
Abstract
Objective:
This study aims to determine whether symptoms of post-traumatic stress disorder (PTSD) form a latent dimension reflecting responsivity to life events and whether PTSD symptoms are specific to traumatic life events.
Method:
A 30-year longitudinal study of a general population sample of 987 individuals were assessed for PTSD symptoms, exposure to adverse life events, and a variety of psychosocial measures. PTSD symptoms were tested using a confirmatory factor model and a range of fitted models were used to identify significant predictors of latent PTSD symptoms.
Results:
The rate of DSM IV PTSD was 1.9%. However, subjects reported high rates of at least one significant traumatic or negative life event and PTSD symptoms. The PTSD symptoms conformed well to a single latent factor. There were strong linear associations between severity of PTSD symptoms and exposure to traumatic and non-traumatic life events. Factors contributing to latent PTSD symptoms were gender, childhood anxiety, neuroticism, self-esteem, and quality of parental care.
Conclusion:
Criteria for PTSD form an underlying dimension reflecting the individual’s level of responsivity to traumatic and non-traumatic stressful life events. PTSD symptoms form a continuum of severity with minor stress symptoms at one end and severe PTSD at the other.
Introduction
Post-traumatic stress disorder (PTSD) links a specific symptom configuration with a distinct class of stressors. The validity of the diagnosis has been repeatedly questioned since PTSD was introduced in DSM III in 1980 (Breslau and Davis, 1987; Davidson and Foa, 1991; Rosen and Lilienfeld, 2008). There are three major areas of concern. First is whether PTSD is a coherent diagnosis (i.e. a distinctive combination of symptoms) or a re-conceptualization of depressive and anxiety symptoms which commonly occur after a stressful life event. Related to this problem is whether PTSD is better conceptualized as the extreme of a continuum of responsivity to stressful events rather than a distinct category (Rosen and Lilienfeld, 2008).
Second, PTSD requires an individual to experience a traumatic event which involves intense fear, helplessness, or horror (criterion A) for the diagnosis to be made. However, studies which have assessed PTSD symptoms after non-traumatic life events have consistently reported that there is no evidence that traumatic life events are more likely to produce PTSD symptoms than non-traumatic negative life events (Mol et al., 2005; Bodkin et al., 2007).
Third, the diagnosis of PTSD assumes that the traumatic event is the major cause of psychological symptoms, implying that individual differences on the responsiveness to trauma are obliterated by the overwhelming impact of the trauma (Breslau and Davis, 1987). Again there is modest evidence that antecedent personal characteristics and life circumstances do exert a significant influence on responses to trauma (Rosen and Lilienfeld, 2008).
Most studies on PTSD have difficulty in addressing these concerns. This is mainly caused by the populations that have been studied. Since the diagnosis of PTSD requires exposure to a traumatic event, PTSD symptoms are not explored unless such an event has occurred. Most studies therefore focus on individuals who have been exposed to a traumatic event or who were in situations, such as war zones or natural disasters, where they were likely to have been exposed.
This paper uses data gathered over a 30-year longitudinal study of a general population sample. We examine the validity of the PTSD diagnosis using structural modelling methods to determine whether PTSD symptoms form an internally consistent distinct latent dimension. By not requiring criterion A and including non-traumatic but still negative life events, we are able to test whether PTSD symptoms are specific to traumatic events. By examining non-life event risk factors such as gender, personality, and family circumstances collected over the 30 years, we are able to study the role of individual vulnerability factors in creating PTSD symptoms.
Methods
Data were gathered as part of the Christchurch Health and Development Study (CHDS). The CHDS is a longitudinal study of a birth cohort of 1265 children born in the Christchurch (Royal Australian and New Zealand College of Psychiatrists Clinical Practice Guidelines Team for Depression, 2004) region in 1977. They have been studied on 22 occasions from birth to age 30 years. At age 30 (in 2007, prior to the Christchurch earthquakes), a total of 987 cohort members were assessed, representing 80% of the surviving cohort. Throughout the study, data have been collected from a variety of sources including parental interview, teacher report, psychometric testing, interviews with cohort members, medical, and other official record data. The study has ethical approval from relevant ethics committees (Fergusson and Horwood, 2001).
Assessment of PTSD symptoms
Participants were interviewed on a comprehensive interview schedule designed to assess aspects of mental health and psychosocial adjustment over the 5-year period since their previous assessment at age 25 including DSM-IV (American Psychiatric Association, 1990) symptom criteria for PTSD. Participants were questioned about their lifetime experience of a range of adverse life events up to age 30 including traumatic or life-threatening experiences which would normally be considered as criterion A in DSM-IV PTSD, as well as other significant serious or chronic life events. A more detailed description of these events is given below. The questions used to assess life event exposure are given in Appendix 1 (available online).
Those who reported experiencing at least one life event before age 30 were questioned about PTSD-related symptoms in the previous 5 years using the diagnostic interview schedule (DIS) (Robins et al., 1995) items for PTSD. Responses to the 17 primary symptoms under criteria B−D were coded on a 3-point scale (1, doesn’t apply; 2, applies somewhat; 3, definitely applies). Duration of symptoms (criterion E) was assessed on a 3-point scale (1, no; 2, yes perhaps; 3, yes definitely). Extent of impairment (criterion F) was also assessed on a 3-point scale (1, not at all; 2, a little; 3, a lot).
Exposure to adverse life events
Two measures were constructed to reflect the extent or severity of exposure to adverse or traumatic life events.
Exposure to traumatic/life-threatening life events
A measure of exposure to traumatic life experiences was based on a count of the number of potentially traumatic or life-threatening experiences reported by the participant up to age 30. These included such things as: a serious or life-threatening accident; being robbed or threatened with a weapon; sexual or physical abuse as a child or as an adult; being caught up in a fire, a war, or a natural disaster; the murder or suicide of a close friend or family member; witnessing the death of someone or accidentally causing the death of another person; and other similar traumatic/life-threatening events nominated by the participant that were not included in the original list.
Other significant life events
A measure of exposure to non-traumatic adverse life experience was constructed based on a count of the number of other significant, serious, or chronic life events reported by the participant. These included such things as: being burgled or robbed (without physical confrontation); a major relationship break-up; major financial problem and serious problems at work or with employment; having a serious or chronic (non-life-threatening) illness; serious problems with studies or education; and other similar or related events nominated by the participant.
Other predictors of PTSD symptoms
To examine other factors that predicted PTSD symptoms, the following measures were taken in addition to gender.
Cognitive ability (8−9 years)
Child cognitive ability was assessed when participants were aged 8 and 9 years using the revised Wechsler Intelligence Scale for Children (WISC-R) (Wechsler, 1974). The reliability of the child’s total IQ score, assessed using split half methods, was 0.93 at age 8 and 0.95 at age 9. The measure used in the present analysis was the average of the child’s total IQ score over the two assessments.
Child anxiety/withdrawal (7−9 years)
At ages 7, 8, and 9, parent and teacher reports of child behaviour problems were obtained using questionnaires that combined items from the Rutter and Connors parent or teacher scales (Conners, 1969; Rutter et al., 1970). Confirmatory factor analysis identified a series of items from these scales that appeared to conform to a unidimensional scale reflecting the extent to which the child exhibited, shy, anxious, or withdrawn behaviours at each age (Fergusson and Horwood, 1993).
Child neuroticism (14 years)
At age 14, sample members were administered a short form version of the neuroticism scale of the Eysenck Personality Inventory (Eysenck and Eysenck, 1964). This α reliability of this scale was 0.80.
Self esteem (15 years)
At age 15, sample members were assessed on the Coopersmith Self Esteem Inventory (Coopersmith, 1981). The α reliability of the total self esteem score used in the present analysis was 0.87.
Family living standards (0−10 years)
These were assessed by averaging interviewer ratings obtained at annual intervals from when sample member was aged 1−10 years. Ratings were made on a 5-point scale from “obviously affluent” to “very poor”. For the purposes of the present analysis, interviewer ratings were averaged over the 10-year period to provide a measure of the family’s average standard of living during childhood. This measure was scaled such that a higher score implied higher living standards.
Changes of parents (0−15 years)
Changes of parents included changes resulting from parental separation/divorce, remarriage, reconciliation, parental death, fostering, and other changes of custodial parent.
Parental bonding (16 years)
At age 16, participants were asked to complete the parental bonding instrument (PBI) (Parker et al., 1979), The PBI has two subscales: the parental care scale describes the extent of caring and nurturant parenting; whereas the parental overprotection scale describes the extent of restrictive and over protective parenting. Separate assessments were obtained for the child’s mother and father. The α reliabilities of these scales ranged from 0.85 to 0.91. For the purposes of the present analysis, the maternal and paternal scores on each scale were averaged to provide two measures reflecting the participant’s report of the overall quality of parental care and the extent of parental overprotection during childhood.
Sample size and sample bias
The analysis is based on 929 (out of the 987) participants who reported experiencing at least one significant life event prior to age 30. Compared with other surviving cohort members, there was a trend (p<0.01) for the sample to under-represent individuals from more socially disadvantaged backgrounds (low SES, low parental education, single-parent family). In addition, there were small amounts of missing data on some of the predictors. These observations raise the issue of the extent to which sample selection bias due to sample attrition and missing data may have influenced the results reported here. This issue is discussed further under statistical analysis.
Statistical analysis
A confirmatory factor model was used to test the dimensionality of PTSD symptom reports. A single factor model was fitted to the variance−covariance matrix of the PTSD symptom measures using Mplus (Muthen and Muthen, 2007) and methods of weighted least squares estimation that were robust to departures from multivariate normality of the observed data. Goodness of fit was assessed on the basis of the model chi-square statistic, the root mean squared error of approximation (RMSEA), and the comparative fit index (CFI). In well-fitting models, the RMSEA should be <0.05, while the CFI should be close to 1 (Joreskog and Sorbom, 1993). From the fitted model, factor score estimates were obtained to estimate the individual’s score on the underlying latent dimension of PTSD symptoms. The associations between the latent PTSD symptom score and measures of life events were tested for significance using one-way analysis of variance tests for linear trend.
The model was then extended to incorporate predictors of latent PTSD symptoms within a structural equation modelling framework. A range of models was fitted to identify a core set of significant predictors on latent PTSD symptoms. In each case, models were fitted to a pairwise deleted variance−covariance matrix of the observed PTSD indicators and predictor variable(s) under the assumption that the data were missing at random. Further supplementary analyses were conducted using either data weighting or missing data imputation methods (Little and Rubin, 1987) to correct for possible sample selection bias. These analyses produced estimates of model parameters and conclusions that were essentially the same as those reported here, suggesting that sample selection bias was unlikely to have influenced the study findings.
Results
Extent of PTSD symptomatology
Of the general population sample of 987 individuals, 929 (94.1%) reported experiencing at least one significant life event before the age of 30. Table 1 summarizes the frequency of primary DSM-IV PTSD symptoms over the 5-year period. Individual symptom prevalences ranged from 4 to 40% for any reported experience and from 2 to 20% for definite symptoms. Overall, 51% of the sample reported at least one criterion B symptom, 45% at least one criterion C symptom, and 50% at least one criterion D symptom. Only 38% reported experiencing no PTSD symptoms in the past 5 years. One in four participants reported that they had probably or definitely experienced some of these symptoms for a month or longer; 33% reported some degree of impairment of functioning, with 13% reporting considerable impairment. Analysis using DSM IV criteria revealed that the prevalence of PTSD was 1.9%. Allowing non-traumatic negative life events as criteria raised the prevalence rate to 3.4%.
Reported frequency of DSM-IV PTSD symptoms age 25−30 years (n=929).
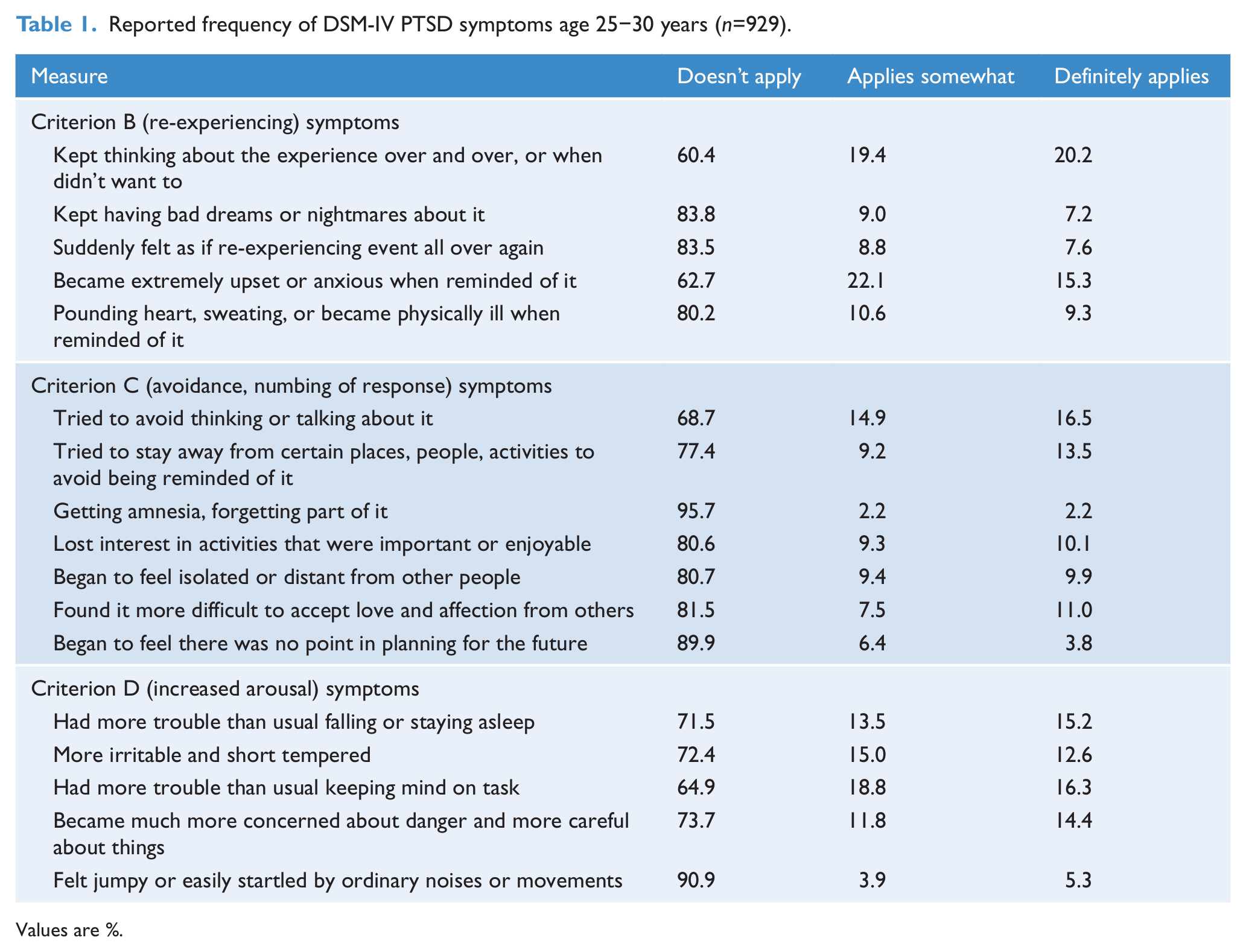
Values are %.
Do PTSD symptoms form a distinct syndrome?
To examine whether the PTSD symptom reports reflected an underlying unidimensional scale, the symptom reports in Table 1 were subject to confirmatory factor analysis (CFA). To simplify the analysis the 17 primary symptom criteria were first reduced to three scale measures by separately summing the symptom reports for the five criterion B symptoms, the seven criterion C symptoms, and the five criterion D symptoms to create scale measures reflecting the extent of re-experiencing symptoms, avoidance/numbing of responsiveness symptoms, and increased arousal symptoms, respectively.
Table 2 shows the matrix of correlations between the three scale measures of criteria B, C, and D symptom severity as well as the measures of criterion E (duration) and criterion F (impairment). There were strong and consistent correlations between all five measures, ranging from 0.52 to 0.73 (all correlations p<0.0001). A single factor model was fitted to the data in Table 2 in which the five measures were assumed to be indicators of an underlying latent construct reflecting the extent of PTSD symptomatology. The initial model showed a relatively poor fit to the data (χ2(5)=41.9, p<0.0001; RMSEA=0.09; CFI=0.90). However, examination of modification indices suggested that model fit could be improved by the addition of a correlation between the disturbances of the duration and impairment measures. With the inclusion of this additional parameter the resulting model had excellent fit (χ2(4)=2.06, p=0.72; RMSEA=0.00; CFI=1.00).
Matrix of correlations between measures of DSM-IV PTSD symptom criteria (n=929).
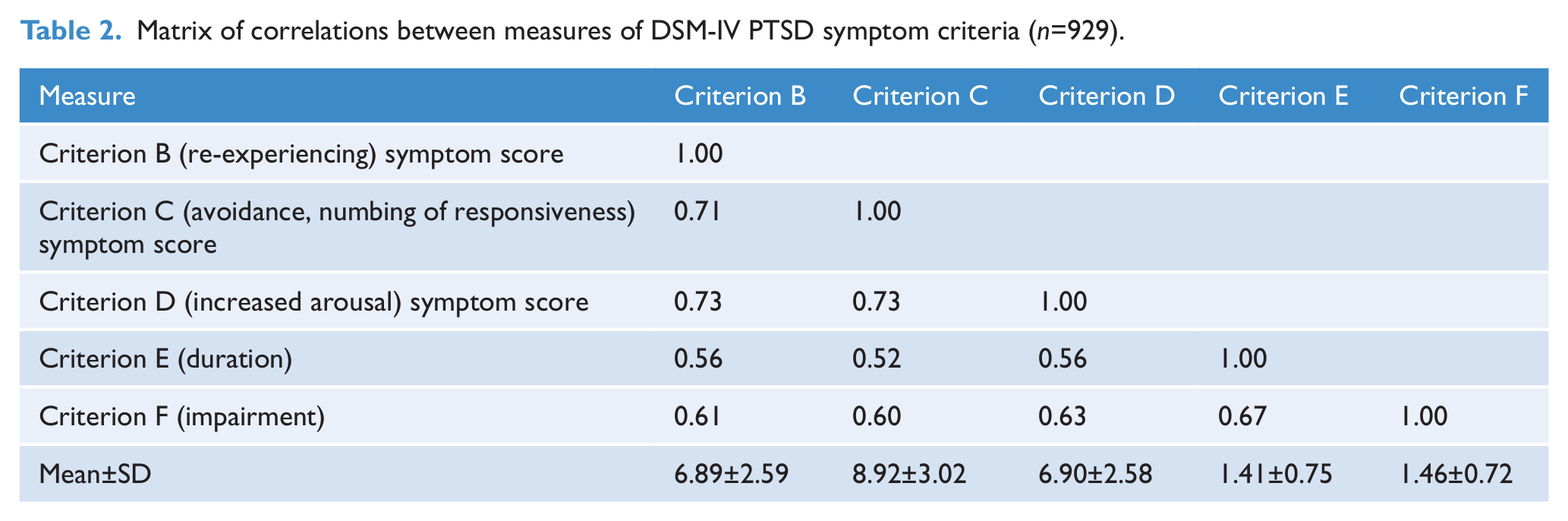
Figure 1 shows the standardized model parameters for the final fitted model, which ranged between 0.63 to 0.87, suggesting that the latent construct accounted for between 40 and 76% of the variance in the observed indicators. There was a correlation of 0.21 between the disturbance terms for symptom criteria E and F, reflecting the fact that increasing duration of symptoms was correlated with increasing impairment. Overall, the excellent model fit combined with the generally high factor loadings clearly suggested that observed data conformed well to a single latent factor.
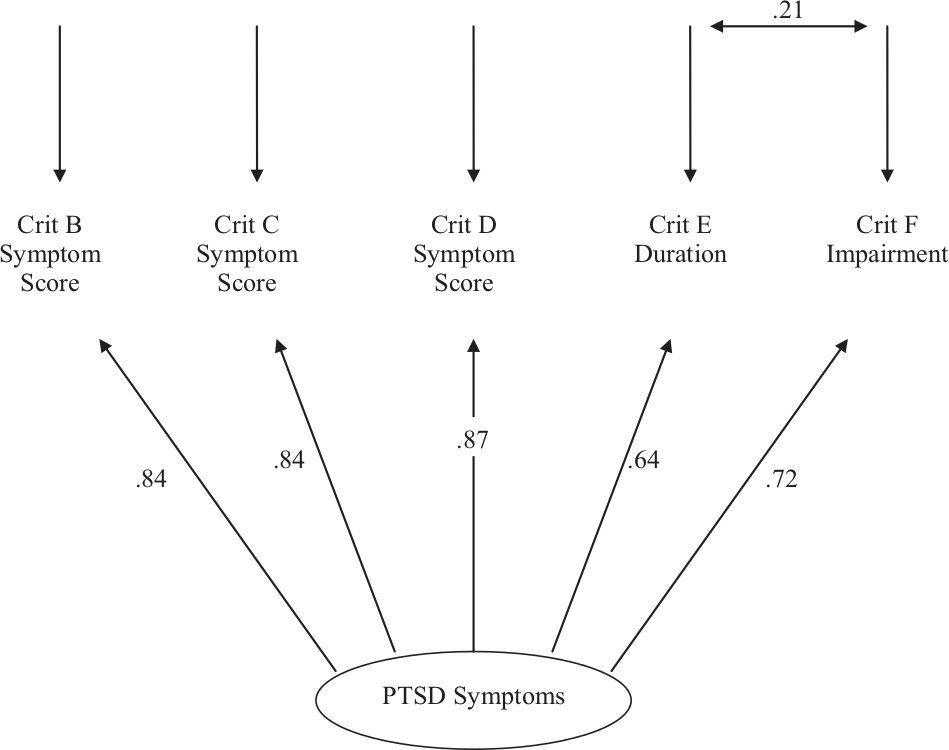
Fitted confirmatory factor model of latent PTSD symptoms (25−30 years) with standardized model coefficients.
Associations between reported traumatic and negative life events and latent PTSD symptoms
To illustrate the associations between life event reports and the severity of PTSD symptoms, the parameter estimates from the fitted model in Figure 1 were used to derive factor score estimates of the individual’s score on the underlying latent dimension of PTSD symptoms. The latent PTSD symptom score was scaled to have a mean of 100 and standard deviation of 10. Table 3 shows the associations between mean latent PTSD symptom scores and two measures of life event exposure: the number of traumatic/life-threatening life events and the number of other significant life events reported by the participants. Each association has been tested for significance using a one-way analysis of variance test for linear trend. The strength of association is summarized by the Pearson correlation between the number of life events and the latent PTSD factor.
Mean PTSD symptom score by number of traumatic/life-threatening events and other significant life events.
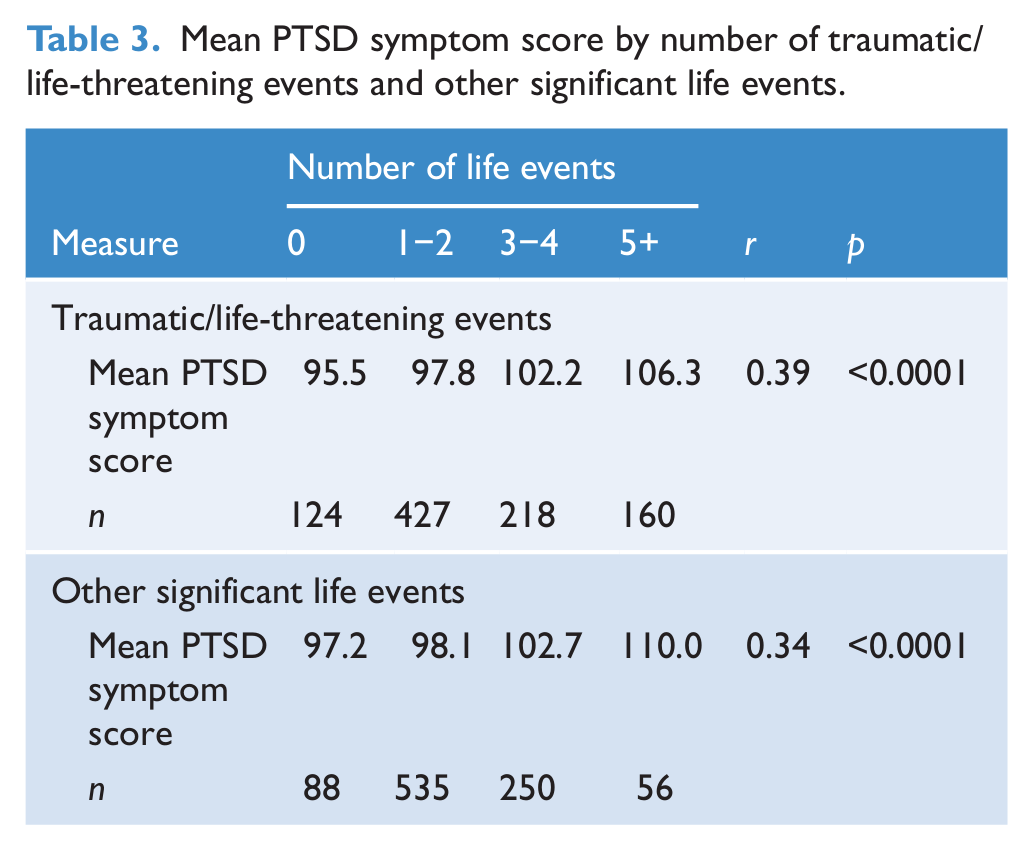
Table 3 shows that there were strong and highly significant (p<0.0001) linear associations between the severity of PTSD symptoms and the extent of exposure to both traumatic events and other negative significant life events. In each case, those who reported exposure to five or more life events had mean PTSD symptom scores that were more than one standard deviation higher than those who reported no significant life events. The correlations between life event reports and severity of PTSD symptoms ranged from 0.34 to 0.39 suggesting that, individually, the life event measures accounted for 12−15% of the variance in latent PTSD symptoms.
The relationship between non-life events and PTSD symptoms
The model in Figure 1 was extended to incorporate other potential predictors of latent PTSD symptoms in addition to the life event measures. These factors included measures of personal characteristics (gender, cognitive ability, childhood anxiety/withdrawal, neuroticism, and self esteem) and measures of childhood family circumstances (family living standards, changes of parents, parental care, and overprotection). A range of models was fitted to the data to identify a core set of significant predictors of underlying PTSD symptoms.
Table 4 shows the estimated Pearson correlation between each predictor and latent PTSD symptoms before adjustment for other factors and the standardized regression (β) coefficients for the significant (p<0.05) predictors of latent PTSD symptoms included in the final prediction model. The table also reports multiple correlation and goodness of fit indices for the final fitted model including only those factors that made significant contributions to the prediction of latent PTSD. At the bivariate level, latent PTSD symptoms were significantly (p<0.001) correlated with all measures of individual characteristics and family circumstances. When all factors were considered simultaneously as predictors, seven factors emerged as making significant net contributions to the prediction of latent PTSD symptoms. These were number of traumatic/life-threatening life events (p<0.0001), number of other significant life events (p<0.0001), gender (p<0.0001), childhood anxiety/withdrawal (p<0.05), neuroticism (p<0.05), self-esteem (p<0.05), and quality of parental care (p<0.05). Measures of significant life events remained the strongest predictors of PTSD symptoms when other factors were taken into account (β=0.23 to 0.28), with other factors having generally very modest effects (β=−0.09 to 0.16). The multiple correlation from the final fitted model was 0.53, suggesting that jointly the seven factors accounted for 28% of the variance in latent PTSD symptoms.
Estimated bivariate correlations between predictors and latent PTSD symptoms and standardized regression coefficients for significant predictors of latent PTSD symptoms from fitted regression model.
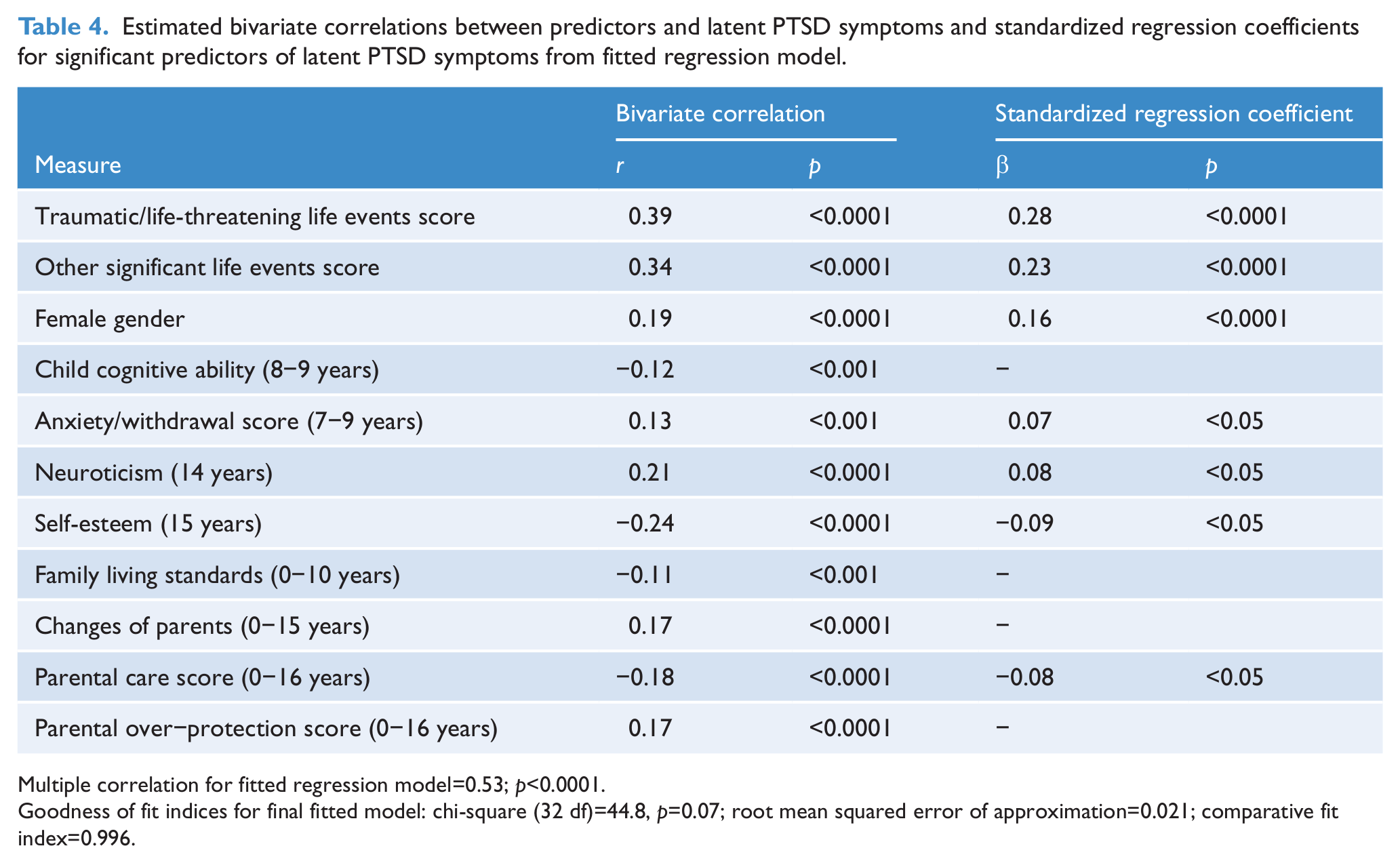
Multiple correlation for fitted regression model=0.53; p<0.0001.
Goodness of fit indices for final fitted model: chi-square (32 df)=44.8, p=0.07; root mean squared error of approximation=0.021; comparative fit index=0.996.
Discussion
The study has four major conclusions. Their implications are discussed below.
PTSD symptoms are common
First, the experience of PTSD symptoms in association with significant life events is common. Over 94% reported at least one significant life event before the age of 30 and of these over 60% reported experiencing PTSD symptomatology in the previous 5 years. The majority reported no or few PTSD symptoms and no impairment, but a small minority experienced severe prolonged symptoms and significant impairment. These findings are consistent with research using taxometric methods which report that PTSD symptoms fall as a continuum of severity with everyday symptoms of stress at one end and severe PTSD symptomatic criteria at the other (Meehl and Golden, 1982). The rates of PTSD as defined in DSM IV are 1.9% in this population.
PTSD symptoms form a distinct syndrome
Second, PTSD symptoms constitute a distinct factor. Confirmatory factor analysis when applied to a series of measures reflecting DSM-IV symptom criteria B−F showed that they conformed well to a single factor model. This suggests that underlying the observed symptom data is a stable unidimensional scale reflecting the severity of PTSD symptomatology.
A number of studies have examined the factor structure of DSM-IV PTSD symptoms using confirmatory factor analytic techniques (Buckley et al., 1998). For the most part, these studies have focussed on the underlying dimensionality of individual PTSD symptoms, and specifically on the issue of whether data are consistent with the three primary symptom domains specified by DSM-IV criteria B−D (re-experiencing, numbing/avoidance, arousal). Some studies have also examined hierarchical or second-order factor models in which the identified symptom domains are assumed to be indicators of a higher latent construct reflecting the overall extent or severity of PTSD symptomatology (DuHamel et al., 2004). The comparability of their findings is constrained by the fact that these studies have typically been conducted on selected or clinic samples. It is therefore not surprising that studies vary in both the number of first-order factors identified (range two to four) and the items that load on specific factors. However, in all cases studies report high correlations between their first-order factors that are consistent with a higher-order factor model. The findings of the present study are consistent with this higher-order factor interpretation.
PTSD symptoms follow non-traumatic life events
Third, the results show that non-traumatic life events are associated with PTSD symptoms as commonly as traumatic life events. There is no evidence linking a specific class of events, traumatic/life-threatening stress, to a distinct psychiatric syndrome. These findings are consistent with two other studies exploring PTSD symptoms following traumatic and non-traumatic stress in a general population sample. Gold et al. (2005) and Mol et al. (2005) not only reported that non-traumatic life events were associated with PTSD symptoms but that the PTSD symptoms were of significantly greater severity in those who had experienced non-traumatic as opposed to traumatic life events. In our study, the correlations between the latent PTSD factor and the measures of traumatic and non-traumatic life events were almost identical (r=0.34−0.39). The findings are also consistent with a large literature linking non-traumatic life events such as marital conflict (Dattilio, 2004), childbirth (Ayers and Pickering, 2001; Olde et al., 2006), employment stressors (Scott and Stradling, 1994), bereavement (Zisook et al., 1998), and cancer (Cordova et al., 2000; DuHamel et al., 2004) with the full range of PTSD symptoms.
Because we utilized a general population sample that had responses to a wide range of life events, we were able to test for a dose−response relationship. This was significant; those in the highest decile of PTSD symptom severity reported more than 2.3-times as many traumatic events and 1.8-times other significant events than those in the lowest 40% of the sample. A recent review concluded that a simple dose−response relationship is often not supported (Rosen and Lilienfeld, 2008). However, this evidence was largely generated from studies of individuals suffering from PTSD or those responding to a single traumatic event.
Non-life-event risk factors for PTSD symptoms
Fourth, while PTSD was originally conceptualized as a response to overwhelming trauma, as early as World War I, there has been debate over the role of individual vulnerability factors (Brewin et al., 2000). Personal characteristics and childhood family circumstances have emerged as potential risk factors. We found female gender, higher neuroticism scores, childhood anxiety, low self-esteem, and poor quality of parental care remained significant in a multivariate predictor mode consistent with most similar reports (McNally and Shin, 1995; Brewin et al., 2000; Perkonigg et al., 2000; Van Loey et al., 2003; Kendler et al., 2004; Nemeroff et al., 2006). Like most studies the variables measured had modest effect sizes (β=−0.09 to 0.16).
Strengths and limitations
A major strength of this study is that it utilized a population-based sample in contrast to most studies selected from clinical populations or on the basis of exposure to a specific traumatic event. A further strength is that measures of personal characteristics and family circumstances were obtained independently from the survey of PTSD symptoms. Limitations are that the results apply to a specific population studied at a specific age. Only a small number of participants had been exposed to severely traumatic events such as war or disaster.
Implications for the classification of PTSD
Any conclusions are limited by the fact that while PTSD symptoms are common in our sample cases of PTSD as defined in DSM IV are relatively rare. Nevertheless, our results suggest that the construct validity of a stress response syndrome is robust. PTSD symptoms described in DSM IV conform to a single latent factor which is distinct from the personal characteristics of an individual or their childhood experiences. This latent factor demonstrates a dose−response relationship with negative life events. The DSM 5 proposal has suggested relatively minor changes: the elimination of criterion A2 (i.e. the peri-traumatic fear, helplessness or horror requirement) and the addition of three new symptoms and a reorganization into four symptom clusters (see Miller et al., 2012 for a fuller description).
Our findings support the evidence that there is no distinction between traumatic versus non-traumatic negative life events in causing PTSD symptoms. It is the total exposure to negative life events that is related to the number and severity of PTSD symptoms and an individual’s reported impairment. Rates of PTSD using only traumatic events as criterion A are 1.9%. These rise to 3.4% if non-traumatic life events are included. Finally, while individual differences do contribute to the likelihood of having PTSD symptoms, the most important factor is exposure to negative life events.
These findings suggest that PTSD might be reconceptualized as a stress response dimension (possibly called “stress disorder”) ranging from an adjustment disorder related to difficult life experiences at one end to severe and persistent symptoms related to significant trauma at the other. The nature of the negative life event would need to be specified since it is possible that some types of events, such as sexual violence or military combat, are more likely to lead to PTSD symptoms (Norris et al., 2002; Gold et al., 2005). The low level of these types of trauma in our sample meant we were unable to test this.
In conclusion, criteria B−F for PTSD form an underlying dimension which affects the individual’s level of responsivity to stressful life events. Traumatic (criterion A) and non-traumatic life events have a strong dose−response relationship with PTSD symptoms. Personal characteristics and childhood family circumstances have a modest relationship to PTSD symptoms. This evidence suggests re-conceptualizing as a “stress disorder” which describes a coherent group of symptoms associated with traumatic or negative life experiences.
Footnotes
Funding
This research was funded by Health Research Council of New Zealand (04/283 and 07/283).
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.