
Abstract
Background:
Most of what we know about the psychiatric consequences of injury is limited to the first year. Determining the prevalence of and risk factors for psychiatric morbidity beyond one year will aid service development and facilitate timely diagnosis and treatment. The aim of this prognostic study was to determine the prevalence of mental disorders in the three years following serious injury and to identify risk factors for the onset of new disorders after 1 year.
Methods:
Of 272 patients assessed in hospital following serious injury, 196 (72.1%) were reassessed at 3 years. Assessment involved gold standard semi-structured interviews for psychiatric diagnoses, risk factors for mental disorder, injury measures and pain scores.
Results:
More than a quarter of all patients were diagnosed with at least one mood or anxiety disorder at some stage during the three years following their injury. The most common diagnoses were major depression (20.0%), generalised anxiety disorder (6.7%) and panic disorder (6.7%). For a third of these patients, the disorder appeared after 12 months, for which persistent physical disability was an independent risk factor.
Conclusion:
Although there is a necessary focus on the early detection and treatment of mental disorders after injury, attention to later onset disorders is also required for those with persistent pain and physical disability.
Keywords
Introduction
Serious injury makes its significant contribution to the global burden of disease through both physical and psychological mechanisms (World Health Organization, 2008). Psychiatric morbidity after injury impairs long-term function (O’Donnell et al., 2013) and reduces quality of life (O’Donnell et al., 2005). Most of what we know about the psychiatric consequences of injury, however, is limited to the first year post injury, despite the common clinical experience of problems continuing well beyond this time. We do not know, for example, what proportions of patients’ disorders are persistent, which types of disorders persist and whether new disorders arise. Furthermore, we do not know the risk factors for persistence or late onset – a necessary step in determining whether they are modifiable.
The most comprehensive prospective study of psychiatric disorder after injury was conducted on almost 1000 patients admitted to level 1 trauma hospitals Australia wide (Bryant et al., 2010). At 12 months, 11.6% of patients described major depression, 9.7% post-traumatic disorder (PTSD), 9.5% generalised anxiety disorder and 6% agoraphobia – findings consistent with earlier studies (O’Donnell et al., 2004b; Shalev et al., 1998; Zatzick et al., 2002). Psychiatric co-morbidity (O’Donnell et al., 2004a) is common, with major depression and PTSD more likely to occur together than in isolation. The diagnostic status of an individual can also change, with only half of those reporting major depression at 12 months having done so at 3 months (Bryant et al., 2010). Little is known about psychiatric disorder beyond 12 months. One indication of its persistence is found in a study by Malt et al. (1988), which used a rating scale to make diagnoses 28 months after injury, and reported the prevalence of PTSD and major depression to be 2.8% and 0.9%, respectively.
Risk factors for psychiatric disorder after serious injury have been identified in the pre-injury, peri-injury and post-injury periods (Table 1). Pre-existing risk factors identified in the general population – age (Barkow et al., 2003), sex (Merikangas et al., 1985) and marital status (Sargeant et al., 1990) – do not necessarily apply to injury patients. Others – family history (Sullivan et al., 2000) and poor social support (Wade and Kendler, 2000) – have not been studied. Post injury, pain (Liedl et al., 2010), persistent medical problems (Mayou and Bryant, 2001) and mild traumatic brain injury (Bryant et al., 2010) all correlate with the development of PTSD. In addition, Bryant et al. (2010) found that functional impairment present 3 months after injury was associated with psychiatric disorder at 12 months.
Risk factors for psychiatric disorder post injury.
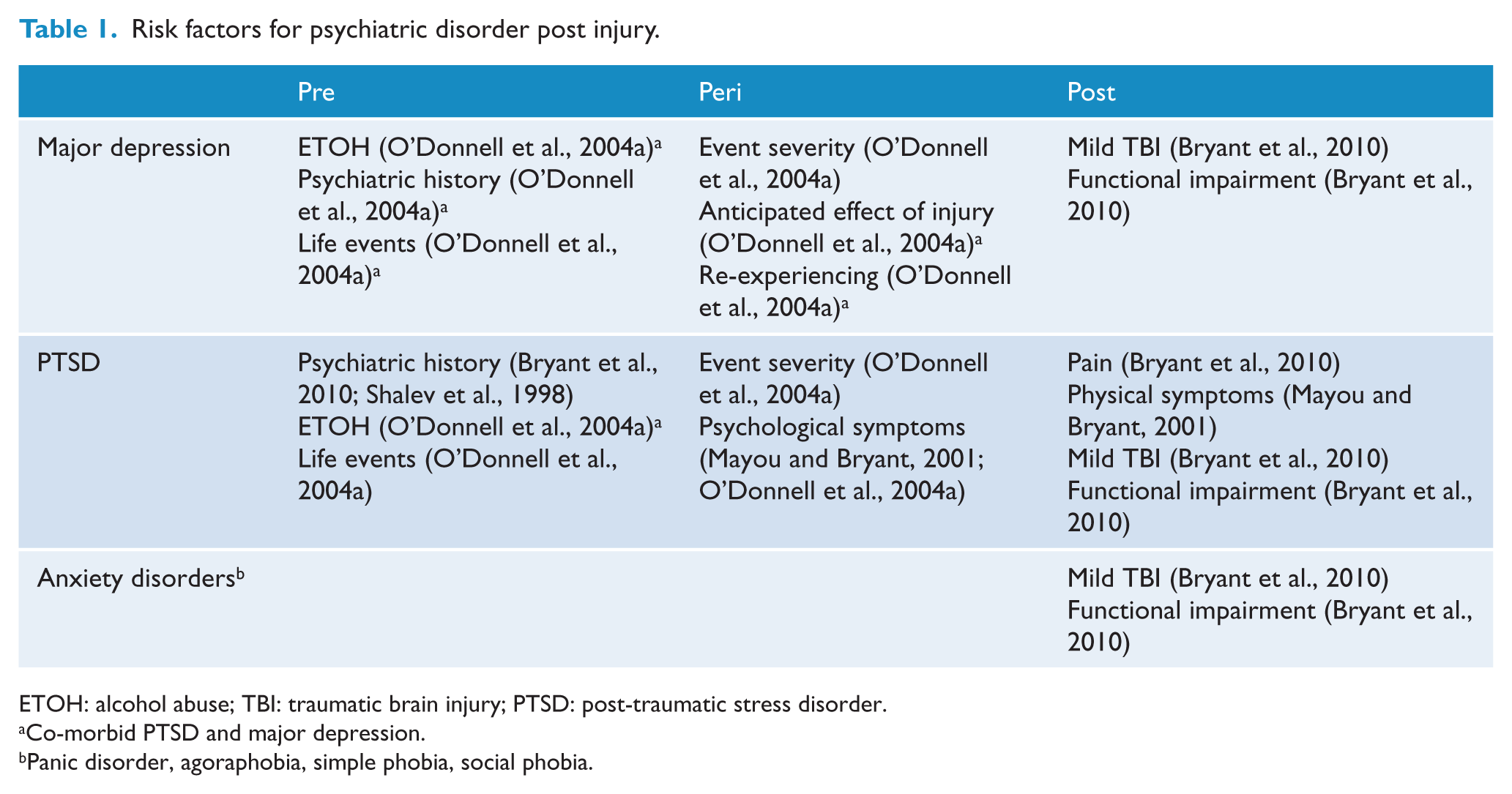
ETOH: alcohol abuse; TBI: traumatic brain injury; PTSD: post-traumatic stress disorder.
Co-morbid PTSD and major depression.
Panic disorder, agoraphobia, simple phobia, social phobia.
This paper describes a prospective cohort study of patients following serious injury in which the presence of psychiatric disorder was determined at index, and 1 and 3 years. Patients with head injury were not included. The aim of the study was to determine the prevalence of new psychiatric disorders emerging in the 3 years after serious injury, to determine the degree to which disorders persisted or new disorders emerged after 1 year, and to identify unique risk factors associated with the delayed emergence of new disorders.
Methods
Subjects
Patients were recruited from sequential admissions to two level 1 trauma centres in Melbourne, Australia. Patients were eligible for the study if they were between 18 and 70 years of age; were admitted for more than 24 hours; scored two or more on the Abbreviated Injury Scale (AIS; Association for the Advancement of Automotive Medicine, 1998); had adequate English; and could be assessed within 30 days of injury. Individuals were excluded if their injury was due to a non-height fall; had a head injury or pre-existing cognitive impairment; or were known to be psychotic or suicidal.
Candidates (n=272) undertook an interview and completed questionnaires when deemed able to provide consent and to engage in the initial assessment. The mean age of the sample was 38.4 years (standard deviation (SD) = 13.0) and 73.0% were male. The mean Injury Severity Score (Baker et al., 1974) was 12.0 (SD=8.4). The most common causes of injury were transport accidents (60.3%), falls (23.1%) and assaults (5.9%). Participants spent an average of 10.0 (SD=9.8) days in hospital. One ninety six (72.1% of original cohort) were reassessed at 3 years. Those who were not able to be reviewed (n=78) were no different in terms of age, sex, marital status, work, injury severity, pain or socio-economic status (SES) .
Mental disorder
Current and past psychiatric disorder was determined using the Structured Clinical Interview for DSM-IV disorders (SCID) (Spitzer et al., 1996). The SCID was administered by trained and experienced practitioners during the index admission and again at 1 and 3 years. At the index assessment, the presence of current or past psychiatric disorder was determined. At subsequent assessments, for each mental disorder, a determination was made as to whether it was currently present or an episode had occurred since the last assessment.
Risk factors
The risk factors for mental disorder were determined with reference to the literature on major depression and PTSD in the general population (Baker et al., 1974; Brewin, 2005) and following injury (Bryant et al., 2010; Mayou and Bryant, 2001; O’Donnell et al., 2004a). Pre-injury and injury data were collected during the index admission whilst post-injury factors were collected at 1 and 3 years.
Pre-injury
Demographic: Age, sex, marital status (single/partnered), living status (alone/shared) and income (greater or less than $90,000).
Social support: The Multidimensional Scale of Perceived Social Support (MSPSS) (Zimet et al., 1990) was completed in relation to the time prior to the injury. The MSPSS is a 10-item self-report questionnaire that informs three subscales of support from family, friends and significant others.
Physical function: The Physical Function subscale of the SF-36 version 2 (Ware and Sherbourne, 1992) was used to assess limitation in function due to physical illness. The SF-36 is a self-report questionnaire used to describe function in the 4 weeks prior to assessment.
Family history: A family history of major depression and psychiatric disorder was assessed using questions requiring ‘yes/no’ answers.
Past psychological distress: Statements requiring answers using an 11-point numerical rating scale (NRS) (0=not at all, 10=totally) were used to measure past depression (‘feeling low or sad has impacted on my life in the past’), anxiety (‘feeling anxious or nervous has impacted on my life in the past’), past psychiatric help (‘I have needed professional help to deal with emotional problems in the past’) and life events (‘previously traumatic events have impacted negatively on my life in the past’).
Injury
Injury severity: Each individual injury was scored using the AIS (Association for the Advancement of Automotive Medicine, 1998). Severity is rated on a scale of 1 to 6, where 1 is equivalent of a superficial cut, 3 a fracture, and 6 an injury incompatible with life. The AIS scores are used to generate the Injury Severity Score (Baker et al., 1974).
Pain severity: Current and 24-hour pain severity was measured at the time of the initial assessment using an 11-point NRS (0=no pain, 10=the worst pain imaginable).
Peri-injury
Anxiety and depression: The severity of anxiety and depression symptoms following the injury was measured using the Hospital Anxiety and Depression rating scale (Zigmond and Snaith, 1983).
Subjective event severity: The answer to ‘During the event, I thought I was about to die’ was rated on an 11-point NRS.
Re-experiencing: The answer to ‘I have sweated, trembled or noticed my heart beating faster when I am reminded about the event’ in the time following the injury was rated on an 11-point NRS.
Anticipated effect of injury: The answer to ‘I am confident that I will fully recover from my injuries’ in the time following the injury was rated on an 11-point NRS.
Post injury
Physical disability: Limitation in function due to injury in the 4 weeks prior to assessment was measured with the Physical Function subscale of the SF-36 version 2.
Pain severity: Pain severity was measured using an 11-point numerical rating scale (NRS) in response to ‘How severe was your pain on average over the past 24 hours?’.
Social support: The MSPSS.
Compensation: The injury was deemed compensable if it was eligible for either the work-based or transport no-fault compensation schemes.
Analysis
Data were entered into the IBM SPSS (Statistical Package for the Social Sciences) for Windows, v.19, 2010 (IBM Corp., Armonk, NY, USA). For each episode of mental disorder, it was determined if it occurred: (1) prior to the injury; (2) in the first 12 months following the injury (early); or (3) in the second and third years after the injury (late).
Logistic regression analysis was conducted in order to determine the risk factors associated with the onset of mental disorder (not including alcohol or substance abuse disorders). Separate analyses were conducted for new episodes of mental disorder occurring early and late after injury. In the first step, a bivariate analysis was conducted to determine the association between each risk factor and the presence of mental disorder. Pearson correlation was used for continuous variables and analysis of variance (ANOVA) for categorical independent variables. All factors with p-scores <0.15 were entered into a logistic regression model. The factors were removed stepwise if they did not contribute independently to the model in order of least contribution to the variance. In the final model, the Nagelkerke R2 statistic was used for an approximate measure of proportion of variance (range 0 to 1) accounted for by the combined factors.
Results
More than a quarter of all patients were diagnosed with a mood or anxiety disorder in the 3-year period following their injury (Table 2). The most common diagnoses were major depression (20.0%), generalised anxiety disorder (6.7%) and panic disorder (6.7%). A third of the disorders appeared in the second and third years after injury: mainly major depression (8.2%), panic disorder (3.6%) and generalised anxiety disorder (3.6%). Only two new cases of PTSD occurred after 12 months. At 3 years, co-morbidity was common, with 43% of those with one mood and anxiety disorder attracting at least one other diagnosis.
Prevalence of mental disorders prior to injury, in the first year, and during years 2-3 after injury.
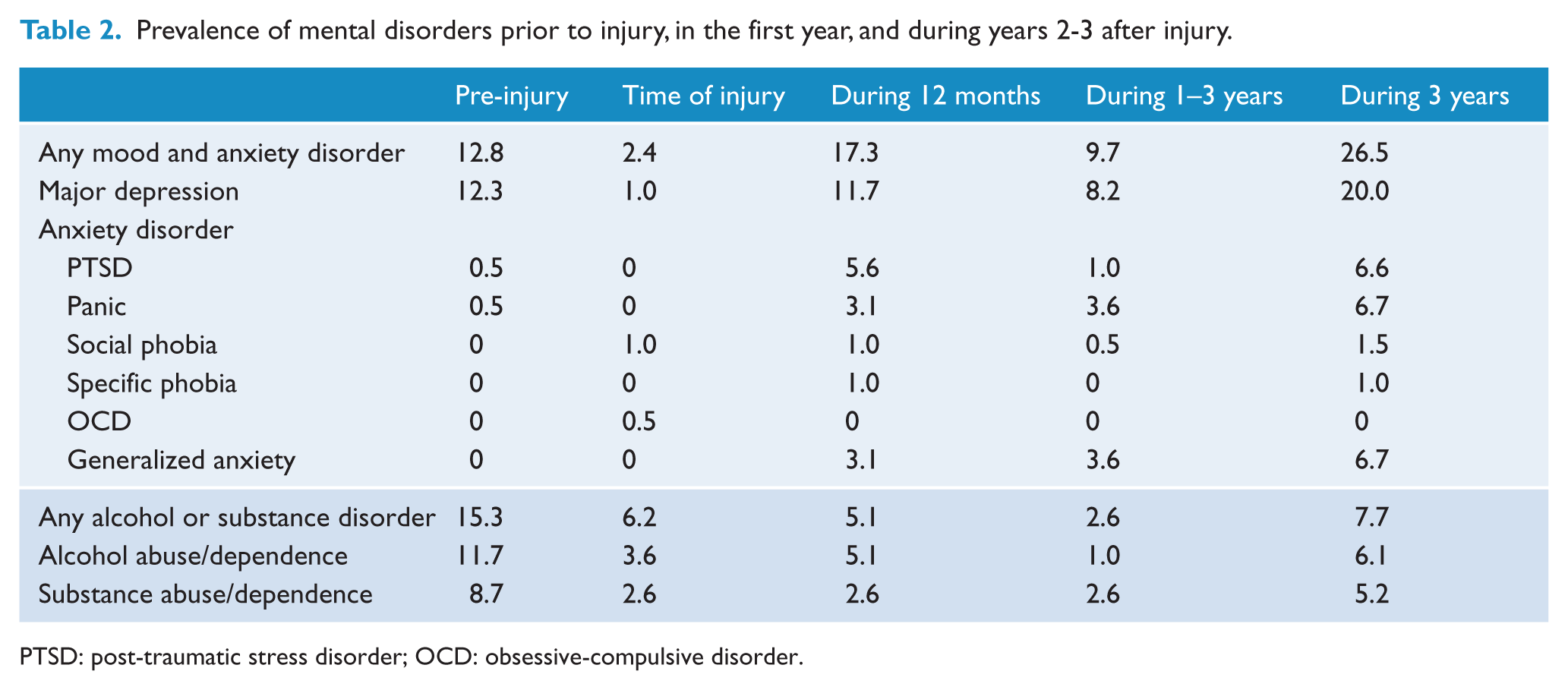
PTSD: post-traumatic stress disorder; OCD: obsessive-compulsive disorder.
In the first step of the logistic regression analyses, the parameters with a bivariate correlation p <0.15 with a mental disorder in the first 12 months were: pre-injury – past depressive feelings, past psychological help, family history of mental disorder or depression, past history of any mental health disorder, major depression, alcohol or substance use disorders; injury – higher total and lower limb injury severity; peri-injury – higher event severity, anxiety symptoms, re-experiencing and lower expectation of recovery; 12 months post-injury – higher pain and physical disability, decreased social support and compensable injury. For late-onset mental disorder, those with a bivariate correlation p <0.15 were: pre-injury – past traumatic events, family history of mental disorder; peri-injury – higher event severity; 12 months post-injury – higher pain and physical disability, and a compensable injury (Table 3).
Bivariate associations for early (first 12 months) and late (1–3 years) onset mental disorder after serious injury.
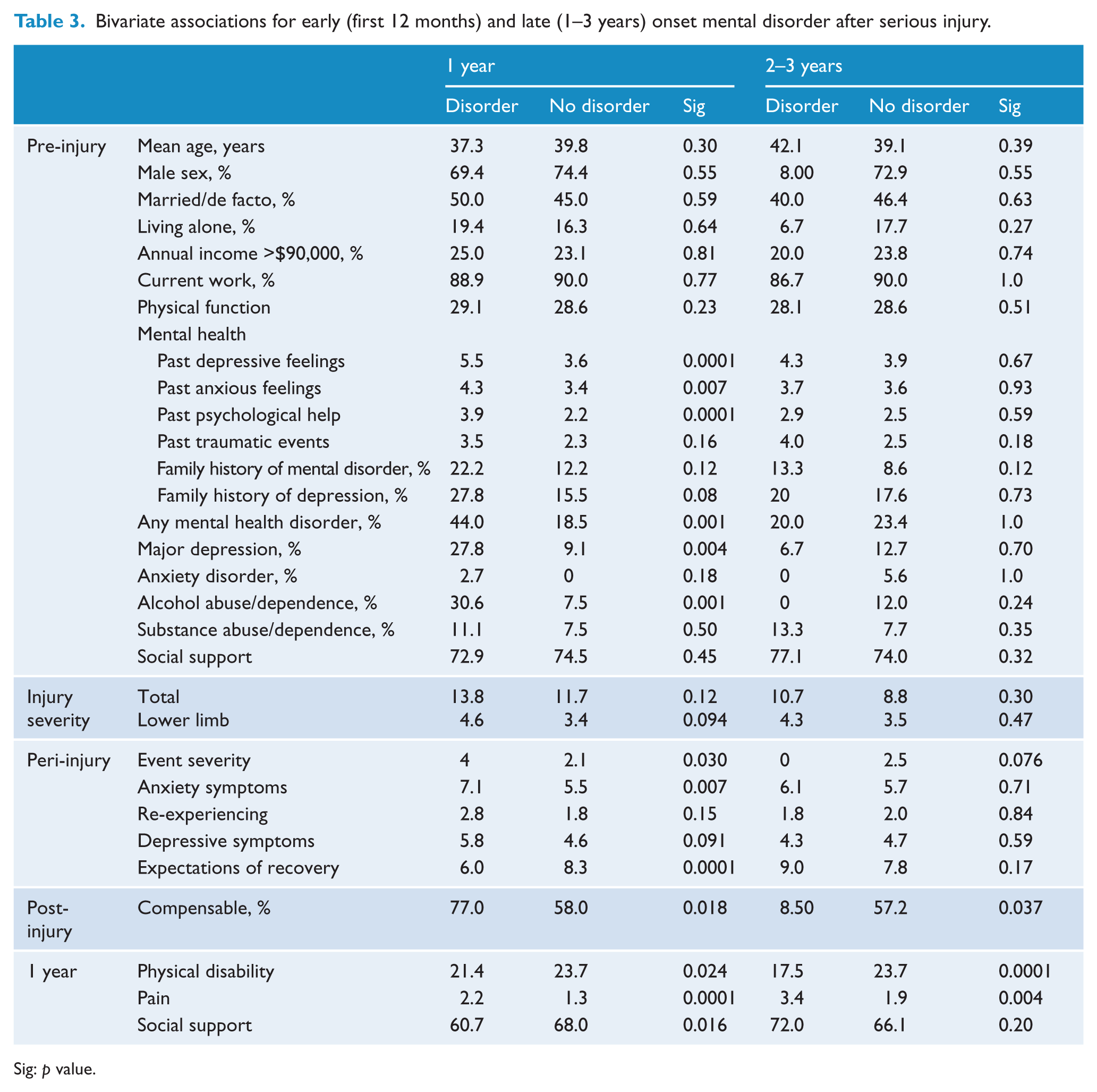
Sig: p value.
In the final regression models, past psychological help and pain severity were associated with mental disorder in the first 12 months (Table 4). Physical disability was an independent risk factor for late-onset mental disorder (Table 5).
Multiple regression model for early mental disorder (first 12 months) after serious injury.
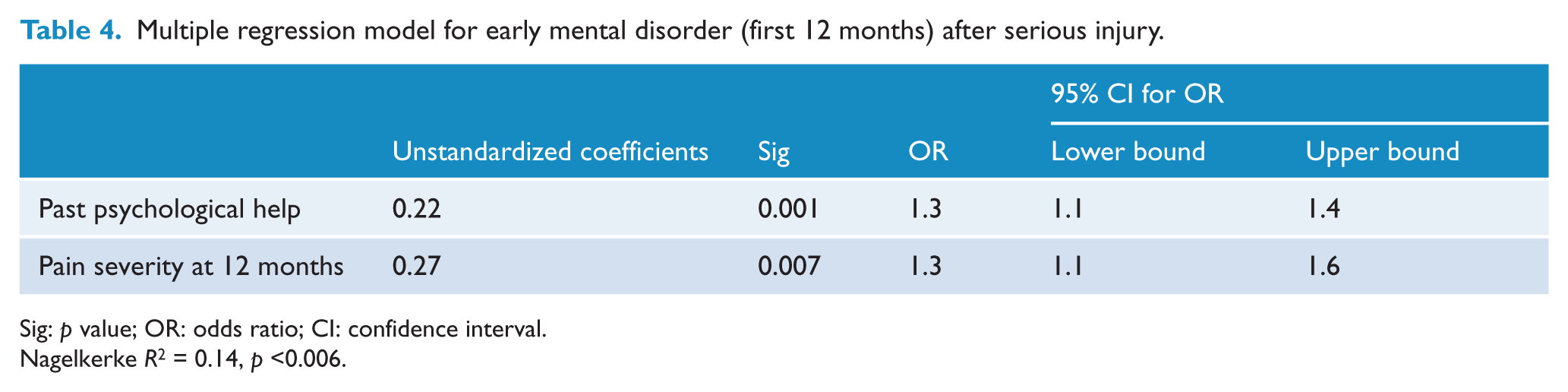
Sig: p value; OR: odds ratio; CI: confidence interval.
Nagelkerke R2 = 0.14, p <0.006.
Multiple regression model for late-onset mental disorder (1–3 years) after serious injury.
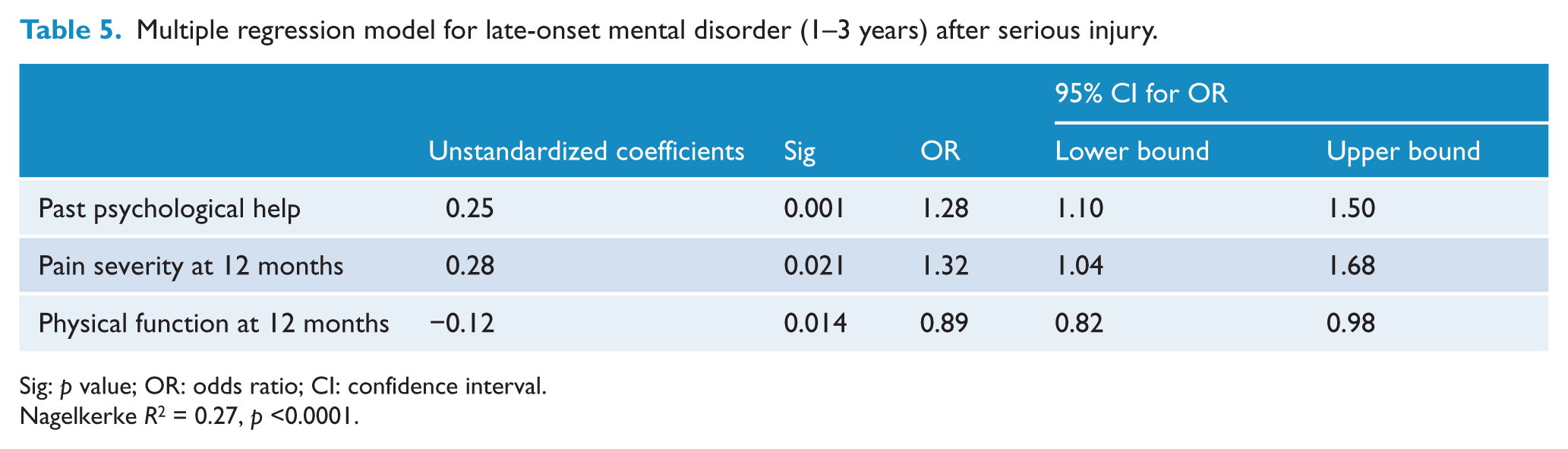
Sig: p value; OR: odds ratio; CI: confidence interval.
Nagelkerke R2 = 0.27, p <0.0001.
Discussion
The psychiatric consequences of serious injuries extend beyond 1 year. More than a quarter of injury survivors experience a mood or anxiety disorder in the 3 years after injury; a third of these emerging after 1 year. The most common late-onset disorders are major depression and non-PTSD anxiety disorders – persistent physical disability emerging as an independent risk factor for their occurrence. These findings suggest that different mental disorders, related to different risk factors, occur at different stages following serious injury.
The prevalence of mental disorder found at 12 months was largely consistent with previous studies. The main differences with those reported by Bryant et al. (2010) were a lower prevalence of PTSD and generalised anxiety disorder. This may be explained by the use of different semi-structured diagnostic interviews. All the risk factors previously identified for major depression and PTSD at 12 months (Table 1) were replicated at a bivariate level. Neither of the factors present in the general population, but not previously tested in injury cohorts (family history, lower social support) were significant in post injury. Although in keeping with self-reported past psychiatric history identified in previous studies (Bryant et al., 2010; O’Donnell et al., 2004a), the form of pre-injury vulnerability most strongly associated with later mental disorder in our study was receipt of past psychological help. This finding may suggest that mental disorder of a severity leading to engagement with treatment services is of greater significance in predicting future problems than past mental disorder alone. Overall, the predicative power of the multivariate models was moderate, reflecting the limitations of the actuarial method, the unpredictable nature of psychological responses and the confounding effect of acute hospital and post-discharge events.
Pain severity was associated with both early and later-onset mental disorder. The relationship between pain and mental disorder has been well established in a range of settings (Demyttenaere et al., 2007), although there is less certainty about the nature and direction of this relationship (Nicholas et al., 2009). On one hand, the distress of persistent pain interacting with individual and social vulnerability may precipitate an episode of mental disorder. On the other, mental disorder may contribute to the pathogenesis and experience of the pain. In our population, both mechanisms are likely to be occurring in the first 12 months. The modelling of mental disorder after 12 months (Table 5), however, is more supportive of the second mechanism.
The most common new diagnoses commencing after 12 months were major depression and non-PSTD anxiety disorders. The factor uniquely associated with their onset was persistent poor physical function. In older populations, functional impairment, alongside chronic illness and cognitive decline, predisposes major depression (Turvey et al., 2009), with some authors believing it to be the predominant factor (Braam et al., 2005). In the case of injury, physical disability is particularly associated with certain types of injury; in particular, spinal cord injury, lower extremity injury, or brain (Holtslag et al., 2007). These injures have been associated with higher rates of mental disorder (McCarthy et al., 2003; Ponsford et al., 2008), with persistent disability emerging as a potential mediating factor. In contrast to the mental disorders aetiologically related to traumatic events, those related to disability are more likely to be delayed in their onset.
The strengths of this study lie in its prospective design, timeframe, use of ‘gold standard’ diagnoses, measurement of covariates and high rates of follow up. The sample size did not allow for analysis of risk factors for individual disorders, although the significance of this is qualified by the high degree of co-morbidity. Patterns of injury type and intentionality will differ, especially internationally, as will the nature of medical and psychological services, and should be considered when interpreting the data.
This study provides empirical support to the common clinical experience that psychiatric disorders, both new and persistent, extend beyond 1 year after injury. Although an understandable focus needs to be placed on the early detection and treatment of mental disorders after injury, ongoing monitoring is required for new episodes, especially in those individuals with persistent pain and physical disability.
Footnotes
Author contribution statement
All authors were involved in the design, implementation and data analysis of the study and the preparation of the paper. AH had a key co-ordinating role and took a lead role in data analysis.
Funding
This study was conducted with funds from the Neurotrauma Initiative following a competitive grant process.
Declaration of interest
MH has received honoraria from Mundipharma. AH has received a grant from the Neurotrauma Initiative in order to conduct this trial. The remaining authors declare no conflict of interest.