
Abstract

To the Editor
A 63-year-old man with a recent diagnosis of alcoholic cirrhosis presented to hospital with symptoms of acute paranoia, grandiosity and aggression. He had no past psychiatric history and his family reported complete abstinence of alcohol in the preceding 2 months. On examination his sensorium was clear and there were no physical stigmata of hepatic dysfunction. He exhibited a slow, shuffling gait and slowed cognition, but smell was normal. On investigation his transaminases were only mildly elevated. Serum bilirubin and ammonia levels were normal, as were iron, copper and ceruloplasmin. Liver ultrasound was consistent with cirrhosis but showed no evidence of portal hypertension. No abnormalities were found on EEG or CT chest, abdomen and pelvis.
MRI brain showed bilateral T1 hyperintensities in the caudate, putamen and globus pallidus (A). T2 signal in the same region was normal (B) (Figure 1). He was diagnosed with acquired hepatocerebral degeneration (AHD) secondary to alcoholic cirrhosis, and admitted to hospital for symptomatic treatment of his psychosis with haloperidol 2 mg daily.
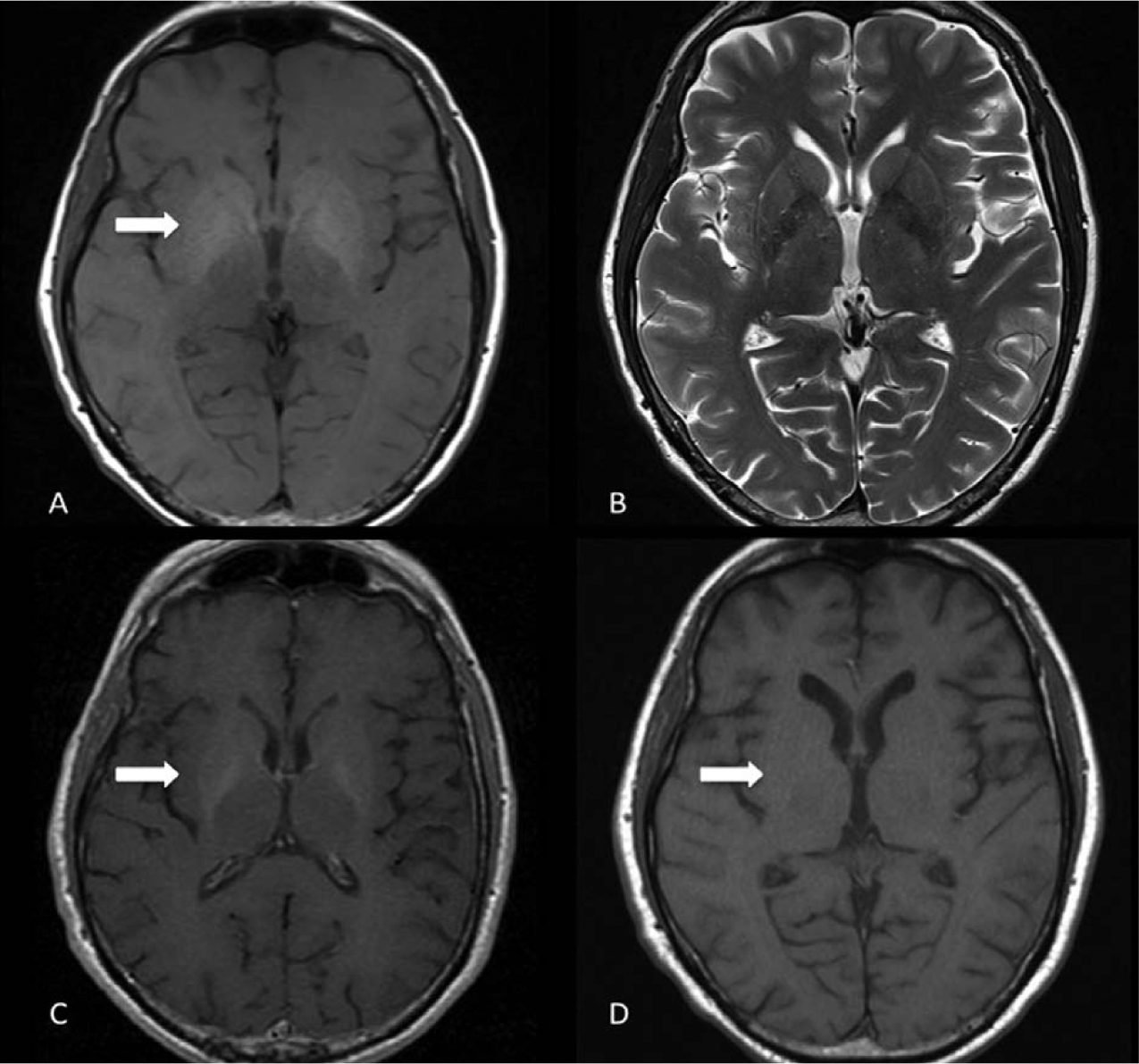
MRI brain showing bilateral T1 hyperintensities in the caudate, putamen, and globus pallidus (A) with a normal T2 signal (B). Improvement in the T1 basal ganglia hyperintensity was seen at 3 months (C) and 9 months (D).
Three months later, the patient’s psychotic symptoms had resolved but he remained disinhibited and demonstrated parkinsonism well in excess of expected medication side-effects. Neuropsychological testing showed significantly impaired information processing speed, visuo-spatial functioning, working memory and executive functioning. Repeat MRI showed subtle improvement in basal ganglia hyperintensity (C). A more marked improvement at 9 months (D) was associated with improvements in both parkinsonism and cognition.
AHD is a sub-acute variant of hepatic encephalopathy. It is not associated with delirium and can affect patients without overt clinical or biochemical evidence of hepatic failure (Ferrara and Jankovic, 2009). Cognitive symptoms include bradyphrenia and impairment of attention, with relative sparing of memory and language (Ferrara and Jankovic, 2009; Stracciari et al., 2008). Symmetrical parkinsonism is common on neurological examination, but chorea, dystonia, dyskinesia and ataxia may also occur (Fernández-Rodriguez et al., 2010; Ferrara and Jankovic, 2009). MRI shows distinctive T1 hyperintensity in the globus pallidi (Fernández-Rodriguez et al., 2010; Ferrara and Jankovic, 2009).
The clinical and radiological features of AHD are associated with elevated manganese levels in the serum, CSF and globus pallidus on autopsy. Potential causes include impaired biliary excretion and portosystemic shunting (Ferrara and Jankovic, 2009). A similar pattern is seen in manganese toxicity from occupational exposure, long-term total parenteral nutrition and intravenous use of manganese-contaminated drugs such as methcathinone (Fernández-Rodriguez et al., 2010; Ferrara and Jankovic, 2009). If left untreated the course is progressive, but symptoms, serum manganese levels and MRI changes all improve when hepatic function is restored (Ferrara and Jankovic, 2009). AHD is therefore an important differential diagnosis when seeking reversible causes of cognitive impairment in patients with alcoholic liver disease.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.