
Abstract
Objective:
To describe PTSD symptom persistence and resolution, including the potential phenomenon of late-onset PTSD, in children and adolescents 18 months after a cyclone disaster; and to investigate factors that predict longer-term symptom outcome.
Method:
71 children and 191 adolescents who were screened three months after a Category 5 Cyclone were re-screened 18 months post-disaster. Child-report measures included the PTSD Reaction Index, measures of event exposure and social connectedness.
Results:
Approximately 1-in-5 children and 1-in-12 adolescents endorsed cyclone-related PTSD symptoms at the moderate to severe level 18 months post-disaster. Of these approximately one-half (44.8%) of children were in the ‘high-persister’ group at 18-month follow-up. Persistence of low symptoms was very common (97.6%) and late-onset PTSD was a rare phenomenon. This pattern was similar in adolescents: 25.0% were in the ‘high-persister’ group and few students experienced late-onset PTSD. In multivariate analysis, only initial severe to very severe PTSD category made a significant independent contribution to explaining persisting moderate to severe PTSD symptoms in primary school students (ORadj=8.33, 95% CI=1.45-47.84). There was a trend for a similar result in secondary students.
Conclusion:
A child or adolescent with few PTSD symptoms three months post-disaster is likely to remain so unless a further traumatic event occurs. However, if symptomatic at three months, there is approximately a 30-45% chance that the child or adolescent will still be symptomatic 18 months after the disaster. Given the high rate of students in the ‘resolver’ group, initial posttraumatic symptoms are a necessary but not sufficient condition for predicting chronic symptomatology. Other targets for predictive modelling include initial threat perception and high and low social connectedness.
Introduction
Natural disasters, such as earthquakes, floods, cyclones or tsunami, have substantial impact on the mental health of children and adolescents. Children who have lived through a natural disaster may develop distressing symptoms, such as sleep or behavioural disturbance or severe emotional disturbance (McLaughlin et al., 2009), or specific disorders, such as depression (McDermott and Palmer, 2002) or anxiety (Hoven et al., 2005). Research following man-made disasters has reported increased substance use in adolescents in the post-disaster period (Reijneveld et al., 2005). Given that most post-disaster research is cross-sectional in design, it is difficult to comment on causation. Possible explanations for drug and alcohol excess include a coping mechanism for general distress or self-medication of specific symptoms, such as sleep disturbance. Post-disaster diminished quality of life (Alisic et al., 2008) and functional impairment have also been demonstrated, including increased school absence correlated with elevated trauma symptoms (Broberg et al., 2005).
Many post-disaster emotional, cognitive and behavioural effects manifest on a spectrum of stress responses, from individuals who report some post-disaster posttraumatic stress disorder (PTSD) symptoms (McDermott and Palmer, 2002), limited-symptom PTSD, to PTSD. Post-disaster child PTSD prevalence rates vary widely. La Greca and Prinstein (2002) suggest rates of 5–10% for meeting full diagnostic criteria across published studies. Rates vary based on methodological differences between studies, parent-, child- or combined symptom report and, importantly, the severity of the disaster. Our previous article regarding children in North Queensland, Australia, who experienced a category 5 cyclone, showed that, 3 months after exposure, 11.3% of children reported PTSD symptoms in the severe to very severe PTSD category (McDermott et al., 2012). There is some literature on the longer-term outcomes of children who experienced significant initial post-disaster symptoms or met the criteria for a diagnosis of PTSD. Current research findings are equivocal. Some reports have indicated that trauma-related psychological symptoms decline significantly over time (Song et al., 2012); others have shown that traumatised children or adolescents continue to experience a moderate degree of posttraumatic stress symptoms for an extended period. Shaw and colleagues (1996) reported a decrease in posttraumatic stress symptoms (PTSS) in 30 6–11-year-old children 21 months after Hurricane Andrew. However, 70% of children still endorsed moderate to severe PTSS (Shaw et al., 1996). Ularntinon and colleagues (2008) noted, of 45 children similar in age to the Shaw sample, who experienced the 2006 tsunami and met the Diagnostic and Statistical Manual of Mental Disorders, fourth edition criteria for a mental illness, that as many as one-third still met these criteria at 36 months post-tsunami. Thus, while symptoms decline in most children, symptom chronicity is common.
Longer-term follow-up studies also report symptom persistence in children and adolescents. Five years after a fireworks explosion, elevated odds ratios (ORs) for conduct and hyperactivity symptoms were demonstrated in schoolchildren whose parents indicated that the child was a victim of the disaster compared to a non-exposed group (Boer et al., 2009). Lifetime PTSD measured using a diagnostic interview was more prevalent among survivors of a shipping disaster compared to controls (Udwin et al., 2000) and more lifetime anxiety disorders 20 years after a devastating bushfire disaster (McFarlane and Van Hooff, 2009). Less is known about the potential for late-onset PTSD in children and adolescents exposed to an earlier traumatic event.
Cross-sectional research has informed many aspects of a vulnerability-resilience model. These include proximal (event-related) factors, such as event exposure and peritraumatic perception of threat to self or loved ones, and distal factors, such as pre-existing child and family characteristics, including the child’s age, sex, and prior life events and coping style. Indeed, a previous publication that focused on the responses of children 3 months after experiencing a cyclone disaster (the first data wave of the sample reported in this paper) reported a strong independent contribution from low social connectedness [adjusted OR (ORadj) 3.96, 95% confidence interval (CI) 1.95–8.03] and elevated threat perception (ORadj 3.88, 95% CI 2.04–7.38) (McDermott et al., 2012). A further advance would be the ability to identify children whose initial symptoms at the time of a disaster will either persist or remit in the longer term. This could potentially influence the assignment of scarce treatment resources. But this is not possible with cross-sectional data. Hence, in this report, we aim to describe the natural history of PTSD symptoms in children and adolescents 18 months after a cyclone disaster and to investigate factors that predict longer-term symptom outcome. As well as reporting symptom persistence and resolution, we describe whether the phenomenon of late-onset PTSD was seen in this sample.
Method
Procedure
Time 1 (T1) data collection comprised a single-phase, school-based, universal screen of all children attending Catholic Education schools in the Queensland Government- designated disaster area 3 months after the cyclone. With school principal and parent consent, students from grades 4–12 completed self-report questionnaires about their cyclone exposure, evacuation experience and other cyclone-related events. Students then completed measures of PTSD and social connectedness. Staff who supervised these tasks were from either the screening team or were local school guidance officers. For further details regarding this procedure see McDermott and colleagues (2010). The time 2 (T2) procedure was coordinated by Catholic Education following human research ethics committee approval and parent consent. Screening questions were read to students at T1 to standardise for reading ability while they were young. At T2, 18 months after the cyclone, students were old enough to complete the questionnaires themselves in their classrooms using an otherwise identical procedure to that deployed at T1.
Participants
The sample frame for the T2 study was all students from grades 5–10 in the cyclone-affected area who participated in the T1 screen. The T2 participation rate was 53.9% of participants who completed T1. Informal parent and teacher feedback suggested many families had left the disaster area to seek employment. Further, very few participants (< 5%) received a disaster-related mental health intervention. Other families were not encouraging of their children talking about the cyclone any further. Of 371 participants, secondary school children were over-represented [63.7% (191/300) versus 30.0% (71/237) primary school children]. Participating high-school students were significantly more likely to be female (57.1%; χ2 = 4.78, p = 0.029) and younger [12.8 years (SD 0.98) versus 13.6 years (SD 1.03), t = 10.352, p = 0.000] than non-participants. Among primary school children, 50.7% were female with an average age of 9.8 years (SD=1.1, range 8–12 years). As noted in our T1 article (McDermott et al., 2010), because of sensitivity about research in the post-disaster setting, we did not collect socioeconomic data. However, compared to Queensland as a whole, Indigenous Australians (7.7% of the relevant Heath Service District population, versus 2.3% in Queensland), individuals who spoke a language other than English at home (8.7% versus 7.7%) and people living with relative socioeconomic disadvantage (36% versus 20%) were over-represented in the sample community (Queensland Government et al., 2004). There was no difference between participants and non-participants on measures of cyclone exposure, such as home damage. Controlling for age, there was no participant compared with non-participant difference on T1 PTSD category (ORadj 1.54, 95% CI 0.73–3.23).
Measures
Posttraumatic stress disorder
PTSD was measured using the PTSD Reaction Index (PTSD-RI; Pynoos et al., 1993), an extensively used, 20-item report measure of PTSD in children and adolescents. The items were adapted to ask about the specific traumatic event, in this case, Cyclone Larry. Responses were recorded on a five-point Likert-type scale and added to generate a total PTSD-RI score (range 0–80) from which a standard case classification was derived (doubtful = 0–11, mild = 12–24, moderate = 25–39, severe = 40–59 and very severe = 60–80). The psychometric properties of the PTSD-RI are well documented, considered suitable for research purposes and demonstrate satisfactory concurrent validity (Pynoos et al., 1993), discriminant validity (La Greca et al., 1996) and internal consistency (Vernberg et al., 1996). In this sample, Cronbach’s alpha was 0.90 (primary school) and 0.92 (secondary school), indicating acceptable scale internal cohesion.
Child connectedness
Child connectedness was measured using four items, two about participation (friends and clubs) and two about cohesion (trust and belonging). Contact with friends and participation in school activities were measured using the following items: ‘I have friends to play with or hang out with during school breaks’ and ‘I go to a school sport team training, or a rehearsal, meeting or club’. Trust in others was measured by: ‘I think most people take advantage of others (like doing things for themselves not others)’. A belonging item was measured by: ‘When I feel lonely, there are several people I could call to talk to’. Children responded to measures on a five-point scale. For further details of this scale, including where items were adapted from, see McDermott et al. (2012).
Proximal factors: Trauma exposure and threat perception
Disaster-related exposure was measured by child self-report about typical cyclone experiences, such as witnessing flying debris, seeing broken windows, damage to part of or their entire roof, experiencing an evacuation or relocation to another place of residence. To assess a perceived threat, children were asked ‘Did you think you were going to die during the cyclone?’ and were asked to considerthat a family member may die. Children also gave their post-disaster global experience of school by endorsing better or worse to the question: ‘Is going to school better or worse since the cyclone?’
Distal factors
In the post-disaster environment, families were understandably focused on restoration of safety, shelter, food and health. Accordingly, our research activities were mindful of the burden on families and children, with the result that our explanatory model did not include measures of pre-disaster coping or personality. However, we included the parent version of the Strengths and Difficulties Questionnaire, emotional subscale (Goodman, 2001), to measure children’s depression or anxiety symptoms in the 6-month period prior to the cyclone.
Statistical analysis
The PTSD outcomes were the PTSD-RI total score (continuous variable) and two dichotomous variables at T1 and T2: PTSD-RI categories moderate to very severe PTSD = 1 and other classifications = 0. We computed a continuous connectedness score and two dichotomous categories: children in the lowest decile of the connectedness distribution were categorised as low child connectedness (low = 1, other = 0) and those in the highest decile as high child connectedness (high = 1, other = 0). We used chi-square tests to compare dispersion between pairs of categorical variables, two-tailed t-tests to compare between-group means for continuous variables, and Pearson product-moment correlation coefficients to test associations between pairs of continuous variables. We took account of potential confounders (e.g. school size) and examined the possible main effects of age and sex. Odds ratios (crude and adjusted) were calculated by logistic regression. Given some loss of power with a categorical-logistic regression approach, multivariate analyses were also performed using the total PTSD score as a continuous variable. There were few missing data and these were imputed using estimation maximisation procedures. Means, SDs and correlation coefficients in the imputed data set were near-identical to those in the data set with missing data and analysis used robust standard errors to adjust for possible inflation of estimates due to the school-based clustering of data. All analyses were conducted in Stata version 11 (StataCorp LP, College Station, Texas, USA) using the imputed data set.
Results
Primary school children
Approximately 20% of primary school children (14/71) reported symptoms that met the criteria for moderate to severe PTSD 18 months after the cyclone. The average PTSD total symptom score of this group was 41.00 (SD = 4.12) compared to the remainder of the primary school sample [M = 19.79 (SD = 1.75), df(69), t = -5.213, p = 0.000]. The two groups (moderate to severe symptom group versus remainder) did not differ by sex or age. Of the primary school children who had severe to very severe symptoms at T1, nearly half (44.8%) were in the high-persister group at T2, i.e. they still had moderate to severe symptoms at the 18-month follow-up (Figure 1). The resolved group (55.2%) were children who were highly symptomatic at T1 but demonstrated low-level symptoms at follow-up. Almost all (97.6%) of the children who showed few or no symptoms at T1 remained in this category at T2. Late-onset PTSD was a rare phenomenon in this sample, only occurring in one case (Figure 1).
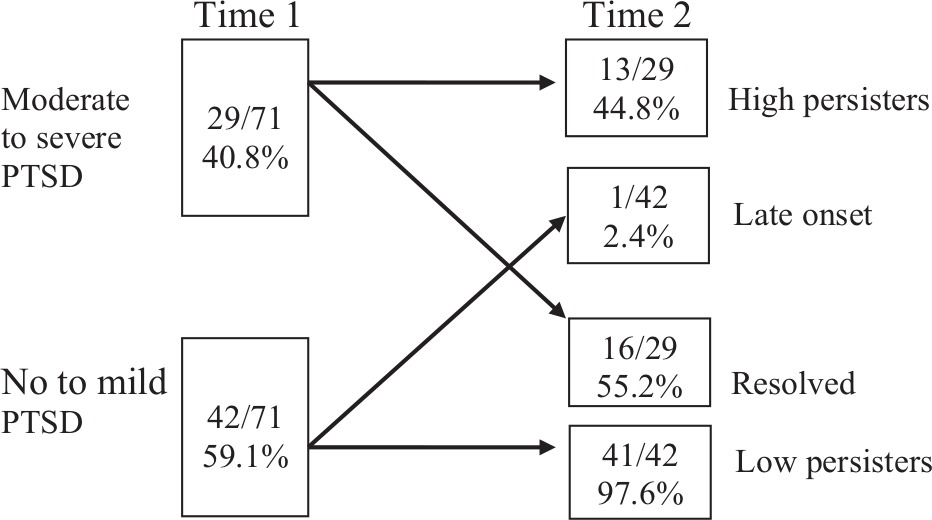
Persistence of moderate to severe PTSD in primary school children.
At bivariate analysis, T1 severe to very severe PTSD, experience of evacuation, perceived threat to self, perceived threat to parents and low social connectedness were significantly associated with T2 moderate to severe PTSD (Table 1). None of the following T1 factors were significantly related to T2 PTSD: possessions needing to be replaced after the cyclone, home repairs finished at 3 months post-cyclone, opinion that school was worse since the event, home damage preventing return home and high social connectedness.
Bivariate associations of PTSD symptom category (moderate to severe versus no symptoms to mild) at 18-month post-disaster follow-up with time 1 (T1) variables.
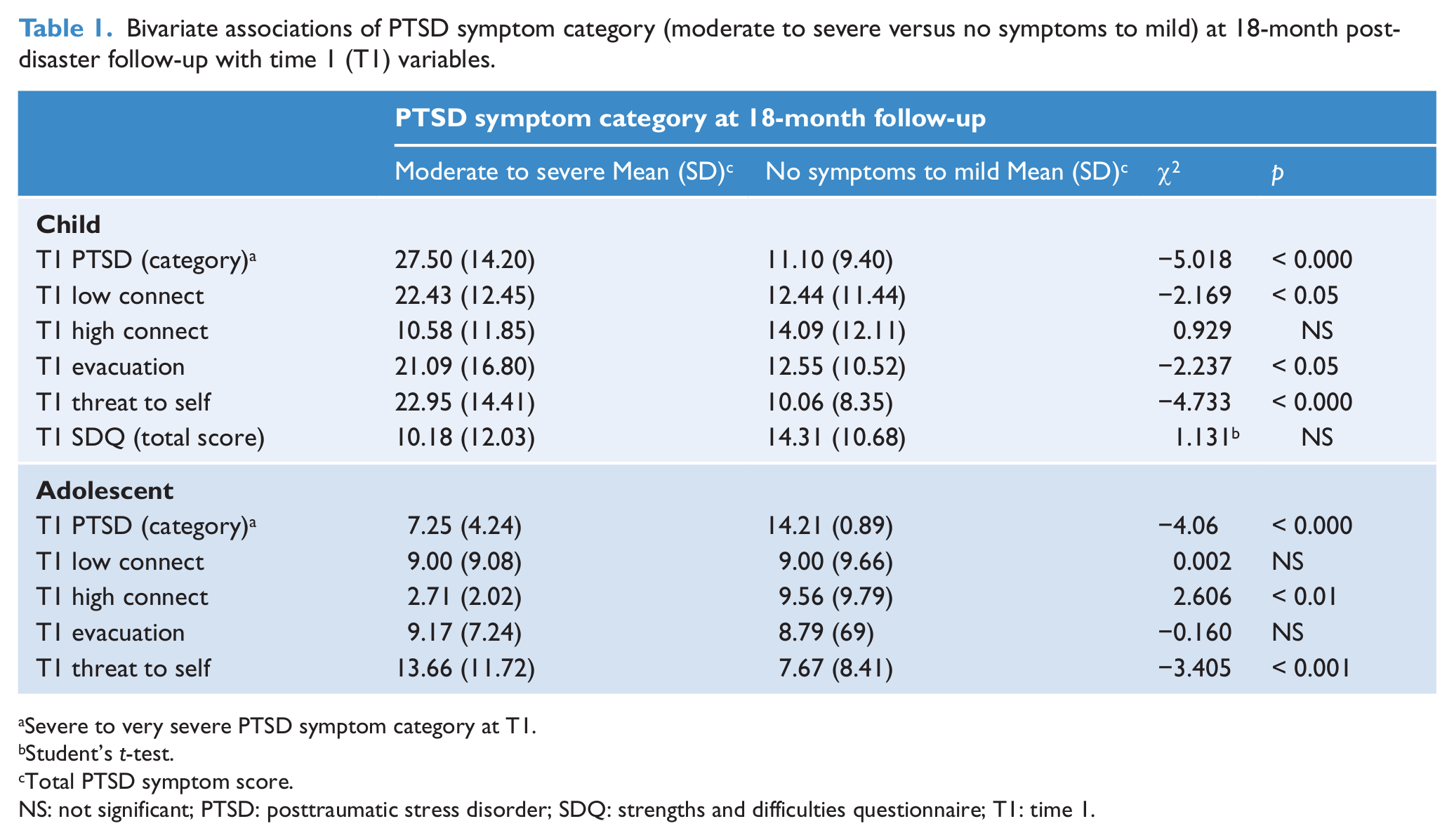
Severe to very severe PTSD symptom category at T1.
Student’s t-test.
Total PTSD symptom score.
NS: not significant; PTSD: posttraumatic stress disorder; SDQ: strengths and difficulties questionnaire; T1: time 1.
Secondary school children
Nearly one-tenth of secondary school children (16/191, 8.4%) reported symptoms that met the criteria for moderate to severe PTSD 18 months after the cyclone. The average PTSD total symptom score of this group was 33.44 (SD = 8.44) compared to the remainder of the secondary school sample [M = 6.50, SD = 5.19, df(189), t = -18.67, p = <0.001). The two groups (moderate to severe symptom group versus remainder) did not differ by sex but were slightly younger. Of the secondary school children who had moderate to very severe symptoms at T1, 25.0% (9/36) were in the high-persister group with moderate to severe symptoms at the 18 month follow-up and three-quarters of this group (27/36, 75.0%) were in the resolved group (Figure 2).
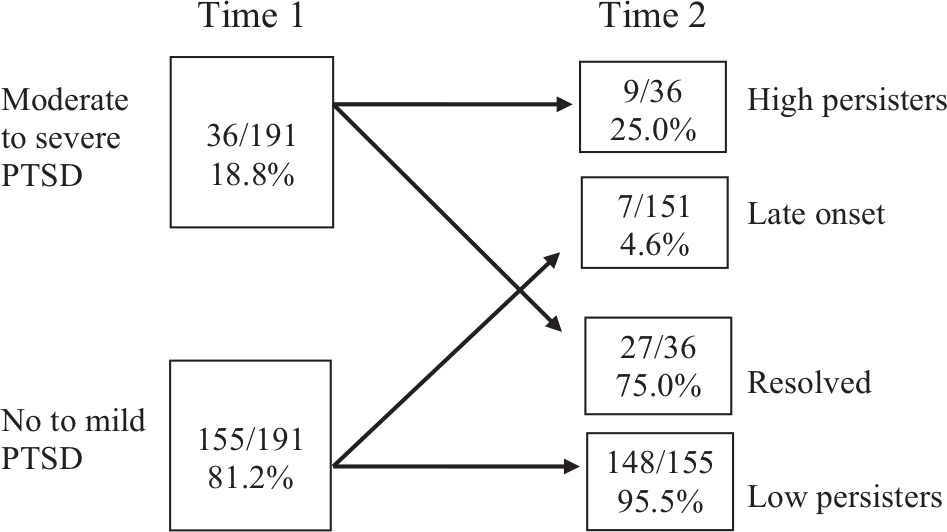
Persistence of moderate to severe PTSD in secondary school children.
Nearly all secondary school children who originally had few or no symptoms were in the low-persister group at follow-up (148/155, 95.5%). Late-onset PTSD was also a rare phenomenon among secondary school children, only occurring in 4.6% (7/155) of cases. Significant bivariate relationships with T2 moderate to severe trauma symptoms in secondary school children were found with T1 severe to very severe PTSD and T1 perceived threat to self. Being a high-connected student at T1 was also significantly associated with a lower PTSD total score at T2 [2.71 (2.02) versus 9.56 (9.79), df(171), t = 2.6026, p = 0.01]. The following T1 factors (the same as reported for the primary school children) were not significantly associated with T2 PTSD: possessions being replaced, home repairs finished, opinion that school was worse since the event and home damage preventing return home.
Prediction of persisting moderate to severe posttraumatic stress disorder
In primary school children, in multivariate analysis, only an initial severe to very severe PTSD category made a significant independent contribution to explaining persisting moderate to severe PTSD symptoms at follow-up (ORadj = 6.45, 95% CI = 4.16–8.73). If an individual had PTSD at T1, they were approximately 6.5 times more likely to experience T2 moderate to severe PTSD. Similarly for secondary school children, in multivariate analysis if an individual had high PTSD at T1, they would be approximately 3–4 times more likely to experience T2 moderate to severe PTSD. Further, for secondary school children there was a trend linking T1 threat to self perception to greater likelihood of persisting trauma (Table 2). High-connectedness status could not be included in the multivariate model because there were no high-connected children in the T2 moderate to severe PTSD group. The significance or non-significance of these associations was replicated when PTSD was analysed as a continuous variable.
Logistic regression model predicting moderate to severe PTSD category in children and adolescents 18 months after a cyclone disaster.
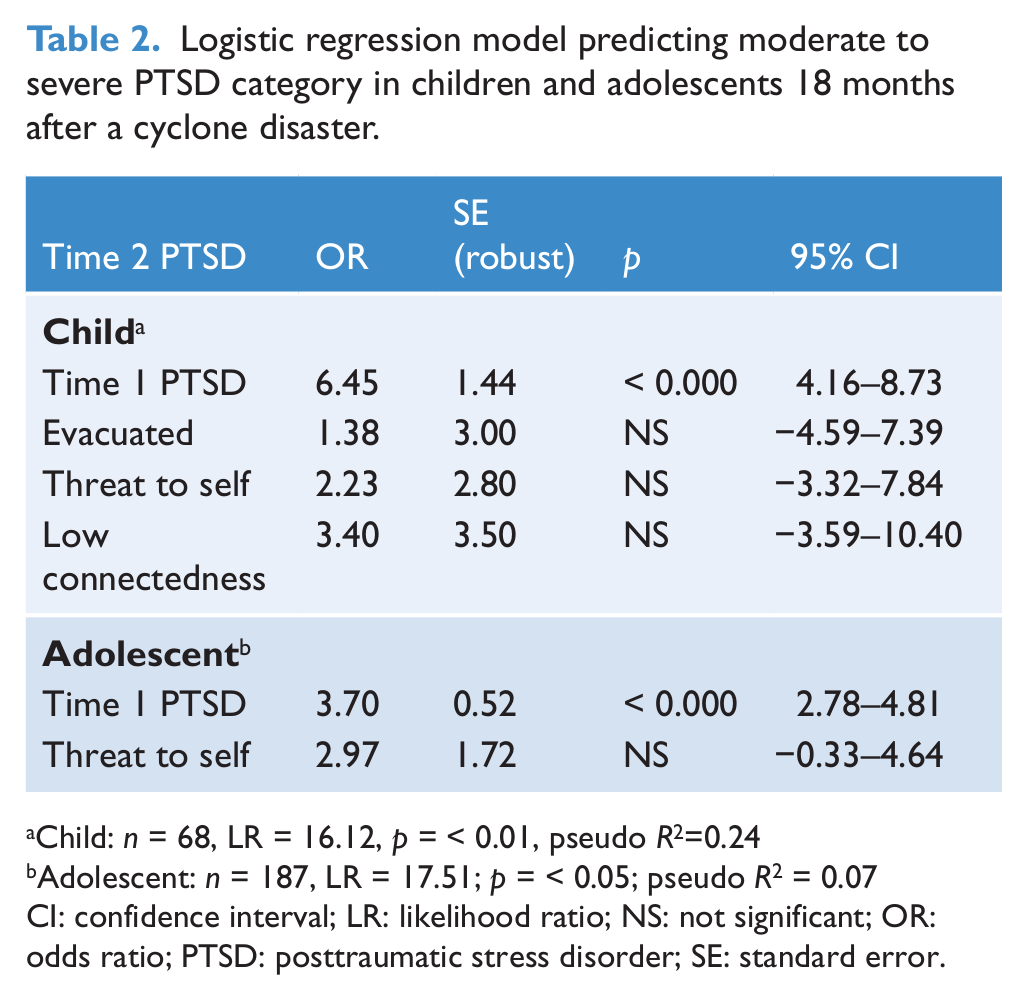
Child: n = 68, LR = 16.12, p = < 0.01, pseudo R2=0.24
Adolescent: n = 187, LR = 17.51; p = < 0.05; pseudo R2 = 0.07
CI: confidence interval; LR: likelihood ratio; NS: not significant; OR: odds ratio; PTSD: posttraumatic stress disorder; SE: standard error.
Discussion
Approximately one in five primary school children and one in 12 secondary school children reported cyclone-related PTSD symptoms at the moderate to severe level 18 months following a cyclone disaster. Our findings that more than half of primary school children with severe to very severe PTSD symptoms 3 months after the cyclone disaster were categorised as resolved 18 months later is very similar to the findings by Shaw and colleagues (1996), who investigated a similar age group after Hurricane Andrew. Our findings are also consistent with those for children who experienced the 2004 tsunami disaster, among whom approximately half of those meeting the PTSD criteria at 1 year had remitted or were categorised as subsyndromal PTSD at the 3-year follow-up (Ularntinon et al., 2008). Our child and adolescent symptom persister groups were larger than the 10% reported 2 years after an accidental injury (Le Brocque et al., 2010), which might be explained by the use of a different PTSD measure and by a different type of traumatic event.
In both age groups in our sample, individuals with elevated symptoms at the 18-month follow-up were those with severe to very severe symptoms at the initial assessment, 3 months after the cyclone. High rates of low symptom persistence were seen in both primary and secondary school children. Consistent with the follow-up categories reported by Le Brocque (2010), late-onset PTSD was almost non-existent in primary school children and rare in secondary school children. When adjusting for age and sex, in both primary and secondary school children, severe to very severe PTSD and high initial threat perception (the latter a trend in adolescents) soon after the cyclone predicted PTSD 18 months later. The relationship of social connectedness with persistence of PTSD is complex in that our results suggest low connectedness is a vulnerability factor for primary but not for secondary school children while high connectedness is a protective factor for secondary but not for primary school children.
While clearly needing replication in larger samples and for different disasters, this phenomenon is consistent with recent differential susceptibility theories in which children’s intrinsic characteristics or stage of development interact with the nature of the challenges they face to produce different responses in each child. For example, different types of childcare environments may be of relative advantage or disadvantage to children with differences in temperamental negativity (Pluess and Belsky, 2009). Similarly, particular genes may confer a susceptibility or, in some circumstances, an advantage (Van IJzendoorn and Bakermans-Kranenburg, 2012). In our disaster context, relatively more children may feel connected in primary school, such that higher connectedness has little capacity to discriminate children’s responses to trauma. Similarly, it may be more typical for secondary school children to feel less connected to school, again making lower levels of connection less predictive of their later outcomes.
These findings carry important clinical and policy implications. Three months after a natural disaster, a child or adolescent with few PTSD symptoms is likely to remain so unless a further traumatic event occurs. However, if symptomatic at 3 months, there is approximately a 30–45% chance of the child or adolescent still being symptomatic 18 months after the disaster. Given the high rate of resolvers in our study and in those by others (Kassam-Adams, 2010; Le Brocque, 2010), elevated initial posttraumatic symptoms are a necessary but not sufficient condition for predicting chronic symptomatology. Particular concern is warranted when young traumatised children have poor connectedness at the time of a disaster; and perhaps a higher likelihood of resolution can be anticipated when older traumatised children start out with high connectedness. Either way, improving child connectedness in places where disasters are common could prove an effective prophylactic intervention.
It is also important to recognise that elevated PTSD symptoms at the time of a disaster predict post-event, non-PTSD psychopathology. That is, if not treated effectively at the time, trauma will generalise. For example, at a 3-year follow-up, children with severe PTSD immediately after witnessing a parent’s death during a school accident were four times as likely as other children to exhibit elevated generalised anxiety (Song et al., 2012); Our recommendation is that severe to very severe symptoms at 3-months post-event should trigger a formal, face-to-face mental health assessment aimed at identifying and treating psychopathology and preventing symptom chronicity. Ideally in such cases, functional impairment should be assessed along with psychopathology (Kassam-Adams et al., 2010).
We note three key limitations in this study. First, small sample size, especially in the primary school sample, limited our ability to obtain robust estimates, which is reflected in wide confidence intervals and reduced power to find significant effects. Nevertheless, the large adjusted ORs for PTSD soon after the cyclone predicting symptoms 18 months later suggest that the initial traumatic response is an important consideration when assessing the risk of longer-term PTSD and other psychiatric disorders in school children who experience a single-event emotional trauma. Second, the difficulties of collecting data immediately after a disaster and lack of resources in these settings meant that we could not conduct semistructured research diagnostic interviews or assess a wider range of psychopathology (e.g. assessing depression, other anxiety disorders and disruptive behaviour disorders would have been useful). Instead, we had to rely on questionnaires and assessing PTSD severity categories based on the recommendations of the authors of the scale. Finally, it is difficult or impossible to find children whose families have relocated from the disaster area and, therefore, to include them in the follow-up. If there are traumatised family members, including school children, in relocated families, our results may underestimate the true burden of PTSD in children 2 years after a cyclone disaster.
Future studies should revisit the longer-term outcomes of school children who were symptomatic at the time of a disaster. Among Australian adults who experienced a physical injury, PTSD symptoms increased over the first 12 months post-disaster (O’Donnell et al., 2007).We did not replicate this finding. Perhaps it would be observed in an older adolescent group. Yet, we know that children respond to trauma differently from adults and, with their substantially greater vulnerability, they merit study in their own right. Greater post-disaster resources would allow the collection of a larger sample, and thus greater power to investigate more complex models. The latter could include biological variables, such as genetic information. Broadening outcomes to better detail functional impairment or posttraumatic growth would be informative and potentially influence interventions.
Footnotes
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.