
Abstract
Context:
It has been suggested that the commonly prescribed class of antidepressants selective serotonin reuptake inhibitors (SSRIs) are associated with birth defects. However, the teratogenic effect of individual SSRIs has not been previously compared using meta-analysis.
Objective:
To determine the strength of the association between individual SSRIs and major, minor, and cardiac malformation among infants born to women taking these medications.
Data sources:
Electronic search of CINAHL, EMBASE, Medline, PsycINFO, and ISI Web of Science using the search terms (SSRI OR antidepressant) AND (obstetric outcome OR malformation OR birth outcome OR teratogen), supplemented by manual searching of published references and requests of primary researchers for unpublished data.
Study selection:
There were 115 studies identified by electronic search and reviewed in full text, which yielded 16 papers reporting 36 data samples for major malformations, nine papers reporting 26 data samples for cardiac malformations, and four papers reporting seven data samples for minor malformations.
Data synthesis:
Fluoxetine (OR 1.14, 95% CI 1.01–1.30) and paroxetine (OR 1.29, 95% CI 1.11–1.49) were associated with increased risk of major malformations. Paroxetine was associated with increased risk of cardiac malformations (OR 1.44, 95% CI 1.12–1.86). Sertraline and citalopram were not significantly associated with congenital malformation. Between-sample heterogeneity was low and a range of methodological considerations had no significant impact on effect size. There was little evidence of publication bias.
Conclusions:
Fluoxetine and paroxetine should be avoided in the first trimester and among those at risk of an unplanned pregnancy.
Introduction
Pregnancy is a time of increased vulnerability for depression, with an incidence of between 10–15% (Bennett et al., 2004). Selective serotonin reuptake inhibitors (SSRIs) comprise the most frequently prescribed class of antidepressant medication and are indicated for moderate to severe depression and anxiety disorders. Prescription databases suggest that 3–6% of pregnant women take an SSRI during pregnancy (Andrade et al., 2008), whilst large pregnancy cohorts report prevalence of congenital malformation at up to 5% (Queisser-Luft et al., 2002). Despite ultrasonographic and other antenatal screening, congenital cardiac defects (Pradat et al., 2003) and neural tube defects (Detrait et al., 2005) occur in approximately one in 1000 live births and may account for an increasing proportion of infant mortality (Rosano et al., 2000). Therefore, co-occurrence of SSRI use and congenital malformations, including those associated with poor infant outcome, can be expected. All SSRIs are known to cross the maternal-placental barrier (Oberlander et al., 2004), and highly powered case–control studies suggest an association between SSRIs and specific congenital malformations (Alwan et al., 2007; Louik et al., 2007). Hence, the safety of SSRIs during pregnancy cannot be assumed and their widespread use is a cause of concern for both pregnant women taking these medications and their doctors (Einarson et al., 2001b).
It has been suggested that paroxetine is more teratogenic than other SSRIs (Udechuku et al., 2011). The US Food and Drug Administration accord paroxetine a pregnancy safety classification of D, which indicates that there is “positive evidence of human foetal risk based on adverse reaction data from investigational or marketing experience or studies in humans”. However, this rating was based on non-peer-reviewed and unpublished data released by the manufacturer. Peer-reviewed analysis of this database revised the incidence of cardiac malformation in the study population downwards (Queisser-Luft et al., 2002), and subsequent meta-analyses of the possible teratogenic effects of paroxetine have yielded conflicting results (Bar-Oz et al., 2007; O’Brien et al., 2008; Wurst et al., 2010). Doubts about the safety of paroxetine have led to recommendations that its use be avoided in early pregnancy in favour of other antidepressants (Udechuku et al., 2011). Conversely, one small meta-analysis concluded fluoxetine was not associated with teratogenicity (Addis and Koren, 2000) and thus may represent a safer alternative. However, there are no published accounts of a meta-analysis that directly compares the teratogentic potential of common individual SSRIs that might indicate which are comparatively safer. Previous studies have reported the teratogenicity of SSRIs as a medication class (Rahimi and Abdollahi, 2006) or have examined aggregates of newer antidepressants agents (including reboxetine, venlafaxine, and bupropion) (Einarson and Einarson, 2005). These studies might be of limited value to patients and clinicians because the teratogenic potential of specific agents might differ from the aggregate result for SSRI or non-SSRI medications as a class. A meta-analysis of individual SSRI medications would provide a more accurate assessment of each drug’s safety and guide alternative treatment where the teratogenic risk of one agent is unacceptable.
Primary research examining the effects of individual agents has significant limitations that can be addressed through meta-analysis. Studies of individual drugs are likely to have limited statistical power because of the smaller number of subjects and the low population prevalence of congenital malformation. Pooled weighted estimates of effect size has the potential to reduce type I errors by increasing power to detect true effects and simultaneously reduce the risk of type II error by contextualizing chance findings. Furthermore, the commercial implications of adverse drug findings or negative studies of less interest to peer-reviewed journals may result in publication bias that can be addressed with quantitative meta-analytic measures.
Importantly, there are a range of methodological factors that potentially confound naturalistic studies of the association between antidepressants and congenital malformation. For example the use of historical data as a control or contemporaneous controls without corrections for potentially confounding variables, such as age, might lead to inaccuracy in estimates of teratogenic effect. Some studies have used patients taking antidepressants from other classes as a control group in order to avoid the confounding factors associated with depression (Wurst et al., 2010). However, this method might confound estimates of effect, because any independent teratogenic effect of other antidepressants could obscure the true estimate of the effect of SSRI medications.
We aimed to determine and compare the potential teratogenicity of each medication within the SSRI drug class using meta-analysis in order to provide clinically relevant information that may improve decision making by clinicians and pregnant women. Our a priori hypothesis was that SSRI medications (fluoxetine, paroxetine, sertraline, and citalopram) are individually associated with an increased risk of major, minor, and cardiac malformation in those infants exposed in utero.
Methods
The methods are based on guidelines for Meta-Analysis of Observational Studies in Epidemiology (MOOSE) (Stroup et al., 2000).
Searches
The systematic search of English-language publications indexed in five electronic databases (CINAHL, EMBASE, Medline, PsycINFO, and ISI Web of Science) is shown in Figure 1. After exclusion of duplicates, all studies were retrieved and examined in full text by NM and HN. The reference lists of review articles and publications included for meta-analysis were hand-searched to locate additional articles not identified by electronic search. Authors of articles that collected data on SSRI as a medication class were contacted with a request for agent-specific data.
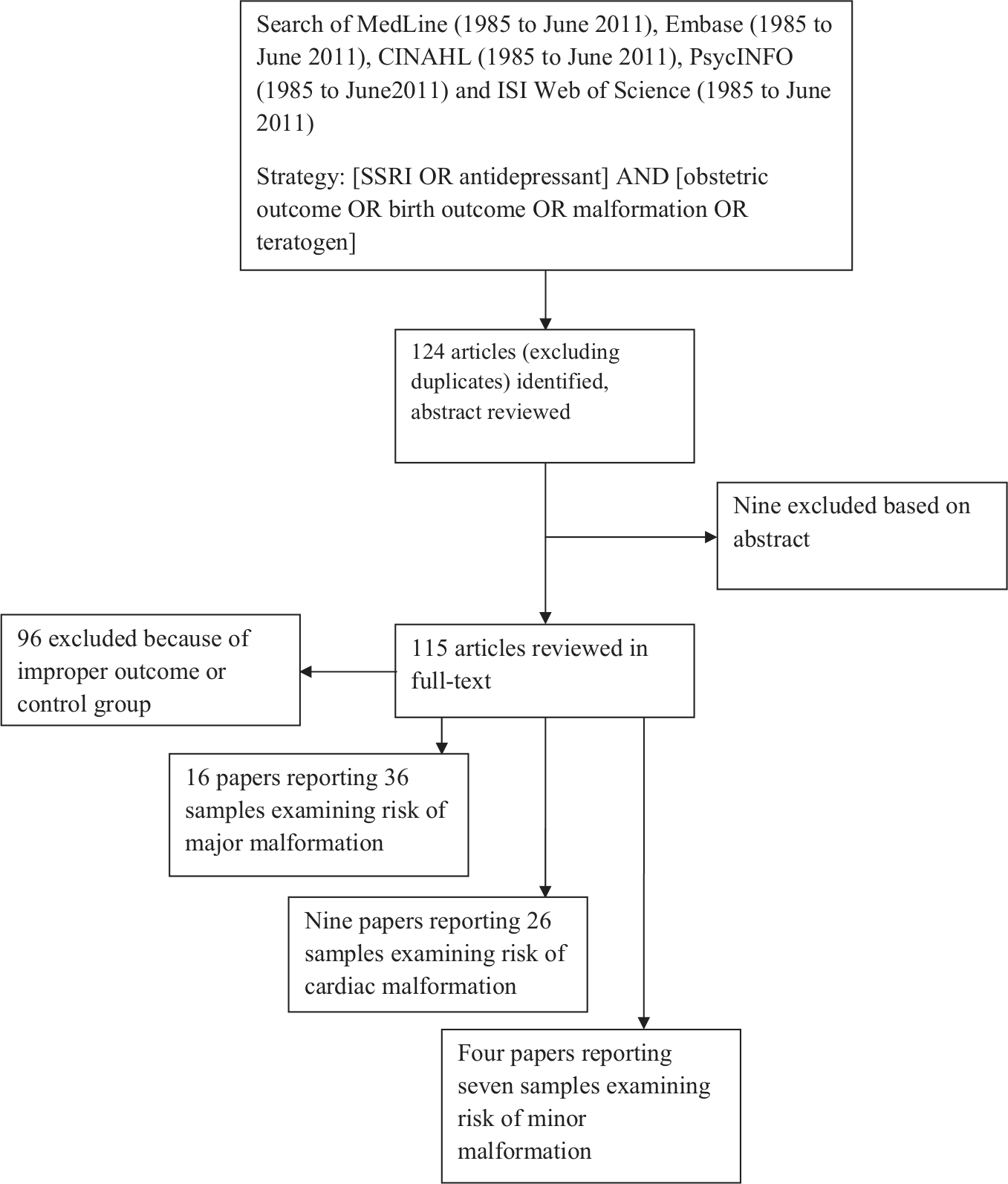
Flow chart of search strategy and results.
Studies were included if they reported: (i) on cohorts of pregnant women exposed to SSRI medications and a contemporaneously matched unexposed control group or on maternal exposure to SSRI in cohorts of those with and without foetal malformations; and (ii) raw data, odds ratio, risk ratio, difference in means, or any other analysable effect size comparing the incidence of major, minor, and/or cardiac malformation.
Studies were excluded if they reported: (i) a control group which was not contemporaneously matched or not derived from the same population of women as the exposed group; (ii) a control group exposed to any antidepressant medication; (iii) exposure as a combination of SSRI with other antidepressant classes; or (iv) exposure as a comparison of temporal variation.
Definition of SSRI exposure
Exposure was defined as exposure to any SSRI medication during the first trimester of pregnancy whether this occurred exclusively in the first trimester or continuously throughout pregnancy. Exposure was quantified differently across various studies. In larger retrospective cohort and case–control studies, exposure was defined by a surrogate marker, usually prescription registries linked to obstetrics records; in prospective cohorts, exposure was usually quantified by patient questionnaire or clinical assessment. Where possible exposure was classified as occurring early (exclusively in the first trimester) or continuously (throughout all trimesters of pregnancy). There was insufficient data to compare the effect of SSRI dosing.
Definition of teratogenic outcome
Major congenital malformation was defined in the primary research and in this study because any anatomical defect likely to have a significant impact on normal functioning present at birth. These diagnoses were usually defined by International Classification of Disease (ICD) codes at birth and broadly included neural tube defects, cleft palate, cardiac malformations, abdominal wall defects, and renal system malformation. A number of studies confirmed the diagnosis at one year of life to exclude spontaneous remission and disease of dubious clinical relevance. Antenatal ultrasonographic evidence of malformation or non-live birth malformation was not defined as a measure of effect in the primary research.
Minor congenital malformation was defined by ICD codes in the primary research. Studies usually defined a malformation as minor if it was clinically obvious but unlikely to interfere with normal function or require corrective surgery. The definition of minor malformation broadly included external auricular malformation, tongue-tie, hypospadias, accessory nipples, and congenital ptosis.
Cardiac malformation is a subtype of major malformation and was classified by ICD codes in many studies. Ventricular or atrial septal defects, vessel transposition, ventricular hypoplasia, outlet or valvular stenosis, aortic coarctation, and tetralogy of Fallot consisted the majority of diagnoses. The major difference in definition between studies was whether patent ductus arteriosus was included or excluded as an outcome.
There were some differences between studies in how some malformations were classified with respect to being minor or major but cardiac malformations, neural tube defects, cleft palate, abdominal wall, and renal malformations were invariably classified as major. However, there was no evidence that the definitions of malformations were applied differently to exposed and non-exposed groups within studies.
Data extraction
HN and NM extracted the data independently. There were three disagreements in effect size, resolved by joint examination of the papers. The following data were extracted:
the number of events in exposed and control groups for each outcome of interest or effect size data such as an odds ratio and 95% confidence interval or a risk ratio and 95% confidence interval
the sample size of exposed and control patients in each sample
the specific agent to which patients were exposed (paroxetine, fluoxetine, sertraline, citalopram); here, escitalopram was considered in analysis with citalopram because it is the S-stereoisomer of citalopram (Rosano et al., 2000)
the timing of exposure (early, continuous, or unspecified)
whether the study was a cohort study or a case–control study (quality measure)
whether samples controlled for maternal age as a confounder either through logistic regression or case matching (quality measure)
whether samples controlled for parity as a confounder either through logisitic regression or case matching (quality measure)
whether samples controlled for maternal use of alcohol, tobacco, or illicit drugs either through logistic regression or case matching (quality measure)
whether samples excluded neonates with known genetic abnormalities (quality measure)
whether samples declared pharmaceutical industry funding as a potential conflict of interest (measure of publication bias).
Meta-analysis of effect size and assessment of possible publication bias
Comprehensive Meta Analysis version 2 (CMA, Biostat Eaglewood, NJ) was used to convert raw data and effect size data reported in the primary research to odds ratios and to calculate pooled odds ratios for individual SSRI agents and SSRIs as a pharmaceutical class. Odds ratios were chosen as the effect size measure because they were used as the outcome measure in most of the included studies and because odds ratios have been shown to be the least biased and most statistically powered way of dealing with meta-analysis of low-frequency events (Bradburn et al., 2007). Odds ratios were also used as the outcome measure in an earlier meta-analysis of antidepressants and congenital malformations (Addis and Koren, 2000). Odds ratios are not affected by population prevalence of events and thus provide a suitable statistic for pooled estimates of cohort and case–control studies. We were able to convert the effect size data from every study into odds ratios; however, because case–control studies by definition do not allow for estimation of population prevalence we were unable to report a meta-analytic estimate of either the absolute risk or the number of patients needed to harm.
Between-study heterogeneity was assessed using the I2 statistic and between-group heterogeneity was assessed using Q-value statistics. A random-effects meta-analysis of independent groups was used on an a priori basis for all analyses because of between-study differences in the populations and study methodology. Random-effects meta-analysis requires only that thresholds are consistently applied within studies and allows for differences in the methods and studied populations, including differences such as the thresholds for inclusion in the exposure group and differences in the definitions of major, minor, and cardiac malformations.
An α-value ≤0.05 was considered statistically significant. We considered that the number of individual SSRI agents and the large number of possible malformations increases the possibility of type I error, so in an effort to address this we pooled different types of malformations and divided the analysis to congenital heart disease and the broader class of major malformation. With respect to SSRI agents, we elected not to use a Bonferroni correction for number of effect size calculations associated with individual SSRI exposure. We elected to do this to avoid adversely affecting power to detect a true effect, thereby reducing risk of type II error. Furthermore, there is no consensus as to when Bonferroni corrections should be used in meta-analysis, especially considering that multiple comparisons to a control group may occur in only some analysed studies, spuriously reducing the power of studies where only a single comparison was made and adversely affecting the overall significance of an aggregate effect.
Four different methods were used to consider publication bias, particularly because studies of low-frequency events are prone to chance findings when the absolute number of events is low and because of the possibility that pharmaceutical industry funding might have influenced publication. First, we inspected a funnel plot of effect size versus variance for the presence of smaller samples, which may have been published because they reported either a high or low rate of teratogenic outcome. Second Duval and Teedie’s trim and fill method (Sutton et al., 2000) was used to examine the possible effect of hypothetically missing samples on the pooled estimate of effect. Third, in the event of a significant result we planned to use the classic fail-safe N to determine the number of studies with an effect size of zero that would be required to return a p-value >0.05. Fourth, sensitivity analysis was undertaken to determine whether industry funding had any significant impact on effect size.
Subgroup and sensitivity analysis of quality studies
We assessed whether between-study heterogeneity in effect size was related to methodological differences and overall study quality by examining a range of factors, including whether or not:
the studies employed a cohort or case–control design, considering the latter is likely to be more highly powered
medication exposure occurred in the first trimester, considering that teratogenicity is only possible during early organogenesis
the studies controlled for maternal age, considering that children born to older women have an increased risk of congenital malformation
the studies controlled for parity
the studies controlled for tobacco, alcohol, or illicit drug use, considering these substances are associated with an increased risk of congenital malformation
single gene or chromosomal defects were excluded from analysis, considering these defects are usually intrinsic and unrelated to medication exposure.
Studies were awarded a score based on giving one point for each of the above quality criteria, such that a sample could score a maximum of six points. A sensitivity analysis of higher quality studies was performed excluding the studies with a quality rating of three or less.
Results
The number of papers yielded for the meta-analyses of major malformations, cardiac malformations and minor malformations is outlined in Figure 1 and are detailed in the Supplementary Appendix (available online).
Searches
Major malformation was reported the outcome in 16 papers reporting on 36 individual samples included in the meta-analysis. This dataset reported an exposed sample size of 23,919 (mean per sample ± SD 664±944) and control sample size of 2,585,550 (mean per sample 71,821±101,071). This data set included three samples derived from additional information provided by one author (Simon et al., 2002). Six authors were unable to provide additional information and the data derived from these samples (Kulin et al., 1998; Einarson et al., 2001a; Wen et al., 2006; Wogelius et al., 2006; Davis et al., 2007; Ramos et al., 2008) was included as an undifferentiated SSRI exposure group. One paper (Kallen and Otterblad Olausson, 2007) was excluded because it reported on a study which was the subject of another paper (Reis and Kallen, 2010); one paper (Einarson et al., 2001a) was excluded because it reported a combined sample which was the subject of two previous studies (Pastuszak et al., 1993; Kulin et al., 1998), and one paper (Malm et al., 2005) was excluded because it reported on a study with a subsequent update (Malm et al., 2011). Various other studies that examined SSRI impact on major malformation were excluded because some mothers in the control group were exposed to other antidepressant medications (Costei et al., 2002; Queisser-Luft et al., 2002; Cole et al., 2007), the exposure group was exposed to heterogeneous antidepressant classes (Chun-Fai-Chan et al., 2005; Maschi et al., 2008; Merlob et al., 2009), the reported effect was based on comparisons of early and late exposure (Berard et al., 2007), or the control group was not contemporaneous to the exposure group (Goldstein et al., 1997) (Figure 1).
Cardiac malformation was reported as the outcome in nine papers reporting on 26 individual samples included in the meta-analysis. This dataset reported an exposed samples size of 22,412 (mean per sample 862±1046) and control sample size of 2,404,278 (mean per sample 92,472±109,121). One contacted author was unable to provide additional data and this sample (Wichman et al., 2009) was included as an undifferentiated SSRI exposure group. Two papers (Kallen and Otterblad Olausson, 2003; Kallen and Otterblad Olausson, 2007) were excluded because they reported on a study which was the subject of another more recent paper (Reis and Kallen, 2010). Some potential samples which examined risk of cardiac malformation following SSRI exposure were excluded because they only reported some types of malformation (Merlob et al., 2009), included controls exposed to other antidepressant classes (Cole et al., 2007), or the reported effect was based on comparisons of early and late exposure (Berard et al., 2007).
Minor malformation was the outcome reported in four papers reporting seven individual samples included in the meta-analysis. This dataset reported an exposed sample size of 2631 (mean per sample 374±288) and control sample size of 497,307 (mean per sample 71,058±65,143). No unpublished data was collected and two papers (Wen et al., 2006; Pedersen et al., 2009) reporting SSRI exposure not differentiated by agent were included as independent samples.
Major malformation
A forest plot of the meta-analysis of major malformation is shown in Supplementary Figure 1. We found that SSRI as a medication class are significantly associated with increased risk of major malformation in children exposed in utero (OR 1.10, 95% CI 1.03–1.16, z=3.07, p=0.002). There was no heterogeneity (Q=31.0, p=0.66, I2=0).
Subgroup analysis of individual agents indicates paroxetine (eight samples, z=3.4, p=0.001) and fluoxetine (nine samples, z=2.0, p=0.04) were significantly associated with increased odds of major malformation, whilst citalopram (seven samples, z=0.6, p=0.55) and sertraline (six samples, z=0.1, p=0.88) were not (Q=7.05, df(Q)=3, p=0.07) (Table 1).
Subgroup analysis of methodological and confounding considerations in meta-analysis of major malformations.
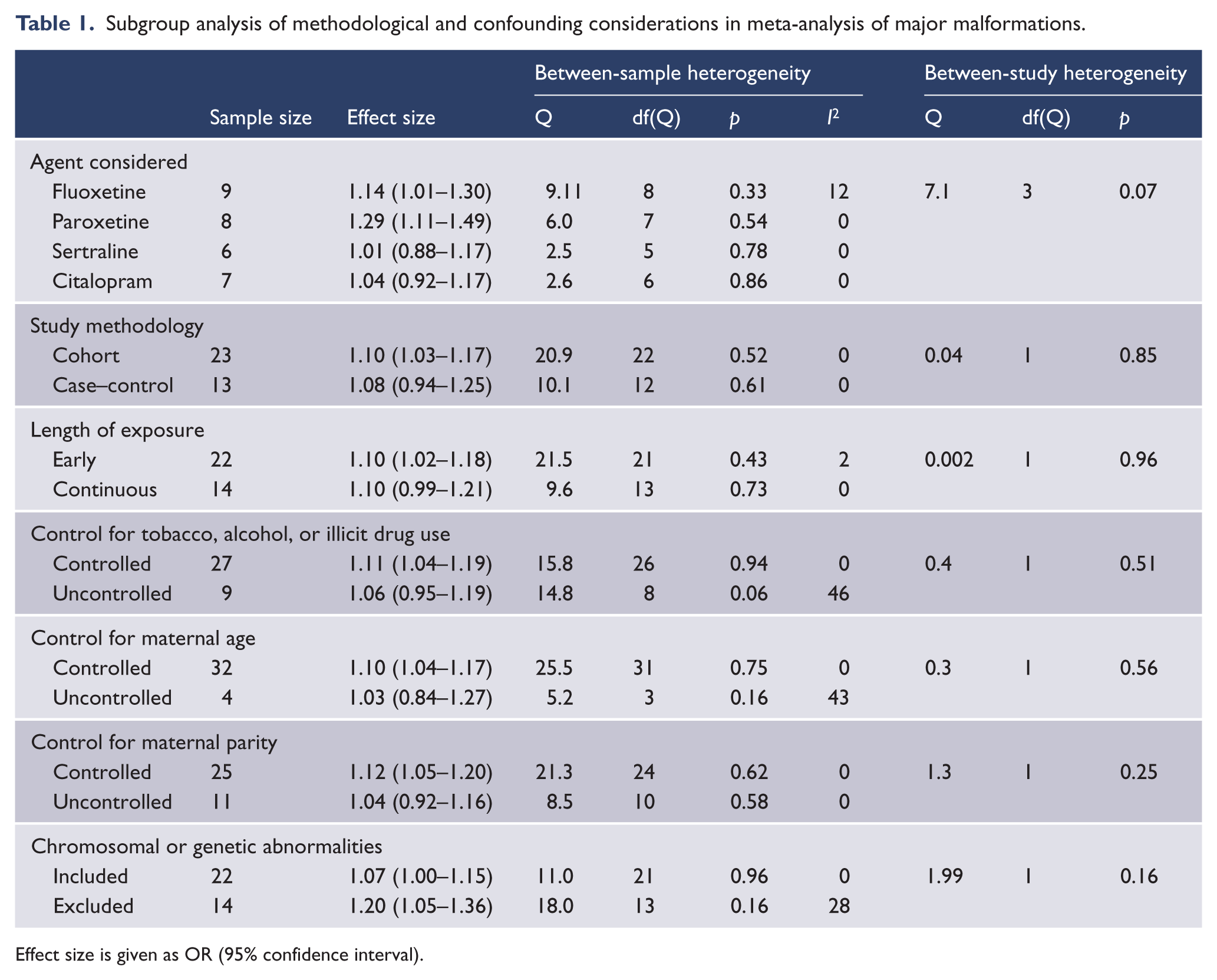
Effect size is given as OR (95% confidence interval).
Subgroup analysis of study methodology, quality, and potential confounders indicated these had no significant impact on effect size (Table 1). When restricted to quality samples only, the effect size for paroxetine (four samples, z=2.8, p=0.005) and fluoxetine (five samples, z=2.1, p=0.04) remained significant and was altered by a magnitude of +8.5% and +7% respectively (Table 2).
Sensitivity analysis of paroxetine and fluoxetine in meta-analysis of major malformations.
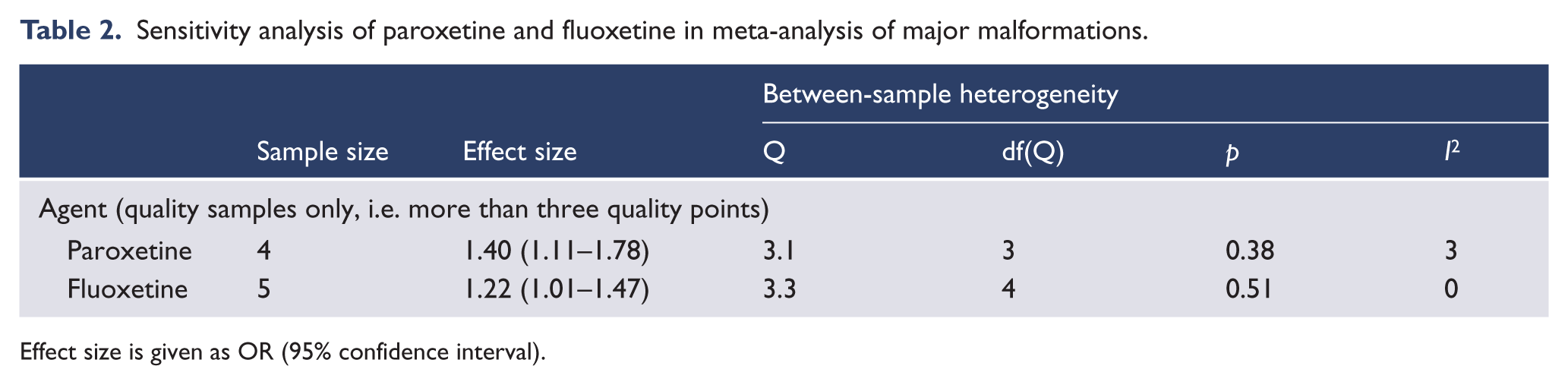
Effect size is given as OR (95% confidence interval).
The funnel plot examining fluoxetine was symmetrical. Trim and fill analysis was unable to demonstrate any hypothetically missing samples. The fail-safe N indicated that two samples with an effect size of zero would be required to return a non-significant effect size.
The funnel plot examining paroxetine was skewed towards the right, indicating publication bias towards reporting a larger effect size. Trim and fill analysis identified one missing study to the left of the mean, that if filled would return an adjusted odds ratio of 1.25 (95% CI 1.07–1.47, Q=9.4). The fail safe N indicated that 18 samples with an effect size of zero would be required to return a non-significant effect size. There were insufficient samples to determine whether industry funding impacted on heterogeneity of effect size.
Cardiac malformation
A forest plot of the meta-analysis of cardiac malformation is shown in Supplementary Figure 2. We found that SSRI as a medication class are not significantly associated with an increased risk of cardiac malformation in infants exposed in utero (OR 1.15, 95% CI 0.999−1.32, z=1.94, p=0.052). Heterogeneity was moderate (I2=34).
Subgroup analysis of individual agents indicated that paroxetine was significantly associated with increased odds of cardiac malformation (eight samples, z=2.8, p=0.005), whilst citalopram (six samples, z=0.2, p=0.81), fluoxetine (six samples, z=1.8, p=0.07), and sertraline (five samples, z=−0.5, p=0.61) were not (Q=6.4, df(Q)=3, p=0.09) (Table 2).
Subgroup analysis of study methodology, quality, and potential confounders indicated that these had no significant impact on effect size (Table 3). When restricted to quality samples only the effect size for paroxetine (five samples, z=2.4, p=0.02) remained significant and was altered by a magnitude of −2.1% (Table 4).
Subgroup analysis of methodological and confounding considerations in meta-analysis of cardiac malformations.
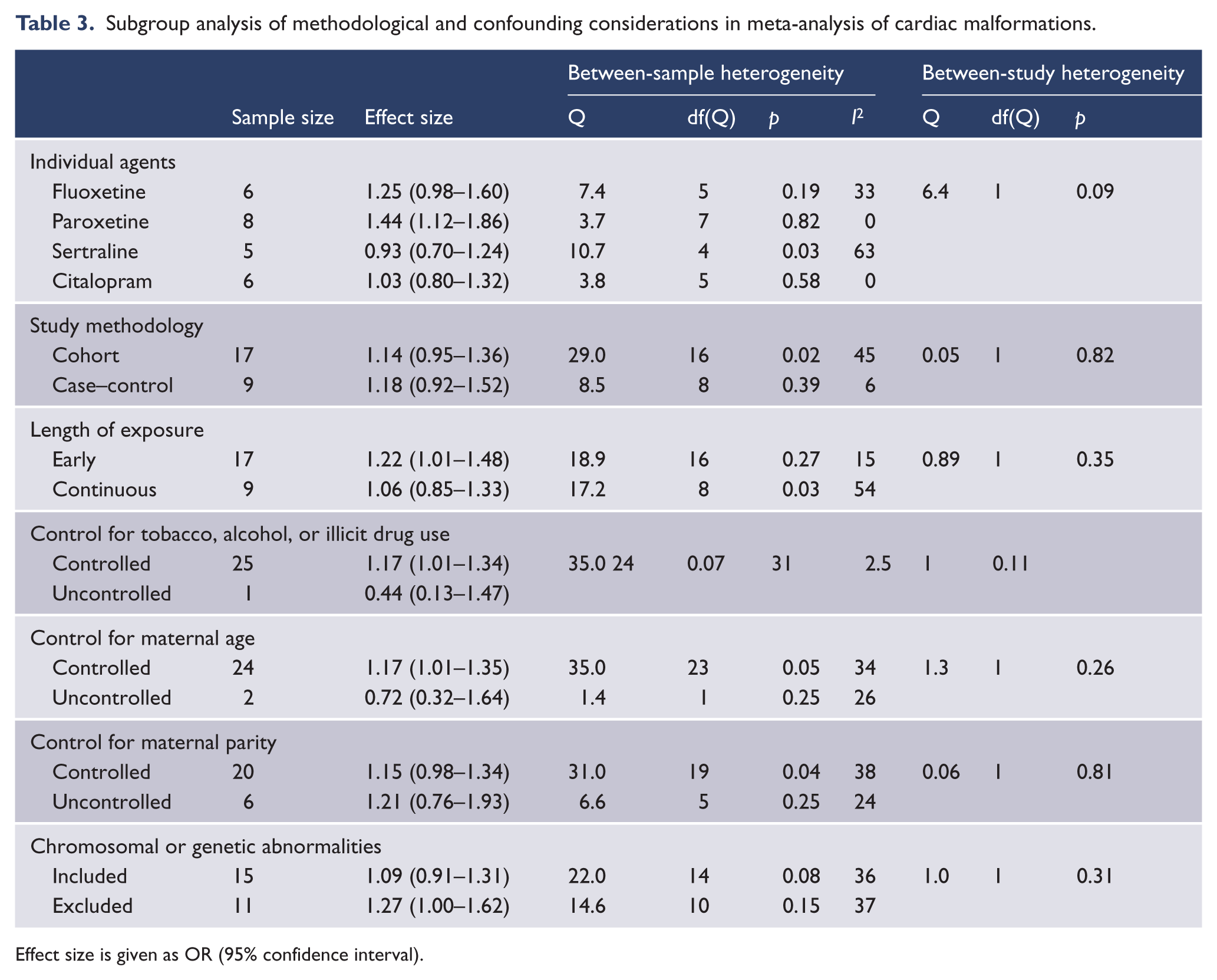
Effect size is given as OR (95% confidence interval).
Sensitivity analysis and publication bias for paroxetine in meta-analysis of cardiac malformation.
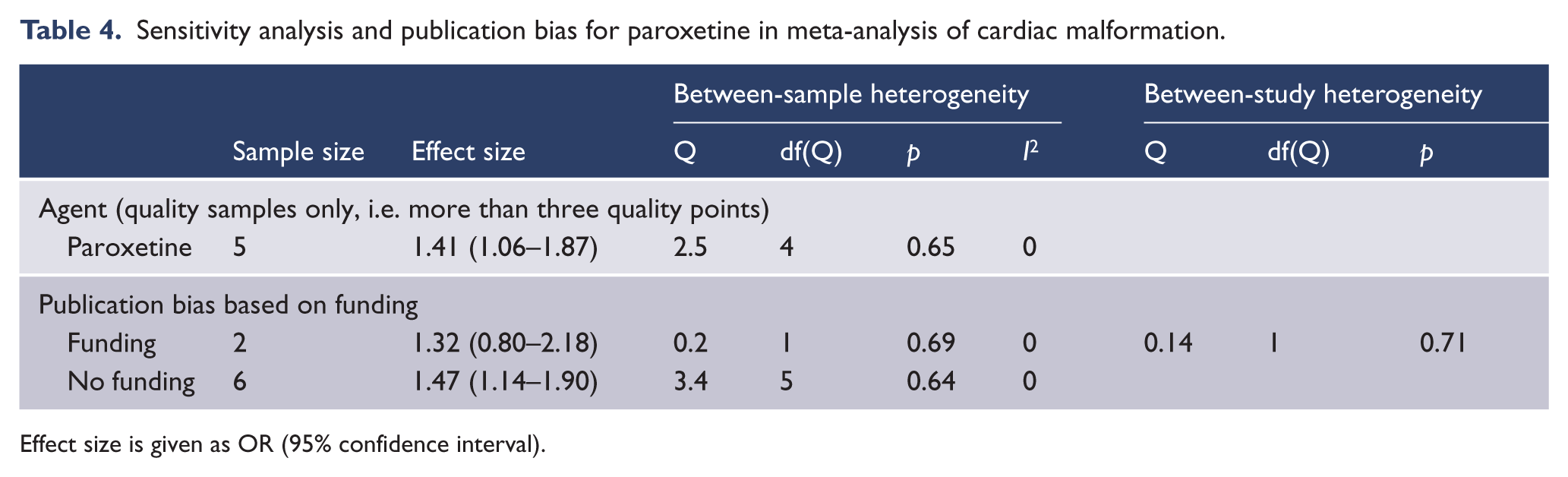
Effect size is given as OR (95% confidence interval).
The funnel plot for paroxetine was symmetrical. Trim and fill analysis was unable to demonstrate any hypothetically missing samples. The classic fail safe N indicated that 10 studies with an effect size of zero would be required to return a non-significant effect size. Subgroup analysis of studies that reported funding bias was not significant (Table 4).
Minor malformation
A forest plot of the meta-analysis of minor malformation is shown in Supplementary Figure 3. We found that SSRI as a medication class are not significantly associated with an increased risk of minor malformation in infants exposed in utero (OR 1.16, 95% CI 0.79–1.71, z=0.75, p=0.45). Heterogeneity was moderate (I2=45).
There were insufficient samples for meaningful subgroup analysis of individual agents, methodological considerations, or potentially confounding variables.
The funnel plot was asymmetrical. Trim and fill analysis identified two asymmetrical studies to the left of mean which if trimmed would result in a greater, though non-significant effect size (OR 1.30, 95% CI 0.91–1.85). Subgroup analysis of funding bias was unable to be performed because no study reported industry funding.
Discussion
This meta-analysis suggests that children exposed in utero to SSRI medications have increased odds of developing major congenital malformations, although not cardiac or minor congenital malformations. Subgroup analysis suggests that the aggregate effect for major malformation is driven specifically by paroxetine (OR 1.29, p=0.001) and fluoxetine (OR 1.14, p=0.04), with citalopram and sertraline exerting a non-significant impact on effect size. Consistent with previous meta-analyses, we demonstrated increased odds of cardiac malformation in infants exposed to paroxetine (OR 1.4, p=<0.01), an effect size larger than previously reported (Bar-Oz et al., 2007; Wurst et al., 2010). This meta-analysis is the first to suggest that fluoxetine is associated with foetal malformation.
Primary research into the teratogenic potential of antidepressants inherently suffer significant methodological limitations including retrospective data collection, incomplete data regarding timing of the exposure and degree of medication adherence, and difficulties separating the adverse effects of medication from the those associated with depressive illness or related comorbidity (Gentile, 2011). Methodological limitations have led some authors to conclude that positive associations between SSRI exposure and congenital malformations might be a result of poor study quality (Tuccori et al., 2010) or covariation between antidepressant use and lifestyle or other factors that may be causative of birth defects (Gentile, 2011). However, there is no evidence to suggest that confounding methodological factors are more likely to affect patients prescribed paroxetine or fluoxetine while sparing patients prescribed sertraline or citalopram. Hence, this study supports the notion that some SSRIs have small but measurable teratogenic potential. Furthermore, an analysis of individual SSRI agents is more clinically relevant than previously published aggregate estimates because patients are usually only exposed to a single agent. While the possibility still exists that the apparent association between SSRI and congenital malformation is not causal, and even though it should be acknowledged that the risk of foetal malformation is not greatly elevated by any SSRI, the current evidence is that the already low risk of foetal malformation associated with fluoxetine and paroxetine is lower still, or non existent, with sertraline and citalopram.
There are, however, a variety of limitations inherent in the primary literature and our analysis that should be addressed. Whilst we were able to accurately estimate an increased risk of major malformation, this non-specific and diverse outcome may obscure the extent to which one or more specific subtypes drove an apparent increase in aggregated congenital defects. It is possible that increased odds of cardiac malformation may explain a large proportion of paroxetine’s effect on major malformation and that paroxetine is not associated with non-cardiac malformations. The low population prevalence of particular congenital malformations including the various subtypes of cardiac malformation inherently reduces the statistical precision of any primary investigation and therefore the data available for meta-analysis. An increased odds of craniosynystosis, omphalocele, and anencephaly were noted in one powered case–control study of exposure to SSRI medications (Alwan et al., 2007); however, these associations were not replicated in another study of similar design (Louik et al., 2007). Also neither study reported an association with ventricular or atrial septal defects, which is the predominant subtype reported extensively in other literature (Wogelius et al., 2006; Cole et al., 2007; Diav-Citrin et al., 2008).
Primary research into the possible teratogenic effects of SSRIs is naturalistic and are not driven by an experimental hypothesis about the association between particular medications or particular malformations. Hence, by design these studies are prone to type I error and chance reporting of specific associations. Nevertheless the low between-study heterogeneity, non-significant subgroup analysis of methodological considerations, and lack of evidence for publication bias suggest that the pooled estimates of effect size are statistically robust and broadly applicable to clinical practice.
Our analysis was also limited by the small number of samples that made it impossible to undertake subgroup analysis within groups of specific SSRI agents, including whether earlier exposure to fluoxetine or paroxetine was associated with an increased odds of malformation when compared to later exposure. As the reporting of individual SSRI agents is prone to the same methodological differences and potential publication bias of SSRI medications as a class, it would have been advantageous to replicate our subgroup analysis at the level of individual agents. Recent recommendations (Gentile, 2011) for future research indicate an urgent need to differentiate the adverse effects of depression from iatrogenic outcomes and suggest that large prospective studies of patients with heterogeneous psychiatric diagnoses are urgently needed. In addition we would also recommend future research be directed towards individual agents rather than SSRIs as a class. It is also prudent that individual or specific malformations be examined due to the effect that an aggregate estimate of major, minor, or cardiac malformation may have on confounding these specific outcomes.
Regardless of these limitations, existing research appears to implicate fluoxetine and paroxetine. This suggests that neither paroxetine nor fluoxetine should be used electively as first line antidepressant therapy in those wishing to become pregnant or in the first trimester of pregnancy when sertraline or citalopram might equally be prescribed. An argument might also be made for avoiding these medications where accidental pregnancy is likely. Some consideration ought also be given to whether fluoxetine should be placed with paroxetine as category D medication in pregnancy. Such a recommendation would have little overall impact on the treatment of depression in this demographic group because citalopram and sertraline have comparable therapeutic effect in major depressive illness (Pradat et al., 2003).
When prescribing any medication with teratogenic potential, there is an inherent risk trade-off that must be considered. Gestational depression and anxiety is associated with increased rates of postnatal depression (Lee and Chung, 2007), poor infant attachment, and long-term developmental outcomes (Murray and Cooper, 1997); decreased use of antenatal care (Bonari et al., 2004); and increased rates of alcohol, tobacco, and illicit drug use which in themselves may increase teratogenic risk. In those women with mild illness manifesting during pregnancy, use of psychological therapies such as cognitive behavioural therapy are as effective as drug treatment. The effectiveness of psychological therapies and SSRI medication is well validated (Dimidjian et al., 2006) and the former is likely to have comparable clinical efficacy whilst avoiding the risk of teratogenicity.
Unfortunately, depressed women are less likely to seek pre-pregnancy counselling (Bonari et al., 2004) and as a consequence are less likely to receive advice on medication switching prior to conception. In this circumstance, the small increased risk of foetal malformation associated with paroxetine or fluoxetine probably does not justify a change in antidepressant. Medication switching at this stage is unlikely to avoid critical first-trimester exposure, may put the woman at risk of illness relapse, and could potentially induce foetal withdrawal, which has been associated with premature delivery, stillbirth, and low birthweight (Cohen et al., 2006). Fluoxetine and paroxetine can also be considered for treatment in illness refractory to other agents. Currently, there is insufficient evidence to recommend preferential use of newer antidepressant classes due to a paucity of literature examining individual agents sufficiently powered to detect significant effects (Einarson et al., 2001a, 2003; Chun-Fai-Chan et al., 2005; Djulus et al., 2006; Ramos et al., 2008; Wichman et al., 2009; Wisner et al., 2009).
Conclusions
Paroxetine and fluoxetine are associated with a small but significantly increased risk of major malformation, and paroxetine in particular is associated with cardiac malformation. The alternative first-line SSRI medications sertraline or citalopram should be considered as first-line SSRI treatments in pregnancy and women of childbearing age.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of interest
Dr Large has received speakers fees from AstraZeneca. Drs Myles, Newall and Ward report no potential conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.