for baseline scores, differences in global functioning (as measured by the Global Assessment of Functioning scale) were non-significant (p=0.05); however, participants with past direct-personal trauma had significantly poorer social and occupational functioning (p=0.04) at the 12-month assessment with medium effect.
Conclusions:
Past direct-personal trauma may predict poorer symptomatic and functional outcomes after first episode psychotic mania. Limitations include that the findings represent individuals treated at a specialist early intervention centre for youth and the retrospective assessment of traumatic events may have been underestimated.
Introduction
Modern theories of bipolar affective disorder (BPAD ) consider the biopsychosocial precipitants of the illness. Environmental stressors (specifically exposure to trauma) have been shown to affect the clinical presentation of BPAD (Post et al., 2003). According to the criteria for post-traumatic stress disorder (PTSD) in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR), a traumatic event can be defined as an individual’s experience of psychological, emotional or physical distress, resulting from exposure to an event that has been or was perceived as threatening to one’s existence, safety, stability or well-being (American Psychiatric Association, 2000). The diagnostic criteria for PTSD include threats to one’s physical integrity. However, for the purpose of this study, the definition has been expanded to include emotional traumas, as research has shown that repeated non-physically threatening experiences such as emotional abuse and neglect could potentially cause more psychological harm than a single disastrous event (Seides, 2010; Spertus et al., 2003). While the effects of past traumatic events on the course and outcome of this disorder are not yet fully understood, in recent years evidence has indicated that there is a significant association between trauma and a poorer overall prognosis for BPAD (Garno et al., 2005; Kessing et al., 2004; Neria et al., 2005). With the recent emphasis on staging models of BPAD (Berk et al., 2007), there is a clear need to investigate the impact of trauma on individuals across the trajectory of their illness. However, even with well-documented models such as the Kindling/Sensitization model (Post et al., 1986) on the effect of environmental stressors on outcomes of BPAD, more research on prior trauma in the first episode psychotic mania cohort is required (Conus et al., 2010; Cotton et al., 2013), particularly in regards to the resultant impact on psychosocial and occupational functioning.
Individuals with BPAD report a higher rate of childhood trauma than either the general population or individuals with unipolar depression (Hyun et al., 2000), such that as many as 50% of people with BPAD have experienced severe childhood abuse (Garno et al., 2005; Leboyer et al., 2007; Leverich et al., 2002). Moreover, Garno et al. (2005) found that 37% of their cohort of 100 people with BPAD reported emotional abuse, 24% experienced emotional neglect, 24% had been a victim of physical abuse, 21% disclosed past sexual abuse, and 12% had experienced physical neglect; with approximately one-third having reported multiple traumas.
With high incidences of trauma reported by people with BPAD (Maguire et al., 2008; Savitz et al., 2008), there has been increased interest into whether these experiences impact the prognosis of BPAD. Researchers have identified that people with a history of trauma have presented with a poorer clinical manifestation of the illness compared to those without such traumas, including: an earlier age of illness onset (Etain et al., 2013; Garno et al., 2005); a higher number of depressive episodes (Brown et al., 2005; Etain et al., 2013); rapid cycling (Etain et al., 2013; Garno et al., 2005; Leverich and Post, 2006); increased severity of current manic symptoms (Garno et al., 2005); more severe psychotic symptoms (Hammersley et al., 2003; Romero et al., 2009); suicide attempts (Brown et al., 2005; Etain et al., 2013; Garno et al., 2005; Leverich and Post, 2006); and an increased likelihood of having comorbid disorders such as PTSD (Brown et al., 2005; Romero et al., 2009), substance abuse (Brown et al., 2005; Garno et al., 2005; Leverich and Post, 2006) and panic disorder (Brown et al., 2005). Trauma may also have a greater impact on the outcomes of females with BPAD than males (Cotton et al. 2013; Etain et al., 2013).
Furthermore, past direct-personal trauma (DPT) defined for the purpose of this study as traumatic events that were directly and personally experienced by the participants, has been linked to poorer outcomes for people with BPAD. For example, Leverich et al. (2002) found that early sexual and physical abuse were related to an earlier onset of illness, rapid cycling, suicidality and an increased likelihood of Axis I (psychiatric), II (personality) and III disorders (medical conditions) over a lifetime in people with BPAD types I and II (BPAD-I and II). In addition, in a cohort of first episode psychotic mania patients, it was found that past sexual and/or physical abuse was associated with a higher likelihood of having a forensic history, poorer premorbid functioning, reduced engagement in treatment, and a decreased likelihood of living with immediate family whilst being treated (Conus et al., 2010).
A systematic review by Daruy-Filho et al. (2011) on the effect of abuse and neglect during childhood provides further evidence of the impact of past DPT in BPAD. The authors found that childhood abuse and neglect were strongly related to an earlier onset of illness, suicidality and comorbid substance abuse in people with BPAD. Childhood physical abuse was the strongest predictor of poorer outcomes in BPAD; however, the review indicated that there has been little research on the impact of emotional abuse and neglect in people with this disorder. Of the few studies that had investigated this relationship, severe emotional abuse during childhood was found to be associated with comorbid lifetime substance abuse and rapid cycling (Garno et al., 2005). Further, emotional abuse and neglect predicted trait aggression in BPAD (Garno et al., 2008). Moreover, Etain et al. (2010) found that childhood emotional abuse occurred more frequently in people with BPAD compared to healthy controls, whilst a recent study by Watson et al. (2013) found, after controlling for age and sex, that emotional neglect was the only childhood trauma that was associated with a diagnosis of BPAD.
While these findings provide considerable support that early traumatic experiences significantly impact the course of BPAD, few studies have researched the effects of past trauma during the early stages of the illness – a crucial time for early intervention (Berk et al., 2010). Most studies have focused on patients with more established or chronic forms of the illness, which potentially leads to confounding variables such as the possibility of more exposure to different stressors over time and medication effects compared to a first episode cohort. Furthermore, few studies have investigated the effects of traumatic experiences in psychotic mania, with most studies including participants across a broader bipolar spectrum (Brown et al., 2005; Kauer-Sant’Anna et al., 2007; Leverich et al., 2002; Maguire et al., 2008; Savitz et al., 2008). Finally, many studies have been limited by their focus on specific types of traumatic exposures (Garno et al., 2005; Kessing et al., 2004; Neria et al., 2005).
The aim of this study was to investigate whether past DPT was related to clinical variations in the symptomatic and functional outcomes of young people who had experienced a first episode of psychotic mania. Symptomatic and functional outcomes were measured at the 12-month time-point to allow for the initiation of treatment and acute episode remission. It was hypothesised that the participants with past DPT would have poorer symptomatic recovery 12 months following their first treated episode of psychotic mania compared to participants without past DPT. It was also hypothesised that the individuals with a history of DPT would have worse psychosocial and occupational functioning 12 months after their first treated psychotic manic episode compared to individuals without these prior traumatic experiences.
Methods
Sample and setting
This is a study based on the prospective follow-up of a cohort of 86 participants involved in a larger 18-month randomised controlled trial (RCT) study, conducted at the Orygen Youth Health Research Centre (OYHRC) between the years 2001 and 2006. This RCT study compared the effect of chlorpromazine and olanzapine combined to lithium in the treatment of first episode mania with psychotic features; the details and methodology are currently in submission (Conus et al., 2014: in submission). Of the 86 participants, three refused to allow their data to be used for other research purposes, two did not complete the Structured Clinical Interview (SCID-I/P) for the DSM-IV-TR to confirm a diagnosis of either bipolar I disorder or schizoaffective disorder, seven had withdrawn or were lost to follow-up consent to the previous study, one was deceased and eight received diagnoses other than bipolar I disorder or schizoaffective disorder. A total of 65 participants in the current study had originally given informed, voluntary, written consent that data collected in the RCT study could be used for research purposes, including permitted access for researchers to obtain their clinical medical and research files. OYHRC is part of the University of Melbourne, based at the Orygen Youth Health (OYH) site, Melbourne, Australia. All participants were from the western and north western regions of Melbourne. The inclusion criteria were met if participants were: (1) aged between 15 and 29 years; (2) had a minimum score of 20 on the Young Mania Rating Scale (Young et al., 1978); and (3) fulfilled criteria for a DSM-IV-TR diagnosis of BPAD-I or schizoaffective disorder. The exclusion criteria included: risk of harm to self or others as determined by case managers and self-report; the use of mood stabilisers or neuroleptics in the 2 months preceding admission; intellectual disability; significant medical illness; pregnancy or lactation in females; any medication allergies or hypersensitivity; and non-fluency in the English language.
Measures
In order to confirm diagnosis, the SCID-I/P for DSM-IV-TR was utilised (First et al., 2002). Symptoms were assessed with the following tools: Brief Psychiatric Rating Scale, version 4 (Overall and Gorham, 1988); Montgomery–Åsberg Depression Rating Scale (Montgomery and Åsberg, 1979); and the Young Mania Rating Scale (Young et al., 1978). Psychosocial and occupational functioning were evaluated using the Global Assessment of Functioning (GAF) and Social and Occupational Functioning Assessment Scales (SOFAS) (American Psychiatric Association, 2000).
Procedure for the assessment of exposure to trauma
All participants in the study were involved in extensive treatment at the early intervention programs provided at OYH-Clinical Program (OYH-CP). The identification of past exposure to traumatic events in either childhood or early adulthood was based on two strategies. First, exposure to traumatic experiences before treatment is routinely assessed by program case managers and treating doctors at OYH-CP and reported in clinical medical files. The investigators received ethical approval to retrospectively review these files. Traumatic events were identified and coded utilising a specific audit tool. The audit tool was used for consistency in extracting and analysing the self-reported traumatic events experienced by the participants. The audit tool divided DPT types into the following categories: sexual abuse/assault, physical abuse/assault, and emotional abuse/neglect. The presence of a traumatic experience was considered as valid if it fulfilled the definition of trauma in the DSM-IV-TR (American Psychiatric Association, 2000) and if participants perceived their safety or well-being was threatened, including emotional traumas. Second, clinical research files from OYHRC were also utilised to identify traumatic events documented in the SCID-I/P. Data from both sources were analysed in depth and any inconsistency in the traumatic events reported between the two files were discussed with the participants’ case managers to gain collaborative evidence of the experience reported. The traumatic events extracted from the participants’ clinical medical and research files were performed by a trained researcher (R.D.) and then cross-checked by an experienced clinician (K.T.H.). Demographic, baseline and 12-month outcome measures were obtained from the clinical research files.
Data analysis
Statistical analyses of data collected were conducted using the IBM® SPSS® Statistics 21 (IBM Corp., Armonk, NY, USA). Descriptive statistics of the prevalence of DPT (sexual abuse/assault, physical abuse/assault and emotional abuse/neglect) in the sample were calculated. Participants were divided into two groups according to the presence (group 1: DPT) or the absence (group 2: nDPT) of past exposure to DPT. Group mean differences and effect sizes (partial eta squared or partial η2) for continuous, dependent variables (symptomatic and functional scale scores) were analysed by a series of two-way analyses of covariance (ANCOVA), with alpha set at 0.05. The independent variables were trauma history and randomised medication, with scores of the respective baseline symptomatic and functioning scales included as covariates to control for individual differences. The dependent variables for each ANCOVA were scores on the symptomatic and functioning scales at the month-12 follow-up. Chi-squared tests (χ2) were performed to evaluate if significant differences existed between non-parametric variables such as sex, age, education level, primary diagnosis, comorbid anxiety and substance abuse diagnoses, suicide attempts and traumatic events.
Results
The participants were aged between 15 and 28 years (M=21.60, SD=2.92) and there were 44 males and 21 females. Fifty-five participants had an index diagnosis of BPAD-I and 10 had an index diagnosis of schizoaffective disorder. Past DPT was identified in 48% (n=31) of the sample, with 52% (n=34) having no history of DPT. The most prevalent trauma experienced was emotional neglect (20%; n=13), which was followed by emotional abuse (14%; n=9). Past physical abuse had occurred in 12% (n=8) of the participants, and 9% (n=6) had disclosed at least one incidence of physical assault. Past sexual abuse was reported by 8% (n=5) of the sample and 6% (n=4) had reported past sexual assault.
Associations with DPT
The trauma groups did not differ significantly with respect to age, sex, education level, country of birth, primary diagnosis, comorbid anxiety disorder, comorbid substance abuse or previous suicide attempts (Table 1). However, participants with DPT were more likely to have been depressed at baseline than those without DPT and the participants randomised to chlorpromazine were significantly more likely to have experienced past DPT than those randomised to olanzapine (p=0.03). Therefore, when analysing the results for differences in outcomes at 12 months, baseline symptomatic scores and the confounding variable of randomised medication were taken into account.
Demographic, diagnostic, medication, clinical and other factors associated with DPT.
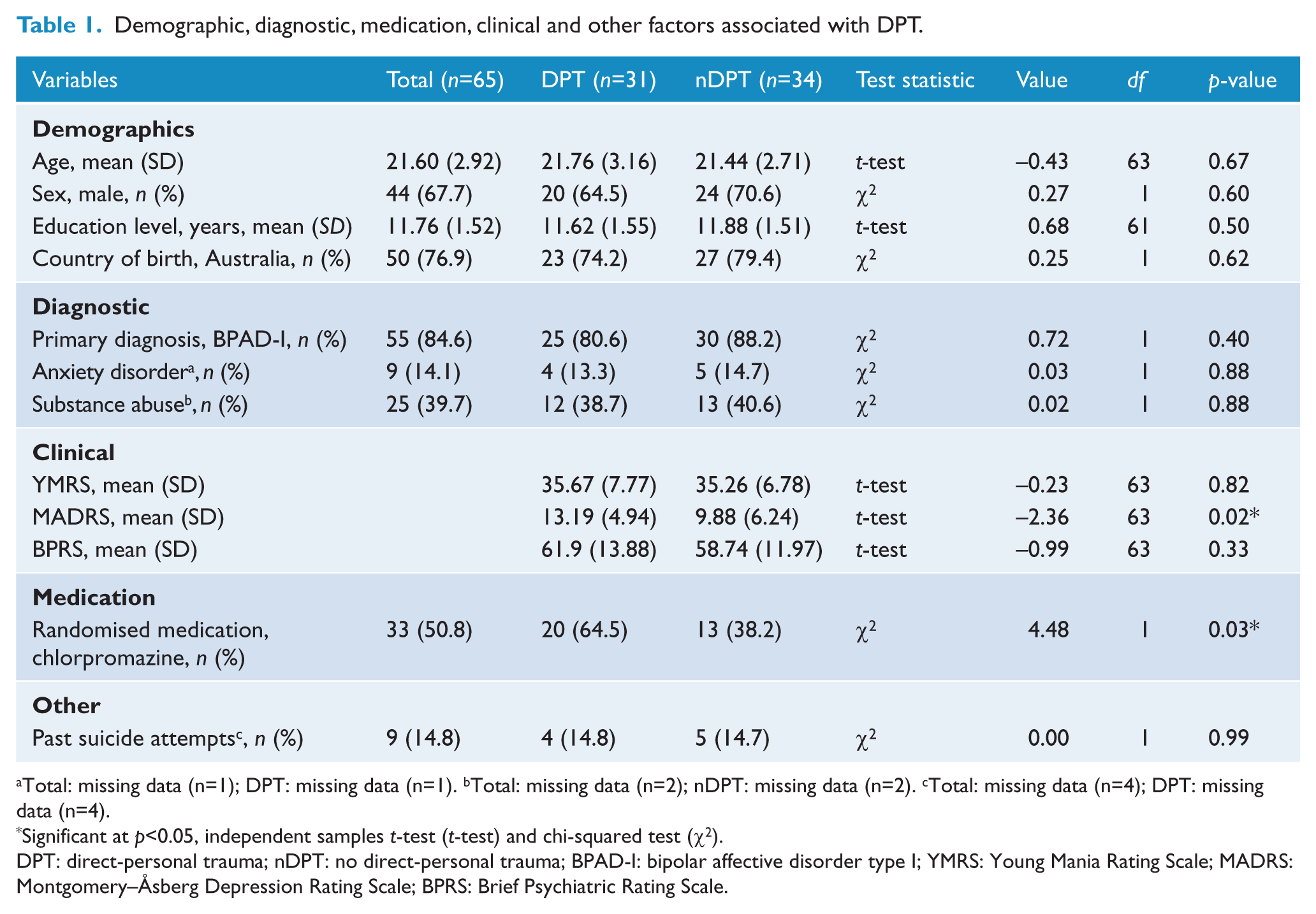
Total: missing data (n=1); DPT: missing data (n=1). bTotal: missing data (n=2); nDPT: missing data (n=2). cTotal: missing data (n=4); DPT: missing data (n=4).
Significant at p<0.05, independent samples t-test (t-test) and chi-squared test (χ2).
DPT: direct-personal trauma; nDPT: no direct-personal trauma; BPAD-I: bipolar affective disorder type I; YMRS: Young Mania Rating Scale; MADRS: Montgomery–Åsberg Depression Rating Scale; BPRS: Brief Psychiatric Rating Scale.
Mania rating outcomes
On average, participants in the DPT group expressed more manic symptoms than participants in the nDPT group (Table 2). The differences in the YMRS scores between trauma groups were significant (p=0.02), with a medium effect size (ηp2=0.11) being observed (Cohen, 1988). There was no main effect in the interaction between trauma history and randomised medication at the 12-month time-point (p=0.75).
Bipolar symptomatology and functional outcome between groups at month-12 assessment.
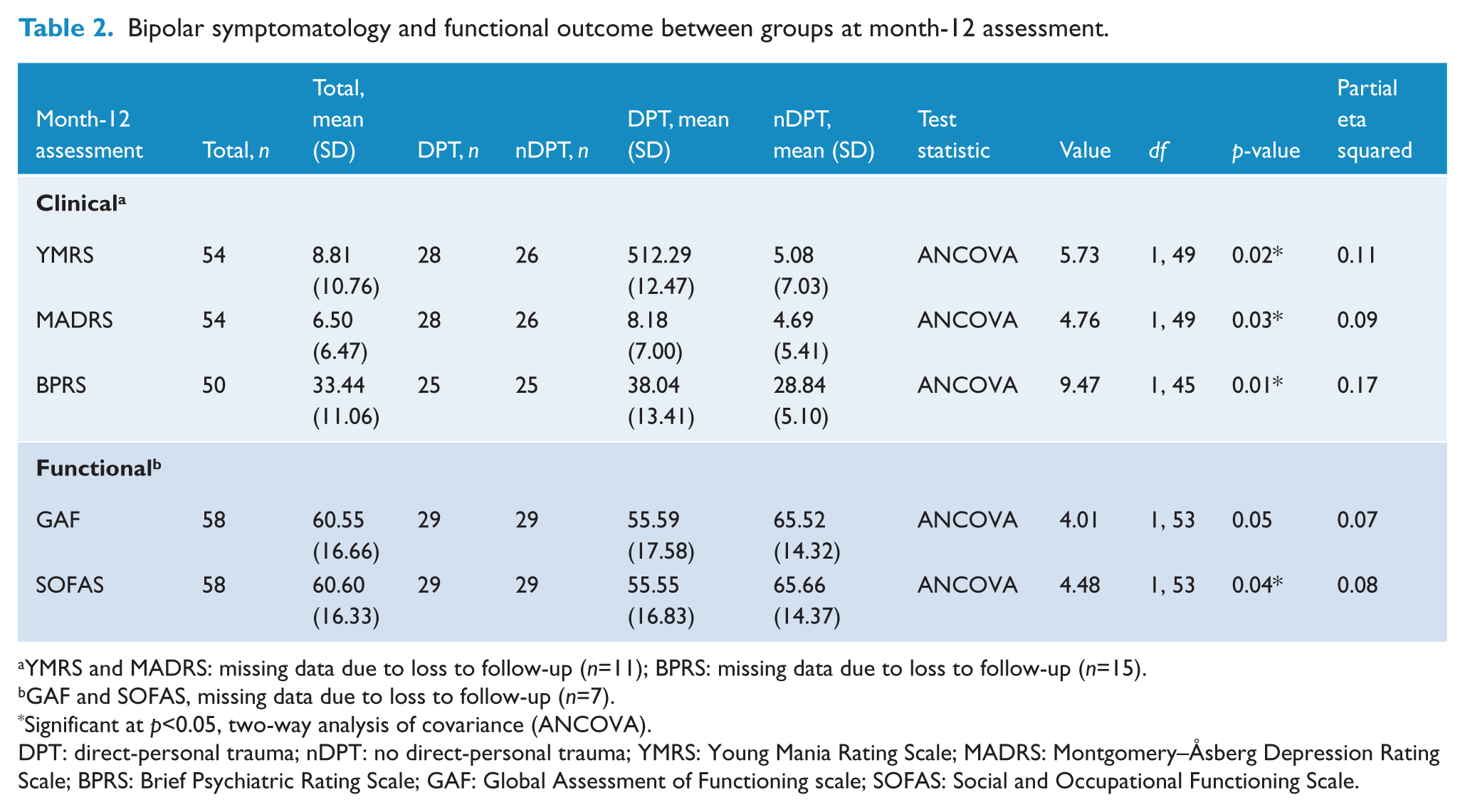
YMRS and MADRS: missing data due to loss to follow-up (n=11); BPRS: missing data due to loss to follow-up (n=15).
GAF and SOFAS, missing data due to loss to follow-up (n=7).
Significant at p<0.05, two-way analysis of covariance (ANCOVA).
DPT: direct-personal trauma; nDPT: no direct-personal trauma; YMRS: Young Mania Rating Scale; MADRS: Montgomery–Åsberg Depression Rating Scale; BPRS: Brief Psychiatric Rating Scale; GAF: Global Assessment of Functioning scale; SOFAS: Social and Occupational Functioning Scale.
Depression rating outcomes
Participants with a history of DPT had significantly worse depressive symptoms compared to the nDPT participants (p=0.03) (Table 2), with a medium effect size noted (ηp2=0.09) (Cohen, 1988). Again, there was no main effect in the interaction between randomised medication and trauma history (p=0.33).
Psychopathology symptomatology
Participants with past DPT had significantly higher mean BPRS total scores than nDPT participants (p=0.01), with a large effect size (ηp2=0.17) (Table 2). The interaction between trauma history and randomised medication was not significant (p=0.29).
Psychosocial and occupational functioning
Participants without past DPT presented with better global functioning than participants with past DPT; however, this difference was not significant (p=0.05) when baseline GAF scores were taken into account (Table 2). The interaction of randomised medication and trauma history was also found to be of no significance (p=0.99). For the SOFAS scale, the findings revealed that the social and occupational functioning of nDPT participants was significantly greater than the participants with DPT (p=0.04) and was of medium effect size (ηp2=0.08) (Table 2) (Cohen, 1988). While the interaction between trauma history and randomised medication was of no main effect (p=0.93), there was a significant difference in baseline SOFAS scores between trauma groups (p=0.04), with a medium effect size (ηp2=0.08) observed (Cohen, 1988).
Discussion
There are three main findings to this study. First, our results confirm that the prevalence of past exposure to trauma in patients with first episode psychotic mania is very high, with nearly half (48%) of the patients in this sample reporting past DPT. Second, patients with exposure to DPT have poorer outcomes in various symptomatic dimensions, including mania, depression and general symptoms. Third, past exposure to DPT is associated with worse functional outcome 12 months after the initial manic episode.
Regarding the prevalence of exposure to trauma, comparison between studies is difficult due to variations in the definition of trauma. In a previous study of a different sample of first episode psychotic mania patients (Conus et al., 2010), we focused on a more restrictive subtype of traumatic events and found that 24% of patients had been exposed to sexual and/or physical abuse (SPA). When focusing on exposure to SPA in the current sample, a comparable rate of 20% was found. Our finding that 48% of the patient sample had been exposed to DPT is in keeping with the literature (e.g. Garno et al., 2005), and the finding that 20% of patients had been exposed to emotional neglect suggests this particular dimension deserves more attention, considering it may play a role in the development of emotion regulation at an early age (Hildyard and Wolfe, 2002).
Exposure to trauma during childhood or early adulthood may impact the way various symptom dimensions evolve after a first episode of psychotic mania. First, in keeping with previous studies (Garno et al., 2008; Leverich et al., 2002; Levitan et al., 1998), we found that manic symptoms were still above the remissions threshold (YMRS score ≤ 12) after 12 months in DPT patients while nDPT patients were in remission. Second, we found that patients with a history of trauma were more likely to display depressive symptoms 12 months after the index manic episode. The average MADRS score for the participants with past exposure to DPT fell within the mild depressive range (MADRS score from 7 to 19), while participants with no previous DPT scored on average within the normal/absent symptom range (MADRS score from 0 to 6) (McDowell, 2006). This again is in phase with previous studies, which have shown that exposure to trauma in BPAD patients is related to inter-episodic depressive symptoms (Maguire et al., 2008), more distress and less happiness (Neria et al., 2005), increased severity of depression (Grandin et al., 2007), higher frequency of lifetime major depression episodes (Brown et al., 2005; Levitan et al., 1998) and an increased risk of suicide attempts (Brown et al., 2005; Garno et al., 2005; Leverich and Post, 2006).
Third, on a global psychopathology scale, we found that DPT patients (with an average BPRS score greater than 31 falling in the ‘mildly ill’ range) were at an increased risk of having ongoing residual symptoms (Leucht et al., 2005) compared to nDPT patients. Our findings of ongoing symptomatology in patients with DPT after an episode of psychotic mania, as well as previous reports of a poorer response to pharmacological treatment and the increased risk of future negative life events in BPAD patients with early adversities (Leverich et al., 2002), signify the importance of implementing coping strategies, cognitive-behavioural therapy and psychoeducation in the routine therapeutic care of these individuals (Post and Leverich, 2006).
In terms of functional recovery, this study revealed that even though on average participants with past DPT had poorer global functioning than those without a history of DPT, this difference was not significant. However, DPT was found to significantly impact social and occupational functioning 12 months following a first episode of psychotic mania. The difference in social and occupational functioning between groups was marked and indicated an increased vulnerability to functional recovery impediments from first episode with this specific comorbidity in the past. The results showed that individuals in the DPT group had moderate difficulty in social and occupational functioning with the possibility of moderate symptomatology at the time of the 12-month assessment; individuals without past DPT had a mild degree of difficulty in social and occupational functioning with the possibility of a few ongoing mild symptoms. These findings support the work of Conus et al. (2010) who identified that individuals with past SPA prior to the onset of first episode psychotic mania were less likely to regain a premorbid level of functioning compared to participants without such experiences.
When one considers the importance of psychosocial recovery early in the illness course (such as first episode) as a protective factor to defend against worsening or chronicity of symptoms (Hollon et al., 2002), these results provide a picture of worse symptomatic functioning in mania, depression and psychosis and more difficulty either returning to previous levels of functioning or progressing through the natural increases in psychosocial functioning across early adulthood. This indicates the importance of incorporating some of this understanding into treatment planning of psychological interventions for people with BPAD-I or schizoaffective disorder that is sensitive to both the risks of previous trauma history and the impact of these events on symptomatic and functional recovery.
There are a number of limitations to this study that need to be considered in the interpretation of the results. First, the generalisability of the findings is specific to young people comparable to those treated by a mental health centre specialising in the management of psychiatric illnesses for youth. The sample selected also represented individuals who experienced first episode mania with psychotic features, a subgroup that typically is more unwell at first episode (Conus and McGorry, 2002). This is particularly important when attempting to contrast the results of this investigation with others that include individuals with BPAD without the presence of psychotic symptoms (e.g. mania without psychosis, or those presenting in the depressive phase). Another important limitation is that past DPTs were not assessed on the basis of an interview specifically aimed at this ‘issue’ and were based on self-report, which tends to be associated with under-reporting and under-estimation of true incidence (Zlotnick et al., 1996). The under-reporting of traumatic childhood events may be due to the victims feeling embarrassed of past abuse or in order to protect the offender (Fergusson et al., 2000). In addition, the presence of affective symptoms may have influenced participants’ recall or the reporting of past traumatic experiences. Hence, the reliability of reports of past traumatic events may vary in response to recall bias and poor insight. However, information gathered from the files reflected interactions occurring in the context of very close case management, and in this frame of such a trusting relationship, as well as considering case managers’ knowledge of the importance of the various contextual characteristics of patients, it is likely that very few traumatic events would not have been discussed over the treatment period. However, traumatic events that may have occurred after the onset of participants’ first episode psychotic mania were not taken into account in this study and therefore careful consideration needs to be taken when interpreting the results. Moreover, trauma interacts with resilience factors, and this study did not include any measures of resilience (Yehuda and Flory, 2007). Finally, childhood trauma has an impact on attachment style and an increased risk of comorbidity with borderline personality disorder, which itself may be a major driver of adverse findings (Liotti et al., 2000; Sabo, 1997). This study did not take into account attachment style or personality disorders in the sample.
However, the strengths of this study are that it included a ‘real world’ cohort of consecutive referrals to a mental health service, had very few exclusion criteria, represented a varied socio-economic demographic and used assessments that were conducted over a 12-month period of care rather than a single cross-sectional interview. The advantages of the latter are that the data collected may be more accurate as it was obtained over time, and in the context of an ongoing therapeutic relationship.
In summary, this study indicates high prevalence rates of childhood trauma and its impact, with nearly half of the participants reporting having experienced DPT before the onset of their first episode of mania. The exposure to these traumas was associated with an increase in manic, depressive and general symptoms 12 months following participants’ first episode of acute mania with psychotic features. Additionally, individuals with past DPT had a decreased level of social and occupational functioning compared to individuals without past DPT. These findings highlight the clinical need of identifying past traumas in people presenting with first episode psychotic mania, and the importance of incorporating interventions that address these issues, particularly in terms of functional recovery.
Footnotes
Acknowledgements
The authors would like to thank the staff and participants at Orygen Youth Health for their assistance with this research.
Funding
This study was supported by an investigator initiated trial grant from Eli Lilly Australia. However, this company had no influence on the study design and was not involved in any way in data collection, data analysis and interpretation of the results.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.