
Abstract
Objective:
To assess the influence of involuntary job loss on suicide and attempted suicide in young adults.
Method:
A population-based case–control study of young adults (18–34 years) was conducted in New South Wales, Australia. Cases included both suicides (n=84) and attempts (n=101). A structured interview was conducted with next of kin (for suicide cases) and suicide attempters admitted to hospital. Controls selected from the general population were matched to cases by age and sex. Job dismissal or redundancy (involuntary job loss) in the 12 months before suicide or attempt was the main study variable of interest. Suicide and attempts were modelled separately and in combination as outcomes using conditional logistic regression modelling. The analysis was also adjusted for marital status, socio-economic status and diagnosis of an affective or anxiety disorder.
Results:
Following adjustment for other variables, involuntary job loss was associated with an odds ratio of 1.82 for suicide and attempted suicide (combined) (95% CI 0.98 to 3.37; p=0.058). Low socio-economic status was associated with an odds ratio of 3.80 for suicide and attempted suicide (95% CI 2.16 to 6.67; p<0.001) compared to high socio-economic status (after adjustment). Diagnosis of a mental disorder was associated with a 7.87 (95% CI 5.16 to 12.01; p<0.001) odds ratio of suicide and attempted suicide compared to no diagnosis (after adjustment). Involuntary job loss was associated with increased odds of suicide and attempts when these were modelled separately, but results did not reach statistical significance.
Conclusions:
Involuntary job loss was associated with increased odds of suicide and attempted suicide. The strength of this relationship was attenuated after adjustment for socio-economic status and mental disorders, which indicates that these may have a stronger influence on suicide than job loss.
Background
Involuntary job loss occurs when an individual loses a job due to workplace closure, being fired or being made redundant (Schröder, 2012). This represents an acutely stressful event in a person’s life and is a different construct from unemployment, which incorporates the process of looking for work (Berchick et al., 2012; Burgard et al., 2007). There is some evidence from longitudinal studies that involuntary job loss is associated with a greater likelihood of depressive symptoms (Berchick et al., 2012; Burgard et al., 2007; Schröder, 2012), although no studies focusing on the relationship between involuntary job loss and mental health have been conducted in Australia.
Most past studies on suicide have focused on unemployment rather than involuntary job loss (Blakely et al., 2003; Morrell et al., 1993, 1998, 2001, 2007). Among the small number of existing studies on involuntary job loss and suicide, two were ecological analyses and therefore may not provide evidence about the relationship between job loss and suicide at the individual level (Classen and Dunn, 2012; Eliason and Storrie, 2009). The remaining study was based on a specific occupational group (two meat processing plants in the Hawkes Bay region of New Zealand) (Keefe et al., 2002). All these studies found that involuntary job loss was a significant risk factor for suicide.
The present study examines the relationship of involuntary job loss to suicide and attempted suicide using a population-based case–control study of young adults (18–34 years) in New South Wales (NSW), Australia. Young adults in Australia have been identified as being at higher risk of suicide attempt, self-harm (Martin et al., 2010) and mortality, including suicide (Australian Bureau of Statistics, 2012), than older age groups. Young adults also have the highest rates of unemployment and under-employment in the working-age population (Australian Bureau of Statistics, 2009; Page et al., 2013). The present study focuses on the potential risks associated with the effects of involuntary job loss, as distinct from investigating the category of unemployment. A strength of the data used in this paper is the sample size, which is comparatively larger than those reported in other studies for this age group (Beautrais et al., 1997; Brent et al., 1993; Charlton, 1995; Lesage et al., 1994) and is also based on matched population-based cases and controls.
Methods
Study design
A population-based case–control study design was used to investigate suicide deaths and suicide attempts in young adults aged between 18 and 34 years in NSW, Australia covering both metropolitan and rural areas.
Case selection
Information on coronial-determined suicides was obtained from The National Coronial Information System (NCIS) and covered a large proportion of NSW, which included the Coronial Court jurisdictions of Sydney, Westmead, Wollongong, Newcastle, Maitland, East Maitland, Bathurst, Orange and Dubbo for the period 2003–2008. We selected these areas a priori to cover both metropolitan and rural areas of the state in order to capture geographical differences in both suicide and job loss.
A coronial file audit was then conducted by the research team for each case to enumerate contact details for the next of kin or significant other. All files on coroner-determined suicides were examined to obtain contact details for the next of kin or significant others (n=219) in consultation with forensic counselling. Of the 219 suicides in the coronial data originally extracted by the authors, 120 cases with available contact information for next of kin were identified after exclusions and deemed suitable for contact by forensic counsellors. An invitation to participate in the research was sent by mail on behalf of the Chief Forensic Pathologist of NSW.
The participation rate was 70% (n=84) of the 120 next of kin contacted. The next of kin took part in face-to-face interviews to complete a questionnaire about socio-demographic factors, life events and other antecedent circumstances of the suicide case. Interviews took place at a time and place convenient for the interviewee either in person (face-to-face) or by phone. One next-of-kin interview was conducted for each suicide case.
Attempted suicide case recruitment occurred when patients were admitted to hospital following a suicide attempt. Patients were recruited at the Mater Hospital in Newcastle and at the Prince of Wales and Sutherland Hospitals in Sydney. All patients in the 18–34 age range admitted to hospital following a suicide attempt were approached by a clinician to ascertain their interest in research participation. Interested patients were then asked if they were willing to receive information about research participation in the study by mail. Prospective participants were subsequently contacted by the research team to arrange an interview. An invitation to participate in the research was sent to 343 potential participants. Contact to confirm interviews was made with 214 young adults and interviews were conducted with 47% (n=101).
Control selection
The sampling frame for population-based controls was provided by the Australian Bureau of Statistics (ABS) and derived from the Census of Population and Housing and the Monthly Population Survey (MPS) design framework. Census Collection Districts (CDs) were selected systematically according to the Socio-Economic Indexes for Areas (SEIFA) and corresponded to the Local Government Area (LGA) characteristics covered by the coronial and hospital jurisdictions described above. CDs were selected such that there was an 80% probability that the residences contained young adults for strata matching to the sex and age group (within 2–3 years) of the cases.
Controls (n=250) were those aged 18–34 years and who resided in the regions from which suicide cases were drawn. Of the 1439 households approached, 304 relatives or friends were nominated, from which a total of 250 interviews were conducted (response 82%). More controls than cases were recruited (3:1 control-to-case ratio) to maximise statistical power given the small number of cases in the geographic catchments accruable over the study period. Suicide controls were asked to nominate an informant (parent, relative or friend), and the informant completed the same interview as completed by the next of kin of suicide cases. As in the cases, the interview for suicide controls was conducted face-to-face and related to socio-demographic factors, life events and other suicide risk factors, eliminating the potential for differential recall bias emanating from differing interview modes between case and control respondents.
Post hoc analysis of recruited controls for metropolitan Sydney and Hunter Region catchments showed similar sex and age distributions to the 2001 Census for corresponding areas, although a higher proportion of 20–24-year-old females were recruited, and a lower proportion of 30–34-year-old males were recruited than in the population. The proportions of males aged 20–24, 25–29 and 30–34 in the Census population were 14%, 15% and 16%, respectively, and for females these were 14%, 16% and 16%. Corresponding proportions for male suicide controls were 12%, 13%, 9% and for female suicide controls were 22%, 14%, 13%.
Survey and interview format
The questionnaire was derived from standard psychiatric and psychological instruments, the National Survey of Mental Health and Well-being (NSMHWB), standard population surveys (particularly the Australian Health Survey) and the Australian Census. The World Health Organization Composite International Diagnostic Interview (CIDI) was used to collect information on self-reported mental health symptoms, which were used to score International Classification of Diseases, 10th Revision (ICD-10) mental disorder diagnoses (Andrews and Peters, 1998; Peters and Andrews, 1995; Wittchen, 1994). High prevalence mental disorders were the focus of this aspect of the study and included substance use disorders (F10–F19), affective disorders (F30–F34) and anxiety disorders (F40–F43).
The interview questions focused on the following domains: (1) socio-demographic factors, including income, education, occupation, employment status and marital status, among others; and (2) psychiatric disorders, particularly affective disorders. The questionnaire was developed to be electronically collected via a laptop computer during the interview. Cases and controls were interviewed by trained clinical interviewers with health, medical, social work or psychology qualifications to minimise interviewer and recall bias.
Variables used in analysis
The outcome variable was suicide or attempted suicide, which were combined in order to achieve sufficient statistical power for the analysis. Past research suggests a number of similarities in the characteristics of those who attempt and die by suicide, including the presence of psychiatric disorders, history of previous suicide attempts, previous contact with services for mental health issues, social disadvantage and exposure to stressful life events (Beautrais, 2001, 2003). At the same time, suicide and attempted suicide have a number of important differences (Mościcki, 2001). For example, those who die by suicide are more often male and use lethal methods compared with those who attempt suicide (Beautrais, 2001, 2003). Recognising these differences, suicide and attempt were also assessed separately. The main variable of interest was dismissal or redundancy from a job in the previous 12 months (referred to as ‘involuntary job loss’ throughout this paper), which was ascertained through the question: ‘In the past 12 months, were you dismissed from a job or made redundant?’. For suicide deaths, this question was phrased in the third person: ‘In the 12 months before [NAME] died, was he/she dismissed from a job or made redundant?’.
The selection of potential covariates was guided by the development of a directed acyclic graph (Glymour, 2008) and informed by relevant literature. Variables that were plausible common causes (confounders) of both involuntary job loss and suicide and attempted suicide were included in analyses (Glymour, 2008). Possible confounding variables included age, sex and marital status (married/de facto, never married, or separated/divorced). A diagnosis through questionnaire of an anxiety and/or affective disorder using the ICD-10 codes for mild, moderate and severe disorders (with and without somatic symptoms experienced in the previous 12 months before the survey or interview) was also used in the analyses. We did not include substance use disorder as a confounder because of the concern that this may have followed involuntary job loss (e.g. was a mediator), rather than preceded it (Henkel, 2011). If we did adjust for this in analysis, it raises the possibility for bias due to conditioning on a mediator variable (Glymour, 2008).
Socio-economic status (SES) was also considered as a potential confounder and measured through a combined education-income measure, as described in Taylor et al. (2004). Education was coded as an ordinal variable: high school education or less, post-school training such as certificate or diploma, and university qualification. Income (AUD) was coded as annual household income: $29,999 or less, $30,000 to $69,999, and $70,000 and over. The income-education measure combined the three levels of household income and education to result in an index with five levels. The lower two categories and upper two categories were then grouped together. This produced a composite socio-economic (SES) measure of ‘low’, ‘middle’ and ‘high’ SES groups. Bivariate analyses of the SES index with suicide and attempts (by sex) also indicated that the index could be reduced to three levels (low, medium and high education-income) with reasonably homogenous odds ratios (ORs) for the outcome variables. Information on the scoring of the index can be seen in Supplementary Table 1.
Statistical analysis
A conditional logistic model (matching for 5-year age group and sex, which were thus excluded as variables from the analysis) were used to assess the effects of study variables on suicide and attempts (together and separately). The rationale for using a conditional model was based on the case–control matching for sex and age. This approach also maximised statistical efficiency, which was necessary given the relatively modest sample size of the study relative to the number of parameters included in the statistical models. Analyses commenced with estimating unadjusted ORs for suicide or attempts in relation to involuntary job loss. Following this the relationship between involuntary job loss was measured, controlling for other variables. All analyses were conducted using Stata Statistical Software: Release 12.1 (StataCorp LP, College Station, TX, USA).
Missing data and sensitivity analysis
There were a proportion of cases with information missing on either education or income in the SES index (50 cases out of a total of 670). In these instances information from the non-missing variable was used in the calculation of the index. For example, if information for a case was missing on income but information on education was not, the index would substitute the education information as the level of SES. To test the possibility that this approach to missing data biased the results, we applied two extreme scenarios: that the missing data represented the highest and lowest possible category of SES. We also conducted sensitivity analysis to assess the influence of substance use disorder (as well as anxiety or depression) on suicide and attempted suicide to account for the possibility that substance use was a preceding cause of both job dismissal and suicide.
The study received ethical approval from the University of Sydney; Southern Sydney, Greater Western, Western Sydney, Hunter New England, South Eastern Sydney (Eastern) and South Eastern Sydney (Southern) Area Health Services; the National Coronial Information System (NCIS); Department of Justice Victoria; and the NSW Aboriginal Medical Health and Research Council Ethics Committee.
Results
Within the suicide case–control analysis, there were 71 male and 13 female (n=84) suicides matched by age-strata and sex with 223 community controls. There were 32 males and 69 females matched with 239 community controls in the suicide attempt case–control analysis. Results suggest that most suicide deaths occurred among those aged 30–34 years (41.7%) and 25–29 years (33.3%). Approximately 5% of suicides were aged 18–19 years and 20% were aged 20–24 years. Among the attempted suicides, the highest proportion comprised those aged 20–24 years and 30–34 years (37.5% in each age group). About 9.4% were aged 18–19 years and 15.6% were aged 25–29 years.
When suicide attempts and deaths were combined in analysis (Table 1), involuntary job loss was associated with significantly greater odds of suicide and attempted suicide (OR 2.12; 95% CI 1.24 to 3.61; p=0.006). This relationship was attenuated in magnitude and was non-significant following adjustment for confounders (OR 1.82; 95% CI 0.98 to 3.37; p=0.058).
Involuntary job loss and suicide and attempted suicide (combined) in young adults aged 18–34 years, NSW, Australia, 2004–2010.
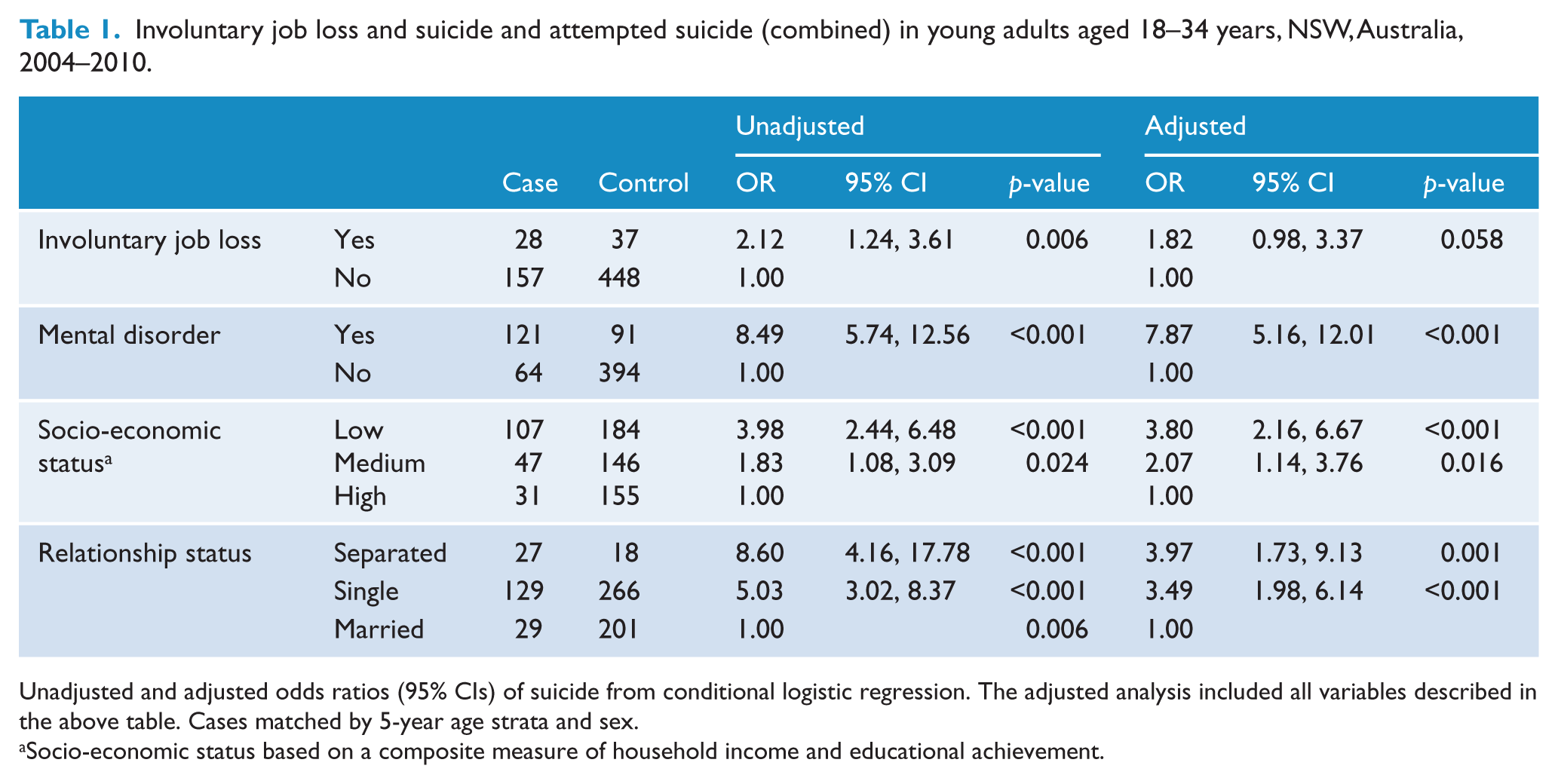
Unadjusted and adjusted odds ratios (95% CIs) of suicide from conditional logistic regression. The adjusted analysis included all variables described in the above table. Cases matched by 5-year age strata and sex.
Socio-economic status based on a composite measure of household income and educational achievement.
As can also be seen in Table 1, adjusted results indicated that a diagnosis of affective or anxiety disorder (mental disorder) was associated with over a sevenfold increase in suicide and attempted suicide compared to no diagnosis (OR 7.87; 95% CI 5.16 to 12.01; p<0.001). Those in the lowest SES group had an odds ratio nearly four times greater than those in the highest SES group (OR=3.80; 95% CI 2.16 to 6.67; p<0.001). Being separated (OR 3.97; 95% CI 1.73 to 9.13; p=0.001) or single (OR 3.49; 95% CI 1.98 to 6.14; p<0.001) was associated with greater odds of suicide and attempted suicide than being married.
When the data were analysed separately for suicide and attempts, the ORs for involuntary job loss were of a similar magnitude but there was little statistical evidence for this association (p-values ranged from 0.062 to 0.398) (Tables 2 and 3). Mental disorder was associated with approximately a fivefold increase (OR 5.12; 95% CI 2.49 to 10.53; p<0.001) in suicide (death) compared to controls in the adjusted analyses (Table 2). Those in the lowest SES group had an odds ratio three times greater of suicide (OR=3.85; 95% CI 1.59 to 9.35; p=0.003) compared to the highest SES group, and being separated (OR 5.44; 95% CI 1.61 to 18.39; p=0.006) or single (OR 5.84; 95% CI 2.37 to 14.39; p<0.001) was associated with higher odds of suicide than being married (after adjustment).
Involuntary job loss and suicide in young adults aged 18–34 years, NSW, Australia, 2004–2010.
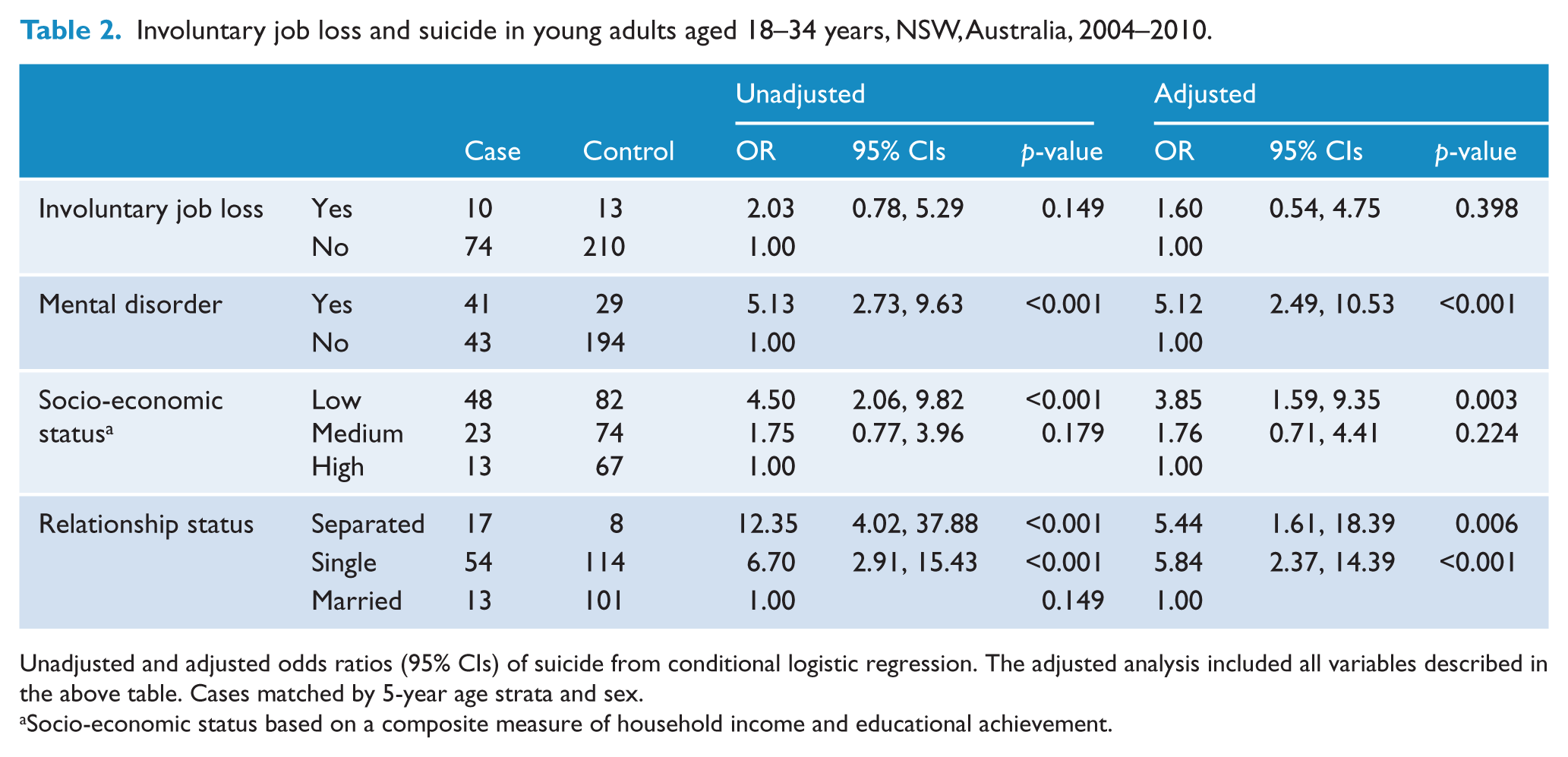
Unadjusted and adjusted odds ratios (95% CIs) of suicide from conditional logistic regression. The adjusted analysis included all variables described in the above table. Cases matched by 5-year age strata and sex.
Socio-economic status based on a composite measure of household income and educational achievement.
Involuntary job loss and attempted suicide in young adults aged 18–34 years, NSW, Australia, 2004–2010.
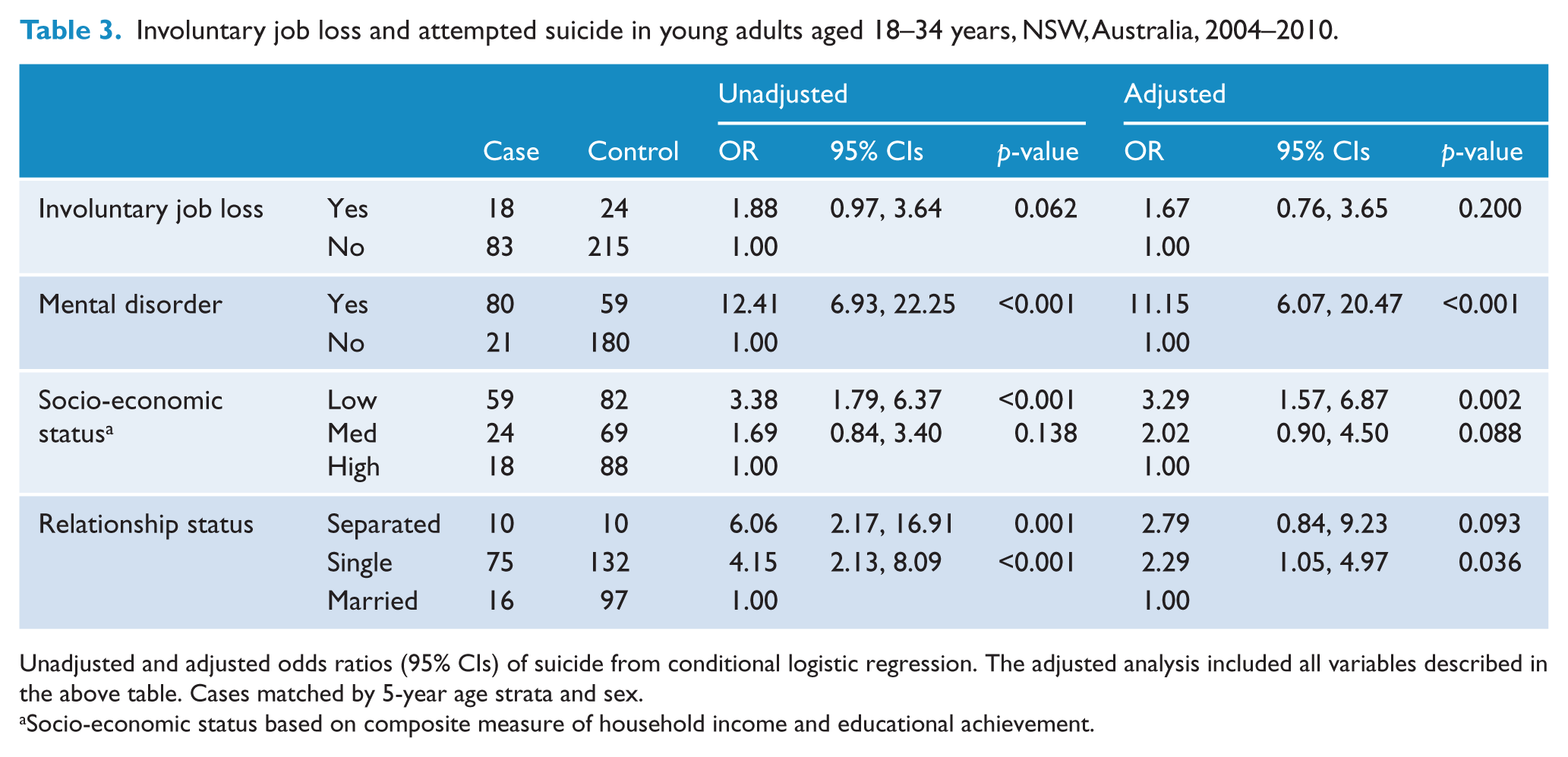
Unadjusted and adjusted odds ratios (95% CIs) of suicide from conditional logistic regression. The adjusted analysis included all variables described in the above table. Cases matched by 5-year age strata and sex.
Socio-economic status based on composite measure of household income and educational achievement.
Mental disorder was associated with an OR exceeding 11 for a suicide attempt (OR 11.15; 95% CI 6.07 to 20.47; p<0.001), and being single (OR 2.29; 95% CI 1.05 to 4.97; p=0.036) was associated with greater odds of attempt than being married (Table 3). Those in the lowest SES group had greater odds of attempts compared to those in higher SES groups (OR 3.29; 95% CI 1.57 to 6.87; p=0.002).
Sensitivity analysis
Sensitivity analysis was conducted using combined suicide and attempt data and can be seen in Supplementary Tables 2 to 4. First, assumptions about the missing SES variables were considered. When the missing SES values were assumed to fall into higher SES groups, the OR for job dismissal decreased but the confidence intervals and p-value were relatively unchanged (Supplementary Table 2). The OR of suicide in relation to the lowest SES group also decreased. The OR for job dismissal did not change substantially when the missing values were assumed to fall into the lowest SES group (Supplementary Table 3), while the OR for suicide in relation to membership in the lowest SES group increased.
Analysis was also conducted on the influence of anxiety, depression and substance use disorders on combined suicide and attempts (Supplementary Table 4). There was a 7.27 odds of suicide and attempts (95% CI 4.73 to 11.17; p<0.001) among those with a substance use, anxiety or depressive disorder compared to those without such disorders. The OR for job dismissal reduced to non-significance (p=0.180) after adjusting for other variables. Compared to those in the highest SES group, there was a threefold increase in the odds of suicide and attempts in the lowest SES group (OR 3.05; 95% CI 1.77 to 5.28; p<0.001).
Discussion
The present study is based on a young adult population, who, in Australia, have had the highest rates of unemployment in the working age-population (Australian Bureau of Statistics, 2009; Page et al., 2013). Involuntary job loss was associated with a twofold increase in suicide or attempted suicide, an association which was reduced in magnitude and to statistical non-significance following adjustment for confounders.
Mental disorder was associated with nearly five times the odds of suicide and 11 times the odds of a suicide attempt. It was not possible to adequately assess whether the mental disorder occurred before or after involuntary job loss. Thus, we are unable to conclude the directionality of relationships (i.e. that those with a mental illness are more prone job, or that job loss leads to mental illness). From an analytic point of view, controlling for mental disorder as a common cause (i.e. confounder) is thus a conservative approach that will underestimate the effect of involuntary job loss on suicide and attempted suicide (Blakely et al., 2003; Milner et al., 2013). An accurate estimate of the relationship between involuntary job loss and suicide and suicide attempt is likely to be somewhere between the adjusted and unadjusted estimates.
It is significant that distal risk factors, such as education and income, remained significant predictors of suicide or attempts even after controlling for mental disorder. Those in the lowest SES group had a threefold increase in the odds of suicide and attempted suicide compared to those in the highest SES group. This finding supports previous literature on the role of socio-economic disadvantage as a risk factor for suicide (Lorant et al., 2005; Morrell et al., 1999b; Page et al., 2002, 2006; Pan et al., 2013). We also found that those who were separated or single had greater odds of suicide than those who are married, which may suggest that these are associated with greater risk compared to marriage, which could be protective against suicide (Corcoran and Nagar, 2010).
There are a number of complexities influencing the relationship between involuntary job loss and suicide not addressed in this study. These include pressures from the economic environment (i.e. the availability of jobs), length of time a person was without employment, the number of times a person has been unemployed previously, and the temporal relationship in the development of mental disorder in relation to job loss (Milner et al., 2013). Further, although the data used in the present study represent the largest Australian case–control study of suicide and attempted suicide in young adults, the sample size still hindered statistical power, which partly explains statistically non-significant results when suicide and attempted suicide were analysed separately. This was addressed by aggregating suicide and attempted suicide as the outcome and analysing both sexes together.
The study may also be subject to recall bias, as are all case–control studies, made more problematic because of the use of proxies (e.g. next of kin) in the suicide component of the study (Pouliot and De Leo, 2006). However, controls for suicides were also proxies (e.g. next of kin) in order to maintain consistency. Suicides were enumerated from both rural and metropolitan areas of NSW; however, it is likely that cases from rural areas are under-represented in this study. Aside from this limitation, we would highlight that the gender ratio of attempts and suicides and the age distribution of cases roughly correspond to nationally representative data (Australian Bureau of Statistics, 2012; Pirkis et al., 2000; Taylor et al., 2004). A strength of the study (compared to previous research) (Beautrais et al., 1997; Brent et al., 1993; Charlton, 1995; Lesage et al., 1994) is that it used population-based cases and controls, which reduces the likelihood of biased exposure information and sample selection. Further, the main study factor was involuntary job loss, which is less likely to be subject to recall bias given this relates to a significant, sentinel event in an individual’s employment history.
Previous international case–control studies (n=4) on suicide among adolescents and young adults have been based on relatively small sample sizes (Beautrais et al., 1997; Brent et al., 1993; Charlton, 1995; Lesage et al., 1994) and most have used non-population-based community controls (Brent et al., 1993; Charlton, 1995; Lesage et al., 1994). A number of other studies on suicide in adolescents and young adults used record linkage cohort designs (Agerbo et al., 2002; Christiansen et al., 2013; Niederkrotenthaler et al., 2012; Zambon et al., 2011). While these types of studies can provide a greater number of cases and controls sampled from the general population, research utilising administrative data collections (without questionnaires) are usually unable to provide detailed information about risk and protective factors for suicide, especially on life events and when these occurred. The present study is significant as it is among the first population-representative case–control studies to provide information on the relationship between involuntary job loss, socio-economic factors and suicide in a sample of young adults.
The results of the present study highlight the importance of providing timely and appropriate treatment to those with anxiety, depression and substance use disorders. From a wider public health approach to prevention, these findings indicate the importance of providing targeted activities for young people in lower SES groups. The present research is particularly relevant in the current labour market climate of countries affected by the global financial crisis where involuntary job loss is an increasing problem. This emphasises the need for employment programs, support services and social welfare policies to address the risk of suicide among young adult workers who have lost their job.
Footnotes
Acknowledgements
We would like to acknowledge the participating hospitals: Calvary Mater Newcastle; Prince of Wales Hospital, Randwick; Sutherland Hospital, Caringbah; and St George Hospital, Kogarah. Acknowledgements are also given to the coroners’ courts, as described in the text.
Funding
This study was supported by a National Health and Medical Research Council (NHMRC) Project Grant 301965 and by the (Australian) Department of Health and Aging (DoHA).
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.