
Abstract
Objectives:
The Arabic-speaking clergy is highly revered and considered the first point of contact for people who suffer from mental illness within their community. The current study aimed to explore the beliefs of Arabic-speaking religious leaders regarding the causes of mental illness and the use of medication for their treatment.
Method:
Participants consisted of 170 Arabic-speaking clerics of Muslim (n = 85) and Christian (n = 85) denominations residing in Sydney, Australia. A questionnaire was administered during face-to-face interviews and included items regarding the causes of mental illness and beliefs about whether psychiatric medications were viewed as helpful or harmful.
Results:
Most of the Arabic-speaking clerics viewed drug and alcohol addiction and psychosocial factors as the most important causes of mental illness. Biological causes such as a chemical imbalance in the brain were less frequently endorsed. Although medications were viewed by most religious clerics as helpful in the treatment of mental illness, there were also concerns about the potential harms of medications, particularly among Muslim clerics. Muslim clerics also endorsed the religious causes for mental illness, such as spiritual poverty, as being more important more so than did Christian clerics.
Conclusions:
The beliefs of Arabic-speaking religious leaders influence how they respond to people with mental illness and may determine whether they refer people to professional mental health services or not. Understanding their perspectives allows opportunities to share information to facilitate collaborative work in the care of Arabic-speaking people with mental illness. Arabic-speaking religious leaders need to be better educated about the mechanisms of action and benefits of medication in the treatment of mental illness.
Introduction
The use of mental health services among Arabic-speaking people is low (Al-Krenawi and Graham 1999; Correa-Velez et al., 2007; Youssef and Deane 2006). Comparisons of people born in refugee-source countries that included many Arabic-speaking countries found that the rates of hospital use for mental or behavioural disorders was lower than compared to Australian-born people (Correa-Velez et al., 2007). Although the reasons for the low rates of mental health service use are not entirely clear, one contributor is likely to be the relatively high use of alternative sources of help, such as religious leaders of Muslim and Christian background (Al-Krenawi and Graham 1999; Lipson and Meleis 1989; Youssef and Deane 2006). Arabic-speaking religious leaders are frequently required to guide and counsel individuals with mental health problems and to assist their families to address these difficulties. However, very little is known about the perceptions of religious leaders about mental illness and its treatment. The present study aimed to explore the perceptions of Arabic-speaking Muslim and Christian religious leaders regarding mental illness and its treatment.
Muslim and Christian perspectives on mental illness
There are many similarities between the historical perspectives of Muslim and Christian religions regarding mental illness and its causes. These perceptions are rooted in the ancient pagan beliefs of possession by demons and jinn which were integrated into the dogma and teachings of Christianity (the Bible) and Islam (the Koran) (Al-Issa, 2000). Arabic-speaking Christian and Muslim clerics use several traditional methods for healing people with mental illness. The Muslim Imam treats diseases and mental illness by referring to medical advice found in the Koran and Hadith, as expounded by the prophet Mohammed (Al-Krenawi and Graham, 1999). Prophetic medicine (Al-Tibb an-nabawi) is a traditional form of medicinal skills and techniques (e.g. the use of spiritual oils) which is the precursor of the contemporary phenomenon of Koranic healing used by Arabic-speaking Muslim sheiks or mullahs throughout the world (Al-Nasimi, 1984). Family and friends may gather for a communal meal where citations from the Koran are read, religious songs are sung and prayers are offered (Al-Krenawi and Graham, 1999). Muslim clerics view their role in working among people with mental illness as one of providing comfort and assistance and enriching their spiritual faith in God/Allah by providing Koranic verses that exorcise demons or jinn (Ali et al., 2005; Al-Krenawi and Graham 1999).
Arabic-speaking Christian clerics also perform prayers, blessings or exorcisms to drive out evil spirits which may be thought to possess people with mental illness (Takriti and Ahmad, 2000). People with mental illness are viewed compassionately and sympathetically by Arabic-speaking Christian clerics who try to provide support and instil hope through faith (El-Bakhoumi, 2003; Jacobsson and Merdasa, 1991; Malaty, 1979). If prayer and blessings are insufficient, clergy may suggest that the mentally ill person spend time in a monastery for prayer, reflection and purification of body, mind and soul to promote healing (Takriti and Ahmad 2000; Wang et al., 2003).
Should these strategies fail to provide a cure, then both groups of Arabic-speaking clerics may encourage the person to seek a professional mental health clinician for treatment and support. Both religions have a diverse theological ideology that may be related to working with mental illness in their communities (Al-Nasimi, 1984; El-Bakhoumi, 2003). There are likely to be differences in religious doctrine, practices and training and hence, it is likely that there will be individual differences in the perspectives of clerics concerning the causes and treatment of mental illness (Malaty, 1979).
Attitudes of the Arabic-speaking community towards medications
There are a range of concerns about medications in Arabic-speaking communities. The contents of some medications can make them highly controversial or prohibited for Muslims. For example, gelatine is a common ingredient in psychotropic drugs and is commonly made from the skin and bones of pigs and cows (Sattar and Pinals, 2002). Fortunately, numerous substitute preparations to gelatine capsules are now available (e.g. liquid form elixir preparations). Another frequently overlooked phenomenon is the practice of ceasing medication during the Muslim holy month of Ramadan due to its requirement for fasting (Sattar and Pinals, 2002). The stigma associated with drug treatment and the belief that drugs may be habit-forming and lead to long-term dependency is another serious concern (Takriti and Ahmad, 2000). The use of psychotropic drugs is perceived to cause diminished awareness, especially at work and in social gatherings (Al-Issa, 2000; Takriti and Ahmad 2000). In general, such concerns are likely to contribute to negative attitudes towards medications in Arabic-speaking Muslim communities. Religious leaders have the potential to be very influential and could help address concerns about psychiatric medications in their communities. To our knowledge, there is no Australian research describing the role of Arabic-speaking religious leaders in mental health care, or their potential roles in collaboration with mental health professionals. The willingness of religious leaders to work in collaboration with mental health professionals may be dependent on their views about the causes of mental illness and their attitudes towards treatment approaches. Research on the Arabic-speaking clergy is limited, but the beliefs of the non-Arabic-speaking clergy regarding mental illness have been investigated in Western societies (Kloos et al., 1995).
The role of religious leaders in mental health care
The efforts of religious leaders in assisting people with mental illness have been widely reported, although their potential contribution has often been underappreciated by mental health professionals (Wang et al., 2003). Individuals frequently seek advice from the clergy when challenged with mental health issues (Loewenthal et al., 2001; Weaver, 1995). The clergy have been described as being in ‘the frontline for the provision of human services’ in relation to mental health (Klimidis and Minas, 1995). For example, in a US study, 8098 community participants were asked about the professional treatment received from the clergy, general practitioners (GPs), psychiatrists, other mental health specialists, human service providers and alternative treatment providers (Wang et al., 2003). Twenty-five per cent of participants who sought help for mental health problems initially went to the clergy. The study indicated that 23.5% of participants preferred contact with a member of the clergy compared to 16.7% with a psychiatrist or 16.7% with a GP. The majority of participants (56%) saw only members of the clergy rather than other service providers in the year prior to the survey.
A survey of 1031 US Methodist pastors found that 20% interacted with people who had a mental illness in a professional capacity, either weekly or more often (Lafuze et al., 1999, 2002). The pastors believed that biological/neurobiological causes (e.g. a chemical imbalance in the brain, genes) were the primary sources of mental illness. Psychosocial causes, such as inconsistent parenting, social pressure and spiritual poverty were thought to contribute less to the cause of a mental illness. Fifty-three per cent of pastors agreed and 86% strongly agreed that medication is helpful in the treatment of mental illness. When asked whether medication is more helpful than prayer and counselling, 76% of pastors were either neutral or disagreed with the statement (Lafuze et al., 1999, 2002).
As noted previously, research regarding such beliefs and attitudes among Australian religious leaders is lacking. Given the preferences for accessing help from religious leaders in Arabic-speaking communities and the high regard they are afforded in these communities, religious leaders have the potential to be positive and powerful influences in the treatment of mental health problems.
Study aim
The aim of this study was to describe the beliefs of Arabic-speaking religious leaders regarding the causes of mental illness and their attitudes towards medications as a treatment. Given some of the concerns described in Muslim communities, we hypothesised that Muslim clerics would have more negative attitudes towards medications in the treatment of mental illness than Christian clerics.
Method
Design
Using a cross-sectional design, a standardised questionnaire was administered during face-to-face interviews with Arabic-speaking clerics of various denominations in the Sydney metropolitan area. Equal numbers of Muslim and Christian clerics were recruited to compare the two groups (n = 85 for each group).
Participants
All potential participants were male religious leaders of Arabic-speaking background, affiliated with either the Muslim or Christian religion. Participants were required to be actively working with and serving the Australian Arabic-speaking community in Sydney, Australia. Those who had previously participated in the initial pilot study (Youssef and Deane, 2006) were not eligible to participate in the present study. The reason for this was that they may have changed their opinions as a result of participation in the initial pilot study.
Snowball sampling was used to identify potential participants. It was considered preferable to other sampling methods, such as the use of posted questionnaires which have typically resulted in low response rates in other similar communities (Ali et al., 2005). A face-to-face approach in conjunction with Arabic-speaking interviewers has been found to be more acceptable to Arabic-speaking people due to the high value their culture places on context and the capacity to provide contextual details if needed (Lipson and Meleis, 1989)
There were limitations in the capacity to select participants in any random fashion. This was in part related to how religious places of worship are listed in telephone directories. Telephone listings of religious places of worship rarely include the name and contact number of a specific religious leader due to privacy. In addition, even when contact is made, there is reluctance to provide such details. Events related to the threat of terrorism and the focus on Arabic-speaking, and specifically Muslim communities, has increased the suspicion of some Arabic-speaking people concerning any activity that may be construed as having governmental involvement.
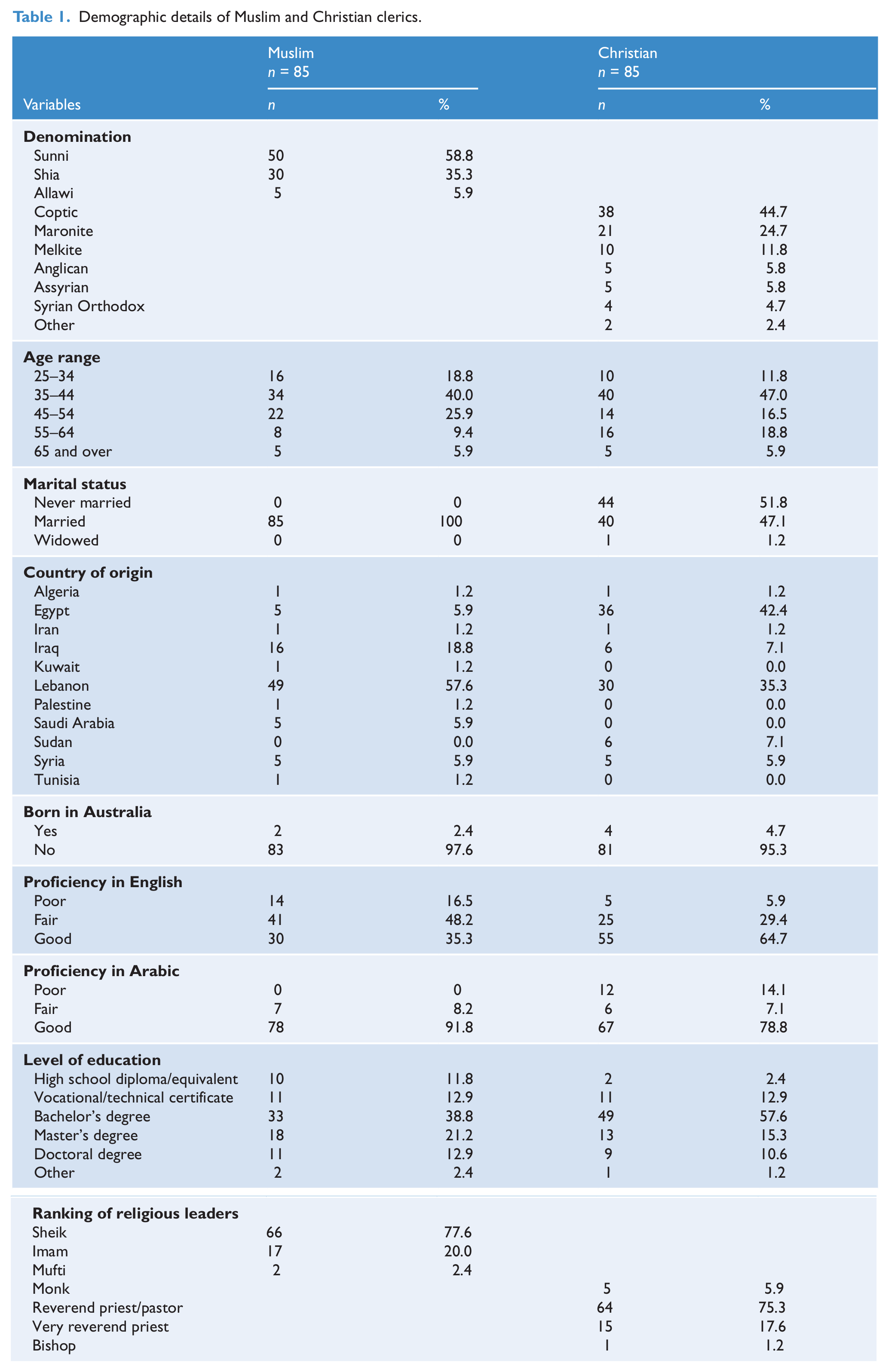
The approach taken involved the first author (JY) initially meeting with one of the Muslim religious leaders who participated in the pilot study, this was done so as to establish a connection for chain referrals for other Muslim religious leaders. Subsequently, recruitment of participants was initiated using snowball sampling or chain referral which identified those clerics with specific characteristics pertinent to the study (Biernacki and Waldorf, 1981; Khavarpour and Rissel, 1997; Lipson and Meleis, 1989). Snowball sampling identified 173 eligible referrals, and 170 clerics (98%) agreed to participate in the interview and survey. Only three clerics refused to participate and they were all Muslim. Reasons for refusal to participate were due to time constraints and lack of availability. The final group of 170 religious clerics comprised 85 Christians and 85 Muslims; details regarding the specific religious denominations along with other demographic data are provided in Table 1.
Demographic details of Muslim and Christian clerics.
Procedure
The research protocol was reviewed and approved by the University of Wollongong Human Ethics Committee. Information sheets, consent forms and questionnaires were available in both English and Arabic (translated and backtranslated by the National Accreditation Authority for Translators and Interpreters). All questionnaires were administered during a face-to-face interview with each participating religious leader.
Initially, participants were contacted by telephone, provided with a brief explanation of the project and offered the opportunity to participate in this research. Potential participants were informed that a more comprehensive explanation of the project and informed consent procedures would be explained further at the face-to-face interview. The majority of clerics agreed to be interviewed at a mutually convenient time in their home or workplace. Most participants preferred the researcher to read each item from the questionnaire and to record their responses on the form. At the completion of each interview, participating clerics were asked to nominate and provide the contact numbers of three other clerics, the reason for this was to access other clerics who had not been vetted previously, in order to gain a wider perception of their views.
Questionnaire
The questionnaire used in this study was adapted from the questionnaire used in the US study of Methodist pastors carried out by Lafuze et al. (1999, 2002). Eleven items from the original total of 57 were deemed inappropriate for this study. Most of the excluded items were considered to have the potential to breach cultural beliefs or boundaries (e.g. reference to immediate family members with mental illness). However, the remainder of 46 items were slightly modified to make them relevant to the context of the research and to facilitate translation into the Arabic language. The term United Methodist Church was replaced with Church and Mosque, respectively. The word God was retained; although the term God is mainly used by Christians and Allah by Muslims, the term God is accepted and understood by both Muslim and Christian religious leaders as being an accurate translation of the word Allah from Arabic into English. The following is an example of an item being altered during translation: ‘prayer and spiritual enrichment are more important than medicine in treating mental illness’ was modified to ‘prayer and spirituality are more important than medication in treating persons who are mentally ill’. Therefore, two new items were added: (1) medications being more helpful than prayer or counselling; and (2) the belief that medications are addictive. Items used the same five-point Likert scale – strongly agree, agree, neutral, disagree, strongly disagree – as the original (Lafuze et al., 1999, 2002). A don’t know option was also added to allow respondents to save face, as clerics in Arabic-speaking communities are often expected to have knowledge and wisdom in all domains.
Lafuze et al. (2002) analysed their questionnaire by dividing the causes of mental illness into three main categories: biological causes, psychological causes and religious causes. Inspection of internal reliability coefficients [(Cronbach’s alpha (α)] in the Arabic-speaking sample indicated that the internal reliability coefficient for biological causes was not satisfactory (α = 0.13). In addition, Lafuze et al. (2002) originally categorised drug and alcohol addiction as a biological cause, whereas we also considered it a potential psychosocial cause. Thus, we described and analysed each cause separately.
Data analysis
The frequency of agreement for the various causes and beliefs about psychiatric medications is provided for the total sample. A few of the items had a moderate skew resulting in violations of the normality assumption. Independent t-tests were used to analyse the comparisons between Muslim and Christian clerics. As a precaution against the undue effects of skewness in the data, we replicated these analyses using non-parametric procedures (Mann–Whitney U test). In all cases, the pattern and significance of the results were the same. Consequently, we have reported the means and t-test results for ease of interpretation. Due to multiple statistical tests being conducted, Bonferroni adjustment of p values (p < 0.005) was used for each block of analyses to reduce the risk of type I errors.
Results
Demographic details
The demographic variables for Muslim and Christian clerics are described in Table 1. An independent group t-test was used to compare the length of stay in Australia, length of time as a religious leader/cleric and size of congregationbetween the two groups of clerics. Results revealed that Muslim clerics had less time as a religious leader (M = 14 years, SD = 9.5 years) and smaller congregations (M = 1228, SD = 2144) than Christian clerics (M = 16 years, SD = 11.5 years; M = 2227, SD = 3064), p < 0.05.
Causes of mental illness
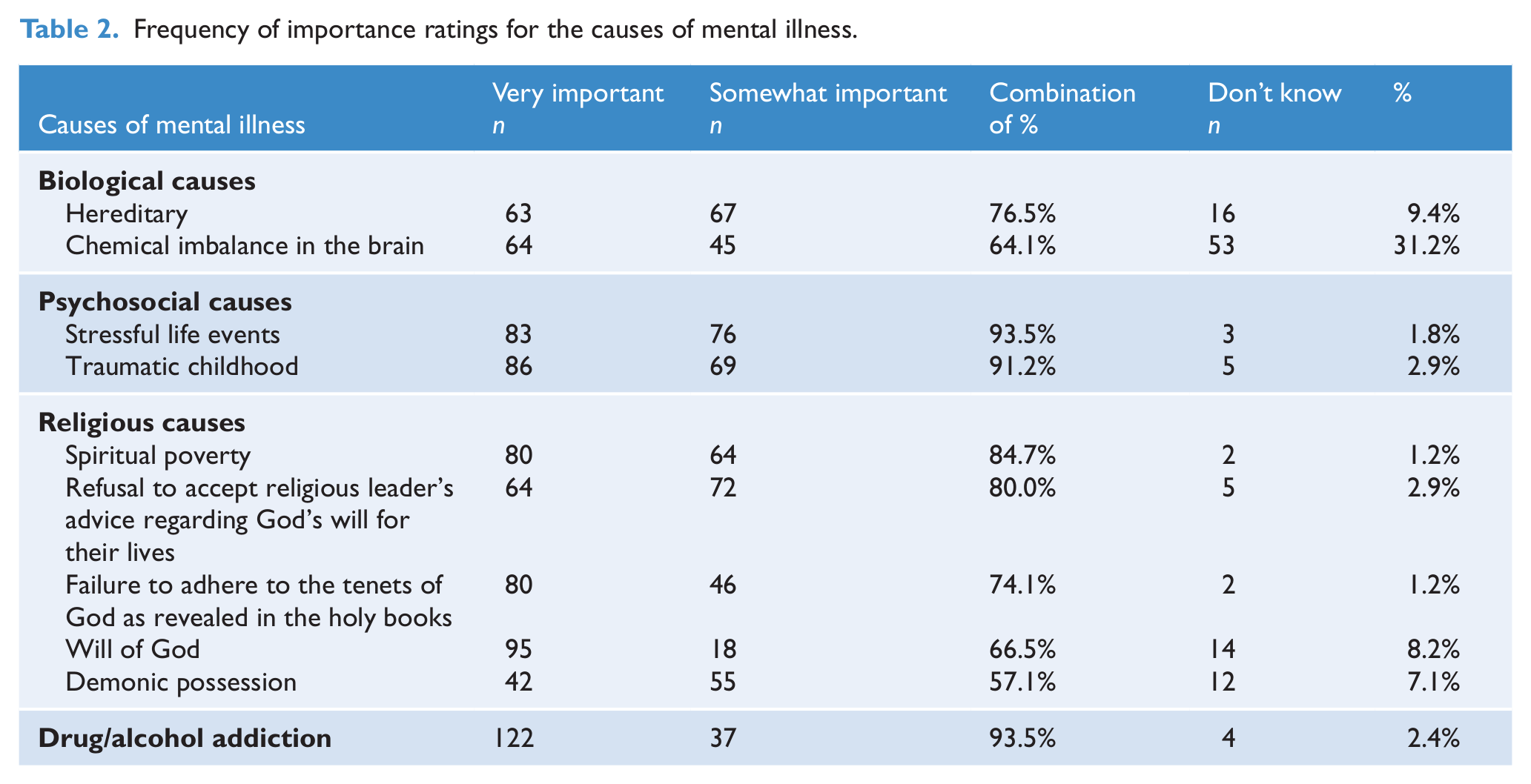
Overall, an average of 70% of participants rated two biological causes as very important or somewhat important (see Table 2). The majority of participants (93.5%) rated drug and alcohol addiction as very important or somewhat important. For psychosocial causes, a range of 91.2–93.5% of the sample rated these as very important or somewhat important. Religious causes had a 57.1–84.7% rating of very important or somewhat important. A high percentage of clerics (31%) responded with don’t know to chemical imbalance in the brain.
Frequency of importance ratings for the causes of mental illness.
Comparisons between Muslim and Christian clerics revealed that differences only occurred in the broad domain of religious causes for mental illness (Table 3). Specifically, Muslim clerics rated religious causes such as the Will of God as more important than did Christian clerics. This was significant for four of the five religious causes.
Comparison of Muslim and Christian clerics’ mean importance ratings for the different causes of mental illness.
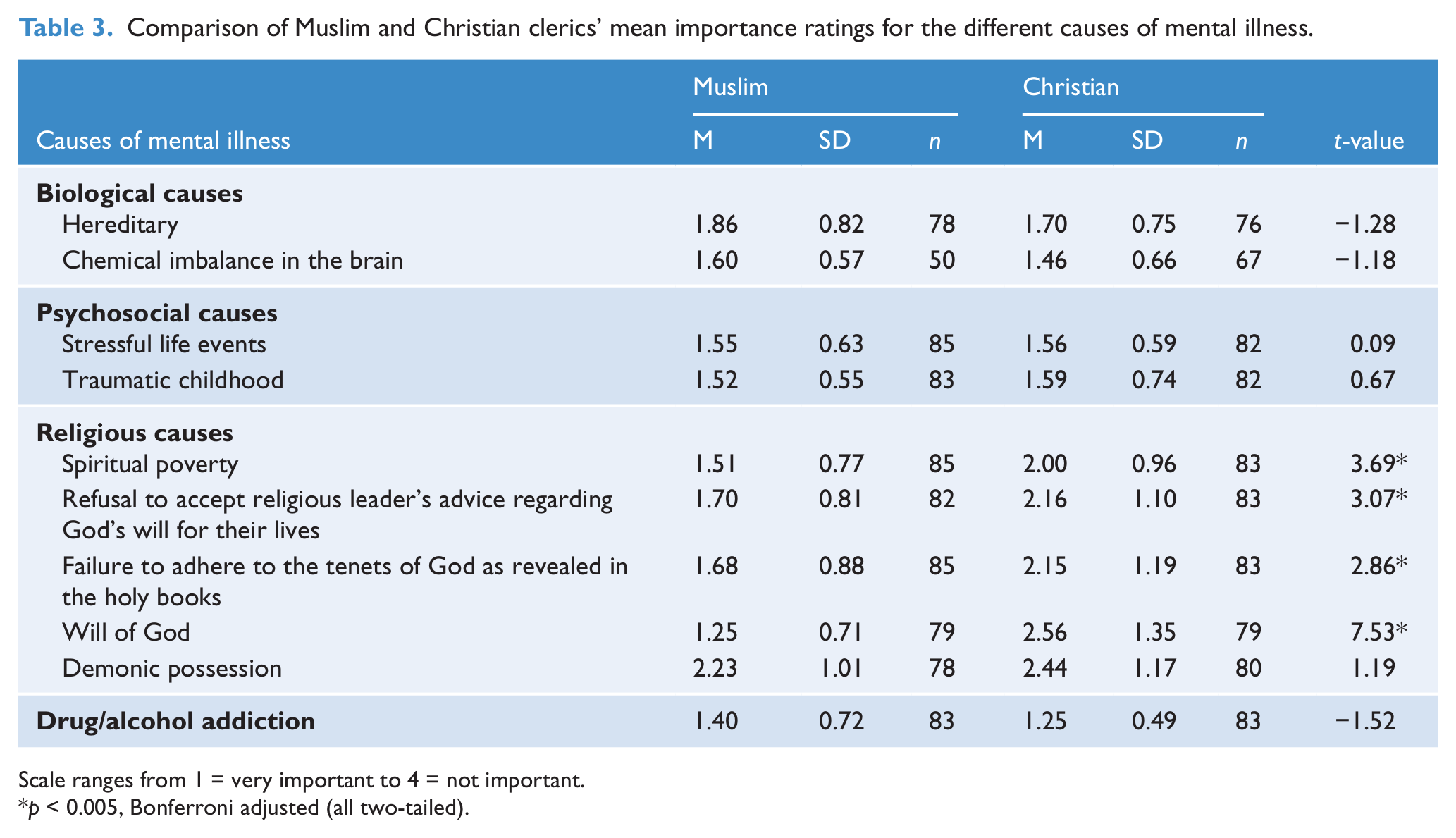
Scale ranges from 1 = very important to 4 = not important.
p < 0.005, Bonferroni adjusted (all two-tailed).
Beliefs about medication
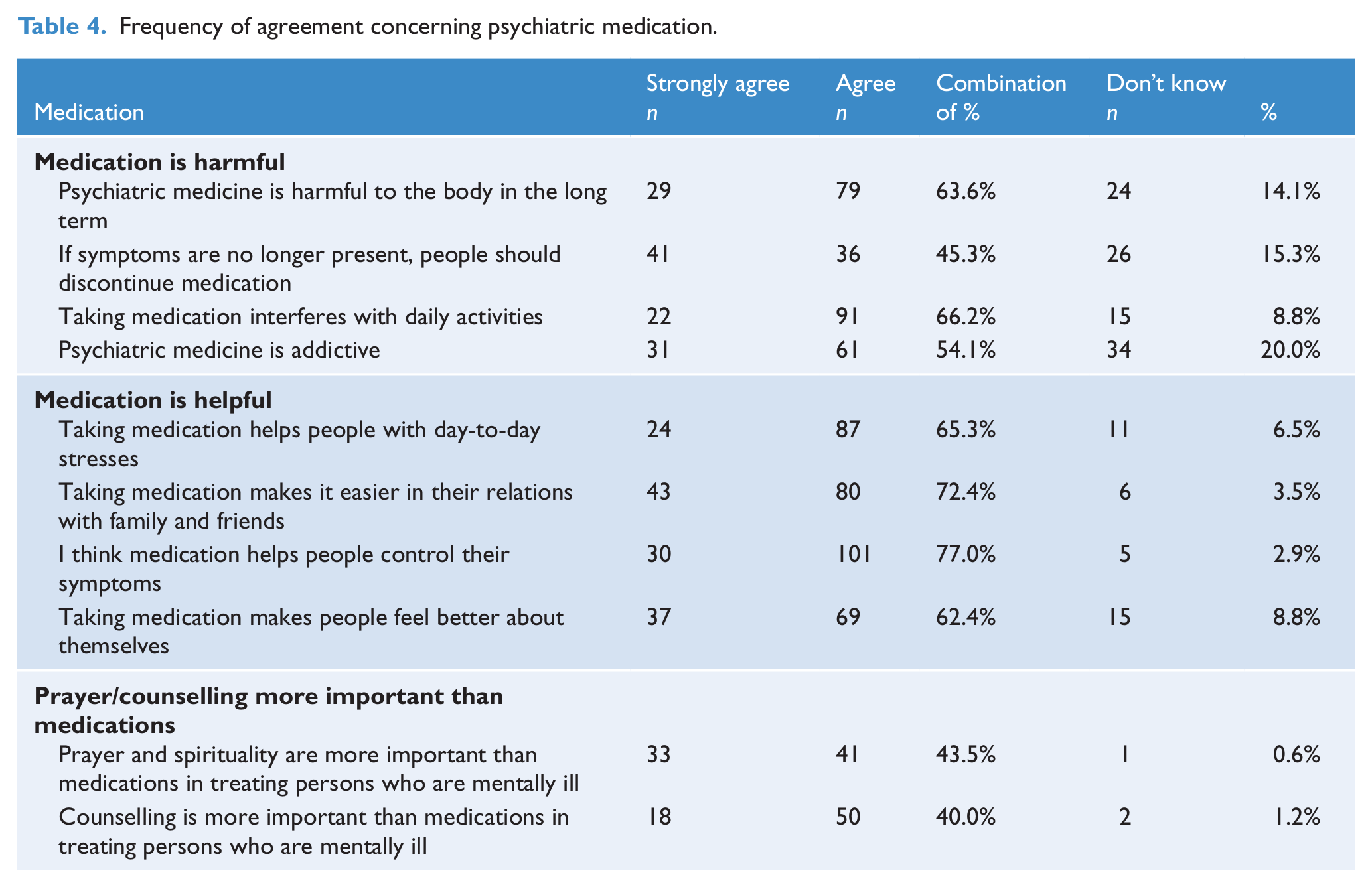
Table 4 provides descriptive data indicating the frequency of agreement with each medication-related item along with the number of don’t know responses. Following Lafuze et al. (2002), attitudes to medication were divided into three categories: medication is harmful (four items), medication is helpful (four items) and prayer/counselling more important than medications (two items). One new item was added to the medication is harmful subscale, (psychiatric medicine is addictive). The resulting α coefficients were: medication is helpful (α = 0.59); medication is harmful (α = 0.76); and prayer/counselling more important than medications (α = 0.71). Inspection of the distributions indicated that the scales were normally distributed; paired t-tests were used to explore whether medication was on average viewed more as helpful or harmful. Lower means indicated higher agreement.
Frequency of agreement concerning psychiatric medication.
All means were significantly different after Bonferroni correction. Medication is helpful (M = 2.15, SD = 0.68, t (166) = 1.11 p < 0.001) had significantly greater agreement than medication is harmful [M = 2.32, SD = 0.78, t(163) = 2.26, p = 0.02], also when compared to prayer/counselling more important than medications [M = 2.90, SD = 1.10, t(167) = 7.42, p < 0.001]. Medication is harmful had a higher mean agreement than prayer/counselling more important than medications [t(164) = -6.52, p < 0.001].
Independent, two-tailed t-tests between the two religious groups regarding their beliefs about medication revealed that the mean values for medication is helpful were not significantly different between the two groups of clerics. There were significant differences between Muslim (M = 2.04, SD = 0.69) and Christian (M = 2.62, SD = 0.76) clerics for the variable medication is harmful [t(163) = 5.18, p < 0.001]. Similarly, Muslim clerics (M = 2.53, SD = 0.97) agreed more with the statement prayer/counselling more helpful than medications than Christian clerics [M = 3.29, SD = 1.10, t(167) = 4.78, p < 0.001]. On average, Muslim clerics believed that medication was more harmful than did Christian clerics. Muslim clerics believed that prayer and counselling were more important than medication compared to Christian clerics. Table 5 shows the comparisons of beliefs about medications at the item level.
Comparisons of the beliefs Muslim and Christian clerics hold regardingconcerning psychiatric medications.
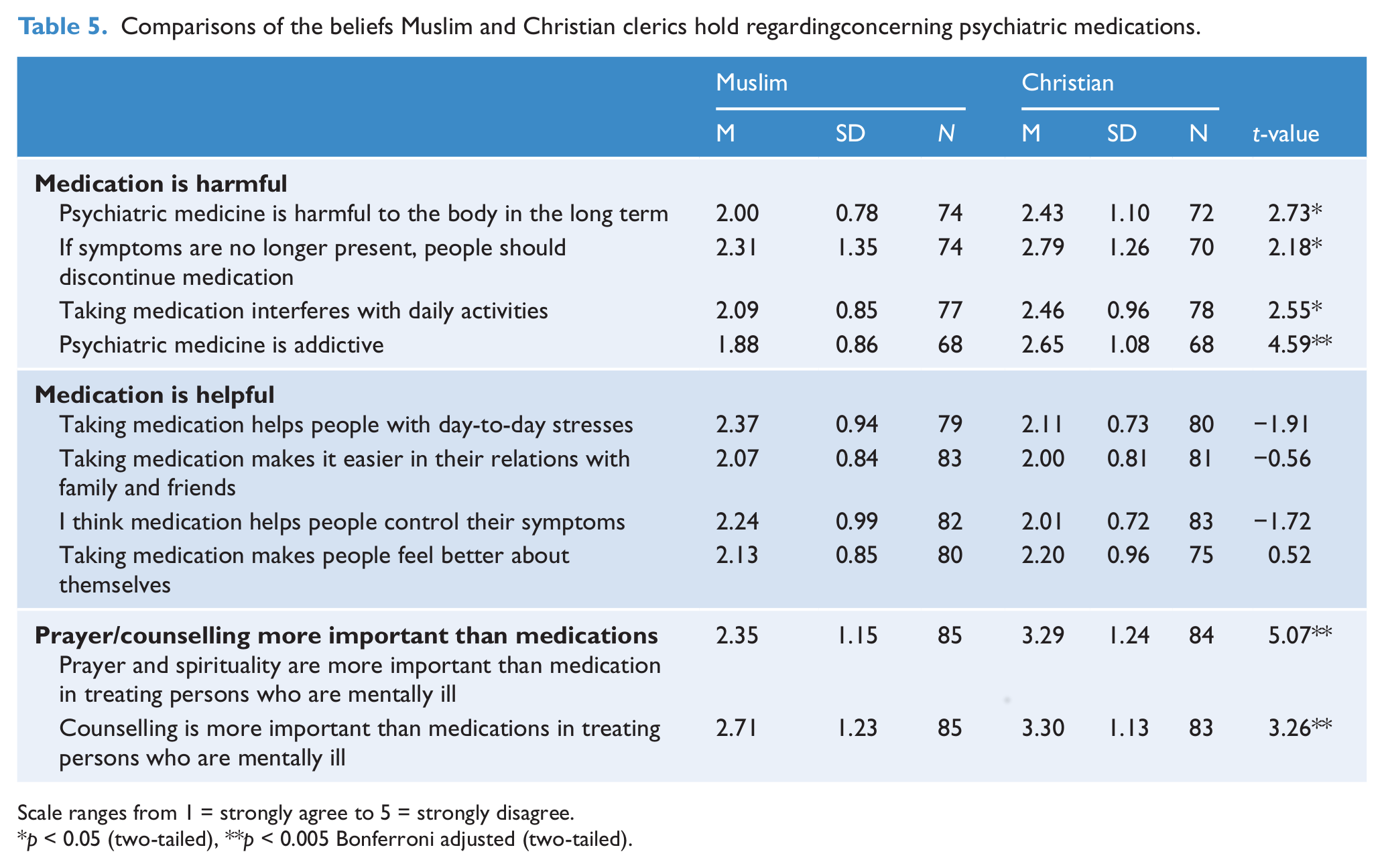
Scale ranges from 1 = strongly agree to 5 = strongly disagree.
p < 0.05 (two-tailed), **p < 0.005 Bonferroni adjusted (two-tailed).
Discussion
The results indicate that the Arabic-speaking religious leaders in our study believed that drug and alcohol addiction and psychosocial factors were the most important causes of mental illness. There was a great deal of uncertainty about whether a chemical imbalance in the brain was a cause of mental illness, although around three quarters of participants believed hereditary factors were important. Although fewer Muslim religious leaders (41%) perceived a chemical imbalance in the brain to be a cause of mental illness compared to their Christian counterparts (56%), mean differences regarding this item did not reach statistical significance. The uncertainty and relatively low rates of endorsement of chemical imbalance in the brain as a cause is in contrast with the US study involving Methodist pastors. Ninety-three per cent of pastors viewed chemical imbalance as very important or somewhat important (Lafuze et al., 1999, 2002).
Over 90% of Arabic-speaking religious leaders in this study considered psychosocial causes to be the principal agent of mental illness. It is unclear whether these religious leaders are responding to perceptions of environmental stress in Arabic-speaking communities related to relatively high rates of Arabic-speaking refugee immigrants (Ali et al., 2005). A study of the beliefs about the causes of mental illness among Christian and Muslim Ethiopians through interviews conducted with their priests and Imams produced similar findings (Jacobsson and Merdasa, 1991).
It is unclear whether the high rates of endorsement of drug and alcohol addiction as a cause of mental illness are related to perceptions of drug and alcohol use in the community or the prohibition of such substances as part of Arabic-speaking community standards and/or religious doctrine. Each of the five items on religious causes was endorsed by between 57% and 85% of clerics. These high percentages are consistent with the strong religious faith of Arabic-speaking clerics and their views that those with a compromised spiritual life will lack emotional stability and peace. Arabic-speaking clerics believe that relief from or cure for a mental illness or spiritual poverty is achieved through faith and prayer (Al-Krenawi and Graham, 1999). Westernised, Arabic-speaking people are viewed by clerics as being at risk of losing their religious identity due to the numerous adjustments that encroach on their spiritual commitments, such as attendance at mosque on Fridays or church on Sundays. Muslim clerics rated the religious causes of mental illness as significantly more important than Christian clerics. The religious item Will of God as a cause of mental illness was endorsed by 66% of Muslim clerics, whereas only 34% of Christian clerics agreed with this item. Arabic-speaking Muslims have a profound belief in God’s will and profess a fatalistic viewpoint, implying that future events, be they beneficial or detrimental, are entirely dependent on God’s will (Al-Nasimi, 1984). The consequences for the sins of ignoring God, being materialistic or being overly self-absorbed include stress, worry and anxiety.
By comparison, the Methodist pastors in the US study (Lafuze et al., 1999, 2002) placed less emphasis on the religious causes of mental illness and endorsed the biological and psychosocial causes more highly than their Australian Arabic-speaking counterparts. The beliefs of Arabic-speaking clerics that religious and psychosocial causes are more important than biological causes may affect their views regarding the treatment of the mentally ill, the use of prescribed medication and the decisions about whether to refer to professional mental health services. For example, if biological causes are not considered important, then the use of medications and referral to a psychiatrist might be a less likely option. However, if psychological processes are thought to be a principal cause, then referral for counselling might be considered more appropriate.
The findings regarding the perceived role and benefits of medications in the treatment of mental illness may also help explain referral rates. Between 62% and 77% of Arabic-speaking clerics endorsed items suggesting that the use of medications is helpful. Perceived helpfulness was similar for Muslim and Christian clerics. There was general recognition that medications help manage symptoms, but this was possibly mitigated by beliefs about the harmful effects of medications. There were concerns about the addictive nature of psychiatric medicines, with 54% of clerics agreeing and a further 20% responding with don’t know to this item. Beliefs that medications may be harmful are broadly consistent with the views of US Methodist pastors (Lafuze et al., 1999, 2002). Muslim clerics agreed significantly more strongly with items indicating that psychiatric medications were harmful and possibly addictive compared to Christian clerics.
Although, to our knowledge there are no other data on the views of Arabic-speaking clerics on psychotropic medications, studies of other samples suggest that the Arabic-speaking community may have less knowledge about medications than the non-Arabic-speaking community. For example, a study of Iranian immigrants to Australia found a high use of analgesic drugs and tranquillisers and limited knowledge of the side effects associated with prescribed drug usage (Khavarpour and Rissel, 1997). Ambivalence concerning the helpful or harmful effects of medications was also reflected by the present study’s findings which indicate that prayer and counselling were viewed as more important than medications in the treatment of mental illness. Again, Muslim clerics agreed with this significantly more strongly than Christian clerics, with the majority of Muslim clerics (62%) agreeing that prayer and spirituality were more important than medications in treatment. This contrasts with only 35% of US Methodist pastors who agreed with this item (Lafuze et al., 1999, 2002).
It has been suggested that the opinions of Muslim clerics may derive from the influence of medical advice for physical and psychological ailments found in the Koran and Hadith, collectively known as prophetic medicine (Al-Krenawi and Graham, 1999, Al-Nasimi, 1984). In Islamic tradition, prayer is recognised as an essential component in healing the sick. Christianity also values prayer as a form of treatment for physical and mental illness. It appears that the belief in the healing power of prayer of Arabic-speaking clerics may also be reflected in their beliefs and attitudes concerning people afflicted with mental illness.
The study has several limitations, requiring caution in the interpretation of the data. First, while the questions used in this survey were derived from a US survey which allowed points of comparison, the measure had no prior reliability or validity data. Internal reliability for some subscales was satisfactory, but it was not so for others, and some analyses had to be conducted using individual items. Further, all questions were administered during face-to-face interviews. As a result, the study was susceptible to potential socially desirable response. Finally, the questions did not differentiate between different forms of mental illness; therefore, it is unclear whether clerics were thinking of people with depression, anxiety or psychotic disorders. Thus, any future research would benefit from differentiating between the major types of mental disorders, perhaps using a vignette methodology.
Despite these concerns, the present study provides an indication of the beliefs of Australian Arabic-speaking clerics about the general causes of mental illness and the use of medications as treatment. These views have important implications for understanding how to target educational strategies for the clergy. In addition, it provides insights into the issues that need to be addressed to facilitate more appropriate ways of working collaboratively with Arabic-speaking clerics, to better recognise the needs of those with mental illness in their communities. For example, the relatively low endorsement frequency for chemical imbalance in the brain as a possible cause of mental illness suggests that Arabic-speaking clerics may benefit from education about the role of neurotransmitters in many mental disorders. Future research is needed to determine whether such educational strategies lead to changes in attitudes and ultimately changes in the willingness of clerics to refer to mental health professionals. Similarly, mental health professionals working with people from Arabic-speaking backgrounds need to be aware of the important role that religious leaders play in their communities. They need to be sensitive to and respectful of the beliefs that may have been transmitted through prior contact with religious leaders. There is a need to open up channels of communication between professional mental health services and Arabic-speaking religious leaders to facilitate collaborative care.
Footnotes
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.