
Abstract
Background:
Patients with psychiatric illness have increased somatic morbidity and increased mortality. Knowledge of how to integrate the prevention and care of somatic illness into the treatment of psychiatric patients is required. The aims of this study were to investigate whether an intervention programme to improve physical health is effective.
Methods:
An extension of the European Network for Promoting the Health of Residents in Psychiatric and Social Care Institutions (HELPS) project further developed as a 12-month controlled cluster-randomized intervention study in the Danish centre. Waist circumference was a proxy of unhealthy body fat in view of the increased risk of cardiovascular diseases and type 2 diabetes.
Results:
Waist circumference was 108 cm for men and 108 cm for women. Controlled for cluster randomization, sex, age, and body fat, the intervention group showed a small, but not significant, reduction in waist circumference, while participants in the control group showed a significant increase in waist circumference.
Conclusions:
The intervention had a positive effect on the physical health of the patients measured by a reduction in the increase of waist circumference.
Keywords
Introduction
The prevalence of physical health problems among patients suffering from severe mental illnesses is higher than that seen in the rest of the population. Cardiovascular disease (CVD) and metabolic syndrome are common in those diagnosed with schizophrenia, a fact that has been known for some time (Brown, 1997; De Hert et al., 2011a). There has been no decrease in the prevalence of physical illness in the Western world during the last 30–40 years (Saha et al., 2007). Furthermore, there is evidence of excess early mortality (Laursen et al., 2013) and an increasing mortality gap for patients diagnosed with schizophrenia (Nielsen et al., 2013).
Reviews describe increased physical morbidity among patients with severe psychiatric diseases (Leucht et al., 2007). Additionally, high rates of cardiometabolic risk factors are seen in Australians living with psychosis (Galletly et al., 2013). The use of second-generation antipsychotics could possibly be a contributing factor in the development of CVD through causing obesity and metabolic syndrome (Allison et al., 1999; Newcomer, 2007). These conditions could subsequently be expected to contribute to even higher mortality (Hamer et al., 2008).
Excess comorbidity as a result of CVD and diabetes has severe consequences for both patients and health budgets. These consequences could be minimized if physical illness was identified and prevented more quickly (Rossler et al., 2005). Some of the main causes of excess comorbidity are because patients with mental illness are often reluctant to seek medical care (Cradock-O’Leary et al., 2002; De Hert et al., 2011a), and medical care given to patients with mental illnesses is of lower quality than that given to patients without mental illnesses (Mitchell et al., 2009). Risk factors of CVD among patients with mental illness are inadequately diagnosed and incompletely treated (Holt et al., 2010; Nasrallah et al., 2006). Increased waist circumference (WC) is a key factor for metabolic syndrome; however, only 10% of patients identified as having metabolic syndrome were followed up and treated after discharge from psychiatric hospitals (Coakley et al., 2012).
In clinical practice, it is simple and cheap to use WC as a measure of unhealthy body fat with regard to the increased risk of CVD and the development of type 2 diabetes (Bigaard et al., 2003). In practice, it may be useful to combine WC with other measures, for example body mass index (BMI) and weight, and compare the values and changes with the medical history of the individual patient. This is also the recommendation in different guidelines on the topic (De Hert et al., 2011b). Furthermore, changes in WCs are caused by both modifications in exercise level (Poulin et al., 2007) and diet changes (Evans et al., 2005). More physical activity will increase muscle mass and reduce fat volume in the body. This health benefit may not be reflected in a lower BMI and therefore BMI is not well suited to measure this change. Measurement of WC is easy to carry out and the results can be used in continuous treatment and as encouragement to the individual patient in their efforts to improve their physical health.
The Cromwell House Program in Manchester, UK, succeeded in the long-term maintenance of weight loss in patients through a behavioural treatment programme (Pendlebury et al., 2007). A European group, European Network for Promoting the Health of Residents in Psychiatric and Social Care Institutions (HELPS), succeeded in defining the planning and management of improving physical health of patients with severe mental illness (Weiser et al., 2009). Guidelines for screening and monitoring of health problems are available (De Hert et al., 2011b), as are strategies for cognitive behavioural therapy for the improvement of physical health in patients with schizophrenia (Attux et al., 2013; Weber et al., 2008). Additional studies initiated by the pharmaceutical industry have been aimed at reducing weight gain from antipsychotic medication (Porsdal et al., 2010). Those studies do, however, often have a short-term scope and may have different methodological problems.
The quality of general health care for patients with severe mental illness and the consensus regarding prevention of somatic illness among vulnerable psychiatric patients needs to be improved. We need more knowledge about how to integrate prevention and care of somatic illness in the treatment of this group of patients. The aim of this study was to test the efficacy of an intervention programme for improving physical health in long-term-treated psychiatric patients.
Methods
Design
The study originates from the HELPS project (Weiser et al., 2009). The first author (PH) was responsible for the Danish part of HELPS. The background and preliminary results from HELPS are continued in the present study, which was designed as a cluster-randomized intervention study involving six facilities. The study used an “active awareness” and motivational interviewing approach to increase knowledge and improvement of physical health in people with long-term psychiatric illness. Three facilities were randomized to the intervention group and three to the control group. All patients in each of the facilities were invited to participate. All data were collected at index at all six facilities. The measures and ratings collected at index were repeated after the intervention period of 12 months. WC was used as the primary outcome as it has proven to be a good measure for the risk of CVD and the risk of developing diabetes (Bigaard et al., 2003).
Two theoretical methods were used in the study: the Method of Motivational Interviewing (Rollnick et al., 2008) and Stages of Change Methods (Prochaska and DiClemente, 1982). These methods were used in the intervention part of the study as they were deemed appropriate and of importance in the management of lifestyle changes for patients with mental illness (Horiuchi et al., 2012; Rubak et al., 2005; Tuah et al., 2011). Furthermore, the methods can be straightforward and appealing to staff working in mental health care. When lifestyle change is required and wanted, there is evidence that patient-centred approaches to health care may have better outcomes than traditional methods. Method of Motivational Interviewing has a patient-centred approach and it provides a way of working with patients who may not be ready to make the behaviour changes that are considered necessary by the health worker (Rollnick et al., 2008).
Participants
The study population consisted of patients cared for in six long-term social psychiatric facilities for severely mentally ill patients in North Jutland, Denmark. To be referred to the facilities, the patients must have extensive mental disabilities. Moreover, the patients suffer to varying degrees from serious negative symptoms and significant cognitive impairment (i.e. the patients were severely and chronically mentally ill and unable to live without round-the-clock psychiatric nursing).
Intervention
The intervention, which is described as active awareness, was performed by the project leader (PH) and a research nurse (HØS), both experienced in psychiatric nursing and the care of physical health in patients with severe mental illness. The intervention focused on both the individual patient and the staff members. The staff are the main care providers for the patients and are regarded as role models. The project leader and/or the research nurse was present at the facilities 3 days per month in this 12-month period, beginning 10 November 2009, except for the period of index data collection when presence was higher in both the intervention and control facilities.
The intervention consisted of the following:
In each of the three intervention facilities, there were focus groups with both patients and staff members separately (each with 5–8 participants). The focus group topics were health problems and methods for improving physical health: (a) health risks/health problems; (b) causes of health problems/common health problems; (c) possibilities for prevention; and (d) preventive measures at own facility. These focus groups were also part of HELPS (Weiser et al., 2009). The interviews were recorded and digitally transcribed and descriptive results were obtained with Maxqda, a computer program for qualitative data. The project leader presented the results from the focus group discussion to the staff, and staff were encouraged to benefit from the results and take action in terms of improving the physical health in their own facility.
PH and/or HØS had individual sessions with the patients and staff members to collect index data. The sessions lasted 1 hour at index and 1 hour at follow up. Method of Motivational Interviewing (Rollnick et al., 2008; Rubak et al., 2005) and Stages of Change Methods (Prochaska and DiClemente, 1982) were used, and the patients were involved in making plans for their own actions to improve their physical health.
During the first third of the study period, three group sessions of 1.5 hours were held with the staff. PH provided information on how to promote smoking cessation among the patients. Practical information on how and where staff could seek professional support and guidance for smoking cessation among patients, as well as themselves, was also provided.
During the first third of the study period, three group sessions were held with the staff about the correct use of antipsychotic medication, according to recommendations from the Danish Health Board (Interior and Ministry of Health, 2010).
During his weekly visits to the facilities, PH constantly provided guidance to the staff and the leaders about ways of maximizing patients’ physical activity in daily life (e.g. daily walks) and encouragement to increase physical activity over time. For some patients, regular fitness and sport activities were more appropriate and they were instructed on how to arrange and how to maintain this over time.
On a monthly basis, PH provided guidance in terms of healthy food consumption. This was directed at staff who had daily contact with the patients and to staff in charge of the food and drinks consumed by the patients.
Treatment was administered as normal in the control group during the study period. There was no interference from the study beyond the necessary measurements to obtain index data. In connection with the measurement of follow-up data, patients and staff in the control facilities were offered individual sessions.
Measures at index and follow up
For patients and staff, measurements were taken for WC (Bosy-Westphal et al., 2010), BMI, bodyweight (measured with Tanita Body composition analyser, model TBF-30), lung positive-end expiratory pressure, blood pressure, physical fitness (measured on an exercise bike, one-point test), and tobacco and alcohol consumption. In addition, for patients only, measurements were taken for blood glucose, high-density lipoprotein (HDL), low-density lipoprotein (LDL), cholesterol, and triglyceride, electrocardiography, and registration of psychotropic medication.
In cooperation with the staff in charge of the individual patients, the prescribed medication was registered before and after the intervention in order to secure accurate data for medication over 24 hours. Depot antipsychotics were included in the calculation of overall doses, taking dosing intervals into account. In order to be able to compare dosages of the various antipsychotics, measurement units were calculated by dividing the prescribed daily doses by the defined daily doses (Leucht et al., 2014; Dixon et al., 2010; Nose et al., 2008). This was in accordance with guidance on treatment with antipsychotic drugs in patients over 18 years from the Danish Interior and Ministry of Health (2010).
There are different ways to measure WC, and they differ in method and accuracy of predicting risk factors for glucose intolerance, type 2 diabetes, and CVD. Overweight patients with a high accumulation of visceral abdominal fat (VAF), compared with overweight patients with a lower degree of VAF, are at greater risk of developing glucose intolerance, hypertriglyceridaemia, and lower HDL (Despres et al., 2001). WC is a practical measure of adipose tissue distribution. Four body sites for WC measurements are used: immediately below the lowest ribs (WC1), the narrowest point of the waist (WC2), the midpoint between the lowest rib and the iliac crest (WC3), and immediately above the iliac crest (WC4). WC values at the four commonly used anatomical sites differ in magnitude depending on sex, are highly reproducible, and are correlated with total body and trunk adiposity in a sex-dependent manner (Wang et al., 2003). In our study, the measurement of WC was done by finding the midpoint between the lowest rib and the iliac crest at the level of the midaxillary line (WC3) (Wang et al., 2003). Participants were asked to breathe normally and the reading of the measurement was taken at the end of gentle exhaling. This prevented subjects from contracting their abdominal muscles or from holding their breath.
Statistical analysis
Power calculations were based on the primary outcome measure (WC). We included a type 1 error of 5% and a power of 80%. Standard deviations of 4.05 and 3.86 have been found in previous studies (Carta et al., 2008; Jensen, 2001). We concluded that a minimum of 60 participants in each of the two arms was necessary for detection of a statistically significant effect (2.0 cm) of the intervention.
The randomization was done at facility level. The facilities were matched by the project leader on the basis of the best fit of homogeneity with the size of the facility and the patients’ diagnoses. The resulting pairs were randomized to either the intervention or the control group. Randomization was made by a person with no knowledge or interest in the facilities, the patients, or the study.
Descriptive analyses were performed initially on all outcomes for the intervention and the control group, respectively. Comparisons of index values between the intervention and the control group were performed using Student’s t-test for continuous and normally distributed variables and Wilcoxon rank sum test for continuous but abnormally distributed variables. Tests of equal proportions were applied for dichotomous variables such as sex and smokers.
Changes at subject level between index and follow up were calculated, and in order to determine a difference between the changes in the intervention and the control group, we used Student’s t-test. These analyses were adjusted for clustering of data within each facility by correction of the test statistics using the intraclass correlation coefficient (ICC) and the design effect. When comparing glucose values, we excluded patients who had diabetes at index.
Finally, linear regression of changes in WC was performed, with group membership, sex, age, and body fat percentage as explanatory variables. For two patients with a BMI <20 kg/m2 at index, the change in WC was reversed compared to the remaining patients (i.e. a possible increase was considered positive). Robust standard errors were estimated in the regression analysis to account for the clustering within the facility. In addition, we applied the method of last observation carried forward and repeated the linear regression analysis.
The statistical analyses were carried out using the statistical software Stata version 11 (StataCorp, College Station, TX, USA) and the chosen level of significance was 5%.
Ethics
The study followed the Helsinki II Declaration, and was approved by the Committee on Biomedical Research Ethics (N-2008004MCH) and the Danish Data Protection Agency. The study was registered at Clinicaltrials.gov (ID: 3,3 270809).
Results
All the patients were diagnosed by psychiatrists; the most common diagnosis was schizophrenia (72 and 73% in the intervention and control groups, respectively). The remaining patients suffered from other severe mental illnesses (e.g. bipolar disorder) and were equally distributed among the intervention and control groups. All were Danish citizens and all but three were Caucasians: two Inuits and one Indian. In total, the six facilities had 174 patients and 330 staff members. Of the 174 patients, 97 were included. The 77 patients who did not participate in the study were older than the participating patients (mean 11 years). Twelve patients dropped out during the study period, leaving 85 patients for analysis. Reasons for dropout were death (three cases), movement from the facilities during the study period (three cases) and wanting to leave the study for personal reasons (six cases) (Figure 1).
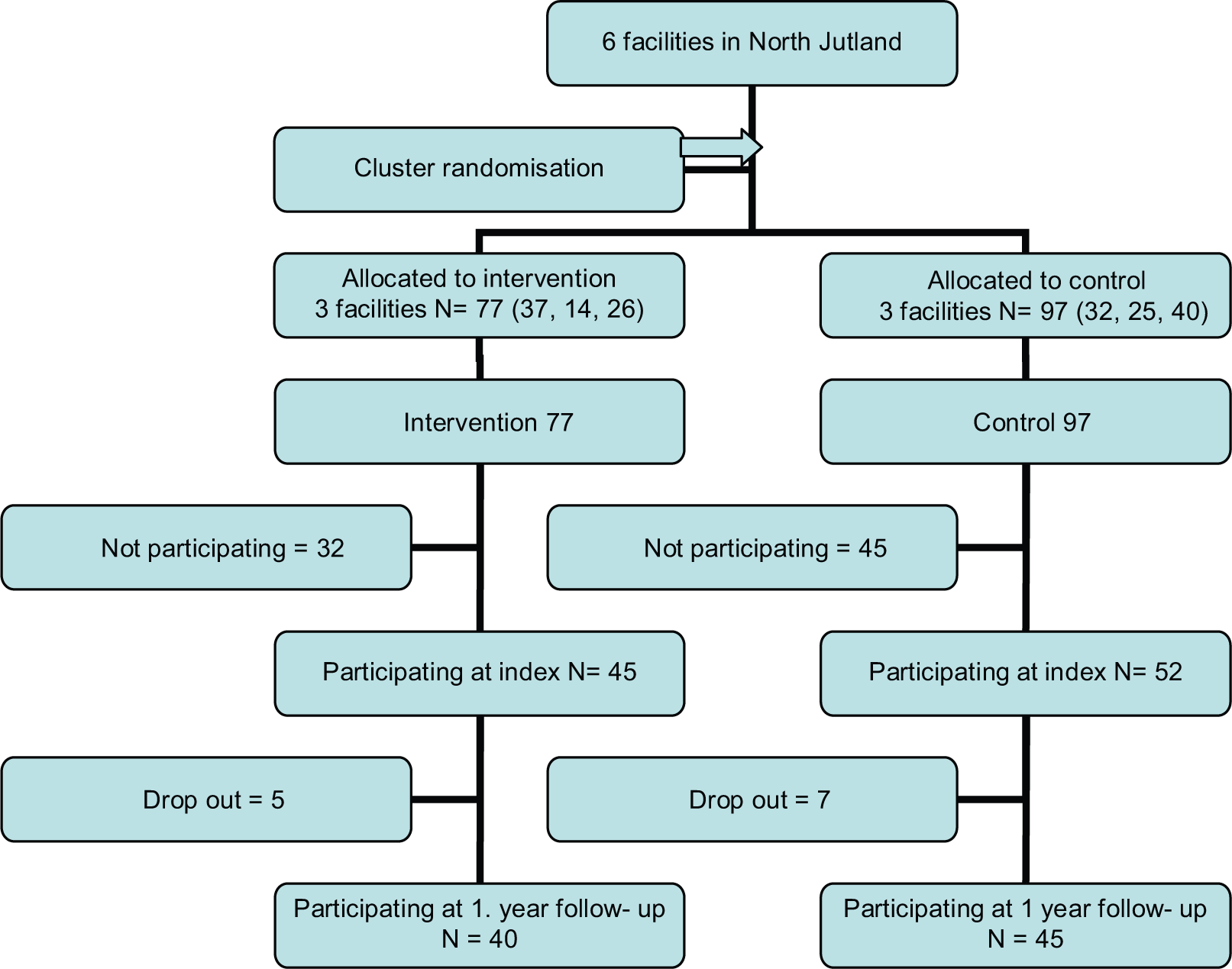
Flow chart illustrating the progress of patients through the study.
The sociodemographic and clinical characteristics of the study sample at index are given in Table 1. Many were obese (BMI >30 kg/m2: 44.3% and BMI >25 kg/m2: 76.3%). WC was on average 106 cm for men and 108 cm for women in the intervention group and 112 cm for men and 109 cm for women in the control group. Furthermore, a majority of the patients smoked (69%), with on average 27 cigarettes daily. There were no differences between the distributions of diagnoses in the two groups.
Patients’ sociodemographic and clinical characteristics at index.
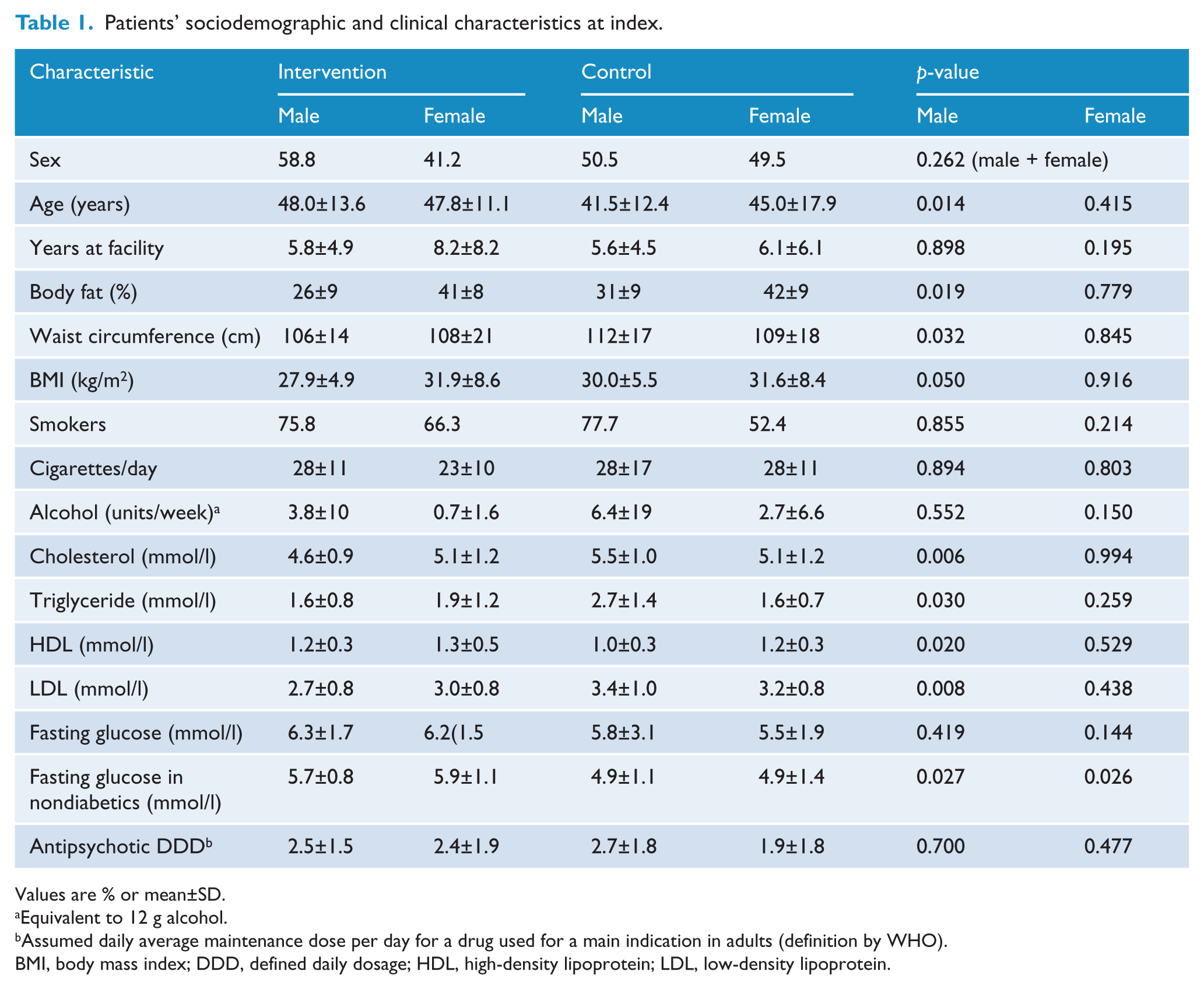
Values are % or mean±SD.
Equivalent to 12 g alcohol.
Assumed daily average maintenance dose per day for a drug used for a main indication in adults (definition by WHO).
BMI, body mass index; DDD, defined daily dosage; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Analyses of the effect of the intervention are given in Table 2. In the intervention group there was a decrease in WC of −0.75 cm (95% CI −2.79 to 1.23). There was an increase in WC of the patients in the control group (2.17 cm, 95% CI −0.37 to 4.71). The cholesterol and LDL levels decreased in both the intervention and control groups. There was a significant decrease in diastolic blood pressure of 3.68 mmHg (95% CI −6.88 to −0.47) in the intervention group. There were no significant changes in HDL and triglyceride. There were no statistically significant changes in fasting glucose between the control and the intervention groups.
Effect of the intervention between index and follow-up measurements.

Nonsmokers at index excluded.
Adjusted for the effect of cluster randomization.
Known diabetics at index excluded.
Truncated at zero.
BMI, body mass index; BP, blood pressure; DDD, defined daily dosage; HDL, high-density lipoprotein; ICC, interclass correlation coefficient; LDL, low-density lipoprotein.
Linear regression analyses controlling for effect of cluster randomization, sex, age, and body fat showed a difference in the change of WC between the intervention group and the control group of −3.1 cm (p=0.018) (Table 3).
Linear regression.

Results in parentheses are from analysis using last observation carried forward.
Discussion
Rates of obesity were high at index (BMI >30 kg/m2: 44.3% and BMI >25 kg/m2: 76.3%), and WC was, on average, above the recommended values for both men and women in both the intervention group and the control group. The study participants in the intervention group showed a small, but not significant, reduction of WC, while participants in the control group showed a significant increase in WC. This indicates that the intervention was not able to cause a reduction in the WC, but it clearly stopped further increase.
Our study offered an intervention to a group of patients with severe mental illness with a high prevalence of risk factors for CVD (obesity, smoking, and abdominal fat). In addition, there were patients with a high level of fasting glucose, which can be interpreted as a group of patients who are in the transition to diabetes, at approximately 5–10% per year (Tabak et al., 2012). During our study, it was possible to modify these risk factors by guiding patients towards healthier lifestyle alternatives.
Epidemiological studies have consistently shown excess mortality due to CVD in patients with schizophrenia. A meta-analysis of 37 studies had a median all-cause standardized mortality rate of 2.6. Additionally, a prevalence of 45–55% for obesity and 50–80% for smoking were demonstrated (Saha et al., 2007). Our study shows comparable prevalence of obesity (44%) and rates of smoking (69%).
The main result from this current intervention study is a reduction in WC. The result is comparable with other studies (Forsberg et al., 2008) showing that, with health interventions and information similar to our study, it is possible to improve or at least postpone the development of risk factors for CVD and diabetes. Targeted behavioural weight-loss interventions have shown that a weight loss of 5% of the initial weight was possible (Daumit et al., 2013) which may cause a improve health or prevent diabetes and CVD. Some studies are limited by methodological problems due to small sample sizes, short study periods of 8–12 weeks, and/or high dropout rates during the study period (Faulkner et al., 2007). Our study had a low dropout rate (12%) and a long study period (12 months). When dealing with lifestyle changes, it is relatively simple to change unhealthy eating habits, increase the level of physical activity, and, as a consequence, lose weight and achieve improved physical health within a short period of time, for example 2–3 months (Mann et al., 2007). It is more difficult to maintain a healthy lifestyle over longer periods. Studies conducted to test weight-reducing strategies on people from the general population show that a majority of the participants regained their initial weight or even put on some extra weight after 1–2 years (Mann et al., 2007). Our study has shown a small reduction in WC after 1 year and this makes it possible to argue that the intervention is effective for this group of patients in the lifelong effort of improving their physical health.
The prevalence of diabetes is double or more in a population of patients with schizophrenia compared with an average population (De Hert et al., 2009; Holt, 2004). This is mainly owing to a high prevalence of obesity and the effect of some antipsychotics (Daumit et al., 2008). Type 2 diabetes develops over one, or even, two decades. In the long term, it is difficult to predict the true scope of the health problem. Furthermore, patients with a mental illness have many serious problems from the illness itself and it may be difficult, or even impossible, to manage a demanding diabetes diagnosis alongside the psychiatric disabilities. In our study, many had high fasting blood glucose. During the 1-year study time, there was a small drop in fasting glucose in the intervention group and an increase in the control group. Although these results were not of statistical significance, it is reasonable to assume that without any action planned in terms of reducing the increasing blood glucose in the patients, more cases of diabetes may be seen in the years to come (Tabak et al., 2012).
Strengths
Dropouts from interventions are important issues because they lower the power of the studies. The number of dropouts can be so high that the results only come from a very select, and presumably more interested and motivated, part of the study population as, for example, in the case of Hassapidou et al. (2011). We used the last observation carried forward in the regression analysis of WCs and the result was robust (–2.50; p=0.039). Keeping this in mind, our study with only a 12% dropout rate seems reasonable to copy in wider groups of patients with severe mental illnesses. Furthermore, our study had an intervention period of 12 months.
The patients and staff in the control group were told that they were participating in a study about physical health for people with mental illness. All the measurements in the control group at index were taken with minimum additional information. Nevertheless, the measurements probably resulted in some kind of intervention, and some participants might have taken the measured values into consideration and tried to change their lifestyle to a healthier one. If the measurements showed values critical to the individual’s health, the project leader urged the staff to refer to medical advice and possible treatment. Overall, these actions may have weakened the results from the intervention in terms of smaller differences, for example, changes in WC.
Data were collected knowing that patients with severe mental illness might have cognitive and reading disabilities. Therefore, data collection was performed in the form of interviews by the project leader, who guided the patients in answering the questions as precisely as possible. This might have increased the validity of the study results.
Limitations
All patients were invited to participate in the study; however, 44% declined. Information on the reasons for not participating was not collected, nor was data of nonparticipants except their age and diagnosis. Analyses showed that nonparticipants were, on average, 11 years older than the participants and it was suggested that older patients did not feel that they had the physical and mental capacity to participate.
The randomization was done at facility level with only six facilities in total. Randomization of few clusters is critical, and in our study we had a skewed outcome as indicated by the control group men who were significantly younger and fatter at index. Although we controlled for age in the statistical analysis it is not certain how this difference in index data impacted on the study results.
The study did not succeed in reaching the planned number of 60 patients in each arm of the study. Fortunately, the dropout rate was low (12%) which was less than the expected 20%; however, the study is underpowered. The absence of statistical power might be one of the reasons that some of our results showed a tendency towards change, but did not reach statistical significance. In fact, the intervention might be more successful at reducing WCs than is apparent from this work.
Implications for clinical practice
In clinical practice, the detected effect seems modest. However, the intervention showed that it was possible to stop the general increase of WC, which is important in future preventive treatment. We are trying to help patients towards a healthier lifestyle. This is a great challenge, as patients with schizophrenia might have more difficulty in breaking the pattern of an unhealthy lifestyle and preventing its consequences as a result of factors related to their illness and treatment (Hasnain and Vieweg, 2011). Another issue is that a lower physical activity level might be due to negative symptoms, cardiometabolic comorbidity, side effects of antipsychotic medication, and social isolation (Vancampfort et al., 2012). Furthermore, low expiratory spirometry parameters may play an important role in physical activity level (Vancampfort et al, 2014). For these reasons, it is even more important that the effort to improve patients’ physical health is proactive and enacted with a high level of professional expertise.
Our study interventions consisted of active awareness, including several components, and we do not know which part was the more efficient because all components were applied simultaneously as a programme. The prevalence of patients with severe mental illness with comorbidities such as CVD and diabetes is high, and the consequences will often be poor physical and mental health for the patients and a worsening in patients’ quality of life. This makes it very important to plan prevention or to delay the onset of CVD and diabetes among this group of patients. The study shows that it is possible to stop further increase in WC and stabilize the level of fasting glucose. In clinical practice it will result in the prevention or delay of CVD and diabetes. The interventions seem manageable in these facilities and can be performed by members of the nursing staff who are interested in physical health. This requires that leaders, staff, and patients in the facilities focus on using active awareness, as shown in this study.
After the study ended, the HELPS TOOLKIT – a tool to promote the physical health of residents in psychiatric facilities (www.uni-ulm.de/helps-net/toolkit/helps_toolkit_international.pdf) was released. Data on staff was collected at the same time and the results will be published in a separate paper by this study group.
Footnotes
Funding
This study was supported by the Region of North Jutland no. 1-26-0013-08, Det Obelske Familiefond no. 61985611, Eli and Egon Larsens Fond Journal no. 8057dh/lh, and the Danish Nurses’ Organization no. 70371.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.