
Abstract
Objective:
Firesetting is often reported to be associated with psychopathology, but frequently these conclusions are based on studies reliant on selective forensic psychiatric samples without the use of comparison groups. The aim of the study was to examine the rates of mental illness, substance use disorders, personality pathology and psychiatric service usage in a population of convicted firesetters compared with other offenders and community controls.
Method:
Using a data-linkage design, the study examined the psychiatric histories and usage of public mental health services by 1328 arsonists convicted between 2000 and 2009 in Victoria, Australia. These were compared with 1328 matched community controls and 421 non-firesetting offenders.
Results:
Firesetters were significantly more likely to have been registered with psychiatric services (37%) compared with other offenders (29.3%) and community controls (8.7%). The firesetters were also more likely to have utilised a diverse range of public mental health services. Firesetters attracted psychiatric diagnoses more often than community controls and other offenders, particularly affective, substance use, and personality disorders.
Conclusions:
This study confirms that there is a link between firesetting and psychopathology, suggesting that there is a role for the psychiatric screening of known firesetters, and a need to consider psychopathology in formulating the risk for further firesetting.
Introduction
Psychiatric disorders are purported to play a role in the aetiology of violent crime (Arseneault et al., 2000; Douglas et al., 2009), and offenders are more likely to come into contact with psychiatric services than community members (Short et al., 2013; Wallace et al., 1998, 2004). However, evidence for the role of psychopathology in firesetting is less clear. This information is pertinent to understanding the potential aetiology of firesetting and in formulating and managing firesetters’ risk of such behaviour in the future. Moreover, having a greater knowledge of the prevalence and nature of mental illness among firesetters will assist in highlighting areas of treatment need. (In this article, the term firesetters will be used to include people who intentionally set fires regardless of motivation or legal status. Arsonists, by contrast, are firesetters who have been convicted of intentionally setting fires.)
Previous research on the nature and rates of psychiatric illnesses among firesetters has yielded inconsistent results, with some studies suggesting that general psychopathology (MacKay et al., 2009), alcohol and substance use disorders (Ritchie and Huff, 1999; Vinkers et al., 2011), intellectual disability (Devapriam et al., 2007; Enayati et al., 2008), personality disorders (Barnett et al., 1997; Wallace et al., 1998) and psychosis (Anwar et al., 2011; Lindberg et al., 2005) are associated with a greater incidence of firesetting and recidivism. Other studies, including those using community samples, find that the rate of psychosis and general psychopathology in samples of firesetters is not necessarily higher than non-firesetting offenders (Enayati et al., 2008; Labree et al., 2010; Stewart, 1993), or is only evident when substance misuse is also present (Wallace et al., 1998).
There is also a dearth of research examining the lifetime use of public mental health services by firesetters, and whether service usage increases at the time of offending. Understanding service usage patterns is vital as it determines whether psychiatric services may be in a position to assist with the prevention of firesetting behaviour. Koson and Dvoskin (1982) found in their sample of incarcerated mentally disordered firesetters that most were either receiving mental health treatment or had recently discontinued treatment at the time of lighting a fire for which they were apprehended. Others reporting on the rates of firesetting amongst offenders and general psychiatric inpatients in secure psychiatric facilities suggest that both a history of firesetting (Quinsey et al., 2006; Räsänen et al., 1995; Swaffer et al., 2001) and the experience of acute psychiatric symptoms in the days prior to a firesetting offence are common (Ritchie and Huff, 1999). Examination of the patterns of service usage of firesetters thus has important implications for intervention with acutely unwell individuals who may also be at increased risk of firesetting.
A significant disadvantage in the quest for obtaining valid information about mental illness and service usage among firesetters is that the firesetting literature is typically limited by the use of selective forensic psychiatric samples. Furthermore, only two, now dated, studies have made use of adequate offender comparison samples (Jackson et al., 1987; Räsänen et al., 1995). It is thus difficult to determine whether firesetters are any more or less likely to suffer from a mental disorder than other offenders, whether this has any impact on their offending, and thus whether firesetters should receive specialist psychiatric attention.
The current study is the first to examine the entire population (n = 1328) of convicted arsonists within a jurisdiction over a 9-year period. A data-linkage design was used to link the sample of arsonists, a matched sample of non-firesetting offenders and a general community sample to the state-wide public mental health database. This allowed for examination of the patterns of psychiatric disorder and public mental health service usage of firesetters in comparison to offenders and community members.
Aims and hypotheses
The current study attempted to overcome some of the methodological limitations of previous research by comparing the rates of mental illness, substance use disorders, personality pathology and service usage among arsonists, other offenders and community controls. The following hypotheses were made:
There will be higher rates of mental health service usage among arsonists compared with community members and offenders.
There will be a higher rate of mental disorder, including childhood disorder diagnoses, personality disorder and substance use diagnoses among arsonists compared with the other groups.
Method
Firesetters
The study group was identified using records from the Sentencing Advisory Council of Victoria (SAC) who provided the names, dates of birth, charges and conviction dates for all 1328 people convicted of arson and other firesetting offences in the state of Victoria, Australia between 2000 and 2009. Where offenders were convicted of more than one offence concurrently, they were included in the sample where arson was the most serious offence conviction. This would exclude only a few cases in which other charges were viewed as more serious than arson (e.g. homicide, attempted homicide or serious personal injury offences).
Arson offences in the sample included: arson causing death, criminal damage by fire (arson), criminal damage by fire – view to gain, criminal damage by fire – endanger life, intentionally cause a bushfire, light fire on public transport commission vehicle or premises, light/use fire to damage or destroy property, light/use fire to endanger property/life, set fire to litter receptacle. Arson-related offences included: light fire in open air without authority, light fire during prohibited period, wilfully give false fire alarm, light fire in open air – country fire danger, light fire on Total Fire Ban day, light fire on day of acute fire danger, fail to extinguish fire, leave fire unattended, allow fire to remain alight, cause false fire alarm to be given, allow fire in the open air to remain alight (Total Fire Ban), fail to extinguish fire on Country Fire Authority direction, light fire in country during extreme weather conditions, fail to prevent fire from spreading, maintain fire during prohibited period, fail to inform authorities of fire, use unsafe equipment during country fire period, cause fire to intentionally destroy, bomb hoax, and in open air throw or drop burning material. Many arson-related offences concern lighting fires on days where the weather conditions make it a hazardous behaviour, typically on days of extremely hot and windy weather. Such behaviour has been criminalised in Victoria as it is one of the most fire-prone environments in the world (Pyne, 1995).
Community comparison sample
The comparison group was drawn from a random sample of 4830 Victorian residents (total population approximately five million) on the electoral roll. Voting is mandatory in Australia and registration on the electoral roll is compulsory for those 18 years and over. A total of 92.28% of those aged 18 and above are on the rolls (Victorian Electoral Commission, 2012). Only limited information on the comparison group from the electoral roll was available, including first name, surname, gender and age range within 2-year bandings. Firesetters were matched on gender and age band to subjects in the comparison group, to constitute 1328 matched controls.
Non-firesetting offender sample
Of the 4830 community cases, 429 (8.9%) people had received a criminal charge. These individuals were selected for use as an offender comparison sample. Eight individuals (1.85% of those with a criminal history, 0.17% of the community sample) in this group had a prior charge for arson and were thus excluded from the sample, reducing the number to 421. Given the small sample size of offenders, it was not possible to match them to the larger sample of firesetters.
Ethics
Ethics approval was granted to conduct data linkages without the express consent of the individuals whose information was obtained. This methodology was developed in accordance with the Australian National Health and Medical Research Council guidelines (2007), and steps were taken to ensure the anonymity of participants by deleting all personal identifiers and only reporting on aggregate, group-level data. This methodology was considered appropriate and approved by four independent ethical committees: the Victorian Department of Justice Human Research Ethics Committee, Victoria Police Human Research Ethics Committee, Monash University Human Research Ethics Committee, and the Victorian Department of Health Human Research Ethics Committee.
Mental health histories
The Victorian Psychiatric Case Register (VPCR) is one of the world’s oldest and most comprehensive psychiatric registers. All contacts with the public mental health service are recorded, including contacts in emergency services, inpatient units, or community services, and forensic mental health services. The VPCR records the date, nature and duration of the contact, diagnosis if made and treatment, if any, that was provided. Mental disorders are recorded according to the International Classification of Diseases (ICD-10), and are typically diagnosed by psychiatrists. Any contacts with private services, including general practitioners and private clinicians, are not recorded on the register. Since most people with psychotic illnesses receive public health care at some point (Department of Health and Ageing, 2010; Jablenksy et al., 1999), the dataset represents the prevalence of those illnesses. However, since most people with low prevalence disorders, substance misuse and personality disorders do not receive public mental health care, the data do not represent the prevalence of these disorders (Wallace et al., 2004). Nonetheless, the data do allow for a comparison across the samples for low prevalence and related disorders.
Primary psychiatric diagnoses were coded into categories, replicating previous research (Cutajar et al., 2010; Short et al., 2010; Wallace et al., 2004). For example, the category ‘psychotic disorders’ included schizophrenia, schizoaffective disorder, schizotypal disorder, shared psychotic disorder, delusional disorders and unspecified non-organic psychosis (ICD-9 codes 295 and 297, plus ICD-10 codes F20, F21, F22, F24, F25 and F29). The latter excluded organic or transient forms of psychosis, such as substance-induced psychosis, depression with psychotic features, or senile psychotic conditions. Given the large number of potential diagnoses an individual may receive over a lifetime, diagnoses were only coded when they were upheld in 75% of the diagnoses given, or there was a clear diagnostic progression over time resulting in a clear diagnosis. This method has been used by several studies and demonstrates good reliability (Bennett et al., 2011; Krupinski et al., 1982; Short et al., 2010).
A ‘substance-use disorder’ was defined as any type of substance abuse, substance dependence, or substance-induced disorder (such as substance-induced psychosis), excluding nicotine-related disorders.
Data linkage
The data-linkage procedure first involved a deterministic then probabilistic approach – extracting exact and then probable linkages from the VPCR using identifying information (first name, surname, aliases, date of birth, age range and gender). Where there were matches, de-identified psychiatric records were obtained for contacts made prior to 21 September 2011.
Analyses
Descriptive statistics and frequencies were used to characterise the sample. Continuous data were compared using independent t-tests or Mann–Whitney U tests, and categorical variables were compared using chi-squared tests of association, using phi correlations as an estimate of effect size. Odds ratios (OR) were calculated with 95% confidence intervals. Age for the firesetters was calculated at the time of the index date, while for the community and non-firesetting offender groups it was calculated at the date of extraction from the database (01 September 2009). The Mann–Whitney U effect size statistic θ was estimated by 1 – U/mn, where m and n are the sample size of each group and θ = 0.5 is analogous to d = 0 (Newcombe, 2006a, 2006b). Data analyses were undertaken using the Statistical Package for the Social Sciences (SPSS), version 20 (IBM Corp., Armonk, NY).
Results
Characteristics
The firesetting group comprised 1328 individuals (1140 males, 85.9%; 188 females, 14.2%), mean age 33.4 years (range 9–83 years; SD 14.4). The community sample comprised an equal number of individuals with the same gender distribution and a similar mean age 34.7 years (range 14.7-77.01; SD 12.4). The offender sample comprised 421 individuals (343 male, 81.5%), mean age 35.0 years (range 15.0-62.3; SD 11.6). In total, 492 (37.0%) firesetters, 116 (8.7%) of the community sample and 123 (29.3%) of the offenders were registered on VPCR. The number of individuals registered on VPCR differed significantly between firesetters and offenders (χ2 = 8.6, p < 0.01, φ 0.07), and firesetters and community members (χ2 = 301.6, p < 0.001, φ 0.34). Of those who were registered, gender did not differ significantly between the firesetters and offenders (χ2 = 0.7, p = 0.41, φ –0.03), nor between firesetters and community members (χ2 = 2.3, p = 0.13, φ 0.06). The age of those registered was significantly different between firesetters and offenders (U = 17,347, p < 0.001, θ = 0.71), and firesetters and community members (U = 20,674.5, p < 0.001, θ = 0.64). Of note, 96 (7.2%) of the firesetters received their first diagnosis only after being charged with the index offence.
Service usage
The age at first contact with mental health services did not differ significantly across groups (firesetters (M = 30.61 years, SD = 12.41, range 10–82), other offenders (M = 31.15 years, SD = 11.35, range 12–59) and community members (M = 30.12 years, SD = 13.69, range 8–59); firesetters vs offenders: U = 15,747, p = 0.53, firesetters vs community: U = 13,840, p = 0.54).
Firesetters had an average of 2.13 (range 0–214; SD = 9.31) episodes of contact with public mental health services, with an average of 616.20 days (range 0–3466; SD = 733.64) between the last registered contact and the index offence. As shown in Table 1, firesetters had significantly more contacts across a range of services than both community members and offenders (firesetters vs community: outpatient contacts (U = 651,474, p < 0.001, θ = 0.63), inpatient admissions (U = 743,624.5, p < 0.001, θ = 0.58) and outpatient contact with child or adolescent services (U = 580,557.5, p < 0.001, θ = 0.52); firesetters vs offenders: outpatient contacts (U = 231,892, p < 0.001, θ = 0.59), inpatient admissions (U = 257,227.5, p < 0.001, θ = 0.54) and outpatient contact with child or adolescent services (U = 270,238, p < 0.01, θ = 0.52)). Firesetters were admitted to inpatient facilities on average 3.16 (SD 10.48) times, offenders 0.71 (SD 1.46) times and community members 0.49 (SD 1.45) times.
Type of contacts with the public mental health service.
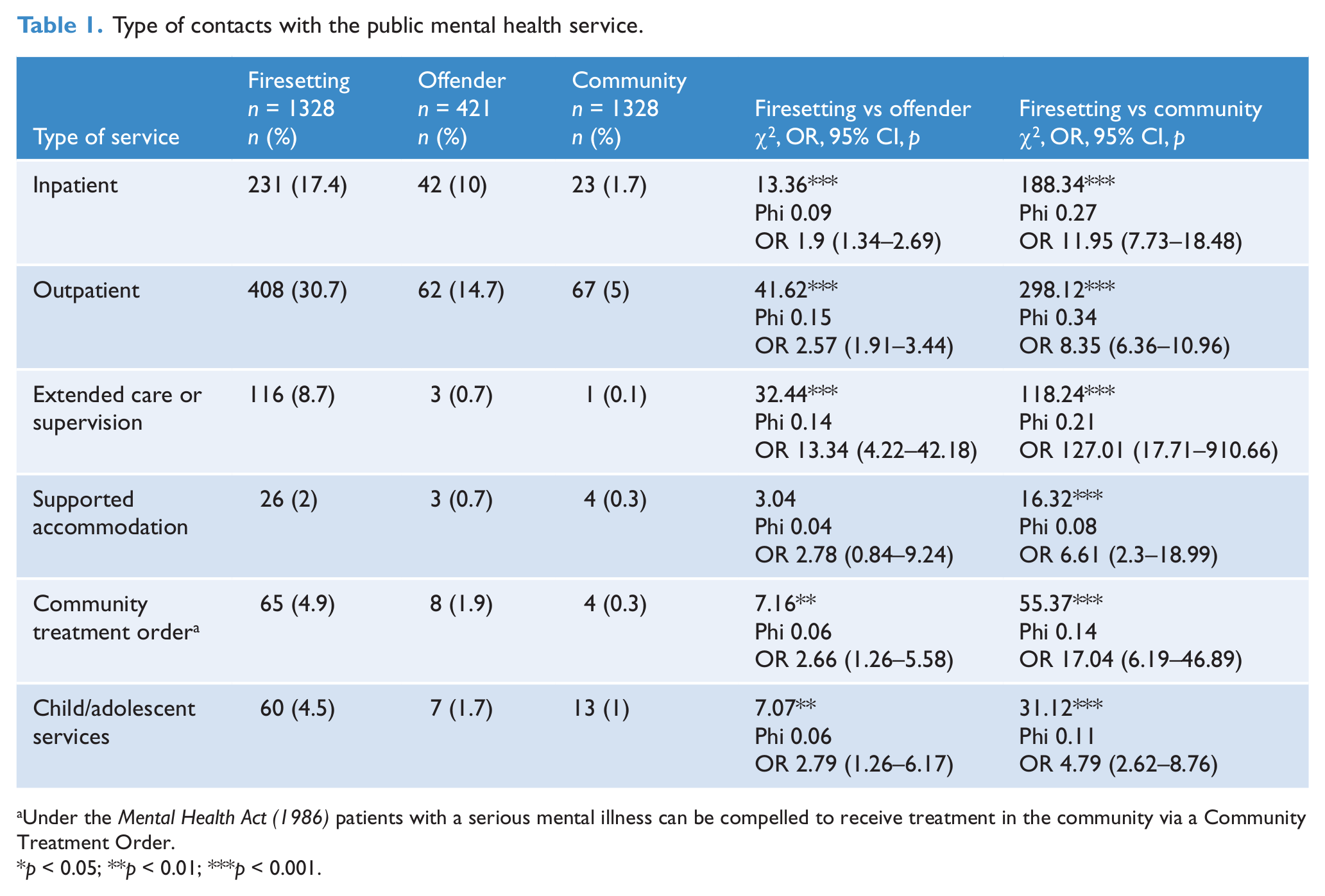
Under the Mental Health Act (1986) patients with a serious mental illness can be compelled to receive treatment in the community via a Community Treatment Order.
p < 0.05; **p < 0.01; ***p < 0.001.
Diagnoses
Tables 2 and 3 compare the clinical and personality diagnoses of firesetters and offenders, and firesetters and community controls. Firesetters had significantly higher rates of all diagnoses than other offenders, with the exception of psychotic disorders and bipolar affective disorder. The most marked between-group differences were found for affective disorders, substance misuse disorders, childhood disorders and personality disorders (especially antisocial and borderline types). Although the type of childhood disorder was only available for the firesetters, the most common diagnosis received was conduct disorder (n = 19, 1.4%). Very few people received a diagnosis of intellectual disability (ID) (n = 20, 1.5%; 17 mild, 1.3%) and they were all in the firesetting group. (Contacts with ID services are recorded on a separate database and thus the figures represented here are vast underestimates of the prevalence of ID in this sample.) There were only two diagnosed cases of pyromania, both in the firesetting sample. Examination of schizophrenia diagnoses alone showed that this category of disorder was more prevalent amongst firesetters than both offenders (89 (6.7%) vs 10 (2.4%), χ2 = 11.2, p < 0.001, φ 0.08, OR 2.95 (1.52–5.73)) and community members (89 (6.7%) vs 8 (0.6%), χ2 = 70.2, p < 0.001, φ 0.16, OR 11.85 (5.73–24.54)).
Frequency and comparison of clinical disorders between groups.
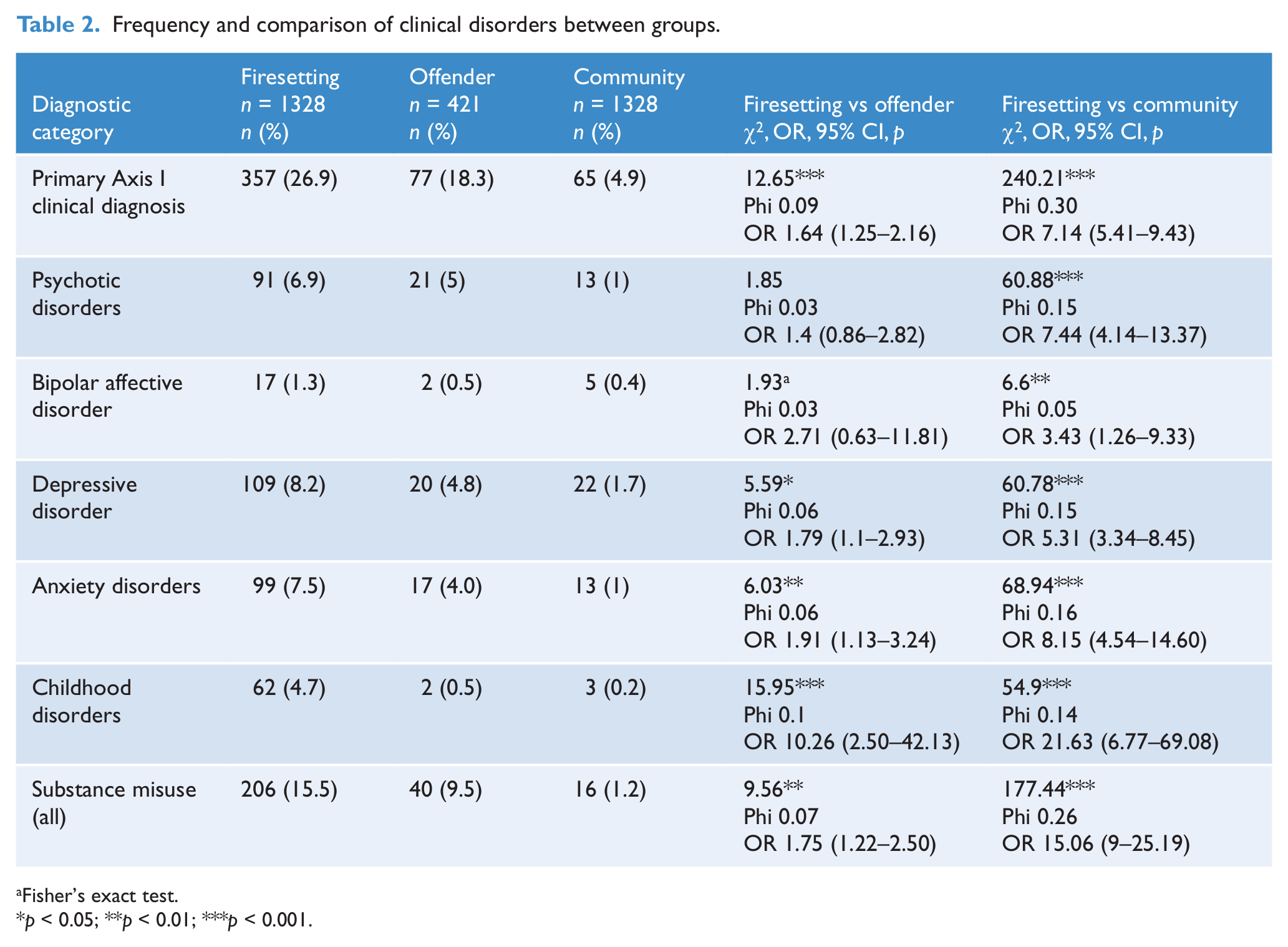
Fisher’s exact test.
p < 0.05; **p < 0.01; ***p < 0.001.
Comparison of the frequency of personality disorders between groups.
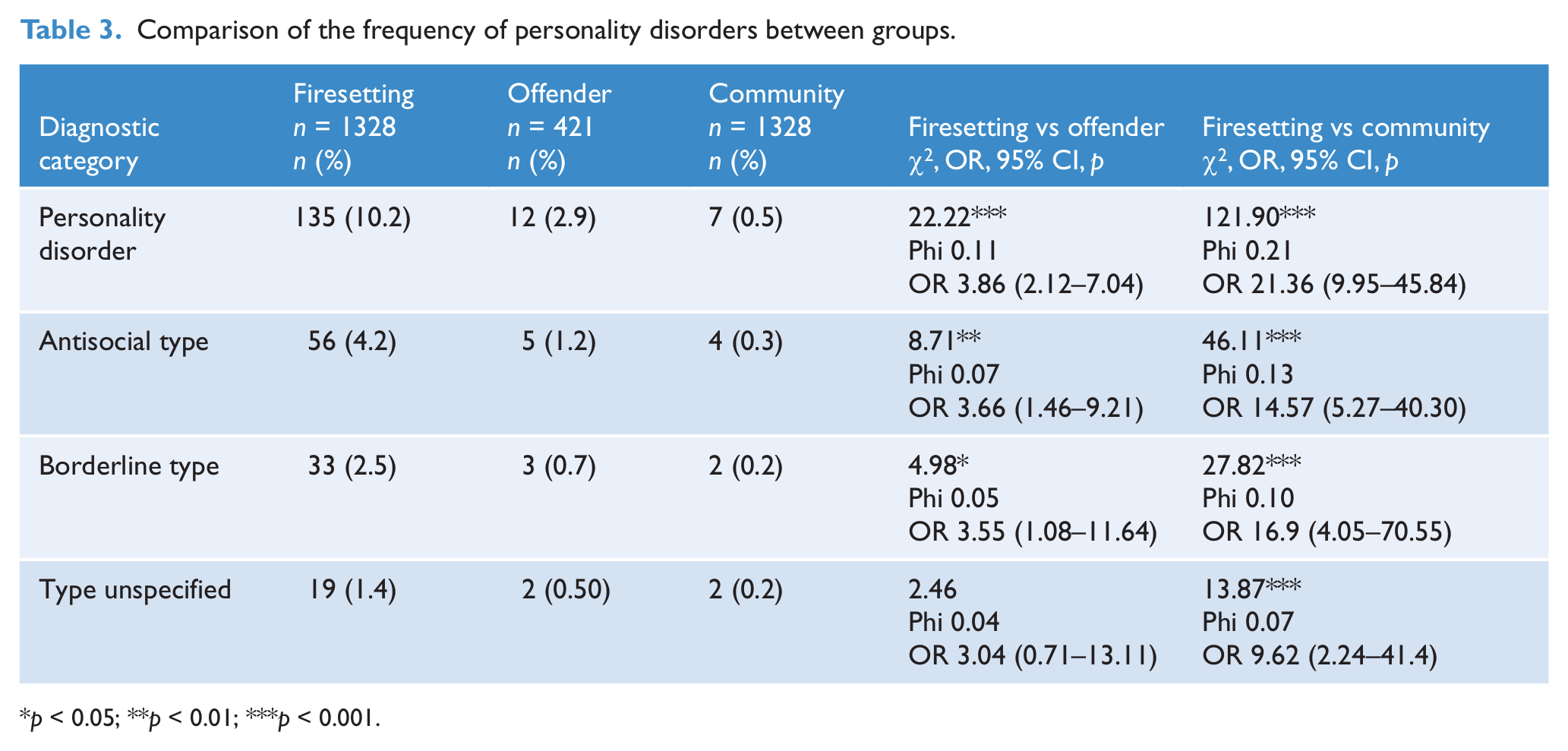
p < 0.05; **p < 0.01; ***p < 0.001.
Discussion
This is the first study to report on psychiatric morbidity and public mental health service usage in an entire population of convicted firesetters. The study is also unique in that it includes comparisons with other offenders and a matched general community sample. More than one-third (37%) of firesetters were registered on the psychiatric register, significantly more than other offenders (29.3%) or community members (8.7%). Firesetters were more likely to have had contact with public mental health services, and they tended to do so at a greater rate and across a more diverse range of services than both comparison groups.
Firesetters had higher rates of virtually all mental disorders when compared to community members. Given the literature that exists on the over-representation of offenders among psychiatric service users in general (Stevens et al., 2012), and firesetters in particular (Blanco et al., 2010; Tyler and Gannon, 2012), this finding was expected. The rate of psychotic disorders in the community sample is consistent with past international and Australian research reporting the lifetime prevalence estimate for schizophrenia (Perälä et al., 2007; Saha et al., 2005; Short et al., 2010; Wallace et al., 2004), suggesting that the higher lifetime prevalence of psychotic disorders amongst firesetters is likely to be an accurate representation.
Also as expected, mental disorders were more prevalent amongst firesetters than other offenders, with the exception of bipolar affective disorder and psychotic disorders (when examined as a category). The lack of statistical significance when comparing bipolar disorder has also been reported by Anwar and colleagues (2011) who conjectured that the symptoms of schizophrenia may be more related to firesetting than those associated with bipolar affective disorder (i.e. command hallucinations, delusions of mind/body). When schizophrenia was examined in isolation, firesetters were shown to be more commonly diagnosed with this disorder than other offenders. The higher prevalence of schizophrenia amongst firesetters may have implications for both firesetting motivations and the contexts in which fires occur for this subgroup of firesetting offenders, and may also explain the level of both acute and chronic service usage by firesetters.
Despite the focus on psychosis in the firesetting literature, it was not diagnoses of psychotic disorders that were most commonly received by any of the groups, but mood disorders. While one would expect this to be the case if diagnoses by private practitioners were included, the nature of the public mental health system is such that it tends to capture the more severe psychopathologies, with less than 10% of individuals with a primary diagnosis of depression or anxiety being treated by the public mental health system (Burgess et al., 2007). Several studies have provided estimates of psychosis in firesetting samples to be as high as 15–37%, while mood disorders are usually diagnosed at a lower rate (Enayati et al., 2008; Puri et al., 1995; Räsänen et al., 1995; Repo et al., 1997; Vinkers et al., 2011). This suggests that past research, particularly where selective psychiatric samples are utilised, may overstate the rate of psychosis in firesetters. Pyromania was only diagnosed in two cases, but these figures may under-represent the true prevalence of the disorder given that it would be rare for an individual to be presenting to psychiatric services with such a disorder (Grant et al., 2005), outside of a court-mandated assessment. However, the low prevalence of pyromania in the sample is consistent with the literature (Koson and Dvoskin, 1982; Ritchie and Huff, 1999); indeed, the lack of empirical evidence for the disorder has seen it considered for removal from the latest version of the Diagnostic and Statistical Manual of Mental Disorders (DSM) (American Psychiatric Association, 2012).
Several researchers have asserted that psychiatric disturbance is more frequent in the histories of adolescent firesetters; an assertion supported by the current study, although the rates are low. However, past studies have defined disturbance variously as drug use, suicidal and self-harming behaviour, depressive symptomatology and antisocial behaviour (MacKay et al., 2009; Martin et al., 2004). None of these would necessarily be captured by the VPCR and thus these findings may represent the more severely disordered individuals who required adolescent inpatient admissions or outpatient follow-up. Previous research has also relied on adolescents’ self-reports of both their firesetting behaviour and psychological difficulties, which is fraught with inconsistencies. While the numbers were few, the current findings suggest that there may be scope to identify and intervene via mental health services in cases where young people are at risk of firesetting.
Limitations
This study relied upon data routinely collected for non-research purposes, which impacts upon the level of detail available. For example, only limited demographic information was available from the databases, thereby limiting the degree to which potential confounds could be controlled for. It is also reliant on diagnoses being made by psychiatrists who are trained in the DSM/ICD system of diagnosis. Given the nature of the psychiatric register, high prevalence disorders, such as mood and substance misuse, as well as personality disorders, are under-represented since they are less likely to come to public mental health services than to be treated by general practitioners and other private health professionals, including psychologists. However, there is no reason to believe that this under-representation would differ between the groups and thus the VPCR still provides a valid comparative measure even though it cannot provide a measure of prevalence. Furthermore, inherent in case-linkage methodologies is a level of error attributable to both the original data entry and data-matching procedures.
Clinical implications
Perhaps the most important implication of the current findings is that while a large proportion of firesetters have had contact with mental health services and have received diagnoses, most did not. Contrary to some existing research drawn from psychiatric samples, it is not the case that most firesetters are mentally ill (for review, see Tyler and Gannon, 2012). As such, it is important to realise that firesetting is not merely the product of mental illness and a variety of other factors are likely to contribute to the behaviour (e.g. biological factors, developmental experiences, culture, social learning and psychological vulnerabilities such as inappropriate fire interest and offence-supportive cognitions (Gannon et al., 2012; Tyler and Gannon, 2012)).
Notwithstanding the information above, this research has important implications for both the early detection of and intervention with the sizeable subgroup of mentally disordered firesetters. More than one-third of the firesetters were known to the public mental health service prior to committing their index offence of arson, and a further 7% came to its notice after committing the firesetting offence. Doubtless many others receive services from general practitioners and other private health care professionals. As such, there are clearly opportunities to treat and assess firesetting risk when individuals become known to psychiatric services. Unfortunately, experience shows that general mental health professionals are unlikely to have expertise in dealing with firesetters and, in most cases, do not even canvass with patients the possibility of firesetting behaviour (Schwartzman et al., 1999).
These findings also strongly suggest a role for routine psychiatric review prior to sentencing for firesetting offences. While mental illness does not necessarily explain firesetting behaviour in all cases, it is clear that it is correlated and thus needs to be considered by the courts when sentencing. In the UK, while there is no specific statutory requirement to obtain a psychiatric report, judges often refer to R v Calladine (1975) in which Justice Boreham recommended that psychiatric reports be obtained before sentencing in all arson cases, reflecting the view that psychopathology is directly related to arson. As a consequence, as Tyler and Gannon (2012) report, approximately 2% of arsonists receive hospital orders from the courts in the UK and 10% of those arrested for arson are recognised as having a mental illness. The effect of such a process is to detect offenders who are mentally disordered, potentially providing the opportunity for diversion into mental health services where appropriate, or at least for including assessment and treatment options in sentencing.
A causal relationship between mental disorder and firesetting is unlikely to exist in the majority of cases but there is certainly evidence to suggest that it impacts firesetting behaviours and may interact with other vulnerabilities, and thus, as suggested by Fineman (1995) and Jackson (1994), and more recently Gannon et al. (2012), mental illness should be considered in formulating the risk of firesetting. These findings provide solid evidence that while there is strong concordance between firesetting and mental disorder (i.e. clinical diagnoses and personality pathology), firesetting is not confined to those individuals with severe mental disorders, such as schizophrenia or bipolar affective disorder, and, in fact, mental illness is not present in the majority of cases. Clinicians therefore need to assess for the presence of all types of mental disorders and to consider their influence when formulating the aetiology and ongoing risk of firesetting. Given the average length of time between last contact with services and index offence date, it would appear that firesetting is not necessarily associated with acute psychiatric symptomatology, even when it occurs in the context of a wider mental illness. Therefore, consideration should be given to the chronic impacts of mental disorder on executive functioning, impulsivity and inhibitive processes in addition to acute symptoms, especially given the preponderance of individuals with personality disorders and substance misuse problems.
Future directions
While psychiatric disorders are likely to be over-represented within populations of firesetters, there is still a need to understand the motivating and cognitive factors that may lead a person to lighting fires. Therefore, further research needs to determine how psychiatric disorder may impact upon firesetting risk, which will provide answers as to the appropriate management of risk in such offenders. In addition, prospective studies are still required to provide a true prevalence rate of psychiatric disorder in firesetters. With a greater understanding of the prevalence of mental disorder among firesetters compared with other offenders, there is a need to examine whether and how this may impact upon recidivism or the types of fires lit. While there is some research examining the motives of mentally disordered firesetters, there is no research examining if and how these may differ to non-mentally disordered firesetters.
Conclusions
The cost of firesetting is considerable, and the price of processing individuals through the criminal justice system burdensome (Teague et al., 2010). While psychiatric disorders do not account for the entirety, or even the majority, of firesetting behaviour, the over-representation of mental illness among firesetters suggests that it should be an important consideration when assessing firesetting behaviour. There may be opportunities for early detection and diversion of individuals who are suffering from psychiatric disorders and are at risk of firesetting. For this to occur, adequate assessments of both the firesetting behaviour and psychiatric disturbance need to be conducted, and future research needs to establish whether there are differences in the rate and type of fires lit by mentally disordered firesetters.
Footnotes
Acknowledgements
The authors wish to thank Dr Karen Gelb and the Victorian Sentencing Advisory Council for their assistance with identifying cases, and Dr Michael Davis for his suggestions and comments on parts of this manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.