
Abstract
Objective:
Smoke-free policies have been introduced in inpatient psychiatric facilities in most developed nations. Such a period of supported abstinence during hospitalization may impact smoking behaviours post discharge, yet little quantitative evidence exists. The aim of this review was to provide the first synthesis of the research evidence examining the impact of a smoke-free psychiatric hospitalization on patients’ smoking-related behaviours, motivation, and beliefs.
Methods:
We conducted a systematic review of electronic databases PubMed, MEDLINE, PsycINFO, and EMBASE from inception to June 2013. Studies were included if they were conducted in an inpatient psychiatric facility with a smoke-free policy and if they examined any change in patients’ smoking-related behaviours, motivation, or beliefs either during admission, post discharge, or both. Risk of bias was assessed using the Cochrane Collaboration Risk of Bias Tool.
Results:
Fourteen studies were included in the review. Of the four studies that assessed change in smoking from admission to post discharge, two indicated a significant decline in cigarette consumption up to 3 months post discharge. Positive changes in motivation to quit and beliefs about quitting ability were identified in two studies. One study reported an increase in the rate of quit attempts and one reported a decline in nicotine dependence levels.
Conclusions:
A smoke-free psychiatric hospitalization may have a positive impact on patients’ smoking-related behaviours, motivation, and beliefs, both during admission and up to 3 months post discharge. Further controlled studies with more rigorous designs are required to confirm this potential.
Introduction
Smoking remains the leading preventable cause of death and disease in Western nations (US Department of Health and Human Services, 2004). People with a mental disorder smoke at higher rates (Lawrence et al., 2009; Morgan et al., 2012), are more dependent on nicotine (Australian Institute of Health and Welfare, 2007), and are less likely to quit than the general population of smokers (Diaz et al., 2006; Hagman et al., 2008). As a result, persons with a mental disorder are more likely to suffer smoking-related diseases, and consequently die 12–15 years earlier than persons without such disorders (Lawrence et al., 2013). Some of the highest levels of smoking have been observed among patients hospitalized for psychiatric treatment (Benowitz et al., 2009; Lineberry et al., 2009).
Smoking bans have been introduced in general hospital settings in a number of countries (House of Commons Health Committee, 2005). Such bans seek to protect patients, staff, and visitors from the harmful effects of second hand smoke exposure (Tobacco Advisory Group, 2005) and have been found to be associated with reductions in staff smoking (Callinan et al., 2010; Fathallah et al., 2012). In addition, clinical practice guidelines recommend the provision of behavioural and pharmacological nicotine dependence treatment in order to manage the impacts of smoking bans for patients and to aid the likelihood of their successful smoking cessation (Fiore et al., 2008). Evidence from general hospital settings suggests that a period of such supported abstinence during a smoke-free hospitalization may be beneficial in increasing motivation to quit (Williams and Jones, 2012) and the likelihood of remaining abstinent for up to 12 months post discharge (Duffy et al., 2010; Rigotti et al., 2000; Williams and Jones, 2012). Recent systematic review evidence further suggests that the provision of nicotine replacement therapy (NRT) and smoking cessation counselling during a smoke-free hospitalization can increase patient cessation rates by 54% at 12 months post discharge (Rigotti et al., 2012).
Clinical practice guidelines similarly recommend the introduction of smoke-free policies incorporating complete smoking bans and the provision of nicotine dependence treatment within psychiatric facilities (American Psychiatric Association, 1996; Tobacco Advisory Group, 2005). While the introduction of smoking bans in these settings has often been delayed and/or reported to be difficult (Campion et al., 2008; Ratschen et al., 2009), evidence suggests that when staff leadership is cohesive, enforcement of the ban is consistent, and appropriate nicotine dependence treatment is systematically provided to patients, smoking bans have not led to increased patient aggression or discharge against medical advice (Lawn and Campion, 2010; Lawn and Pols, 2005; Moss et al., 2010).
Although a smoke-free psychiatric hospitalization may positively impact on patients’ smoking behaviours, as evidenced among smokers in general hospital settings (Duffy et al., 2010; Rigotti et al., 2000; Williams and Jones, 2012), few studies have examined the impact of a smoke-free psychiatric hospitalization on patients’ smoking outcomes. The aim of this systematic review was to provide the first synthesis of the evidence examining the impact of smoke-free policies on patient smoking behaviours, motivation, and beliefs both during and post discharge from an inpatient psychiatric facility.
Methods
A systematic review was conducted in June 2013 in line with the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) statement (Moher et al., 2009). A PRISMA checklist for the review is included in Supplementary Table A1 (Appendix 1, available online). The electronic databases PubMed, MEDLINE, PsycINFO, and EMBASE were searched from inception to June 2013 using the following terms: “smoking” AND “psychiatric department, hospital” AND “patient discharge”, “tobacco” AND “mental health” AND “admission” OR “discharge”, “psychiatric” AND “smoke-free policy” OR “smoking ban” AND “inpatient”, “smoking” AND “mental health” AND “hospitalized”, “smoking” AND “psychiatric” AND “restricted”, “tobacco dependence treatment” AND “psychiatric” AND “hospital”, and “smoking cessation treatment” AND “psychiatric” AND “hospital”. Individual searches of each database were conducted and the results combined. Results were restricted to studies with humans and those written in English. Articles were excluded if they did not report original data (e.g. review articles). The reference lists of prior reviews and key articles were searched for papers relevant to the study aims.
This review is registered on the National Institute for Health Research international prospective register of systematic reviews (PROSPERO; registration number CRD42012002770; available at www.crd.york.ac.uk/PROSPERO/).
Included papers were required to examine changes in patients’ reported smoking-related behaviours (including abstinence from cigarettes, quit attempts, cigarette consumption, nicotine dependence, and use of smoking cessation supports), motivation, or beliefs during or following an admission to an adult inpatient psychiatric facility with a policy incorporating restrictions on smoking. Papers were excluded if they surveyed clinical staff only. Study findings were examined with regard to risk of bias (Higgins and Green, 2011) and with respect to a number of aspects of smoke-free policies, including: the nature of the smoking restrictions (“complete – all buildings and grounds”, “incomplete with smoking permitted outdoors”, “incomplete with smoking permitted indoors”, or “incomplete with smoking permitted in designated rooms or at designated times”); adherence to such restrictions (“adherence evident”, “non-adherence evident”, or “not reported”); and provision of nicotine dependence treatment (“psychological only”, “pharmacological only”, “combined”, or “not reported”).
A data extraction form was developed based on guidance literature (Popay et al., 2006) with data being extracted independently by the first and second authors (EAS and JAB) and analysed by systematic narrative synthesis.
Assessment of risk of bias
Risk of bias in the included studies was examined using the Cochrane Collaboration tool for assessing risk of bias (Higgins and Green, 2011). The tool comprises five domains of bias: selection, performance, detection, attrition, and reporting, with a sixth domain for “other biases”. Reviewers are required to make a judgement of risk of bias with supporting statements for each domain (“low risk”, “high risk”, or “risk unable to be determined”). Given this review was not limited to randomized controlled trials, the tool was modified by the study authors for the purpose of assessing nonrandomized and noncomparative studies. For assessing selection bias, the categories “random sequence generation” and “allocation concealment” were replaced with “comparability of groups” (in the case of studies with multiple groups) and “sample representativeness”, respectively. Comparability of groups included an examination of whether the authors provided adequate detail that the groups were comparable on relevant prognostic factors at baseline (e.g. age, gender, length of admission, level of smoking, psychological distress). Sample representativeness included an examination of whether the authors provided adequate detail that the included sample was representative of the target population. Given that participants in the included studies would most likely be aware of the hospital’s smoke-free policy (i.e. not blinded to the intervention), the domains for performance and detection bias were combined into a single domain named “blinding”, which assessed blinding of outcome assessors. For the other domains, criteria for determining risk of bias were retained as per the original tool (Higgins and Green, 2011). Risk of bias was assessed independently by the first author (EAS) and by a research assistant, and discrepancies were resolved via consensus with the second author (JAB). Assessors were not blinded to study authors, institution, or journal as they were familiar with the literature. No studies in the review were excluded from the narrative synthesis on the basis of risk of bias.
Results
Figure 1 describes the results of the search and paper selection process. The search identified a total of 334 papers, of which 156 were unique, and 178 were duplicates. By reviewing the title, abstracts and reference lists of the 156 papers, 86 were identified as potentially relevant and 70 were excluded as they were not relevant to the search topic. The first author reviewed the 86 articles and their reference lists, resulting in 71 being excluded (25 did not examine patients’ smoking-related behaviours, 21 in inpatient psychiatric facilities without a smoke-free policy, 21 no original data, four surveyed clinical staff only). The remaining 15 publications (based on 14 studies) were included in this review (Table 1). As the publication by Shmueli et al. (2008) reported on the same sample as Prochaska et al. (2006), both papers were considered as one study and have been cited as the earlier study.
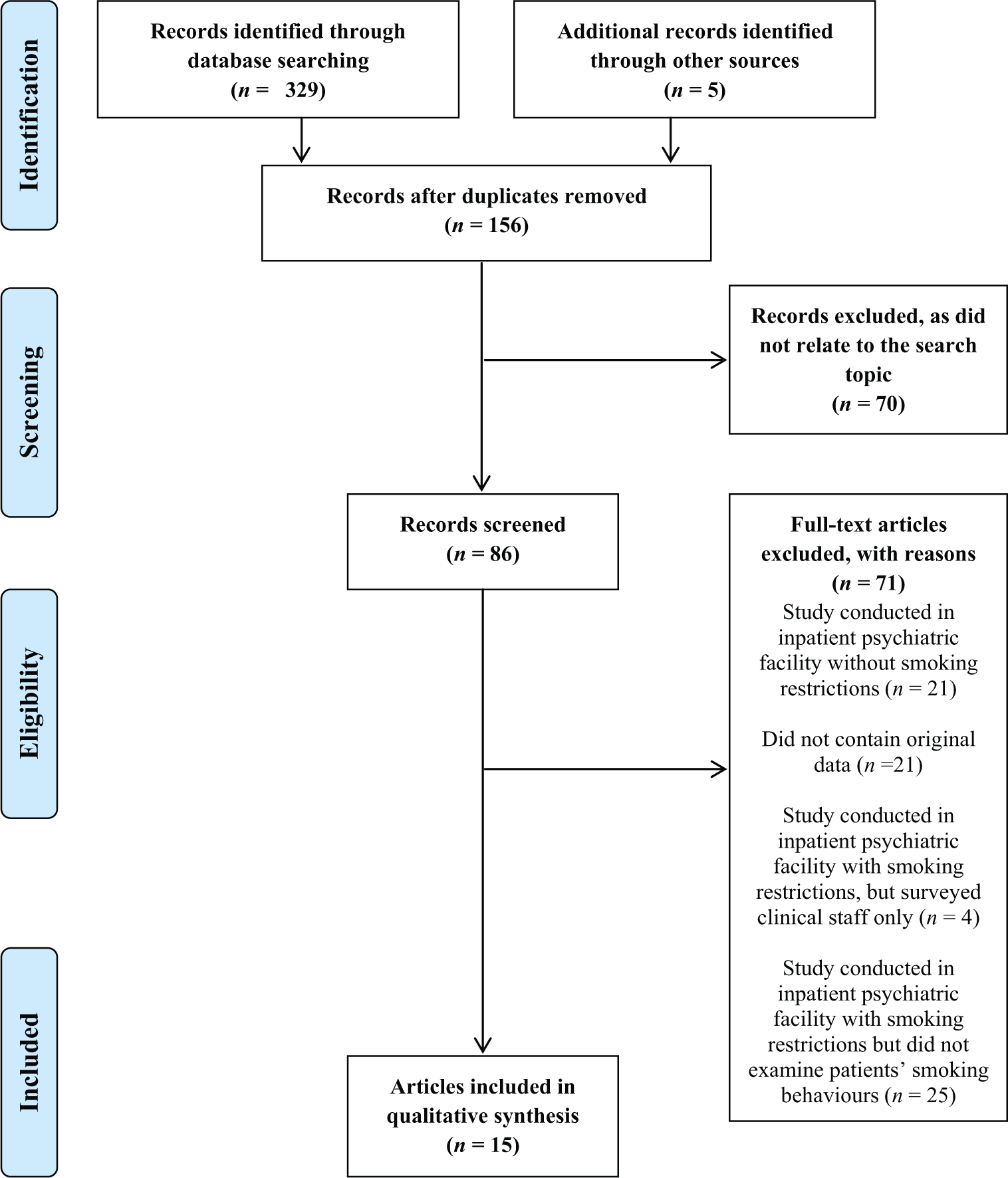
PRISMA flowchart of the study selection process.
Characteristics and findings of studies included in the review.

FTND, Fagerstrom Test for Nicotine Dependence (Fagerstrom et al., 1996); HSI, Heaviness of Smoking Index (Kozlowski et al., 1994); NRT, Nicotine Replacement Therapy; NWC, Nicotine Withdrawal Checklist (Shiffman et al., 2002); PRN, Pro re nata (as needed); SCS, Stages of Change scale (DiClemente et al., 1991); TAQ, Thoughts about Abstinence Questionnaire (Hall et al., 1990).
Study characteristics
A description of the 14 included studies is provided in Table 1 regarding: study location, design, setting, and sample; the nature of the smoke-free policy (including the type of smoking restriction, adherence with the policy, and provision of nicotine dependence treatment); the smoking-related outcomes assessed and measures used, and the study findings.
Seven studies were conducted in the USA (Downey et al., 1998; Jones et al., 2004; Patten et al., 1995; Prochaska et al., 2006; Resnick and Bosworth, 1989; Smith and Grant, 1989; Smith et al., 2012), three in Switzerland (Etter et al., 2008; Keizer and Eytan, 2005; Keizer et al., 2009), two in the UK (Ratschen et al., 2010; Smith and O’Callaghan, 2008), and two in Australia (Hehir et al., 2012; Siru et al., 2010). None of the studies involved randomized controlled trials. Six studies were conducted as cross-sectional surveys at a single time point (Hehir et al., 2012; Keizer and Eytan, 2005; Ratschen et al., 2010; Smith and Grant, 1989; Smith and O’Callaghan, 2008; Smith et al., 2012) and four as cross-sectional surveys at multiple time points in the same facility and at various stages of smoke-free policy implementation (Etter et al., 2008; Keizer et al., 2009; Patten et al., 1995; Resnick and Bosworth, 1989). Four studies used repeated-measures designs, two of which examined changes in smoking-related behaviours over time in a single group (Jonas and Eagle, 1991; Prochaska et al., 2006) and two examined changes in smoking-related behaviours over time in two groups (Downey et al., 1998; Siru et al., 2010), one of which used general hospital patients as a comparison group (Siru et al., 2010). The number of patients included in the studies ranged from 15–467. Where reported, length of admission ranged from 1–990 days.
Level of smoking restriction in place and adherence
Six studies were conducted in facilities with complete smoking bans (Hehir et al., 2012; Jonas and Eagle, 1991; Prochaska et al., 2006; Ratschen et al., 2010; Siru et al., 2010; Smith et al., 2012), and eight in facilities with incomplete bans, four of which banned smoking indoors only (Etter et al., 2008; Patten et al., 1995; Resnick and Bosworth, 1989; Smith and Grant, 1989), three restricted smoking to designated smoking rooms (Keizer and Eytan, 2005; Keizer et al., 2009; Smith and O’Callaghan, 2008), and one restricted smoking to five predetermined intervals per day (Downey et al., 1998). Five studies were conducted in facilities which introduced or had a change in a smoke-free policy during the study period from none/minimal to more thorough restrictions on smoking (Downey et al., 1998; Etter et al., 2008; Keizer and Eytan, 2005; Keizer et al., 2009; Patten et al., 1995; Resnick and Bosworth, 1989).
Of the six studies conducted in facilities with complete bans, one indicated that all participants abstained from smoking during admission (Jonas and Eagle, 1991) and two indicated some level of nonadherence (Ratschen et al., 2010; Smith et al., 2012). Of the eight studies conducted in facilities with incomplete bans, five indicated some level of nonadherence (Etter et al., 2008; Patten et al., 1995; Resnick and Bosworth, 1989; Smith and Grant, 1989; Smith and O’Callaghan, 2008). Six studies did not provide comment on policy adherence (Downey et al., 1998; Hehir et al., 2012; Keizer and Eytan, 2005; Keizer et al., 2009; Prochaska et al., 2006; Siru et al., 2010). Evidence of nonadherence typically comprised patient self-report that they themselves had smoked in prohibited areas of the facility (Ratschen et al., 2010; Smith and Grant, 1989; Smith and O’Callaghan, 2008), were aware of family or friends smuggling cigarettes onto the ward (Resnick and Bosworth, 1989), were exposed to continued smoking by other patients (Smith et al., 2012), or were aware of sharing of cigarettes between patients or between patients and staff (Etter et al., 2008). One study used medical records to identify that several patients had smoked in a prohibited area during their admission (Patten et al., 1995).
Provision of nicotine dependence treatment
In ten of the 14 studies, facilities were reported as providing nicotine dependence treatment to patients as part of routine care, including NRT and brief advice to quit (Etter et al., 2008; Hehir et al., 2012; Jonas and Eagle, 1991; Patten et al., 1995; Prochaska et al., 2006; Ratschen et al., 2010; Resnick and Bosworth, 1989; Siru et al., 2010; Smith and Grant, 1989; Smith et al., 2012). In six of these, complete smoking bans were implemented (Hehir et al., 2012; Jonas and Eagle, 1991; Prochaska et al., 2006; Ratschen et al., 2010; Siru et al., 2010; Smith et al., 2012) and smoking was banned indoors only for the remaining four facilities (Etter et al., 2008; Patten et al., 1995; Resnick and Bosworth, 1989; Smith and Grant, 1989). None of the four studies that were conducted in facilities which permitted smoking in designated rooms or at designated times reported the provision of routine nicotine dependence treatment (Downey et al., 1998; Keizer and Eytan, 2005; Keizer et al., 2009; Smith and O’Callaghan, 2008). Rates of receipt of nicotine dependence treatment are provided in Table 1 and, overall, indicate suboptimal treatment.
Risk of bias in included studies
Supplementary Figure A1 and Supplementary Table A2 (Appendix 1) describe the assessed risk of bias for each included study. Most studies were small, and incomplete in their reporting of outcomes. Consequently, risk of bias was mostly unable to be determined, or determined to be high. Only studies large enough to report statistical comparisons are considered in depth below (in addition to information already provided in Table 1).
Changes in smoking behaviour during admission
Facilities with complete smoking bans
Two studies with complete smoking bans assessed smoking behaviour during admission (Ratschen et al., 2010; Smith et al., 2012), with one of these (Smith et al., 2012) large enough to conduct statistical comparisons. The study conducted by Smith et al. (2012) indicated that patients’ cigarette consumption was significantly lower during admission than pre-admission (p<0.05). Although combined nicotine dependence treatment was available, usage was not reported (Smith et al., 2012).
Facilities with incomplete smoking bans
Of the three studies with indoor smoking bans that examined changes in smoking behaviour during admission (Etter et al., 2008; Patten et al., 1995; Smith and Grant, 1989), only one conducted a statistical analysis of the results. Etter et al. (2008) reported a significantly larger proportion of participants making a quit attempt, from 2.2% when smoking was permitted in designated rooms to 18.4% when smoking was banned indoors (p=0.01; Table 1; Etter et al., 2008). Although the increased proportion of participants making a quit attempt in this study was accompanied by an increase in patients receiving NRT and advice to quit (both p<0.001), nonadherence to the policy was reported (Etter et al., 2008).
Three studies with designated smoking rooms examined changes in smoking behaviour during admission (Keizer and Eytan, 2005; Keizer et al., 2009; Smith and O’Callaghan, 2008). Of these, two reported statistical analyses. Keizer and Eytan (2005) reported that relative to pre-admission, 43.2% of patients increased and 27.3% decreased their daily cigarette consumption during admission (Keizer and Eytan, 2005). These rates were 25.5% and 37.3%, respectively, in the 2009 follow-up study (Keizer et al., 2009), with changes reaching significance for heavy smokers (p=0.001; Table 1; Keizer et al., 2009).
Changes in smoking behaviour post discharge
Facilities with complete smoking bans
Four studies with complete smoking bans examined changes in smoking behaviours post discharge (Hehir et al., 2012; Jonas and Eagle, 1991; Prochaska et al., 2006; Siru et al., 2010). All three studies that used repeated-measures designs to examine smoking from admission to discharge reported that the majority (89.6%, Siru et al., 2010; 80%, Jonas and Eagle, 1991; 76%, Prochaska et al., 2006) of participants resumed smoking within 5 days post discharge (Table 1). However, both the more recent and larger studies reported significant reductions in daily cigarette consumption at 14 days (Siru et al., 2010) and 3 months (Prochaska et al., 2006) post discharge relative to pre-admission levels. Both were conducted in facilities that provided combined nicotine dependence treatment, with the majority of participants in both studies having used NRT during admission (60%, Siru et al., 2010; 70%, Prochaska et al., 2006); however, receipt of advice to quit was low (2%, Prochaska et al., 2006; 20%, Siru et al., 2010) and neither study provided details of smoke-free policy adherence. Jonas and Eagle (1991) reported no change in cigarette consumption from the time of admission to 6–18 months post hospitalization. Of these three studies, only one study biochemically validated self-reported abstinence, reporting that 4% of participants were abstinent at 3 months post discharge (Prochaska et al., 2006), and self-reported abstinence was 10.3% at 8 weeks in one study (Jonas and Eagle, 1991), and 6.3% at 6 months post discharge in the other (Siru et al., 2010). The remaining study reported that 58% of patients (n=12) were abstinent post discharge; however, this study was of cross-sectional design, had a small sample size, and patients were discharged to the care of facilities that imposed smoking restrictions and provided combined nicotine dependence treatment and thus were effectively still in institutional care (Hehir et al., 2012).
Facilities with incomplete smoking bans
Patten et al. (1995) reported that all participants (n=15) resumed smoking immediately after discharge; however, 5.3% self-reported abstinence at 16–18 months. This study reported provision of combined nicotine dependence treatment, with 26% of participants reporting using NRT during admission; however, nonadherence with the smoke-free policy was evident.
Changes in smoking-related motivations or beliefs during admission
Facilities with complete smoking bans
Four studies with complete smoking bans examined smoking-related motivations or beliefs during admission (Hehir et al., 2012; Prochaska et al., 2006; Ratschen et al., 2010; Siru et al., 2010). Of these, the only study to examine such changes using a repeated-measures design and statistical analyses reported that participants expected to be significantly more successful (p<0.05), and perceived significantly less difficulty in staying quit following a quit attempt at discharge compared to on admission (p<0.01; Prochaska et al., 2006). In this study, the majority of participants (70%) used NRT during hospitalization, and nicotine doses predicted these increased expectations of success with quitting (p<0.05; Table 1; Prochaska et al., 2006).
Facilities with incomplete smoking bans
Four studies with incomplete smoking bans examined smoking-related motivations or beliefs during admission (Downey et al., 1998; Keizer et al., 2009; Resnick and Bosworth, 1989; Smith and Grant, 1989). In the largest and most recent study, Keizer et al. (2009) found a significantly larger proportion of participants in the contemplation and preparation/decision stages of change when smoking was unrestricted (4.9%) as compared to when smoking was permitted only in designated rooms (18.5%; p=0.02), indicating an increase in motivation to quit. However, authors did not report provision of nicotine dependence treatment, or adherence to the smoking ban. In the earlier study of Downey et al. (1998) which permitted smoking at designated times, participants admitted to the facility during the “restricted” period when smoking was limited to five intervals per day reported a significant decline on the “action” stage of change scale from admission to discharge, suggesting a decline in motivation to quit. However, participants admitted during the unrestricted “ad lib” period reported a significant increase in motivation to quit (p<0.05). In the two older and smaller cross-sectional studies with indoor bans, the majority of patients reported that the smoke-free policy would lead them to reduce their smoking or to try to quit post discharge (Resnick and Bosworth, 1989; Smith and Grant, 1989). In both studies, nicotine gum was made available to patients; however, rates of receipt were not reported and nonadherence to the smoke-free policy was evident (Resnick and Bosworth, 1989; Smith and Grant, 1989).
Discussion
The findings of this review suggest that a smoke-free psychiatric hospitalization may have the potential to impact positively on patients’ smoking behaviours and on smoking-related motivation and beliefs. Positive changes in smoking-related outcomes identified included declines in daily cigarette consumption post discharge (Prochaska et al., 2006; Siru et al., 2010), increases in patients’ motivation to quit (Keizer et al., 2009; Prochaska et al., 2006), and an increase quit attempts (Etter et al., 2008); however, one older study indicated a decline in motivation to quit (Downey et al., 1998). Of the 14 included studies, many were small and incomplete in their reporting of outcomes, thus limiting the ability to draw firm conclusions regarding the impact of smoking bans on patients smoking behaviour.
Recently conducted, larger studies appeared more likely to have been undertaken in facilities with comprehensive restrictions on smoking and which provided combined pharmacological and behavioural nicotine dependence treatment. These studies also appeared to be associated with more positive smoking outcomes; however, limitations in the data available precluded any quantitative assessment of this trend. Studies conducted in the 1980s and 1990s being undertaken at a time where smoking restrictions were still being introduced in general medical settings and rare in inpatient psychiatric facilities may have some bearing on this finding (House of Commons Health Committee, 2005). Specifically, both studies that reported significant declines in patients’ daily cigarette consumption up to 3 months post discharge were conducted more recently, and in facilities with complete smoking bans and concurrent provision of combined pharmacological and behavioural nicotine dependence treatment (Prochaska et al., 2006; Siru et al., 2010). Furthermore, two studies reported more positive smoking outcomes when stricter smoking rules were introduced, including significantly larger proportions of patients making a quit attempt (Etter et al., 2008) and reporting a desire to quit (Keizer et al., 2009). Additionally, in one of these studies, the larger proportion of patients making a quit attempt was accompanied by higher rates of patients receiving NRT and advice to quit (Etter et al., 2008). Conversely, of the four studies conducted in facilities that permitted smoking in designated rooms or at designated times, three reported increases in cigarette consumption (Keizer and Eytan, 2005; Keizer et al., 2009; Smith and O’Callaghan, 2008) and one reported a reduction in motivation to quit (Downey et al., 1998). None of these four studies reported provision of nicotine dependence treatment, and one study suggested continued exposure to cigarette smoke on the unit, despite the introduction of the smoking restrictions (Smith and O’Callaghan, 2008). These findings also suggest that adherence to the smoking ban and receipt of nicotine dependence treatment during a smoke-free psychiatric hospitalization may be important factors that influence patients’ smoking behaviours, as evidenced in general medical settings (Rigotti et al., 2000; Williams and Jones, 2012).
The findings of this review suggest that smoking bans generally, and complete bans in particular, may have a beneficial effect in terms of helping patients initiate changes in their smoking behaviour. However, none of the identified studies suggested significant increases in smoking cessation post discharge. Such findings suggest that the smoking bans, of either form, may have had a limited long-term beneficial effect. The extent to which such outcomes were a function of the effectiveness of smoking bans per se or of the manner of their implementation in the specific study facilities is unknown as the included studies did not adequately describe the extent of smoke-free policy adherence and provision of nicotine dependence treatment, key determinants of the likely success of a smoking ban (Bowman and Stockings, 2012; Lawn and Campion, 2010; Rigotti et al., 2000). Where these details were reported, patient receipt of NRT and brief advice to quit were suboptimal, and in half the studies, smoking continued to occur on the unit despite the smoking restrictions (Etter et al., 2008; Patten et al., 1995; Ratschen et al., 2010; Resnick and Bosworth, 1989; Smith and Grant, 1989; Smith and O’Callaghan, 2008; Smith et al., 2012), which may have impacted post-discharge smoking behaviours The limited findings for cessation post discharge should also be considered in light of the knowledge that smokers with a mental disorder have greater difficulty in quitting than the general population (Cooper et al., 2012), and as such it is not surprising that few participants successfully abstained from smoking without further cessation aids post discharge. These findings are consistent with previous research conducted in general medical settings indicating that a post-discharge effect on smoking rates is most likely to occur when cessation support is provided to patients post discharge, in addition to that provided during the inpatient stay (Rigotti et al., 2012). Consequently, the positive changes in smoking behaviour identified in this review are perhaps of greater importance, particularly so given that no studies reported that the purpose of the smoking restrictions were to encourage cessation post discharge. These findings further highlight the opportunity provided by a smoke-free psychiatric admission in initiating smoking cessation treatment among smokers with a mental disorder.
An important limitation of this review is the lack of adequately powered, high-quality, controlled studies in this field, which precluded any quantitative examination of the results. Ideally, future research in this area should describe the level of smoking restriction imposed and the nicotine dependence treatment routinely provided by the facility. Patient receipt of nicotine dependence treatment (including the type(s) of NRT used, daily dosage, and length of use), its adequacy in managing nicotine withdrawal, and details of patient adherence to the smoking restrictions should be collected either through medical record audit, patient observation, or self-report. Examination of such factors may assist in developing a greater understanding of the potential impact of admission to a smoke-free hospital on patients’ post-discharge smoking behaviour.
Consistent with health policy initiatives, total smoking bans in general medical settings reduce second-hand smoke exposure (Tobacco Advisory Group, 2005) and are associated with reductions in smoking and improvements in health behaviour among staff and clients (Duffy et al., 2010; Gadomski et al., 2010). Psychiatric treatment settings carry equal legislative responsibility to provide a safe and healthy environment for their staff and clients (Tobacco Advisory Group, 2005). Implementation of total smoking bans in inpatient psychiatric settings, including routine identification and treatment of tobacco use, is imperative in achieving this goal (Royal College of Physicians and Royal College of Psychiatrists, 2013) and for providing an opportunity for patients to address their tobacco smoking in a supportive environment (Prochaska, 2009). However, it is apparent that continued cessation support following discharge is needed to increase the likelihood of cessation being maintained.
Footnotes
Acknowledgements
EAS is supported by an Australian Postgraduate Award. The authors would like to thank Miss Jane Goodwin and Dr Luke Wolfenden for their assistance with the risk of bias assessment.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.