
Abstract

It is well recognised that mood and behaviour are significantly influenced by social and environmental circumstances. In particular, social contagion theory hypothesises that emotions can behave like infectious diseases spreading through groups of intimates in social networks (Hill et al., 2010), leading to population clusters with higher rates of mood symptoms. Hazell (1993) used the same infectious disease model to describe the potential clustering of adolescent suicide. Until recently, the social transmission of mood and behaviour has been hard to track. The complex and dynamic nature of human relationships makes it difficult to quantify the effect of mood contagion at a population level. Using sophisticated social network analysis of large datasets, such as the Framingham Heart Study (FHS), Christakis and Fowler (2012) have examined the structural and qualitative architecture of social networks and the dynamic changes that took place over a 32-year period in the FHS. Utilising complex mathematical modelling, they were able to assess how the social architecture of a community influenced the incidence and spread of a variety of health and behavioural outcomes in Framingham, Massachusetts.
Emotional contagion is often considered to be transient but the FHS studies found the effects could be long term and profound. Obesity, smoking, alcohol use, depression, loneliness and happiness spread through the web of relationships within broader social networks, with effects occurring over decades (Cacioppo et al., 2009; Christakis and Fowler, 2007, 2008; Fowler and Christakis, 2008; Rosenquist et al., 2010, 2011). Using this unique longitudinal dataset of the FHS, the studies showed that there was a social contagion component for mood including depression, loneliness and happiness (Christakis and Fowler, 2008, 2012; Hill et al., 2010; Rosenquist et al., 2011).
Their model (Christakis and Fowler, 2012) specifically demonstrated that these social health effects were not just a selection effect in that ‘birds of a feather flock together’ or that there was a shared environmental exposure. Depressed people not only sought out others with depressive symptoms, but also they changed each other’s mood over extended periods of contact. Interestingly, they found that ‘friends of a friend of a friend’ (up to three degrees of separation) were influenced by the contagious spread of mood (Hill et al., 2010; Rosenquist et al., 2011). Of particular importance was the finding that friends were significantly more influential than family members in the spread of mood, especially among women (Rosenquist et al., 2011). This latter finding of the more marked influence of peers compared to family members is somewhat surprising and certainly warrants further investigation.
Positive and negative emotional states behaved much like infections, gradually spreading through social networks (Hill et al., 2010). The effects were cumulative, with increased risks associated with the number of contacts with low or positive mood. Contagion of mood states likely relates to a combination of the spread of ideas, behaviours and affect. The precise mechanism is not known but it likely has both unconscious and conscious elements. The unconscious element could relate to automatic mimicry (Hatfield et al., 1993) and the mirror neuron system (Ocampo and Kritikos, 2011). Through afferent feedback, the receiver feels the sender’s expressions, and this leads towards emotional convergence (Hatfield et al., 1993). The conscious component could be due to shared communication styles such as co-rumination, especially amongst young women (van Zalk et al., 2010). Peer influence mechanisms in the adolescent literature include engaging in high-status behaviours, matching the social norms of a valued or desired group, engaging in behaviours that are reinforced by peers and engaging in behaviours that contribute to a favourable self-identity (Brechwald and Prinstein, 2011). People may also adjust their communication styles based on social comparison in order to dynamically fit the social environment (Barsade 2002; van Zalk et al., 2010). In contagion research, we need to understand human influence moderators and this relates to identifying the characteristics of the individual, characteristics of the influencing person, the target-influencer relationship and the type of behaviour in question (Brechwald and Prinstein, 2011).
Social contagion theory and the network analysis of the FHS have important clinical and public policy implications for mental health. In this modelling, the social network is the potential cause of both positive and negative mood (Hill et al., 2010). Specifically, if friends or family are depressed, this might cumulatively increase the chance of the index person being depressed. Equally, the person’s depression could have measurable long-term effects on the moods of his or her contacts for three degrees of separation.
Implications for psychiatry and clinical practice
The FHS shows the clustering of high and low mood in groupings within networks, with depressed moods spreading through intimate contacts among friends and families over long periods of time (Fowler and Christakis, 2008; Hill et al., 2010; Rosenquist et al., 2011). Social network analysis highlights the importance of social relationships in mood creation. The influence is a ‘two-way street’ between the person and his or her social network.
In public health, it is known that influential people can change the patterns of contagion in peer social networks and deliver positive messages about health behaviour. For instance, popular and well-liked members of the gay community were able to spread the message about ‘safe sex’ behaviour (Kelly et al., 1997). A randomised community-level study showed that: ‘Natural styles of communication, such as conversations, brought about population-level changes in risk behaviour’ (Kelly et al., 1997; 1500). Influential students have been trained in smoking prevention during adolescence, which is the formative stage for health behaviour. The ASSIST smoking prevention program used peer nominations to select influential students who promoted non-smoking within their informal social networks (Campbell et al., 2008). Reductions in smoking prevalence were of public health significance. In Australia, a Mental Health First Aid program focused on football clubs to address depression among rural youth (Pierce et al., 2010). Football clubs are the social hubs of many small Australian country towns. Coaches were selected as influential and trained to become mental health advocates to promote depression awareness, reduce stigma and increase help-seeking.
The work of Christakis and Fowler shows that mental health problems are not randomly distributed in social networks (Figure 1). Emotional contagion increases the clustering of mood disorders in the population (Rosenquist et al., 2011). The individual’s mental health is correlated with the adjustment of his or her intimates: if your friends are depressed, you are more likely to become depressed in the future. This general tendency is illustrated in Figure 1, which shows the clustered pattern for depression in a social network of 957 friends, spouses and siblings. Clusters identified in blue have higher mean levels of depression (Rosenquist et al., 2011). These tended to be towards the edge of the network. The network map suggests that screening and case finding could be directed towards the social circle of people identified with depression. Many patients who present to psychiatrists have social contacts in their family and friendship circle who are ‘at risk’ of similar problems. A public health approach could include tracing contacts and offering help within a depressive cluster.
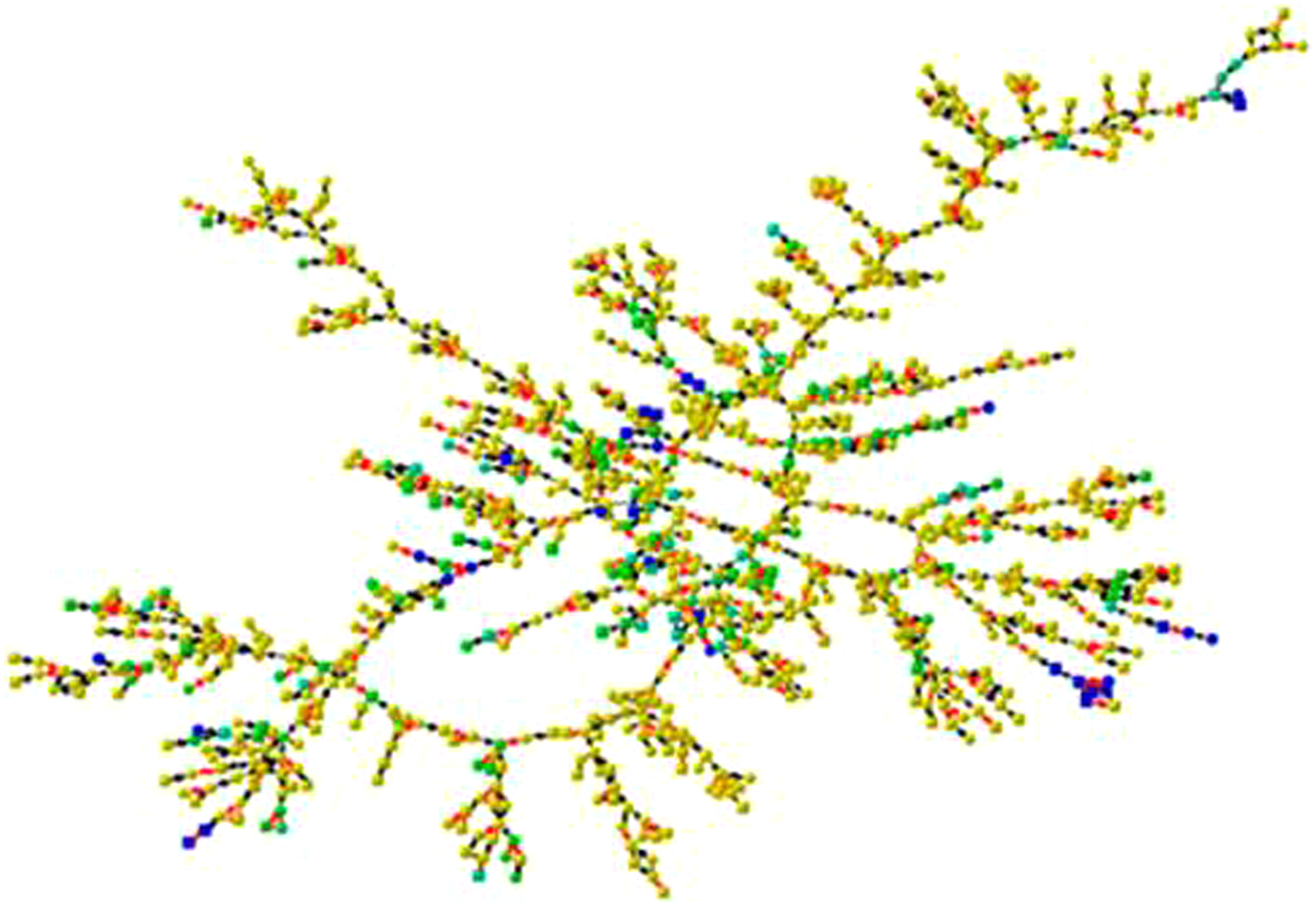
Depression Clusters in the Framingham Social Network (Rosenquist et al., 2011). This graph shows the largest component of friends, spouses and siblings at exam 7 (centered on the year 2000). There are 957 individuals shown. Each node represents a subject and its shape denotes gender (circles are male, squares are female). Lines between nodes indicate relationship (red for siblings, black for friends and spouses). Node color denotes the percentile score of the mean level of depression in ego and all directly connected (distance 1) alters, with yellow being below the 80th percentile, shades of green being the 80th to 95th percentile, and blue being above the 95th percentile (the most depressed).
Close ties are the building blocks in Christakis and Fowler’s models. The architecture of social networks is remarkably consistent across human societies, with each person usually having an intimate support group of about five (family members and best friends) and an active social network of around 150 (people you know who also know you) (Sutcliff et al., 2012). The size of the active network is probably biologically based and related to the carrying capacity of the social brain (Sutcliff et al., 2012). Obviously, active networks are severely diminished in some clinical populations. Psychotherapy includes conversations about contacts throughout the person’s available social network. Patients use discursive social narratives to describe relationships in various sections of their extended network. These 150 ties provide them with multiple pathways into the broad community networks described by Christakis and Fowler.
In clinical practice, social contagion theory can be incorporated within a comprehensive biopsychosocial formulation to enrich our understanding of influence from a patient’s regular social contacts on his or her emotional state. Sociograms are a familiar tool in family therapy and interpersonal therapy. Using more comprehensive network sociograms, one can explore a complete picture of the dynamics of the patient’s social network, including friends, family and work colleagues and also the known connections of the patient’s networks. It includes the structure of the network, the quality of the connections between members, and their emotional status. The extended sociogram assists in identifying the strengths and weaknesses within the patient’s network and the people who can assist. The sociogram may form a key component of psychoeducation. Obviously this is a subjective assessment of the network but it helps in understanding the patient’s social perspective better; aids therapeutic engagement by constructing the sociogram as a collaborative process; and is helpful for exploring the influence of the broader web of relationships. Understanding the immediate network through a sociogram is particularly relevant given contagion is much stronger for immediate friends compared to friends of a friend, and friends of a friend of a friend (Rosenquist et al., 2011).
The social network information obtained from this thorough assessment informs many aspects of treatment and social rehabilitation. Psychotherapy can be used to assist the patient to reflect upon and better navigate his or her social network. One pragmatic aim is to encourage greater contact with those network members who have a positive effect on the patient’s mood. Therapeutic intervention is directed at shared activities that have a beneficial effect on the overall functioning of network groups. For instance, pleasant activity scheduling, as part of behavioural activation, would be more meaningful if the patient’s supportive social network is incorporated in the activities.
Patients can develop better skills in navigating their networks. This may involve approaching those who have a beneficial effect on their presenting problems and having more contact with these sections of their network. Managing the impact of problematic relationships is a core therapeutic issue in clinical practice. However, the importance of positive support in depression treatment is also vital, especially from social contacts beyond the immediate family. For instance, clinicians can utilise direct peer support as part of the treatment for depression. Placing the emphasis on the social network and strengthening a broader range of relationships enhances the social scaffolding of our patients and could ultimately contribute to resilience and positive mental health.
Social network approaches to treatment are emerging in the field of alcohol dependency. These network therapies focus on the immediate social circle of close friends and family. In a large multicentre trial, the UK Alcohol Treatment Trial (UKATT) (UKATT Research Team, 2005) compared manualised motivational enhancement therapy (MET) with manualised social behaviour and network therapy (SBNT). Results showed that SBNT was as effective as the proven MET with a 45% reduction in alcohol consumption after 12 months. SBNT initially focuses on identifying the social network of the alcohol user that he or she identifies as potentially supportive of his or her efforts to change. The social network is then developed to support change using a variety of strategies and continues to help in the maintenance of the goals achieved during SBNT. Significantly, UKATT shows network therapy can be done in the real world for difficult problems. Based on the above important finding, it is possible that similar approaches could be applied in conditions such as mood disorders or eating disorders.
Limitations of the contagion model
Modelling these social interactions is undoubtedly a complex area that continues to be debated – with disagreements about the statistical modelling and the conclusions derived (Cohen-Cole and Fletcher, 2008). Christakis and Fowler (2012) have submitted a rebuttal to these criticisms of their work and methodology in a review paper.
Major depression is clearly a multifactorial disorder. An individual’s probability of suffering from an episode of major depression is related to: genetic influences, childhood sexual abuse, premature parental loss, predisposing personality traits, low self-esteem, exposure to trauma, low social support, substance misuse, marital difficulties, a prior history of major depression and recent stressful life events (Kendler et al., 2002). The contagion hypothesis therefore has to be understood in the context of these other prominent factors. It is of note that several twin studies have failed to show evidence for a familial–environmental contribution to the aetiology of major depression (Kendler et al., 2002). This is somewhat surprising in light of contagion theory for depression. However, the social network depression study FHS social network studies (Rosenquist et al., 2011) finds more strength of association for peer compared with family effects for depression contagion.
Given the complex multifactorial aetiology for depression, it is unlikely that any one risk factor will explain its development. It is also unlikely that focusing on a single risk factor like contagion will be sufficient to prevent depression. It is more likely that the accumulation and interaction between multiple risk factors could lead to depression (Kendler et al., 2002).
The UKATT approach to alcohol misuse reduces exposure to friends who are still drinking. This kind of approach could be seen as blaming or stereotyping other drinkers. More broadly, the work of Christakis and Fowler (2012) raises the possible risk of blaming and stigmatising people who are overweight or depressed, for example. Criticism of their work relates to concerns about the potential for discrimination (Merritt Johns, 2010). We were mindful of the sensitivity of this topic whilst writing this viewpoint but felt this was an important concept that needed to be understood, analysed, discussed and debated by the psychiatric profession. The FHS have potentially important societal and ethical implications. Whilst understanding the sensitivity of this topic, we also believe that understanding social contagion theory may improve the assessment, treatment and clinical outcomes for our patients.
Conclusion
An early pioneer in social and group psychology, Le Bon (1896) noted the powerful effects of groups and concluded that:
We see, then, that the disappearance of the conscious personality, the predominance of the unconscious personality, the turning by means of suggestion and contagion of feelings and ideas in an identical direction, the tendency to immediately transform the suggested ideas into acts; these, we see, are the principal characteristics of the individual forming part of a crowd. He is no longer himself, but has become an automaton who has ceased to be guided by his will.
This process of ‘the individual forming part of a crowd’ can be adaptive. Group cooperation is the key to human survival and success. Human beings are unique as species in that we form longstanding, non-reproductive unions with unrelated individuals (Apicella et al., 2012). It is thought that social networks may have contributed to the emergence of cooperative behaviour and possibly conferred an evolutionary advantage to individuals and groups who could cooperate (Apicella et al., 2012).
Genetic similarities can underlie the formation of these cooperative friendship groups. Fowler et al. (2011) found that people seek out friends who have the same genetic variants that they do beyond just physical characteristics. They hypothesise ‘that a person’s genes may lead to selection of friends with certain (social/asocial) genotypes which in turn facilitates or modifies the expression of a person’s own genes’. This provides a possible gene environment linkage accounting for the expression of clinical psychiatric disorders mediated through social networks. A better understanding of the structure of social networks may help to further contextualise the complex interaction between nature and nurture.
Group moods may help to direct cooperative behaviour in ways that can increase group success. The importance of moods of social groups has been explored in the management literature where there is recognition of the role of emotional contagion (Barsade, 2002) and the impact of charismatic leadership on influencing the group mood (Bono and Ilies, 2006). Increasing emphasis is being placed on understanding team dynamics and teamwork to facilitate positive group attitudes, group mood and better outcomes (Barsade, 2002). This understanding of contagion could be of importance to the leadership of our mental health teams as a mechanism to improve patient outcomes: positive team morale leading to better patient morale.
In clinical practice, social contagion theory of emotion illuminates both a potential cause of depressed mood and a possible solution to that from a population perspective. Emotional signals tend to spread across social groups and can tend to direct a patient’s behaviour in ways that may not be immediately apparent. Drawing on the work of Christakis and Fowler, psychiatrists can envisage low morale in broad social network clusters whilst also understanding individual vulnerability factors of the index patient.
Over the course of psychotherapy, it can become clear that social contagion of mood and behaviour is influencing the emergence and course of emotional disorders. In this context, psychiatrists could consider social contagion as a potential factor in the aetiology of the common psychiatric disorders. This may be particularly relevant for the treatment of depressive and anxiety disorders, eating disorders and somatisation. Future research studies in psychiatry may need to now focus more specifically on the concept of contagion as an aetiological factor.
Treatment effects might also be contagious. It is reassuring to know that the benefits of effective treatment for depression could extend up to three degrees of separation (Rosenquist, 2011). Individual treatments might help a wide social network.
As we come to understand social networks, psychiatrists may be able to better track contagion and become involved with improving the morale of the patient’s whole social group. This broader focus and reorientation could have positive benefits for the patient and his or her family, friends and community at large. If emotional contagion were similar to transmission of infectious disease, then increasing the emotional resilience would be akin to increasing immunity levels for infectious disease at a population level and hence could be a potentially important preventive strategy in psychiatry.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.