
Abstract
Objective:
Schizophrenia patients experience impairments across various functional roles. Emotional unresponsiveness and an inability to foster intimacy and display affection may lead to impairments in parenting. A comprehensive cognitive understanding of parenting abilities in schizophrenia has the potential to guide newer treatment strategies. As part of a larger study on functional ability in schizophrenia patients, we attempted a cognitive deconstruction of their parenting ability.
Methods:
Sixty-nine of the 170 patients who participated in a study on social cognition in remitted schizophrenia were parents (mean age of their children: 11.8 ± 6.2 years). They underwent comprehensive assessments for neurocognition, social cognition (theory of mind, emotion processing, social perception and attributional bias), motivation and insight. A rater blind to their cognitive status assessed their social functioning using the Groningen Social Disabilities Schedule. We examined the association of their functional ability (active involvement and affective relationship) in the parental role with their cognitive performance as well as with their level of insight and motivation.
Results:
Deficits in first- and second-order theory of mind (t = 2.57, p = 0.01; t = 3.2, p = 0.002, respectively), speed of processing (t = 2.37, p = 0.02), cognitive flexibility (t = 2.26, p = 0.02) and motivation (t = 2.64, p = 0.01) had significant association with parental role dysfunction. On logistic regression, second-order theory of mind emerged as a specific predictor of parental role, even after controlling for overall functioning scores sans parental role.
Conclusions:
Second-order theory of mind deficits are specifically associated with parental role dysfunction of patients with schizophrenia. Novel treatment strategies targeting theory of mind may improve parenting abilities in individuals with schizophrenia.
Introduction
Patients with schizophrenia frequently experience extensive deficits in cognitive functions such as attention, planning, memory, processing speed and social cognition (SC). These social and non-social or neurocognitive deficits have a significant relationship with their functional impairment as is consistently demonstrated across various study designs (Fett et al., 2011; Hoe et al., 2012; Schmidt et al., 2012). Schizophrenia characteristically has an onset in the childbearing and early child nurturing years (Mowbray et al., 2005; Tandon et al., 2008) and results in severe impairments across personal, social and occupational spheres of the individual’s functioning, leading to substantial disability (Murray and Lopez, 1997; Tandon et al., 2008; Ustun et al., 1999).
One of the important consequences of this dysfunction is the impact on parenting capacity. Parenting has been defined as a transactional, purposive activity between children and parents aimed at ensuring the survival and development of children (Maccoby and Martin, 1983). It is a cross-species (Clutton-Brock, 1991) and pan-cultural (Leckman et al., 2004) role that an individual assumes to care for and nurture the progeny. The importance of good parenting cannot be understated as it shapes the child’s growth and development across all spheres and also fosters psychological development of the parent.
Parenting has been conceptualized as a multidimensional model (Belsky, 1984; Conley et al., 2004; Darling and Steinberg, 1993) that includes, in addition to contextual characteristics and child characteristics, innate parent psychological and illness characteristics (including schizophrenia). Key elements of parenting include responsiveness and control (behavioral and psychological). It has been suggested that cognitive processes operating in social contexts (empathy, emotion processing and intrinsic motivation) may underlie parental responsiveness. General cognitive processes (executive functions, decision making and selective attention) are proposed to underlie behavioral and psychological control (Baumrind, 1971; Conley et al., 2004).
Emerging factor analytic evidence points to two distinct (SC and neurocognition) patterns of cognitive deficits in patients with schizophrenia (Mehta et al., 2013). While neurocognition involves affect-neutral and more general information-processing abilities such as attention, memory and speed of processing, SC subsumes an inter-subjective quality, requiring reflective (meta-cognitive), affective and social inferential abilities to be applied in social interactions (Brothers, 1990; Dimaggio et al., 2008). SC encompasses the dimensions of theory of mind (ToM), emotion processing, attributional bias and social perception (Green et al., 2008). ToM or mental state attribution is the ability to infer intentions, dispositions and beliefs of the self and others (Baron-Cohen et al., 2001). It is broadly divided into first-order ToM (the capacity to infer ‘A believes that x’), second-order ToM (the capacity to infer ‘A believes that B believes that x’) and higher-order ToM that includes more complex mental state attributes such as recognition of faux pas or social blunders (Baron-Cohen, 1985; Brune, 2005). Emotion processing refers to accurately identifying and appropriately managing emotions, which is tested through facial or voice demonstrations of emotions (Green et al., 2008). Attributional bias (Green et al., 2005) refers to cognitive styles that reflect how people typically infer the causes of particular positive and negative events (e.g. patients with persecutory delusions often attribute negative events to others). Social knowledge and perception refers to one’s awareness about social roles, societal rules and social context, and the ability to identify these in social interactions (Green et al., 2008; Penn et al., 2008).
It is plausible that these higher cognitive functions applied in social situations are also applied during parenting. For example, ToM may be used in understanding the thoughts and behaviors of children before responding to them; emotion processing may also be used in perceiving and responding to the child’s emotional needs. Evolutionarily conserved hypothalamic-midbrain-limbic-paralimbic-cortical circuits act in concert to regulate emotional response, intrinsic motivation and reward in response to offspring (Swain et al., 2011). It has also been proposed that evolutionarily wired neuroanatomical networks and neuro-hormonal interplay (between oxytocin, vasopressin and dopamine) that handle social behavior (including parenting) are involved in the neurobiology of various human psychopathologies (including that of schizophrenia) (Leckman et al., 2004). Hence, patients with schizophrenia may be at risk of having difficulties with parenting.
In the second Australian national survey of psychosis, 28.3% of fathers and 21.3% of mothers with psychosis had obvious/severe impairments in their ability to care for their offspring (Campbell et al., 2012). Other studies have found mothers with schizophrenia to be more remote, silent, verbally and behaviorally intrusive, self-absorbed, flaccid, insensitive and unresponsive, and less demanding (Riordan et al., 1999) and with fewer mutually satisfying interactions with their children (Wan et al., 2007) when compared to mothers with affective disorders such as unipolar or bipolar depression. They have been described as being more likely to recognize their infants as passive and to misinterpret their affective cues (Cohler et al., 1970). The data are sparse for fathers with schizophrenia. The impact of paternal schizophrenia may be different from, and in some areas of functioning less than, the impact of maternal schizophrenia on the development of children (Phares and Compas, 1992).
Difficulties in parenting roles are experienced by schizophrenia patients even after clinical recovery (Wan et al., 2007), suggesting that antipsychotics may not be sufficient to enhance parenting-specific functional abilities. In a study to ascertain predictors of mother–infant interactions in major mental illnesses, a diagnosis of schizophrenia was a stronger predictor of poor mother–infant interaction than severity, duration of illness, higher medication dosage, socioeconomic status or poor social stability/support (Wan et al., 2007). Thus, subtler features such as social and neurocognitive deficits may better explain poor parental sensitivity in schizophrenia than the usual indicators of illness severity. The association of social and neurocognitive deficits with parenting has not been studied in patients with schizophrenia. A comprehensive cognitive deconstruction of parenting abilities in schizophrenia has the potential to guide newer treatment strategies. In this study, we explored the relationship between cognitive deficits and parenting role in parents with schizophrenia. Specifically, we aimed to assess how SC abilities relate with parental role dysfunction in patients with schizophrenia. We examined this relationship after controlling for effects of confounding factors, including neurocognition, motivation, insight and negative symptoms. We hypothesized that patients with parental role dysfunction would have greater SC deficits even after controlling for effects of confounding factors.
Methods
Subjects
The data for this study comes from a larger study on determinants of functional outcome in remitted schizophrenia patients (Bhagyavathi, 2011). The patients were diagnosed independently by two qualified psychiatrists according to Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) criteria and confirmed using the Mini-International Neuropsychiatric Interview (M.I.N.I.) (Sheehan et al., 1998). They fulfilled operational criteria for remission (scoring ≤ 3 on the Positive and Negative Syndrome Scale (PANSS) rated for the previous 6 months) in psychotic and disorganization dimensions, according to the proposed multidimensional criteria for symptomatic remission by The Remission in Schizophrenia Working Group (Andreasen et al., 2005). Patients with substance dependence in the previous 6 months (except nicotine), presence of co-morbid neurological or medical disorder, clinically diagnosable or self-reported visual or auditory impairment, current pregnant or postpartum state, clinically diagnosed intellectual disability and a score of ≤ 19 on the Hindi Mental Status Examination (Ganguli et al., 1995) were excluded from the study. All patients were on stabilized doses of antipsychotics 4 months prior to evaluation.
The Institute’s ethics committee approved the study and written informed consent was obtained from all participants. Sixty-nine out of 170 schizophrenia patients recruited for the larger study were parents and their parental role functioning was analyzed in this study.
Assessments
Parenting: Dysfunction in a parental role was assessed using the ‘parental role’ of the Groningen Social Disabilities Schedule (GSDS) (Wiersma et al., 1988). The GSDS is based on social role theory and is developed from the WHO-Disability Assessment Schedule (WHODAS-II). It is valid and applicable across different cultures, as it takes a reference group from each culture for making precise comparisons to assess a person’s dysfunction. The information was obtained from reliable caregivers with whom the patients were staying. In the GSDS, parental role is assessed in two dimensions: active involvement (the patient’s role in raising children, disciplining them and engagement in joint activities, the presence of problems in relationships and the ability to solve them) and affective relationship (quality of the relationship, mutual concern and attachment, sharing of each other’s feelings, talking openly, handling criticisms and quarrels). Dysfunction is rated as none (0), mild (1), moderate (2) and severe (3) for each of these dimensions. The overall role score equals the higher of the dimensional ratings.
Social cognition: Consistent with recommendations of the Measurement and Treatment Research to Improve Cognition in Schizophrenia New Approaches Conference (Green et al., 2005) and the National Institute of Mental Health (NIMH) sponsored meeting ‘Social Cognition in Schizophrenia: Basic Definitions, Methods of Assessment, and Research Opportunities’ (Green et al., 2008), we selected four domains of SC: ToM, emotion processing, social perception and knowledge, and attributional bias. ToM, social perception and attributional bias were assessed using the Social Cognition Rating Tools in Indian Setting (SOCRATIS) (Mehta et al., 2011). Emotion processing was assessed using the Tool for Recognition of Emotions in Neuropsychiatric Disorders (TRENDS) (Behere et al., 2008).
Theory of mind: Tasks included two each of first-order (based on the Sally–Anne (Wimmer and Perner, 1983) and Smarties (Perner et al., 1987) tasks) and second-order (based on the ice-cream van (Perner and Wimmer, 1985) and missing cookies (Stone et al., 1998) tasks) false belief picture stories, two metaphor-irony stories (adapted from Drury et al., 1998) and 10 faux pas recognition stories (based on the faux pas recognition test (Stone et al., 1998)). These story-based tasks examined the ability, at different complexity levels, to ‘meta-represent’ the mental states of others (e.g. Suresh thinks that Rani will go to the temple area to buy the ice-cream because she has not seen the ice-cream man go towards the school). Social perception: A set of 18 true/false questions were asked on social (e.g. Ali asked many questions about the movie because he was trying to impress Sunil) and non-social cues (e.g. Harish and Lakshmi were looking over a book together) after showing the subjects four each of low and high emotion videos depicting a social interaction. This test was adapted from the social cue recognition test (Corrigan and Green, 1993). Emotion processing: Facial emotion recognition ability was assessed using 52 static images and 28 dynamic videos portraying two different intensities (low and high) of six basic human emotions (happy, sad, fear, anger, surprise and disgust) depicted by four trained actors (one young male, one young female, one older male and one older female). Attributional bias: This was assessed using a 32-point questionnaire where subjects were required to make causal attributions for positive and negative social events, adapted from the Internal, Personal and Situational Attributions Questionnaire (Kinderman and Bentall, 1996). Both these test batteries SOCRATIS and TRENDS have been validated in the Indian cultural setting with satisfactory psychometrics in terms of content, construct and known-groups validity, and internal consistency. Each test except the attributional biases provides an index of the respective test performance, which is equivalent to the score of an individual on the test divided by the maximum score possible (Mehta et al., 2011). For attributional styles, external and personalizing bias scores were calculated according to Kinderman and Bentall (1996).
Neurocognition: Standardized tests were used from the National Institute of Mental Health and Neuro Sciences’ (NIMHANS) neuropsychological battery to assess speed of processing and cognitive flexibility (Color Trails Tests A and B (D’Elia et al., 1994), Digit Symbol Substitution Test (Wechsler, 1981)), verbal learning and memory (Rey’s Auditory Verbal Learning Test (Rey, 1941)), visual learning and memory (Rey–Osterrieth Complex Figure Test (Osterrieth, 1944)) and planning (Tower of London test (Shallice, 1982)).
Symptom assessment: PANSS (Kay et al., 1987) was used to define ‘remission’ status and to assess the psychopathology of the subjects.
Insight: The Scale to Assess Unawareness of Mental Disorders (SUMD) (Amador et al., 1994) was used to assess clinical insight (combined awareness and attribution scores) of patients.
Motivation: The motivation subscale of the Quality of Life Scale (Heinrichs et al., 1984), which is a measure of deficit schizophrenia, served as a proxy for intrinsic motivation.
All the tests were completed on the same day, in divided sessions.
Statistical analysis
Independent samples t-test and χ2 test were used to examine differences in independent variables (social and neurocognition, insight, negative symptoms, motivation, age, gender, duration of illness/remission, education and socioeconomic status) across patients with parental role dysfunction (score > 1 on parental role of the GSDS) and those without (score = 0). Effect sizes of the differences were estimated using Cohen’s d (Cohen, 1988). Variables having a significant relationship with parental role functioning in univariate analysis were used as independent variables in a logistic regression analysis with parental role functioning as the dependent variable.
Results
Clinical and socio-demographic data
A total of 69 schizophrenia patients who were parents, with a mean (SD) age of 38.01 (9.5) years and education of 10.39 (4.29) years were studied; 45% (n = 31) were mothers. The majority (56.5%) were of middle socioeconomic status. A total of 54 (78.3%) patients had a diagnosis of paranoid schizophrenia. The mean (SD) duration of illness was 107.1 (88.75) months. Symptom scores, as expected, were low (mean (SD) of 7.42 (0.77) and 10.49 (4.12) for positive and negative symptoms, respectively, as measured by PANSS) as patients were under remission for a mean (SD) of 18.57 (17.79) months. Forty-eight (70%) had no or a mild overall disability (mean GSDS score = 0–1); 21 (30%) had a moderate to severe overall disability (mean GSDS score > 1). All patients who were parents were married; none was divorced and only four (5.8%) were living separately from their spouses. None had co-morbid substance use dependence (except nicotine). Their offspring’s ages averaged (SD) 11.86 (6.20) years. Fifteen (21.7%) patients had children in the pre-school age range (0–5 years), 41 (59.4%) patients had children in the age range 6–16 years and 13 (18.8%) patients had children > 16 years age. A total of 58 (84.1%) patients had one or two offspring and all the offspring were their biological children.
Parental roles
Figure 1 depicts the parental roles of the 69 patients. Eighteen (26.1%) and 24 (34.7%) had mild to moderate dysfunction in the affective relationship and active involvement dimensions, respectively. Overall, 30 (43.5%) patients had mild to moderate dysfunction in their parental roles.
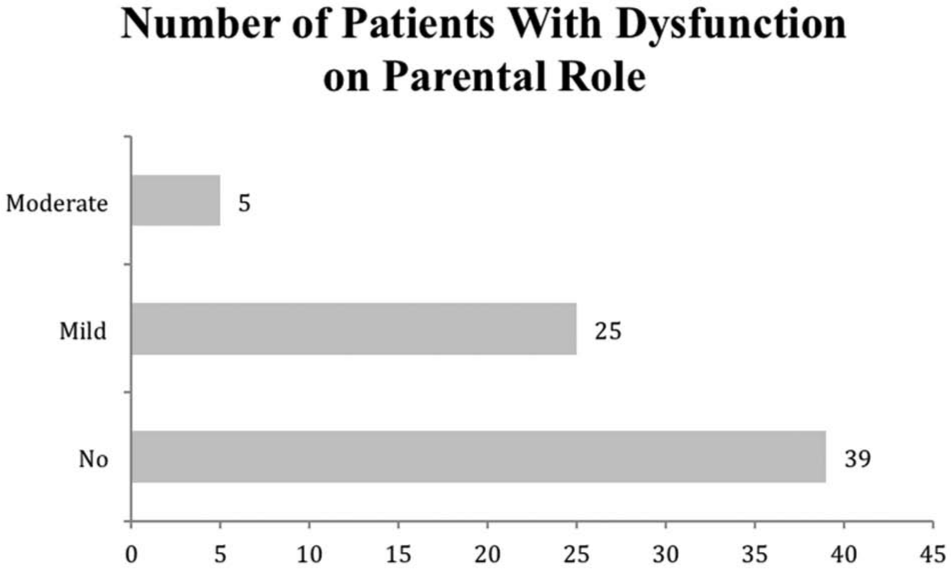
Distribution of parental role dysfunction in schizophrenia patients (n = 69).
Relationship of cognition, symptoms and socio-demographic characteristics to parental role
Table 1 presents the results of the independent samples t-test to assess the relationship of symptoms, neurocognition and social-cognition with the presence of dysfunction on parental role. Lower ToM ability (first-order ToM (Cohen’s d = 0.61) and second-order ToM (d = 0.81)), longer duration to complete trail-making A (d = 0.64) and B (d = 0.53) and lower motivation scores (d = 0.66) were observed in patients with dysfunction on parental roles than those with no dysfunction. We adjusted for multiple testing (eight SC variables were tested as part of the primary aim) using Bonferroni correction (corrected error probability of 0.05/8 = 0.006), following which only second-order ToM remained significant (p = 0.002). Table 1 also shows the relationship of various socio-demographic variables with dysfunctional parental role assessed using independent samples t-test and χ2 test. None of these variables differed significantly between the patients with and without parental role dysfunction. We also examined the differences in SC scores between fathers and mothers with schizophrenia and found no statistically significant differences (data not shown).
Socio-demographic, clinical and cognitive predictors of dysfunction in parenting role.
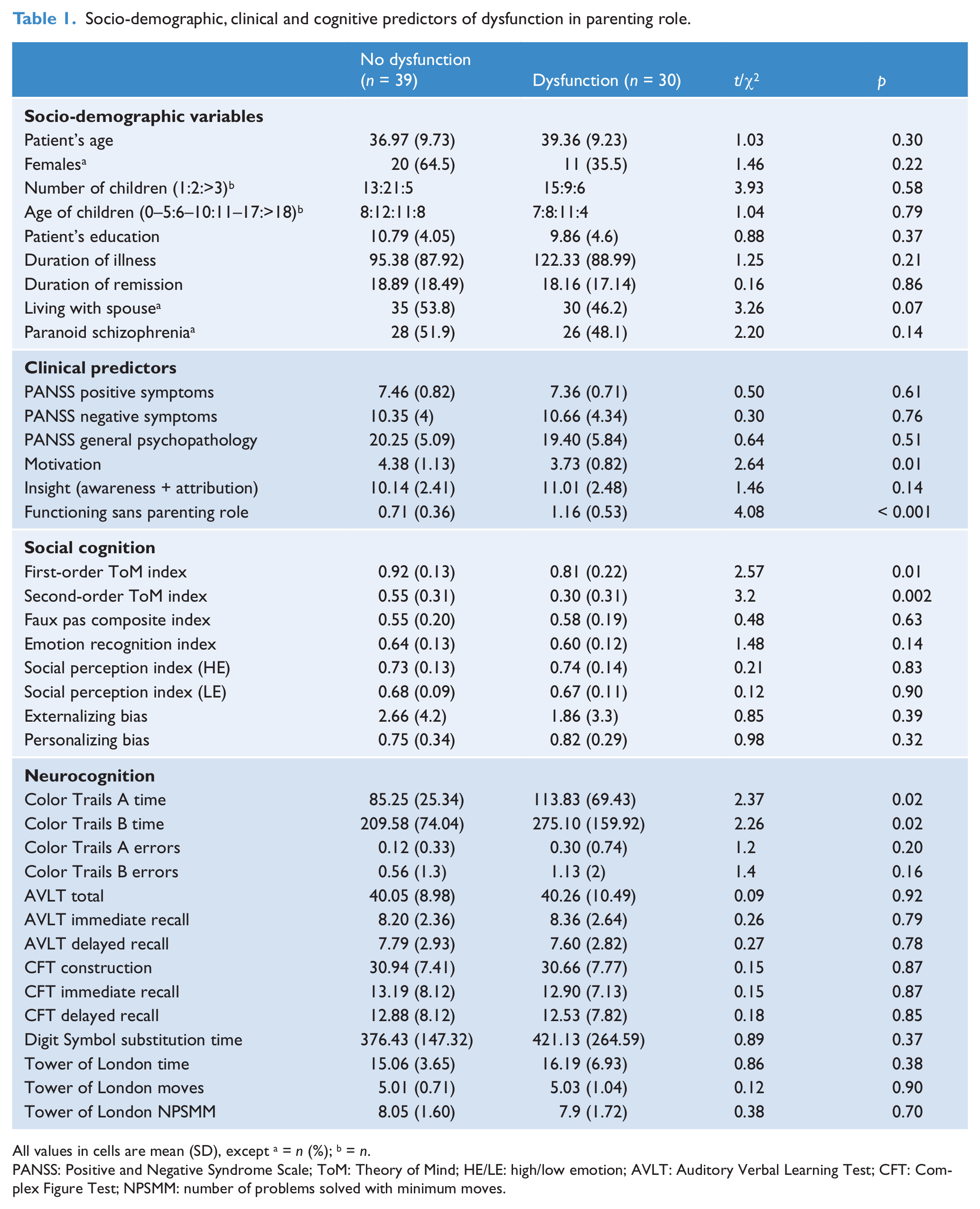
All values in cells are mean (SD), except a = n (%); b = n.
PANSS: Positive and Negative Syndrome Scale; ToM: Theory of Mind; HE/LE: high/low emotion; AVLT: Auditory Verbal Learning Test; CFT: Complex Figure Test; NPSMM: number of problems solved with minimum moves.
We conducted a multivariate logistic regression analysis with parental role dysfunction as the dependent variable and variables that showed significant (uncorrected error probability) association with the dependent variable in univariate analysis (i.e. first- and second-order ToM indices, time taken to complete Color Trails A and B, and motivation) as independent variables. The model comprising the second-order ToM index (adjusted odds ratio = 0.093, p = 0.01) and time taken to complete Color Trail A (adjusted odds ratio = 1.01, p = 0.08) was significant (χ2 = 24.9, df = 3, p < 0.001) and could classify 71% of subjects correctly.
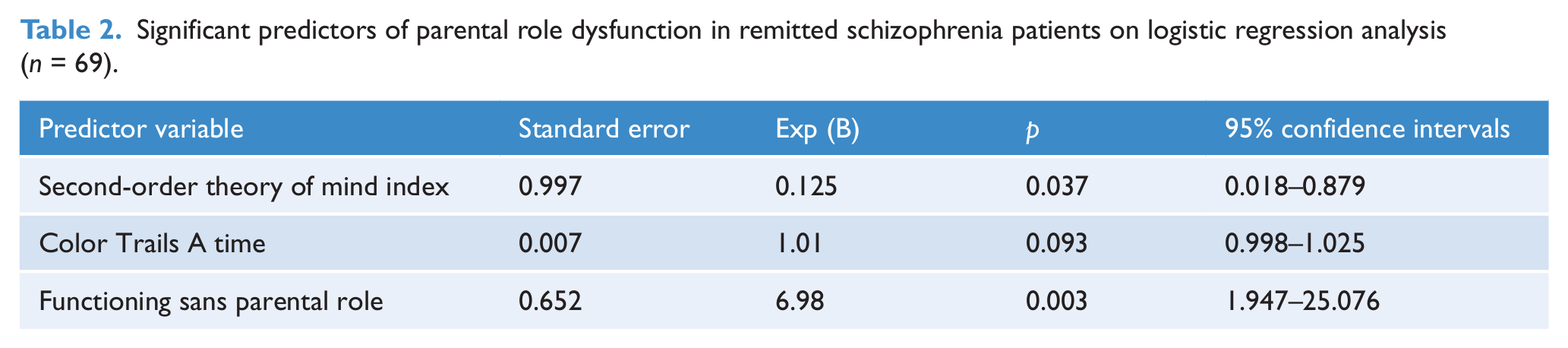
Additionally, in order to control for the effect of overall social dysfunction and gender of the parent on the association between predictor variables and parental role functioning, we included the mean GSDS score (without the parental role (mean = 0.91, SD = 0.49)) and gender (father versus mother) as independent variables in the regression analysis. The model comprising the second-order ToM index (adjusted odds ratio = 0.125, p = 0.037), time taken to complete Color Trail A (adjusted odds ratio = 1.01, p = 0.093) and overall functional ability (group mean GSDS without parental role score) scores (adjusted odds ratio = 6.98, p = 0.003) was significant (χ2 = 24.9, df = 3, p < 0.001) and could classify 76.8% of subjects correctly. Table 2 shows that the second-order ToM index continued to have a significant association with parenting role dysfunction (p = 0.037) after controlling for the effect of overall functioning.
Significant predictors of parental role dysfunction in remitted schizophrenia patients on logistic regression analysis (n = 69).
Lastly, to ascertain whether the age of offspring had an impact on the relationship between cognition and parental role, we repeated the above-mentioned logistic regression for patients with children aged 16 years and under (n = 56). The model comprising the second-order ToM index (adjusted odds ratio = 0.06, p = 0.010) and the overall functional ability (group mean GSDS without parental role score) (adjusted odds ratio = 4.95, p = 0.019) was significant (χ2 = 17.32, df = 2, p < 0.001) and could classify 68% of subjects correctly.
Discussion
Patients with schizophrenia experience difficulties in cognitive abilities and various functional roles. The parental role is an important dimension of functioning that has gained importance over recent years. Though the cognitive basis of functioning in general has been extensively researched, there is a scant evidence base regarding the cognitive determinants of the parental role in schizophrenia. Cognitive remediation strategies (Eack et al., 2011) are increasingly finding a place in recovery-oriented treatment programs and are found to have encouraging results in enhancing the functioning of patients. An attempt at cognitive deconstruction of parenting in schizophrenia during the symptom remission stage will highlight the important cognitive predictors of parenting. This has the potential to guide emerging parenting intervention programs tailored for parents with schizophrenia.
This research investigated the social and neurocognitive basis of parental role dysfunction in schizophrenia patients remitted from positive and disorganization symptoms. Results indicated that first- and second-order ToM, speed of processing, cognitive flexibility and motivation were significantly associated with parental role dysfunction. A model comprising second-order ToM and speed of processing was found to significantly predict parental role functioning. Other socio-demographic and clinical parameters such as gender, age of parents and children, education of patients, marital status, type of schizophrenia, duration of illness and remission, symptom scores and insight did not have any association with parental role dysfunction. Interestingly, all the patients in this study were married and only a small minority was separated from their spouses with none being legally divorced. This reflects the important cultural differences demonstrated in previous studies that have shown higher rates of marriage and lower rates of separation in patients with schizophrenia in India than in developed countries (Hutchinson et al., 1999; Murthy et al., 1997; Thara and Srinivasan, 1997).
These findings support the role of second-order ToM deficits in determining parental role dysfunction in schizophrenia patients who are remitted from positive and disorganization symptoms. That second-order ToM deficits were associated with parental role dysfunction after controlling for their association with overall functioning sans the parental role is particularly interesting as it indicates a specific association between second-order ToM deficits and parental role dysfunction. Second-order ToM classically involves our capacity to infer what one person – other than the self – thinks about another person’s thoughts. It is unsurprising as these are necessary cognitive abilities for developing and maintaining an affective relationship between parent and child and are proposed to underlie parental responsiveness (Baumrind, 1971; Conley et al., 2004). It is also of relevance given the theoretical and empirical basis of parenting capacity from an evolutionary perspective and its link to the origins of psychopathology (Belsky et al., 1991; Leckman et al., 2004). Social and neurocognitive processes have been proposed to underlie parental responsiveness and behavioral/psychological control, respectively (Conley et al., 2004). The findings of this research support a cross-sectional association of ToM with parenting abilities in schizophrenia patients. Prospective studies are needed to establish a causal role for ToM and neurocognition in parenting ability. We did not find any gender difference in the parenting ability of schizophrenia patients. This may indicate a common cognitive deconstruction of parenting across maternal and paternal roles. None of the socio-demographic or clinical parameters including insight had any association with parenting. This is consistent with findings in an earlier study (Wan et al., 2007). Interestingly, the majority of our patients (56.5%) had no parenting impairments. This is despite the fact that no attempt was made to choose only high-functioning patients.
These findings are fundamental in the light of the recent trend of parenting intervention programs (Barlow and Coren, 2001), some of which are tailored for parents with schizophrenia – and mothers in particular. The associations of second-order ToM and speed of processing with parental role dysfunction underscores the need to include cognitive remediation elements. Perspective taking, context appraisal and affect regulation by training in the accurate perception of and appropriate response generation to verbal/non-verbal cues, by means of role plays, video feedback and experiential practical exercises, through individual and group-based sessions, may be incorporated in such parenting interventions (Eack et al., 2007; Phaneuf and Lee McIntyre, 2007). Novel methods to improve ToM (the imitation-inhibition training exercise) can also be employed in such interventions. Here, subjects are trained to inhibit their tendency to the imitate actions of others. This has been shown to enhance their ability to adopt the perspectives of others (Santiesteban et al., 2012). Such an intervention could also be useful for parents with school-going or teenaged children who face difficulties in fulfilling their parental roles for which the literature is scant. Further active ingredients of such parenting interventions can be borrowed from (a) existing intervention programs tailored for parents with infants or toddlers in mother–baby psychiatric units (Wan et al., 2008); (b) newer cognitive remediation therapies to improve the overall functioning of patients with schizophrenia (Hogarty et al., 2004); and (c) novel parent management training interventions for parents of children with problem behaviors, which utilize emotion coaching paradigms (Havighurst et al., 2013).
It is important to understand these results in the light of a neurobiological framework. Estrogen priming is a highly conserved mammalian neurophysiological process (Brunton and Russell, 2010) of enhancing adaptive maternal behaviors and enhancing the likelihood of perceiving a reward in stimuli from offspring (Choleris et al., 2006). This process is mediated by polymorphisms on the estrogen receptor-α gene that play a role in the proliferation of oxytocin receptors in the parent brain (Pfaff et al., 2011). Neural activation during SC in mothers has been shown to mediate the association between genetic variation in the estrogen receptor gene and adverse parenting (Lahey et al., 2012). Interestingly, variants in the estrogen receptor-α gene contribute to the risk of developing schizophrenia (Weickert et al., 2008). This provides a neuro-endocrine framework for exploring the relationship between schizophrenia, SC and parenting (especially in mothers with schizophrenia) in future studies.
Though there was a relationship between ToM and parenting, it was surprising to note that no association was found with other SC domains including emotion processing, social perception and attributional styles. A possible reason for this lack of association may be the lack of parent–child contexts in tasks used to assess SC. For example, emotion recognition stills and videos in TRENDS and SoCueReTI (Social Cue Recognition Test–Indian Setting) have emotions of adults and not children. There is little data on the relationship between mentalizing abilities and parental roles in normative samples. Future studies need to assess this question in detail to guide our understanding about the specificity of this relationship between ToM and parental roles in schizophrenia.
It should be noted that these findings are results of a larger study to assess the determinants of functional outcome in remitted schizophrenia patients. The tool used by us as the outcome variable is primarily a tool to assess socio-occupational dysfunction and disability in the psychiatrically ill in general and schizophrenia in particular (Wiersma et al., 1988). Parental role is a sub-measure of this larger scale. The gamut of parental role assessed (affective relationship and actual involvement), though considerable, may have been insufficient to tap the broad and complex dimensions of parenting. Importantly, it may be noted that there is no gold standard tool to assess parenting. The methods used in earlier studies have been quite varied, ranging from questionnaires (Campbell et al., 2012) through observer-rated measures (Abel et al., 2005) to analysis of video recordings of mother–baby interactions in perinatal psychiatric wards (Wan et al., 2007). Not having assessed premorbid functioning and intellectual quotient, which may have an impact on parenting abilities, is another limitation.
Earlier studies have focused on parenting in post-partum mothers with infants or very young children, focusing especially on mother–infant interactions (Abel et al., 2005; Chandra et al., 2006; Riordan et al., 1999). Our study included offspring with a broad age range when compared to previous studies that have assessed parenting capacity in schizophrenia patients. We found little difference between parents with children above and below 16 years of age in terms of the association between parenting and cognitive abilities. The challenges involved in and the skills required for parenting children of different age groups within these two broad categories may vary. However, as the number of parents with children in narrower subgroups was small, we could not analyze the data for such subgroups. Future studies involving larger numbers of patients in each subgroup of offspring would throw useful light on the differential effects of the cognitive determinants of parenting in schizophrenia patients. Indeed, a similar study in the symptomatic phase of schizophrenia would yield insights into the relative contribution of symptoms and cognitive impairments in predicting parenting.
The tools used to assess social and neurocognitive functions are comprehensive and have been validated in the Indian cultural setting. Important clinical parameters such as insight and motivation, which are known predictors of functional outcome, were also used to explore the association with parental role. Moreover, these results to our knowledge are the first to show a relationship between ToM deficits and parental role dysfunction in schizophrenia patients.
In conclusion, a cognitive deconstruction of parental role in schizophrenia subjects has the potential to guide the development of more effective parenting interventions for schizophrenia patients who are parents. These findings gain relevance when assessed during symptom remission, as that is the stage which heralds active recovery-oriented treatment interventions. Our findings of second-order ToM deficits being significantly associated with parental role dysfunction take us one step closer to designing better parenting interventions, and understanding parental role deficits in schizophrenia.
Footnotes
Acknowledgements
We thank Professor Prabha S Chandra for proof-reading the manuscript and providing valuable input and Dr Rakshathi S Basavaraju for her help with part of the data collection.
Funding
We thank the Indian Council of Medical Research (MD financial assistance award 2007–2009, to UM Mehta) for the financial support. Funding and/or grant number: No. 3/2/2008/PG-Thesis-MPD-29.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.