
Abstract

People with severe mental illness have higher mortality rates due to cardiovascular disease than the general population (De Hert et al., 2011b). Accordingly, many risk factors of cardiovascular disease are associated with mental illness, such as hypertension, abdominal obesity, diabetes and dyslipidemia (Galletly et al., 2012; Ostergaard and Foldager, 2011). Currently, risk factors of cardiovascular disease are frequently under-diagnosed and under-treated in psychiatric inpatients (De Hert et al., 2011a,b). In this respect there are at least three challenges: Firstly, psychiatrists self-reported clinical practice concerning medical illness is not up to date with current guidelines of diagnostics and treatment (Bauer et al., 2008). Secondly, screening rates for cardiometabolic risk factors in psychiatric wards are generally low (Holt et al., 2010). Thirdly, there is a tendency for workers in psychiatry to abrogate responsibility of physical health (Lawn, 2012).
Today, a common solution to under-diagnosing is implementation of screening guidelines. But in doing so, we often forget to ask the essential question: Why are our patients under-diagnosed in the first place? To answer this, we must remember three things: (i) Good clinical work is a complex process comprising multiple steps (e.g. clinical examination, treatment) and multiple functions (e.g. nurses, doctors). (ii) In order to find out where to focus efforts of improvement most efficiently, the process must be broken into its components and analysed as such. (iii) Causes for the same problem may vary between institutions and departments, and so may the solutions to correct it.
The question is then: How do we practically, and in the context of local clinical practice, identify the cause(s) of under-diagnosing and under-treatment? We suggest an approach that is both quantitative (how many diseased patients do we miss?) and qualitative (in what aspects of clinical assessment do we fail?). The aim is to understand how we assess our patients and thus guide us to a customised solution in the context of local circumstances. The model comprises three steps: First, all consecutive admissions over a given period are screened for the variables that one wishes to evaluate (in this example hypertension, diabetes, dyslipidemia and abdominal obesity). Second, patients who are identified with both (a) untreated and undiagnosed disease and (b) previous admission on a different but recent occasion to the ward in question, are selected as cases for a retrospective evaluation. Third, the medical records of cases are scrutinised for information on how each measure was assessed clinically at previous admission. This is done by posing a series of four questions, where lowest level of assessment is ‘no examination performed’ and highest level of assessment is ‘generation of action’ (e.g. treatment) (Figure 1, model).
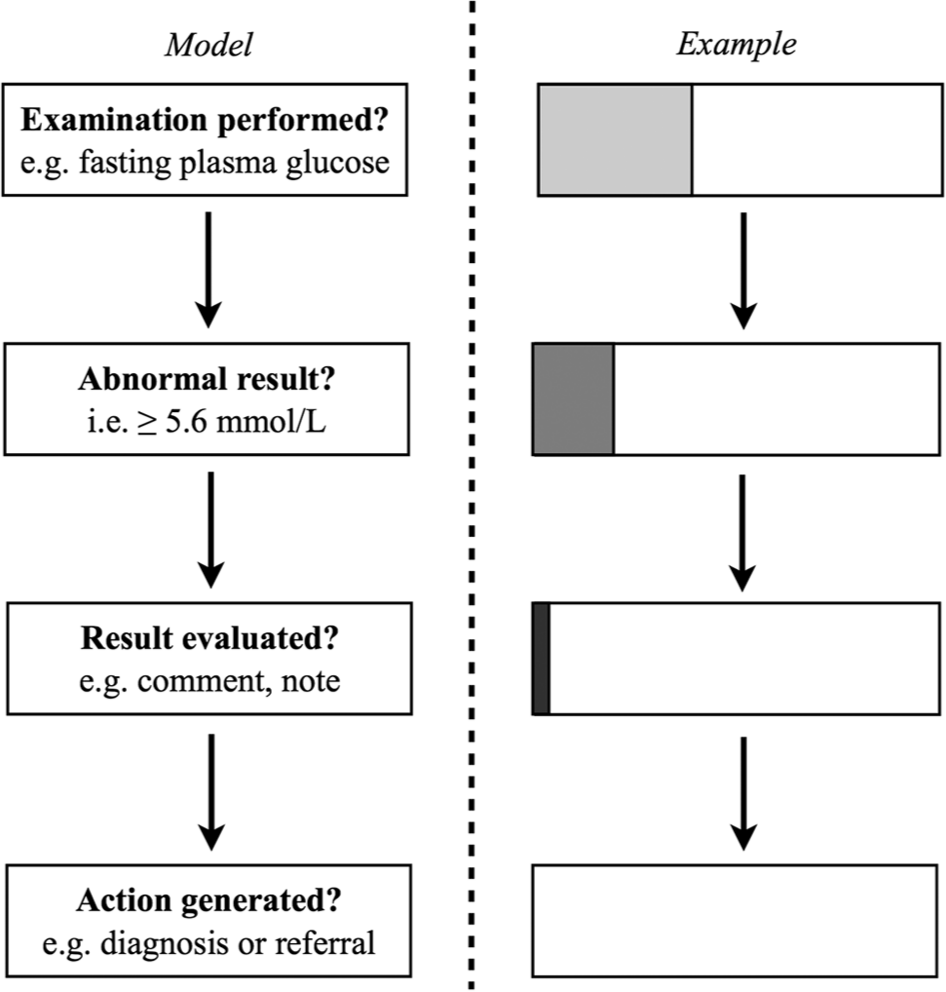
Sequence of questions to evaluate clinical practices
Example: At Risskov Psychiatric Hospital in Denmark, from 15 May through 15 August 2012 (93 days), all consecutive admissions (n = 63) to an inpatient ward were screened for hypertension, dyslipidemia, abdominal obesity and diabetes 1 . This was carried out by recording blood pressure (raised ≥ 130/85 mmHg), waist circumference (central obesity ≥ 94 cm for men and ≥ 80 cm for women), fasting blood glucose (raised > 5.6 mmol/l), fasting plasma triglycerides (raised > 1.7 mmol/l) and high-density lipoprotein (reduced < 1.0 mmol/l for men and < 1.3 mmol/l for women) (Alberti et al., 2009). From the screened subjects, we identified those fulfilling both of the following: (a) Presence of undiagnosed and untreated hypertension, dyslipidemia, abdominal obesity and/or diabetes; and (b) admission on a separate occasion within the previous 2 years to Risskov Psychiatric Hospital. These patients (n = 32) were selected for a retrospective patient file review and their medical records were scrutinised for information on how each cardiometabolic measure was assessed at previous admission.
The results for our department showed that during admission, relevant examinations were performed in 38% of cases (Figure 1, example). The most infrequently performed examination was fasting glucose (17%) and the most frequently performed was blood pressure (89%). The results of the examinations were abnormal for 54% of cases, which was expected. Interestingly, however, abnormal test results were evaluated in just 14% of cases and none of the evaluated results were acted upon.
Dissecting clinical practices into its components has several advantages: First, the evaluation can serve to argue for the allocation of (economic) resources. In our clinic, this could be education in options of diagnostics and treatment when presented with patients with abnormal cardiometabolic test results. Second, the evaluation can serve as an incentive to change clinical practices. This could be done by presenting the results as feedback to the clinicians involved. In a recent discussion paper, Lawn (2012) argues that common barriers to people with mental illness receiving adequate care for their physical health are lack of knowledge, motivation and responsibility, from the view of health care workers. This has the implication that rigorous examination and testing of patients is only of value if clinicians have the essential knowledge to interpret the results and feel responsibility to do so. Our findings support this argument. Just 38% of relevant examinations were performed, and this number is, without a doubt, too low. A solution could be routine screening of newly admitted patients, but before doing so, it is of utmost importance that we enhance the level of knowledge among health care workers about hypertension, diabetes, obesity and dyslipidemia. Also, we must work with their motivation to take responsibility for translating abnormal test results into diagnoses and treatment.
See Viewpoint by Lawn, 2012, 46(1): 14–17, see also Research by Galletly et al., 2012, 46(8): 753–761
Footnotes
Acknowledgements
We thank Søren Dinesen Østergaard and Mette Høegh Wendelboe for valuable comments on the manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.