
Abstract

Introduction
It is little news to any of us that psychiatry is a difficult exercise. Core diagnoses around which we built our practice, such as major depression and generalised anxiety, have turned out to have ‘questionable’ and ‘unacceptable’ reliability when formally assessed by the very organisation that proposed them (Regier et al., 2013). Our best efforts at painstaking diagnosis are often unstable over time, as illness evolves and psychosocial circumstances and phenomenology shift the face of the presentation (Ruggero et al., 2010). Even more concerning, landmark studies such as CATIE and STAR*D demonstrate the limitations of current treatment, and highlight the concern that appropriate and diligent treatment simply does not produce remission in large groups of patients (Insel and Wang, 2009; Lieberman et al., 2005).
Given these constraints, it is inevitable that we will both become stuck and make mistakes, not as a function of inattentiveness or incompetence, but rather, as an unavoidable consequence of the nature of our profession. Further, this is substantially more common than we think. Diagnostic error occurs in approximately 15% of general medicine cases (Berner and Graber, 2008), and is likely more frequent in psychiatry, particularly in contested areas such as bipolarity, where approximately half of patients are misdiagnosed at some point (Smith and Ghaemi, 2010; Zimmerman, 2010).
Options for addressing our own fallibility are, of course, well described, and nearly every treatment guideline suggests we consider a second opinion or a tertiary referral in the face of treatment resistance (Malhi and Adams, 2009). However, while we all overtly endorse this, in the case of tertiary referral, this principle may be more honoured in the breach than in the observance. At the two major academic centres in Sydney that offer tertiary outpatient mood disorder assessment, most referrals come from GPs (Table 1). Fewer than 100 patients are referred by a psychiatrist annually, a number likely less than the number of psychiatrists in our shared catchment areas.
Referral patterns in tertiary assessment of mood disorders in Sydney.

There are numerous possible reasons for this apparent gap between the likely frequency of diagnostic difficulty and the engagement of tertiary expertise. It is possible, for example, that it is simply a parochial issue, or that it is due to factors unrelated to clinical decision making, such as awareness, or service capacity. The large proportion of GP referrals suggests a structural gap may also be present, with direct tertiary referrals filling some of the gulf between the public sector’s focus on severe mental illness and the private sector’s financial constraints. However, the relative underuse of tertiary expertise by psychiatrists may also reflect a broader failure to clarify the nature of tertiary assessment, and we therefore aim to use this paper to reflect on the way in which tertiary assessment intersects with psychiatric decision making.
Tertiary services and expertise
The first waypoint in most definitions of tertiary service is expertise. Almost all tertiary services invoke the concept, either through direct assertion or through endorsement of related homilies such as status as a ‘centre of excellence’. This is not an unreasonable proposition, as many of these services are run by highly experienced clinicians who can legitimately make such claims, and it seems superficially reasonable that an impasse at a secondary level should be resolved by triangulating in someone with more expertise. However, this is far more complex than it appears.
Specifically, if we differentiate secondary and tertiary care on the basis of expertise, this implicitly creates a challenge to the competency of the referrer. That is, in order to refer on the basis of expertise, a referrer must acknowledge that they have reached the limit of their confidence, which is inherently difficult. Professional self-esteem and therapeutic relationships are built on confidence in one’s skill, and any discussion of clinical acumen thus risks becoming a narcissistic threat which triggers defensiveness. If we define tertiary referral as an expertise-driven exercise, then it is easy to pursue only when this threat is somehow defused or counterbalanced; for example, when the referral pertains to issues peripheral to our professional sense of self (as with a presentation outside our area of interest), or when our discomfort rises to a point where it is unavoidable (as with a patient who is so ill or risky that we want to share responsibility). Reliance on expertise is even further complicated by the recognition that clinicians are biased towards overconfidence, such that we tend to overestimate our grasp on our patients’ problems (Berner and Graber, 2008).
Additionally, empirical examination of medical decision making suggests that lack of expertise is not the main reason for error. The hoary aphorism that ‘more is missed by not looking than not knowing’ turns out to be true indeed, as most medical errors stem from subtle cognitive biases or blind spots, rather than from a deficient fund of knowledge (Crandall and Wears, 2008). Further, these blind spots are better addressed by process and systemic factors (Graber et al., 2012; Singh et al., 2012), rather than cognitive sophistication or cleverness (West et al., 2012).
Expertise, then, is unlikely to function well as the sole anchor for tertiary care. Rather, it may be helpful to consider how clinical decision making goes wrong, and how the tertiary process might address this from a systemic perspective.
Tertiary services and clinical decision making
Current models divide expert thinking, such as medical diagnosis, into two interlocking modes of thought: the first is rapid, associative/heuristic and intuitive, and the second is slow, systematic and analytical (Norman and Eva, 2010). In psychiatry, as in any expert endeavour, problems are usually approached using the intuitive model first. In this mode of thinking, rather than computationally analysing information, we automatically generate and confirm hypotheses by comparing the current situation to internal mental heuristics or maxims. These are not strict representations of evidence, but rather, fluent paradigms derived from our own experience.
This is rapid, efficient, and usually correct. However, it is also fallible – we are inevitably sometimes wrong. The process works well when a classic problem presents classically, as this fits effortlessly into our heuristics, and treatment proceeds accordingly. However, because intuitive thinking is affirmative rather than sceptical, when a patient’s presentation meshes poorly with our heuristics, we tend to slot it into those patterns regardless, and often fail to realise that this has occurred. If treatment fails, therefore, we are at risk of progressing to the next step in the treatment algorithm rather than revisiting the diagnosis, and attributing the problem to the patient’s pathology rather than our own error. Systematic consideration using the second, analytical approach has the potential to counter this, but we must both realise it is necessary and undertake it rigorously.
Once viewed from this perspective, a reconfiguration of the role of tertiary referral in psychiatry becomes necessary. If tertiary care is built around expertise, then relatively little is added to secondary care – it simply brings another individual’s heuristic to bear, and we must have faith that the person knows more than we do. However, if tertiary referral is conceptualised as an opportunity to address the possibility of cognitive error, this opens up a much more substantive field, as the frame of assessment can be designed to illuminate blind spots and address potential errors.
The two conceptualisations of tertiary care are quite different, and they create quite different patterns of engagement and referral, both of which we see at our own tertiary service, the CADE Clinic (Clinical Assessment and Diagnostic Evaluation Clinic; www.cadeclinic.com).
Specifically, the two different paradigms are associated with different questions at the point of referral. Those who use an expertise-based model tend to present a synopsis and ask for treatment advice, funnelling the assessor towards a specific question about the next step within the referrer’s paradigm. Alternatively, those who are implicitly endorsing a decision-making model tend to ask for a fresh approach, and thus, explicitly recognise their own fallibility and invite fresh formulation. The relative strength of the two approaches becomes immediately clear when the possibility of diagnostic error is raised. For example, if one asks, ‘what medication should I give to this treatment-resistant bipolar patient?’, then this does not address the possibility that the patient is not in fact bipolar, whereas asking ‘what if there is something I’ve missed?’ allows a more full discussion.
Building a tertiary assessment frame
If we want to approach tertiary assessment through the lens of decision making, however, then we need to explicitly consider how it can add value to secondary assessments.
Reassessment itself
The first element of this discussion is the simple observation that reassessment itself is an error-checking strategy which improves decision making (Croskerry, 2003). Any referral outside the basic dyad will bring to bear a new heuristic for comparison, and thereby either validate or redirect formulation. However, the enrichment which this offers has to be weighed up against the fear that someone else will destabilise the therapeutic relationship, override our frame, and perhaps upset the apple cart altogether. A second opinion from a close colleague is a ‘safe bet’ in this regard, but also potentially less rewarding, as someone who has a very similar mindset to us may recreate the same errors we made ourselves. Tertiary referral ought to be ideally placed to negotiate this dilemma, as it allows a heuristic from outside our immediate professional world, but in order for this to function fluently, the transaction needs to be negotiated in advance. The tertiary service must have freedom to fully reassess and reformulate, but the process must be collaborative and must enrich, rather than override, the secondary care dyad.
Reassessment, therefore, is not a rescue from recalcitrant difficulty, but rather, a routine error-checking mechanism which supports good practice by performing the sort of detailed assessment that may be impractical for the referrer.
Multiple minds
This process of reassessment is also improved by the number of different heuristics brought to bear on a single patient. Simple checking of our own heuristic is routine, and occurs when we discuss the case with another psychiatrist, but in tertiary referral, we can enrich the process by routinely involving an experienced group, all of whom consider every case. The clinical team at CADE, for example, usually includes three psychiatrists (with a range of interests), along with clinical and research psychologists (again with varied interests), and an advanced trainee. This allows every assessment to be parsed through multiple paradigms simultaneously, with different ideas iteratively considered, evaluated and integrated. This process is such an integral part of our clinic that we do not see patients unless we have a quorum of assessors.
Time and information gathering
Adequate information gathering is also a rate-limiting step in formulation, and this is a salient risk to any cross-sectional assessment. However, systematic enquiry picks up a great deal of relevant information that is missed in routine care. For example, the Black Dog Institute recently noted that tertiary assessment identified previously unrecognised information relevant to formulation in over half of cases (Parker et al., 2011), and Stevenson and colleagues (2011) demonstrated that a structured interview identified personality disorder at approximately five times the frequency of routine care. Both these series use structured and systematic information gathering methodologies to explicitly avoid blind spots in information gathering, which may be both impractical in a generalist setting, and necessary in the context of treatment failure.
It is worth noting, however, that information is gathered to enrich formulation, not to supplant it. Questionnaires and automated assessment tools currently do not have good enough psychometrics to replace proper assessment (Lampe and Hagiwara, 2013; Zimmerman and Galione, 2011), and anything that suggests diagnosis risks funnelling a clinician towards a particular paradigm, and thereby creating, rather than eliminating, bias. Diagnostic prompting may be a helpful strategy in primary care, where diagnostic awareness may be limited, but, in tertiary care, a heuristic-matching approach may foster bias rather than eliminating it, and we should therefore provide unvalenced information for clinical assessment, rather than suggesting diagnosis even before we have seen the patient.
Formulation-centric assessment
Fluent formulation is an explicit synthesis of both intuitive and analytical modes of thinking, which is central to psychiatric practice. Unfortunately, surprisingly few of our referrals contain a formulation (Table 2a). Some referrals are excellent, and are striking for their clarity and for a depth of understanding that reflects great empathy and long engagement with the patient, and psychiatrists are unsurprisingly well ahead of GPs in this regard. At a cohort level, however, we see a bias towards the provision of medical-model information, such as symptomatology, axis I diagnosis, and medication history. Psychological information is typically addressed as a list of modalities trialled, with a note as to the success or otherwise of each; social information is variably included. Formulation is often not explicitly addressed, and although many referrals outline past treatment failures, remarkably few postulate barriers to recovery or the steps taken to address them. This pattern might simply reflect an unrecognised bias in the composition of our cohort, but given that our recommendations tend to emphasise psychological and pharmacological care equally (Table 2b), this seems relatively unlikely. Our two most common recommendations, for example, are rationalisation of medication regime, and exploration of new avenues of psychological treatment (particularly around under-emphasised attachment or stage of life difficulties and personality factors).
Content in CADE referrals (a) and reports (b).
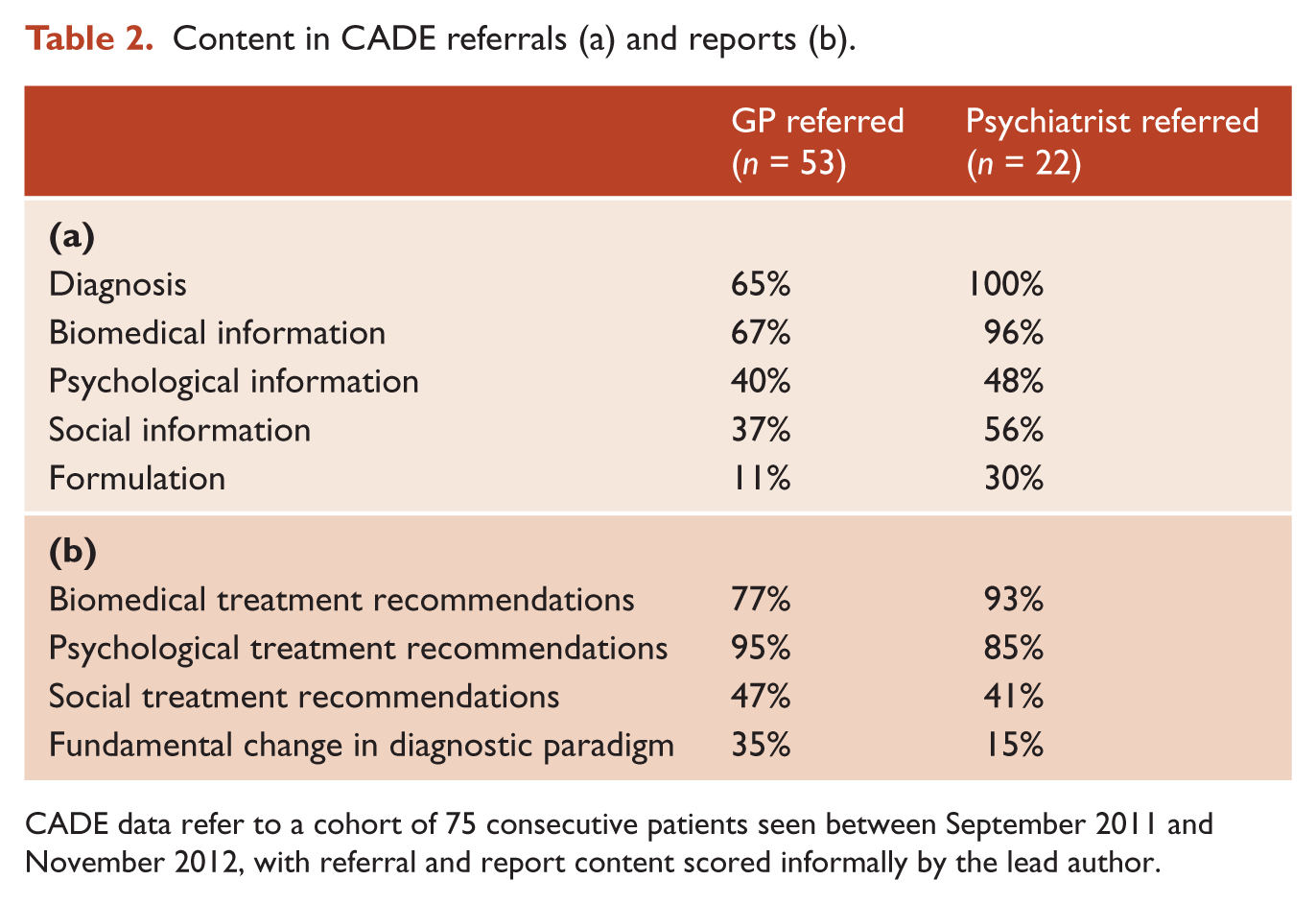
CADE data refer to a cohort of 75 consecutive patients seen between September 2011 and November 2012, with referral and report content scored informally by the lead author.
The methodological quality of these data is low, and it is certainly possible that the apparent pattern is an artifact of the informal scoring methodology, our own theoretical bias, or both. However, our findings echo well-demonstrated trends in current psychiatric practice, such as the emphasis of diagnosis at the expense of personality factors (Rosenbluth et al., 2012), and it certainly seems plausible that the dominant biomedical paradigm creates subtle cognitive biases that shape practice.
Conclusions
If we accept the old idea that it is human to err, and the rather more confronting proposition that this applies to us routinely, then we need a way of checking for the errors that will inevitably arise. Tertiary assessment provides an opportunity to address this by building a frame which bypasses many of the limitations inherent in secondary care, such as time constraints or diversion of attention towards crisis management, and directly addresses sources of potential diagnostic error. Systematic information gathering methodologies explicitly invoke rigorous analytic thinking as a necessary substrate for formulation, and routine discussion with multiple assessors minimises the risk that a single individual’s blind spots or cognitive biases will distort care. Explicit focus on formulation as a necessary component of assessment also mandates that the assessor must engage both intuitive and analytic modes of thinking in order to address the presentation. Finally, this is all facilitated by the availability of time and resources that would both be impractical and impossible to adequately reimburse as core features of secondary care.
This repositions tertiary care substantially. It shifts the interaction away from an expertise-driven model, in which the tertiary assessor is implausibly lionised as a virtuoso thinker who cuts the Gordian knot, and towards a more sensible and collaborative model, in which it is a routine response to error-prone practice in a difficult area.
Footnotes
Funding
We acknowledge funding from an NHMRC Program Grant #510135.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.