
Abstract
Objective:
To describe lifetime and 12 month prevalence of common DSM-IV mental disorders, their demographic correlates, and association with service utilisation and disability in Australians aged 65–85 years of age.
Methods:
The sample included Australian residents aged 65–85 years who participated in the 2007 Australian National Survey of Mental Health and Well-being (n=1905). The prevalence of DSM-IV mental disorders was estimated using the lay-interviewer administered World Mental Health version of the Composite International Diagnostic Interview.
Results:
Eight percent had experienced an affective disorder, 10% an anxiety disorder, and 12% a substance use disorder at some point in their life. Sex, age, and marital status were significant correlates of any lifetime mental disorder. Approximately, 2%, 4%, and 1% of old age respondents met criteria for mood, anxiety, and substance use disorders in the past 12 months, respectively. The presence of physical disorder, disability, and greater treatment service use were associated with any mental disorder in the past 12 months. Prevalence of lifetime and 12 month disorders by age band revealed a decrease as age increased.
Conclusions:
A substantial number of community dwelling old age Australians have experienced a mental disorder in their lifetime. Demographic correlates of mental disorder were relatively consistent between lifetime and 12 month prevalence of disorders, although sex made less of an impact and the presence of physical disorders more of an impact in recent disorders. Twelve month prevalence data suggest that a high proportion of old age Australians still experience mental disorders, predominantly anxiety and major depression.
Introduction
Mental disorders represent a significant burden of disease in Western countries (Moussavi et al., 2007; Murray et al., 2012; Vos et al., 2012). In an effort to quantify and examine this burden, a number of countries have conducted national population-based surveys to generate a snapshot of the relative prevalence and correlates of these disorders in the community. In 1997, the first Australian National Survey of Mental Health and Wellbeing (NSMHWB) estimated that a sizable proportion (one in five) of the population had a mental disorder, but few received evidenced-based treatment (Andrews et al., 2001). An analysis focusing specifically on the mental health of old age respondents revealed one in six community-dwelling older Australians had been affected by a mental disorder in the past year (Trollor et al., 2007). Older women were more at risk of experiencing mood or anxiety disorders whilst older men were more at risk of substance use disorders and these disorders were found to be significantly related to levels of distress and poor physical health (Trollor et al., 2007).
Ten years later, Australia conducted a second NSMHWB, thereby providing an opportunity to review the current status of old age mental health in the new millennium. In addition to 30 day and 12 months point prevalence data, the 2007 NSMHWB also assessed the prevalence of disorders that occurred across each respon-dent’s lifetime. Within the survey sample, the old age cohort offers an interesting opportunity to review the notion of ‘lifetime’ prevalence at a greater breadth than that offered by younger cohorts. Bench marking lifetime prevalence in an old age cohort is a first step in what is likely to be an active period of research addressing topical questions about cohort differences, including: temporal ordering of disorders, age-of-onset peaks, survivor effects, and the applicability of the survey instrument’s methodology across cohorts.
Although the recent or current prevalence and service use data generated by the survey informs government policy makers about the community burden and trends for service planning, lifetime data offers valuable information to researchers and clinicians who are interested in taking a long-term or historical view of mental disorders, comorbidity (mental and physical disorders), and clinical presentations. Indeed, recent research in areas such as dementia and cardiovascular disease has highlighted the importance of taking a long term view of uncovering possible risk factors or antecedents of disease including a history of major depression (Butters et al., 2008; Byrne and Pachana, 2010; Herrmann et al., 2008; Hickie et al., 1997). Furthermore, a history of substance use, particularly alcohol, has been indicated as a risk factor in a number of neuropsychiatric disorders (Christensen et al., 2006). Robust prevalence estimates of mental disorders as they occur across the lifespan and within an old age cohort will assist with the interpretation of these critical variables in future research results (Kessler et al., 2007). Until now, no such prevalence estimates have been available in Australia and their utility will be supplemented by additional information collected by the NSMHWB about ‘co-morbidity’ as well as socio-demographic and physical health correlates. In what follows we present an analysis of lifetime, 12 month, and 30 day prevalence of the common mood, anxiety, and substance use disorders from the 2007 Australian NSMHWB in adults aged 65 years and over. The current article also explores sex differences, correlates of lifetime and recent disorder, co-morbidity, disability, and service use.
Method
Sample
Data for the current study were from the 2007 Australian NSMHWB, a cross-sectional household survey of the Australian general population (excluding very remote areas). The survey employed a randomly selected, stratified, multistage area design. The survey resulted in 8841 households participating (a response rate of 60%). The current study focused on the 1905 respondents aged between 65 and 85 years.
Assessment
Diagnostic information
The Composite International Diagnostic Interview version 3 (CIDI 3.0; Kessler and Üstün, 2004) was used as the base instrument to derive DSM-IV diagnoses of the mood, anxiety, and substance use disorders. This is a lay-interviewer administered structured diagnostic interview. The CIDI 3.0 possesses sound psychometric properties that have been described in detail elsewhere (Kessler et al., 2004). The mental disorders that were assessed in the 2007 Australian survey included: depression, dysthymia, bipolar disorder (manic episode), panic disorder, social phobia, agoraphobia, generalised anxiety disorder (GAD), substance use disorders (alcohol harmful use/abuse, alcohol dependence, alcohol abuse/dependence, drug harmful use/abuse, drug dependence, drug abuse/dependence), obsessive-compulsive disorder (OCD), and post-traumatic stress disorder (PTSD). Cognitive impairment was measured using the Mini Mental State Examination (MMSE; Folstein, Folstein and McHugh, 1975). To measure cognitive impairment, scores on the MMSE were dichotomised so that respondents with a score of 23 or less were defined as having some degree of cognitive impairment (mild to severe).
The 2007 survey also measured the presence of certain physical conditions experienced at some point in the respondent’s lifetime and over the previous 12 months. Physical conditions assessed by the survey included: asthma, any type of cancer, stroke, heart or circulatory conditions (heart attack, angina, high blood pressure), gout, rheumatism, arthritis, diabetes, and high blood sugar levels. Respondents with one or more of these physical conditions were coded as present for ‘any physical condition’ in subsequent analyses.
Disability and distress
The World Health Organization Disability Assessment Schedule 2.0 (WHODAS) was used as a self-report measure of activity limitation and disability due to either physical or psychological disorders in the past 30 days. The WHODAS consists of 12 items on a 5 point scale. Scores range between 0 and 100 with higher scores indicating greater disability. The WHODAS has evidenced a stable factor structure (Andrews et al., 2009) and good reliability and validity in relation to other measures of disability (Üstün et al., 2010). Additional items of disability were included in the survey to assess the respondent’s total number of days out of role in the past 30 days due to their health.
Service utilization
All respondents reported whether they had ever seen a doctor or health professional (e.g. general practitioner, psychiatrist, psychologist, mental health nurse, social worker, counsellor, occupational therapist, specialist doctor, herbalist, or naturopath) for a mental health condition, such as anxiety, depression, or substance use.
Data analysis
All reported prevalence estimates and descriptive data were weighted to reflect the age and sex distribution of the Australian population and to control for the probability of being sampled. The SUDAAN statistical software package was used to adjust the standard errors and confidence intervals around the odds ratios (OR) for the complex survey design using a balanced repeated replication technique. Logistic regression analyses were performed that examined the relationship between gender and lifetime and 12 month mental disorders controlling for age. Multivariate logistic regressions were used to calculate the adjusted ORs and examine the independent association between lifetime and 12 month mental disorders (collapsed into three disorder groups; any affective, any anxiety, and any disorder) with socio-demographic factors, cognitive impairment and the presence of any physical disorder. Separate univariate multinomial logistic regressions were used to examine the relationship between the level of observed co-morbidity and the proportion of respondents with a current disorder, one or more mental health consultations in the past 12 months, and disability as measured by the WHODAS.
Results
Socio-demographic characteristics
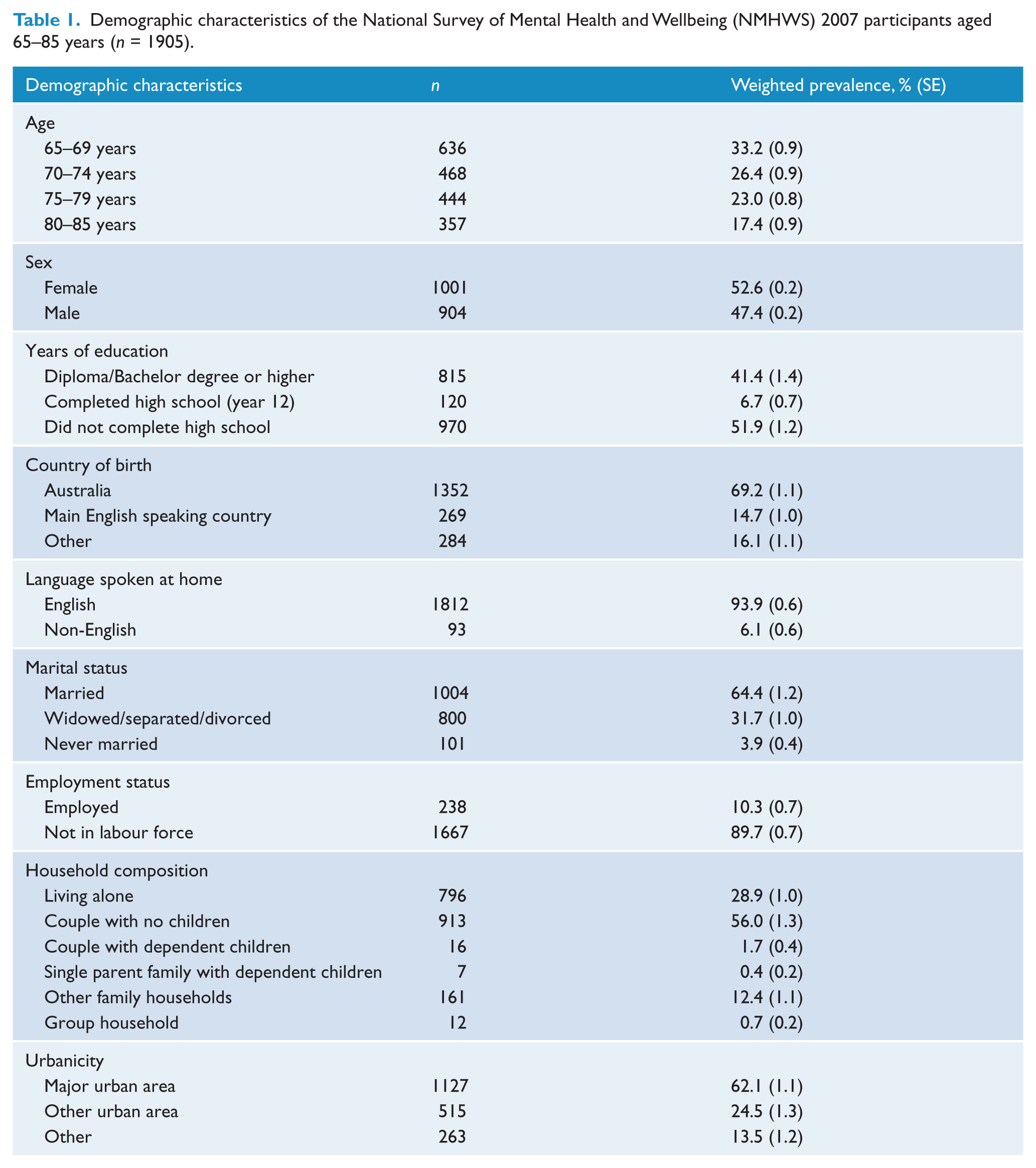
The socio-demographic characteristics of the current sample are provided in Table 1. The majority were Australian born individuals (69%) living in a city/urban environment (62%). About half the group were female (53%), and most were not in the workforce (90%). Nearly half the sample had completed high school or further tertiary study. The majority (65%) of participants were married or in a de facto relationship, 32% were widowed or separated and 4% had never married. A sizeable minority (29%) were living alone. Similar socio-demographics characteristics were found for Australians over the age of 65 who took part in the 2006 Australian national census, albeit the current sample contained slightly more Australian-born individuals (compared to 59% from census data) and were more educated (compared to 21% who completed high school from census data).
Demographic characteristics of the National Survey of Mental Health and Wellbeing (NMHWS) 2007 participants aged 65–85 years (n = 1905).
Prevalence of psychiatric disorders in the elderly group
As observed in Table 2, about one in four older respondents met criteria for a lifetime affective, anxiety, or substance use disorder. Substance use disorders across a lifetime were observed in 12% of the sample, closely followed by anxiety disorders (11%), and then affective disorders (8%). In the past 12 months, 6% of the sample met criteria for an affective, anxiety, or substance use disorder and this was reduced to 3% in the past month. In contrast to the lifetime pattern, anxiety disorders in the past 30 days were common, followed by affective disorders in the past 30 days and substance use disorders in the past 30 days were rare. The MMSE indicated that 6% of the sample experienced cognitive impairment (scored less than 24 points).
Population prevalence of DSM-IV mental disorders and univariate logistic regression comparing the population prevalence of DSM-IV mental disorders in NSMHWB 2007 participants aged 65–85 years by sex controlling for age.
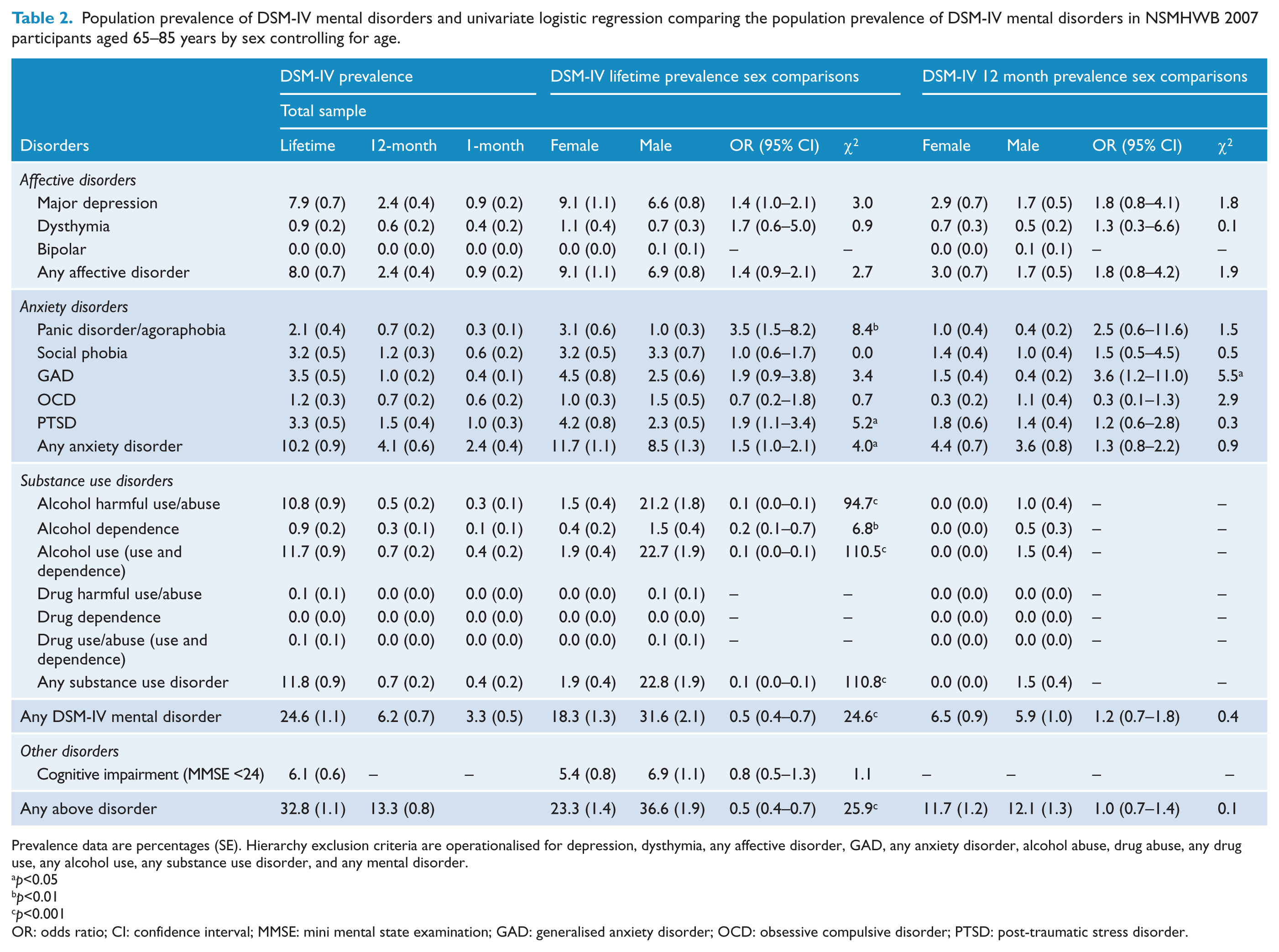
Prevalence data are percentages (SE). Hierarchy exclusion criteria are operationalised for depression, dysthymia, any affective disorder, GAD, any anxiety disorder, alcohol abuse, drug abuse, any drug use, any alcohol use, any substance use disorder, and any mental disorder.
p<0.05
p<0.01
p<0.001
OR: odds ratio; CI: confidence interval; MMSE: mini mental state examination; GAD: generalised anxiety disorder; OCD: obsessive compulsive disorder; PTSD: post-traumatic stress disorder.
Sex differences in the prevalence of psychiatric disorders
Lifetime
As can be seen in Table 2, there was an overall difference in the proportion of mental disorders between sexes (OR 0.5, df = 1, p<0.01). Males were more likely to meet criteria for a mental disorder than females and this was largely driven by the dramatic contrast in prevalence of alcohol abuse/use and, to a smaller degree, dependence between the groups. Significant sex differences were also observed for the anxiety disorders, with females being three times more likely to have experienced panic disorder/agoraphobia, and almost two times more likely to have experienced PTSD than males.
Twelve months
There were few significant differences in 12 month prevalence of disorder between the sexes; however, low overall prevalence may have contributed to some of the findings (see Table 2). Odds ratios indicate a theme of increased prevalence in females for affective disorders and anxiety disorders but only a gender difference in generalized anxiety disorder (GAD) was significant.
Correlates of mental disorders
As can be seen in Tables 3 and 4, age was significantly related to disorder with the general theme of lower prevalence in older age bands than in those aged 65–69. Marital status was significantly related to lifetime affective disorders, and any lifetime disorder, with married respondents having a decreased likelihood of any lifetime disorder. In the 12 months data, the presence of a physical disorder had a significant impact on the likelihood of any mental disorder. Perhaps not surprising is that independent variables with a ‘current’ aspect such as current employment status and current physical disorder were not significant in the lifetime regression analyses.
Multivariate logistic regressions showing the demographic correlates of lifetime DSM-IV mental disorders in respondents aged 65–85 years.
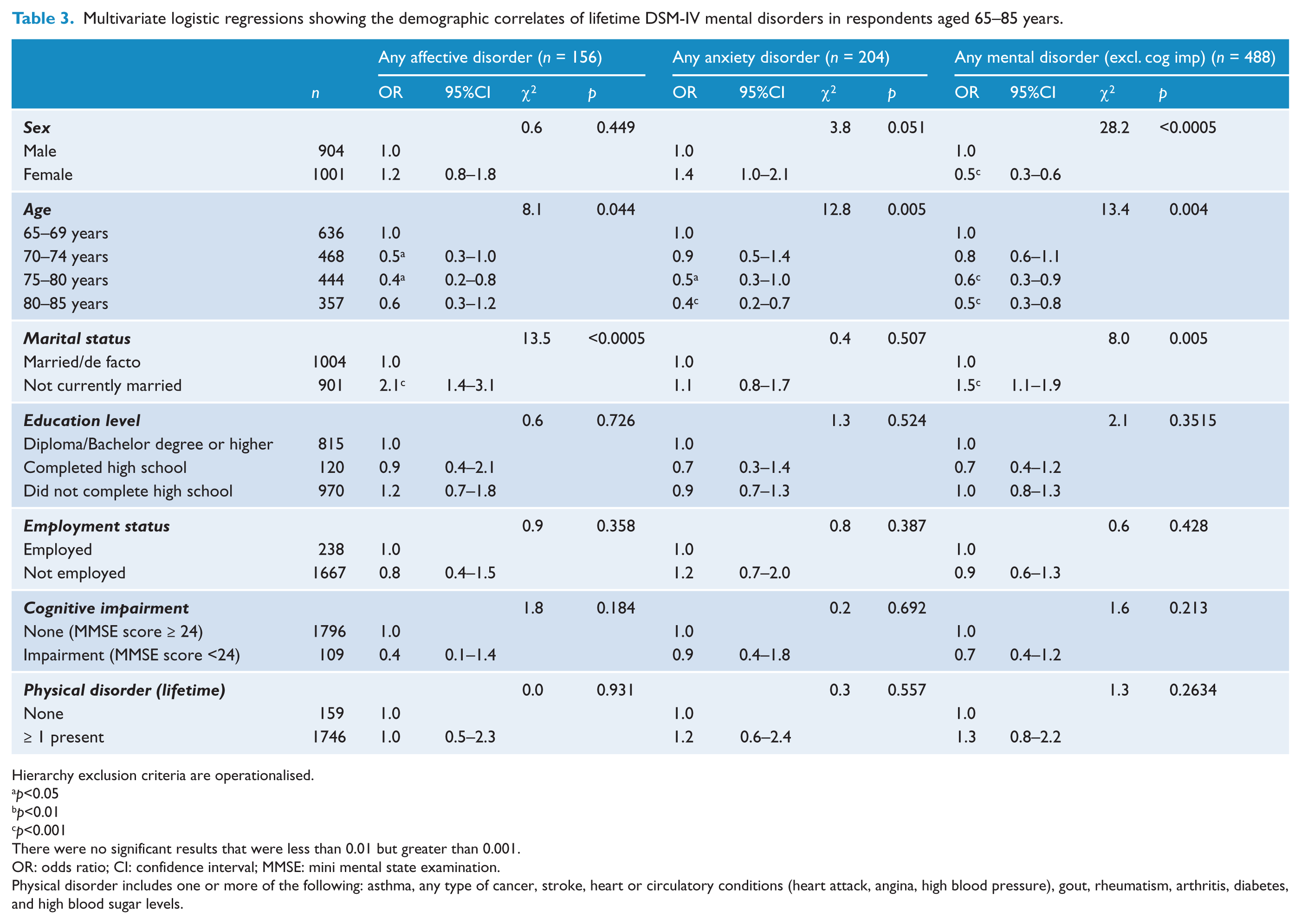
Hierarchy exclusion criteria are operationalised.
p<0.05
p<0.01
p<0.001
There were no significant results that were less than 0.01 but greater than 0.001.
OR: odds ratio; CI: confidence interval; MMSE: mini mental state examination.
Physical disorder includes one or more of the following: asthma, any type of cancer, stroke, heart or circulatory conditions (heart attack, angina, high blood pressure), gout, rheumatism, arthritis, diabetes, and high blood sugar levels.
Multivariate logistic regression showing the demographic correlates of 12 month DSM-IV mental disorders in respondents aged 65–85 years.
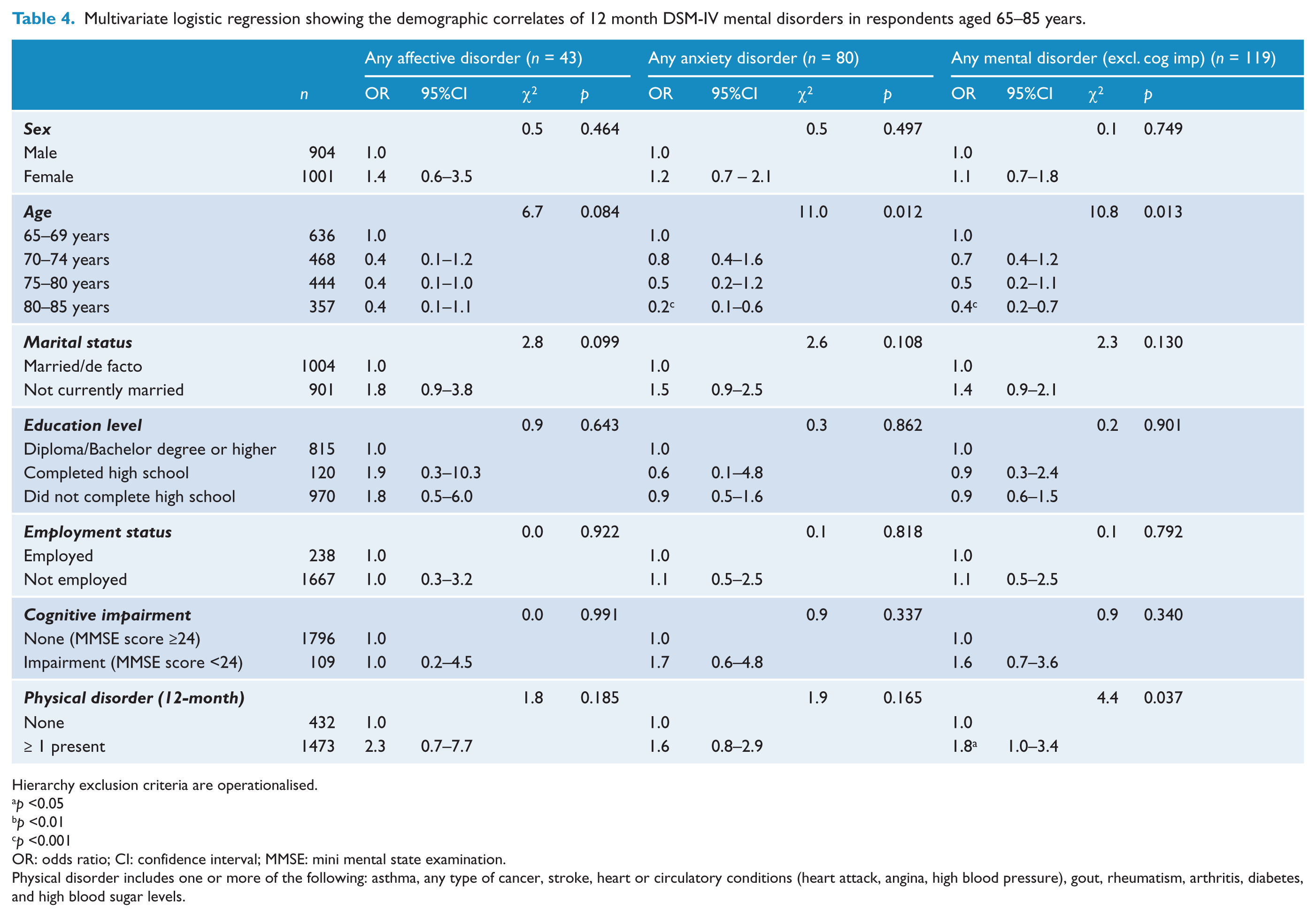
Hierarchy exclusion criteria are operationalised.
p <0.05
p <0.01
p <0.001
OR: odds ratio; CI: confidence interval; MMSE: mini mental state examination.
Physical disorder includes one or more of the following: asthma, any type of cancer, stroke, heart or circulatory conditions (heart attack, angina, high blood pressure), gout, rheumatism, arthritis, diabetes, and high blood sugar levels.
Old-old age and prevalence of mental disorders
The correlates of mental disorder observed in Tables 3 and 4 indicate that disorders were reduced as age increased. In Table 5 we present the prevalence of DSM-IV lifetime and 12 month disorder by age bands. For lifetime disorders, a theme of decreasing prevalence was mostly observed for the older age bands, often with a 5–10% disparity in prevalence between the ‘young-old’ (defined in this study as 65–69 years) and ‘old-old’ (defined in this study as 80–85 years). An exception was lifetime and 12 month major depressive disorder; with the ‘old-old’ experiencing less disorder than the ‘young-old’ but not those aged 70–80 years. Of note, closer inspection of the age band data reveals that of those aged 65–74 years around one in three have experienced a mental disorder (excluding cognitive impairment) in their lifetime.
Population prevalence of lifetime and 12 month DSM-IV mental disorders in NSMHWB 2007 participants aged 65–85 years.
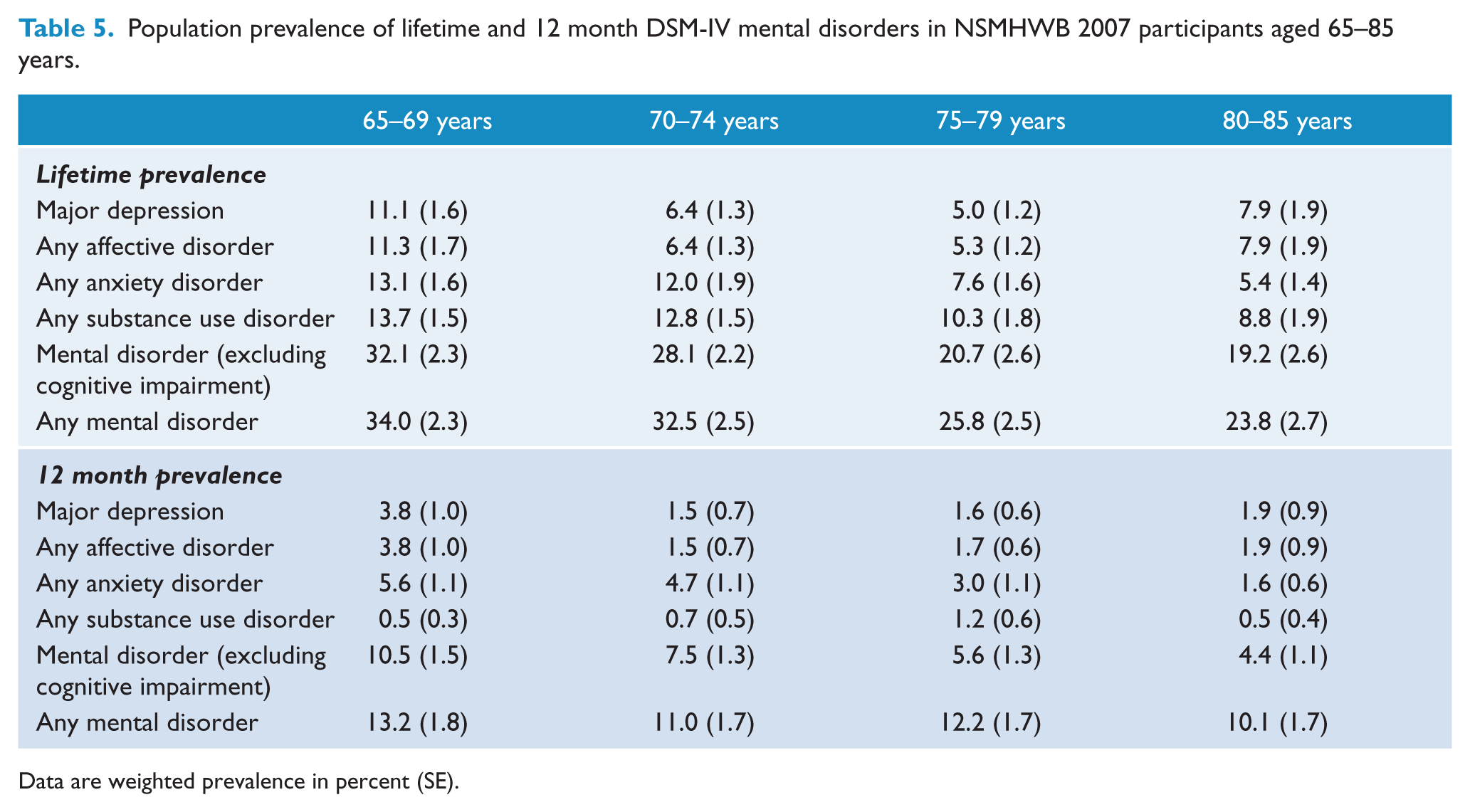
Data are weighted prevalence in percent (SE).
Co-morbidity and its association with disorder chronicity, disability, and service utilisation (12 month mental disorders)
Disability scores and service utilisation by number of disorders experienced are provided in Table 6. Of those who met criteria for 12 month DSM-IV disorder, the majority had a single disorder. For those with one or more disorders in the past year, 46–66% still met diagnostic criteria in the past 30 days. Only 26% of those with a single disorder had consulted a health professional for a mental health problem in the past 12 months, but this significantly jumped to 66% for comorbid cases (F(3, 57)=40.73, p<0.01) . The total sample of older adults generated a mean WHODAS score of 11 (SE = 0.42) and had on average 3 (SE=0.27) days out of role in the past 30 days due to poor health. Older individuals with any mental disorder in the past 30 days scored an average of 22 (SE=2.6) for the WHODAS and an average of 6 (SE=1.2) days out of role in the past 30 due to poor health. Older individuals with any affective disorder in the past 30 days scored an average of 27 (SE=6.0) for the WHODAS and 8 days out or role due to poor health. Conversely, older individuals with any substance use disorder reported lower WHODAS scores and days out of role with an average of 14 (SE=7.1) and 1 (SE=1.0), respectively. WHODAS scores were significantly associated with comorbidity (F(3, 57)=19.29, p<0.01) and respondents with three or more mental disorders were more likely to receive a high score on the WHODAS than those with a single disorder. Similarly, respondents with a single disorder were more likely to receive a high score on the WHODAS than those with no mental disorders. Conversely, there was no significant difference in mean WHODAS scores between those with one disorder and those with two disorders. It is important to note that among this sample mental health comorbidity was not significantly associated with the presence of physical conditions in the past twelve months (F(3, 57)=1.22, p=0.31), therefore the observed increase in impairment associated with mental health comorbidity could not be attributed to an increased probability of physical conditions.
Relationships between comorbidity, current (30-day) disorder, service utilisation, and disability for persons with one or more 12-month DSM-IV mental disorders.
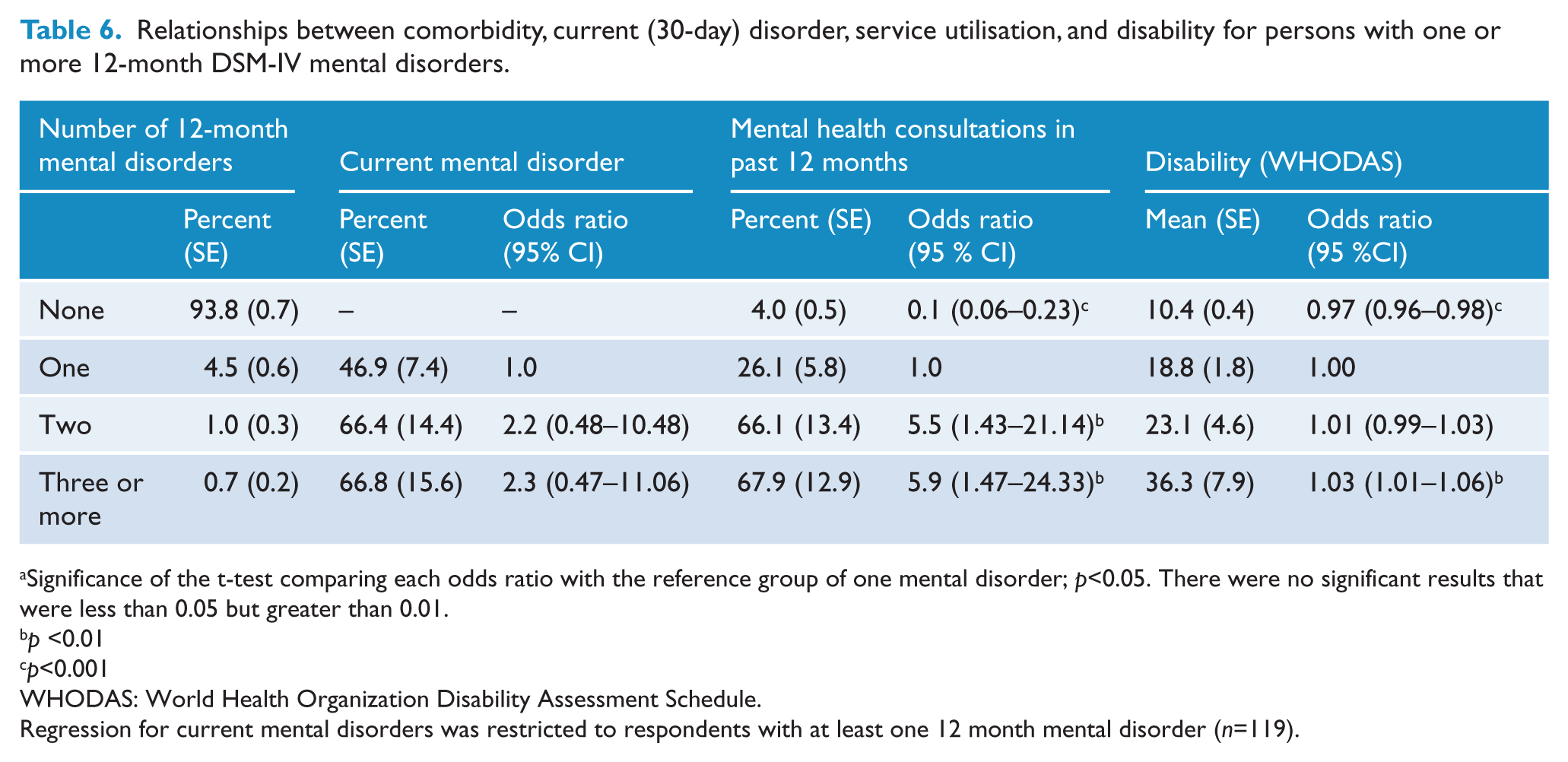
Significance of the t-test comparing each odds ratio with the reference group of one mental disorder; p<0.05. There were no significant results that were less than 0.05 but greater than 0.01.
p <0.01
p<0.001
WHODAS: World Health Organization Disability Assessment Schedule.
Regression for current mental disorders was restricted to respondents with at least one 12 month mental disorder (n=119).
Discussion
A substantial number of community-dwelling older Australians have experienced a mental disorder in their lifetime (approximately one in four). The prevalence of mental disorders in this group, however, is substantially reduced for 12 month and current (30 day) disorders (approximately one in 16 and one in 30, respectively). The prevalence estimates for lifetime and 12 month disorders appear to drop off in the older age bands with an approximate 12% drop in lifetime prevalence from respondents aged 65–69 to respondents aged 80–85 and an approximate 5% drop in 12 month prevalence. This observed decrease in prevalence in the older respondents may be partially explained by (but not limited to) several possible factors; the first is a survival effect, i.e. that only relatively healthy individuals will survive to the older age bands, the second is a cohort effect, i.e. that older generations may be more mentally healthy than slightly younger generations, and the third is a resilience effect, i.e. older individuals may be more resilient to the effects of mental health or have accepted that it is a natural part of aging and are not as equally effected by health problems. The reduced prevalence could be an artefact of retrospective assessment, i.e. older individuals may not recall or remember as many lifetime episodes of poor mental health in comparison to younger respondents (Ernst and Angst, 1995; Jorm, 2000; Streiner et al., 2009). Moreover, researchers have raised some doubts over the validity of the diagnostic instrument used by the NSMHWB to assess mental health in older adults, which may have influenced the observed change in prevalence in comparison to younger adults (O’Connor and Parslow, 2009; 2010a; 2010b). Finally, despite extensive non-response analysis (see Australian Bureau of Statistics, 2009), the response rate for the current survey was not optimal and the significant differences between the education level from the current sample with census data as well as exclusion of older individuals with mild cognitive impairment may indicate that we have a higher functioning sample of older individuals.
Demographic correlates of mental disorders in this old age population remain relatively consistent between lifetime and 12 month disorders although sex makes less of an impact and the presence of physical disorders more of an impact in mental disorders experienced in the past 12 months. Current marital status is significantly related to the presence of lifetime mental disorders, with older respondents not currently married demonstrating a greater risk of past lifetime affective disorders compared to those currently married or in a de facto relationship. Conversely, current marital status is not related to the presence of a mental disorder in the past 12 months. This finding suggests that marital status is an important correlate of affective disorders experienced earlier in life compared to episodes experienced later in life; however, this relationship might be explained by current levels of social, community, and family support.
Comorbidity between mental disorders in the last 12 months or the occurrence of multiple mental disorders in a lifetime is relatively common. Importantly, the results suggest that the level of disability and service use increase with greater levels of comorbidity. These results are consistent with data from the wider population and provide an image that mental health comorbidity is related to higher degrees of severity, disability (functional impairment), and service use across the various age bands (Teesson, Slade and Mills, 2009). In this context, levels of comorbidity could be interpreted as a cumulative indicator of general psychopathology and severity or the tendency to experience several related disorders rather than conceptualising comorbidity as two truly distinct disorders that randomly co-occur within the same individual. Comorbidity was greatest between the mood and anxiety disorders only or a combination of mood, anxiety, and substance use disorders. There were no respondents with two or more substance use disorders only with the vast majority of cases presenting with alcohol use rather than illicit drug use. These findings confirm those found previously that suggest substance use disorders peak in adolescents and young adults before rapidly declining with older age (Mewton et al., 2011).
The data shows a history of substance use disorders in elderly men (more than one in five), despite very low prevalence of current/recent substance use disorders in old age respondents. Many had experienced multiple episodes of a single disorder, and a high proportion had experienced more than one disorder across their lifespan. Researchers may wish to consider their research protocols in light of these data. For example, studies may ask about current drinking and screen for current mental wellbeing but neglect to comprehensively assess psychopathology in the past that could prove to be salient. In short, to some degree the lifetime data suggest that when working with older Australians it cannot be assumed that ‘well now’ equates to well in the past given that one quarter have experienced a diagnosable disorder in their lifetime. Moreover, the results suggest that possibly many older adults have now recovered from common mental disorders that they have experienced in the past. Consequently, the inclusion of historical health/mental health variables in studies where casual links are suspected does seem warranted.
The decreased lifetime prevalence observed in older individuals is surprising to those who would expect the high lifetime prevalence observed in the young and middle age cohorts to continue on and remain constant, if not increase, through to old age (Streiner et al., 2009). The contradictory results have been explained by numerous potential factors including a significant cohort effect and/or a survival effect. Most notably, however, researchers have speculated whether the use of lifetime prevalence is valid in terms of the respondent’s ability to recall sufficient detail required to form a diagnosis. Researchers have attempted to investigate the extent of recall bias by comparing prevalence estimates generated from prospective studies with estimates generated from retrospective studies and have demonstrated substantially higher estimates using prospective designs (Moffitt et al., 2010; Patten, 2009). However, prospective studies have also been criticised for overestimating prevalence due to sensitisation from repeated measurements over time and increased sampling bias due to drop outs (Merikangas, 2011). With these limitations in mind, we acknowledge the fragility of the lifetime prevalence construct, particularly in this population. Caution should be exercised when interpreting the reported estimates as they represent a potentially lower estimate of prevalence in comparison to estimates produced by more robust survey designs.
Researchers, clinicians, and policy makers interested in this geriatric group should be mindful that many of our older community members appear to have had previous experience with mental health adversity. However, a majority of those who previously experienced poor mental health in their lifetime do not currently meet criteria for any disorder. This may reflect disorders with recurring and remitting course, access to effective treatment services, and/or robust mental health literacy (i.e. knowledge and beliefs about mental disorders) of our older community members. The data may also reflect the overall notion of resilience (cognitive and biological) as an explanation for the lower prevalence observed in old age. Public health initiatives may focus on lifetime prevalence data to inform recovery and resilience programs. Researchers investigating various diseases may focus on lifetime data as a reminder that as much as one quarter of old age research volunteers, despite reporting current mental wellbeing, may have a history of mood and anxiety disorders and an alcohol use disorder that may need to be considered.
Footnotes
Funding
MS was supported by a National Health and Medical Research Council Early Career Fellowship (no. 1052327) and a National Health and Medical Research Council Project grant (no. 1045013). TMA, PSS, and GA were supported by a National Health and Medical Research Council Program Grant (no. 350833) and a National Health and Medical Research Council Capacity Building Grant (no. 568940).
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.