
Abstract

Introduction
Autoimmune disorders often remain undetected in psychiatric settings. Many patients who present to mental health services and are treated for a primary psychiatric diagnosis may have an autoimmune disorder of the central nervous system that responds to immunotherapy (Lennox et al., 2012). New research has identified a growing number of antibodies to receptors and ion channels in the central nervous system (Kayser and Dalmau, 2011). The related autoimmune neurological disorders can present as disorders of affect, perception, thought, cognition, sleep and consciousness. They are under-recognized in psychiatric practice, often leading to inappropriate treatment and poor outcomes.
Liaison and neuropsychiatry services have begun to identify and treat these disorders in conjunction with neurology, gynaecology, oncology and general medical services. However, clinical pathways are poorly defined. This leads to delays in investigation and initiation of appropriate treatment. Once appropriate immunotherapy has been commenced on a neurological ward, their behavioural manifestations can render multidisciplinary care challenging.
The prototypical disorder in this group is autoimmune limbic encephalitis. This was once considered a rare disorder, almost always related to cancer, and refractory to treatment. New evidence shows that limbic encephalitis is a relatively frequent disorder that is often unrelated to cancer, and can respond to treatment. The new antibodies described are directed against neural surface proteins, unlike the classic paraneoplastic onconeural antibodies that are directed against intracellular antigens. This distinction is crucial as disease associated with neural surface proteins responds well to immunotherapy, unlike that associated with intracellular antigens (Tuzun and Dalmau, 2007).
The newly described antibodies include those directed against the voltage-gated potassium channel (VGKC) complex, the N-methyl-d-aspartate (NMDA) receptor, the alpha-amino 3-hydroxy 5-methyl 4-isoxazolepropionic acid (AMPA) receptor and the gamma-aminobutyric acid type B (GABA-b) receptor (Kayser and Dalmau, 2011). They can be detected by simple blood or cerebrospinal fluid (CSF) tests. Good outcomes are associated with early treatment (Somers et al., 2011). A recent study suggests that a significant proportion of patients presenting with a first episode of psychosis have autoantibodies suggesting an underlying autoimmune illness (Steiner et al., 2013). Other presentations include anxiety, depression, confusion, amnesia, personality change, seizures and sleep disturbances (Tsutsui et al., 2012). The discrimination between functional psychiatric presentations and the psychiatric presentations of autoimmune neurological disorders can be difficult.
Care pathways in western psychiatric practice have been subject to progressive demedicalization in recent years. Referrals may be assessed by practitioners with little experience of clinical medicine. This jeopardizes the timely identification and treatment of these disorders. This emerging scenario calls for the closer integration of psychiatry with neurology and the rest of clinical medicine. The current situation where psychiatry and its practitioners have retreated into an institutional silo is becoming unsustainable.
Clinical spectrum of neural surface protein autoimmunity
Voltage-gated potassium channel (VGKC) complex antibody encephalitis
VGKC complex autoimmunity can be encountered in both idiopathic and paraneoplastic contexts, in adults and children. It has a spectrum of neuropsychiatric manifestations. Patients usually present with confusion, memory problems and seizures (Vincent et al., 2004). Hyponatraemia is common. They have a high prevalence of psychiatric symptoms and can present to psychiatric services (Table 1). Such patients can also present with characteristic facio-brachial dystonic seizures that precede neuropsychiatric manifestations and changes on magnetic resonance imaging (MRI). These can be misinterpreted as myoclonic jerks or functional motor symptoms (Irani et al., 2011).
Clinical profile.
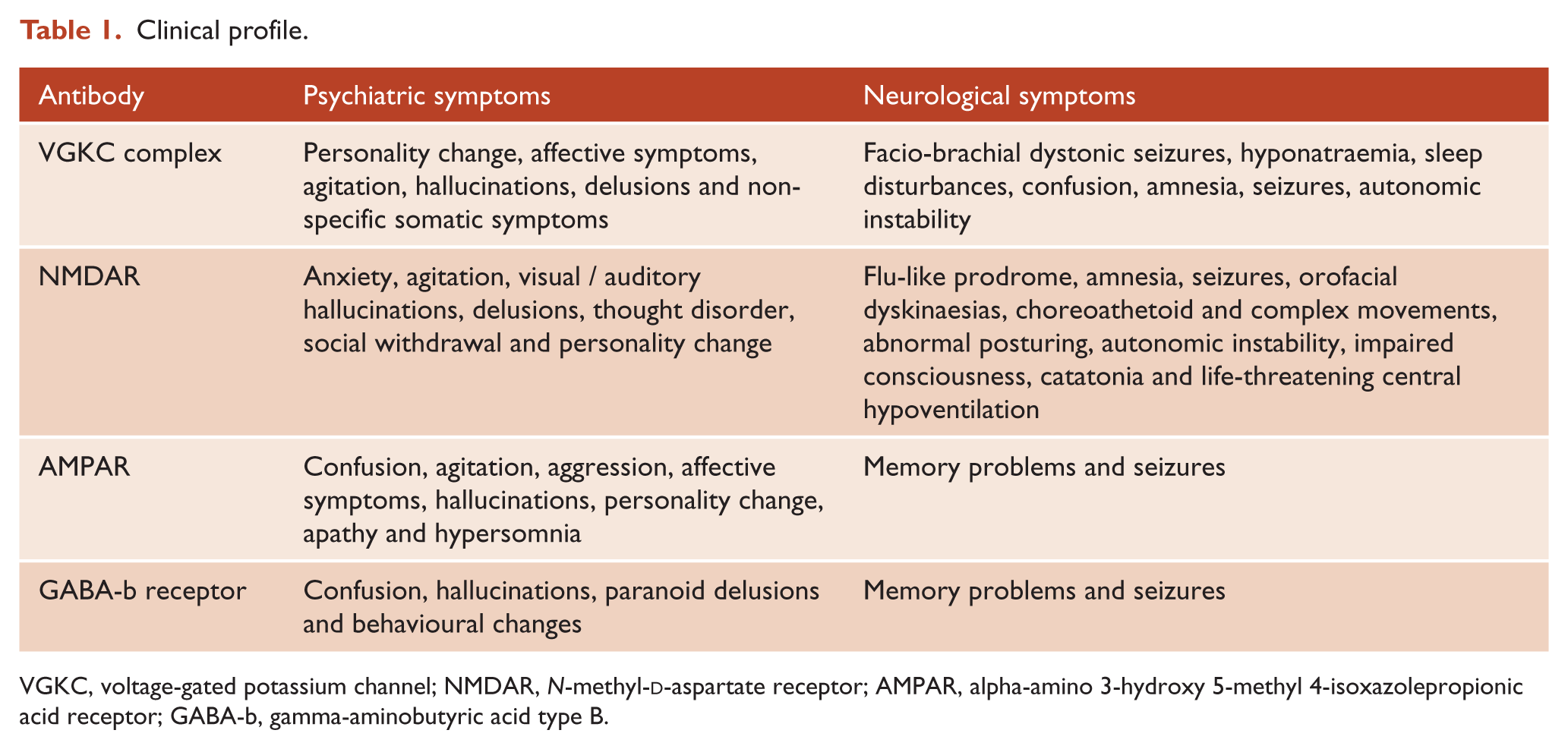
VGKC, voltage-gated potassium channel; NMDAR, N-methyl-d-aspartate receptor; AMPAR, alpha-amino 3-hydroxy 5-methyl 4-isoxazolepropionic acid receptor; GABA-b, gamma-aminobutyric acid type B.
Patients with medium or high VGKC complex antibody titres (> 10 nmol/litre) are significantly more likely to have neuropsychiatric presentations (Somers et al., 2011). Confusion, amnesia, objective neurological signs and limbic encephalitis are common in those with a florid neuropsychiatric decompensation. These patients tend to have characteristic abnormalities on MRI viz. hippocampal atrophy or hyperintensity on the medial temporal lobes. Patients with milder neuropsychiatric presentations tend to present with affective symptoms and nonspecific somatic complaints, and are less likely to demonstrate neurological signs or MRI findings (Somers et al., 2011). Antibody levels are higher in serum than CSF (Vincent et al., 2004). Though the majority of seropositive adult patients are cancer-free, diverse cancer types have been detected in the rest. Prognosis depends on time to initiation of immunotherapy and removal of tumours where applicable. A significant proportion of patients need longer-term immunosuppression to maintain remission of symptoms.
N-methyl d -aspartate receptor (NMDAR) antibody encephalitis
NMDAR autoimmunity mostly occurs in young women and in the presence of a tumour, most frequently an ovarian teratoma. However, they can occur in other age groups and men, in the absence of identifiable tumours, and also in pregnancy (Dalmau et al., 2011). The majority of patients have a flu-like prodrome in the weeks preceding hospital admission, with a subacute-acute onset of illness. NMDAR antibody encephalitis is a two-stage illness. Patients usually present with prominent psychiatric symptoms (Table 1). Memory problems and seizures are as common but are often overshadowed by the psychiatric symptoms (Irani et al., 2010). In most cases, the illness progresses into a second stage within 10–20 days, with overt neurological symptoms (Table 1). This includes orofacial dyskinaesias, choreoathetoid and complex movements of the extremities, abdomen and pelvis, and abnormal posturing (Dalmau et al., 2011).
There is a correlation between NMDAR antibody titres and severity of illness: patients with higher titres have severe syndromes and poorer outcomes. Patients with tumours have higher titres of antibodies (Irani et al., 2010). When present, the best outcome occurs with tumour removal, usually in combination with immunotherapy. In their absence, good outcomes can be achieved with immunotherapy. In both instances, early initiation of treatment is critical to outcome. Levels of NMDAR antibodies are higher in serum than in CSF (Dalmau, 2011). Up to 55% can have hyperintensity on MRI in medial temporal lobes, corpus callosum and brainstem (Dalmau et al., 2008).
Alpha-amino 3-hydroxy 5-methyl 4-isoxazolepropionic acid receptor (AMPAR) antibody encephalitis
AMPAR autoimmunity is rare, and it generally presents as classic limbic encephalitis with neuropsychiatric symptoms, memory problems and seizures in women over the age of 50. Most patients have an identifiable tumour. Antibodies may be undetectable in serum but detectable in CSF (Graus et al., 2010). Though initial response to appropriate treatment is good, relapses are common – even in the absence of cancer recurrence (Kayser and Dalmau, 2011). Neuropsychiatric symptoms can occur in the absence of focal neurological symptoms. These patients did not respond to neuroleptics but made an excellent recovery with immunotherapy and oncological treatment (Bataller et al., 2010; Graus et al., 2010).
Gamma-aminobutyric acid type B (GABA-b) receptor antibody encephalitis
A recent case series describes limbic encephalitis associated with GABA-b receptor antibodies (Lancaster et al., 2010). The majority of affected patients were over 60 years; both sexes were represented. Patients present with prominent seizures, memory problems, confusion and may have psychiatric symptoms (Table 1). GABA-b receptor antibodies were detectable only in the CSF in three patients. Most patients had hyperintensity on MRI in the medial temporal lobe and one in the corpus callosum. The majority recovered with immunotherapy and oncological treatment.
Autoimmunity in psychiatry
The literature on autoimmune presentations includes cases of depression, anxiety, obsessive-compulsive symptoms, bipolar affective disorder, schizophreniform disorders and cognitive impairment. These are comorbid with either systemic (e.g. systemic lupus erythematosus, rheumatoid arthritis, antiphospholipid syndrome) or organ-specific (e.g. thyroid: Hashimoto’s encephalopathy) autoimmune diagnoses. Emergent psychiatric symptoms may not correlate with exacerbations of physical disease. Patients respond poorly to standard psychotropics but respond better with immunotherapy. However, immunosuppression can lead to infections, confounding diagnosis and management. Outcomes remain suboptimal.
Limbic encephalitis was first described in 1960 (Brierley et al., 1960). In the 1980s and 1990s, advances in neuroimaging and the discovery of several paraneoplastic antibodies directed against intracellular antigens (anti-Hu, anti-Ma2, anti-CV2/CRMP5, anti-Ri and anti-amphiphysin) culminated in the identification of several clinical-immunological variants (Tuzun and Dalmau, 2007). It was established that their occurrence had been underestimated; they were often associated with lung, thymic and testicular tumours. Though their prognosis is generally poor, even after tumour removal and immunotherapy, there is some awareness of these disorders within mainstream psychiatry.
Limbic encephalitis mediated by VGKC complex autoantibodies was identified in 2001 (Tuzun and Dalmau, 2007). Since then, data have steadily accumulated to support the role of ion channel and receptor autoimmunity in the pathogenesis of such disorders. Recent studies demonstrate that these autoantibodies also mediate disease in a subset of purely psychiatric disorders. Steiner et al. (2013) studied a clinically diverse German cohort, detecting NMDAR antibodies in 9.9% of patients with an initial diagnosis of schizophrenia, 2.8% with major depression, none with borderline personality disorder and 0.4% of controls. This supports findings by Zandi et al. (2011) who detected NMDAR antibodies in 6.4% of British patients with first-episode schizophrenia and VGKC complex antibodies in 2.1%. Other studies report NMDAR antibodies in 7.8% of a Japanese sample with schizophrenia and schizoaffective disorders (Tsutsui et al., 2012) and 2.9% of a German sample with psychosis (Choe et al., 2013). In all populations, seropositive patients met the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) criteria for diagnoses and had no differentiating clinical features.
Specific cases of first-episode schizophrenia with VGKC complex antibodies responsive to immunotherapy have been reported elsewhere (Parthasarathi et al., 2006). In a cohort of 6814 patients from the Mayo Clinic, VGKC complex antibodies were detected in 2.2%, of which 44% presented with neuropsychiatric symptoms and only 1.3% were initially treated for primary psychiatric diagnoses (Somers et al., 2011). Though Steiner et al. (2013) found no antibodies to AMPAR, case reports describe AMPAR antibodies in patients presenting with acute psychoses that responded well to corticosteroids (Graus et al., 2010).
The psychiatric manifestations of ion channel and receptor autoimmunity are diverse and protean. Despite this, discussion in the psychiatric literature has largely focused on psychosis (Lennox et al., 2012). This may be a symptom of the clinical priorities that drive publicly funded psychiatric services in the West.
Conclusions
Psychiatric diagnosis is based on symptom clusters that describe clinical syndromes rather than specific disorders with clear underlying pathophysiologic abnormalities. Individual diagnostic categories are heterogeneous and of uncertain aetiology, despite decades of research.
Does the presence of antibodies to neural surface proteins in limbic encephalitis, psychosis, depression and normal controls represent a spectrum of causal autoimmune seropositivity in the population? There is some evidence to support this proposition. The associations of NMDAR and VGKC complex antibodies with clinical presentations are strong, biologically plausible and consistent across studies. Patients with higher antibody titres develop more severe illness and have poorer outcomes. MRI abnormalities correlate with severity of clinical disease and antibody titres. Clinical improvement correlates temporally and quantitatively with a fall in antibody titres, resolution of MRI abnormalities and tumour removal. Preliminary evidence shows that the repertoire of antibody classes and NMDAR receptor subunit targets are wider in schizophrenia, major depression and controls compared to limbic encephalitis (Steiner et al., 2013).
What does this mean for psychiatry? If endophenotypes linked to detectable biomarkers can be identified, it would open an exciting new horizon for psychiatric research. It can potentially revolutionize our understanding of the aetiopathogenesis and presentation of mental disorders. It can transform treatment from symptom-focused strategies to strategies that tackle the cause of illness.
How should psychiatry respond to this challenge? Large sero-epidemiological studies are required to determine the frequency of these antibodies in the psychiatric population and identify endophenotypes. This is a pressing need, as treatment strategies and prognosis are significantly different in this subset of patients. The identification of a reliable clinical signature will enable screening and timely diagnosis, which would then lead to appropriate treatment and good outcomes.
Given this evidence, how should psychiatrists alter their clinical practice? Autoimmune limbic encephalitis should be considered as a differential diagnosis for all patients with a first-episode psychosis. The probability is heightened in the presence of a flu-like prodrome, protean disturbances of affect, perception and thought, memory problems, seizures, movement disorder, hyponatraemia, sleep disorders, confusion, autonomic instability and rapid deterioration. Milder forms of illness (formes frustes) with predominant or apparently isolated psychiatric symptoms, seizures or movement disorders can occur. Facio-brachial dystonic seizures, orofacial dyskinaesias and catatonia, as well as a poor treatment response (with/without episodes of hypotensive collapse) to antipsychotics should amplify suspicion. Potentially pathogenic autoantibodies to neural surface proteins should be considered as a likely causal influence even in the absence of limbic encephalitis.
As professionals with medical training, psychiatrists should be directly involved in screening all referrals and conducting initial assessments. This calls for a rethinking of current psychiatric training, clinical practice and service models to enable comprehensive diagnostic assessments with formulation of aetiology and diagnosis followed by specific treatments (Craddock et al., 2008). The assessment should include a cognitive, physical and neurological examination; we recommend a low threshold for early serological testing for antibodies against NMDAR and the VGKC complex. We also recommend testing for erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), a full blood count (FBC), serum electrolytes and anti-nuclear antibodies (ANA). CSF is not usually required but a clinical immunologist should be consulted for advice. Request an electroencephalogram (EEG) if the index of suspicion is high. Epileptiform discharges and encephalopathic features should trigger rapid referral and aggressive treatment. The finding of increased T2 or FLAIR signal in the medial temporal lobes is strongly suggestive of antibody-mediated limbic encephalitis and supports rapid treatment.
Treatment recommendations include early removal of tumours (if paraneoplastic) and intravenous or oral methylprednisolone in conjunction with plasma exchange, intravenous immunoglobulins or both, in order to reduce the level of antibodies quickly. Remission is maintained by either high-dose steroids, or steroids in conjunction with steroid-sparing immunosuppressants. Though recovery is often excellent, this is not always the case; patients can relapse, have persistent deficits and die. There is a significant correlation between clinical improvement and time to initiation of treatment; early detection and treatment are crucial to positive outcomes.
Treatment should be in collaboration with neurology and other general hospital colleagues. Joint case-conferences, explicit care pathways and psychiatric training for general hospital colleagues can improve outcomes. Liaison and neuropsychiatry services are already involved in managing neuropsychiatric symptoms, and challenging behaviour may require mental health nursing in the general hospital. Unless shared care protocols are developed and clinical psychiatry returns to its medical roots, the opportunity will pass and clinical pathways will become largely ‘neurologized’. That would be unfortunate, as these disorders offer a clinical combination hitherto unknown to psychiatrists: a characteristic clinical syndrome, a set of identifiable biological markers that are diagnostic, a quantifiable dose–response relationship with biomarkers and an excellent response to timely and appropriate treatment.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest.