
Abstract
Background:
The relapse rate after a first episode of schizophrenia is high, often due to non-adherence with medication. Long-acting injections of antipsychotics (LAI) are used to promote adherence to medication.
Objective:
To review the literature on the use of LAIs in first-episode and early schizophrenia.
Method:
A systematic electronic search of all original data containing peer-reviewed studies published in English using EMBASE, MEDLINE, Cochrane and PsychINFO from the onset of records. Reference lists from retrieved articles were examined for further relevant studies.
Results:
Ten studies were identified: two cohort studies; three randomised controlled trials; and five open studies. These studies, although limited, demonstrated the effectiveness of LAI in early schizophrenia. Seven of the 10 studies had risperidone long-acting injection as the only LAI.
Conclusion:
LAIs may be useful in the treatment of early schizophrenia in terms of symptom control and relapse reduction, particularly if chosen by the patient or when medication adherence is a priority. There is a need for a large-scale, randomised controlled trial comparing oral and LAI antipsychotics to assess long-term outcomes.
Introduction
Long-acting injections (LAIs) of antipsychotics, also known as depots, are specifically designed to improve adherence to medication in people who can acknowledge that they are forgetful or who do not accept the need for ongoing treatment (Davis et al., 1994; Johnson, 2009; Keith et al., 2004). Recent guidelines (Kane and Garcia-Ribera, 2009; National Institute of Clinical Excellence (NICE), 2009) advocate the use of LAIs as maintenance treatment when adherence to oral antipsychotics has been problematic. Adherence has been defined as the extent to which a patients’ behaviour (including taking medications, following a diet, modifying habits and attending follow-ups) coincides with the medical and health advice (Davis et al., 1994; Mackay et al., 2011). Studies have shown non-adherence rates to oral medication in schizophrenia to be as high as 50% (Glazer, 2007) but LAIs are only prescribed in a small proportion of these patients (Kane and Garcia-Ribera, 2009).
Use of LAIs in the early stages of schizophrenia is controversial. There is evidence to show that non-adherence and partial adherence are most problematic during the earliest stages of schizophrenia (Coldham et al., 2002), culminating in high relapse rates (Robinson et al., 1999), self-harm and incomplete or unsustainable remission of symptoms (Andreasen et al., 2005). Furthermore, suicide occurs in 5% of individuals with schizophrenia, with young age and positive symptoms being identified as specific risk factors (Hor and Taylor, 2010). Birchwood et al. (1998) proposed the ‘critical period’ hypothesis, which considers the early phase of psychosis to be the period in which both the long-term outcome is affected and the biological and psychosocial influences show maximum plasticity.
LAIs are known to be safe and efficacious (Haddad et al., 2009) and LAI or depot formulations have been associated with a 50–65% reduced rehospitalisation rate compared to the identical medication in oral form (Tiihonen et al., 2011). Presumably, concerns regarding individual autonomy, perceived coercion, and patient choice limit the use of LAIs in first-episode schizophrenia, although there is a credible scientific rationale for early LAI use in terms of secondary prevention, avoiding relapse and sustaining remission, as well as arguably reducing suicide. Here we debate the use of LAIs in early schizophrenia after systematically reviewing their safety and efficacy in this population.
Method
Search strategy and eligible studies
A comprehensive electronic search of published peer-reviewed articles was performed using databases including EMBASE, Cochrane, PsychINFO and MEDLINE to identify relevant studies, from the onset of records. The subject headings consisted of:
(a) “long acting injection” or “depot” or “long acting antipsychotic”, and
(b) “psychosis” or “schizophrenia” or “schizoaffective”, and
(c) “first episode” or “early” or “acute”.
The abstracts of the articles found in the search were reviewed and studies were shortlisted if they: were published in English; were case–control, cohort or follow-up studies; had a patient diagnosis of schizophrenia, psychosis or schizoaffective disorder; had subjects who were first episode or were in the early stages of their disease; were being treated with an LAI form of antipsychotics.
Retrieved article reference lists were examined for further relevant studies.
Results
Data extraction
A total of 400 published peer-reviewed articles were identified by the search strategy (Figure 1). However, 379 papers did not meet the inclusion criteria. The remaining 21 papers were retrieved for further detailed assessment. Studies were not included if they did not address the objectives of this study, or did not include any outcome measures assessing the safety or efficacy of LAIs. A total of 10 articles were identified for more detailed analysis (Table 1). Data relating to the efficacy and safety of the LAIs in early and acute schizophrenia were reviewed and summarised.
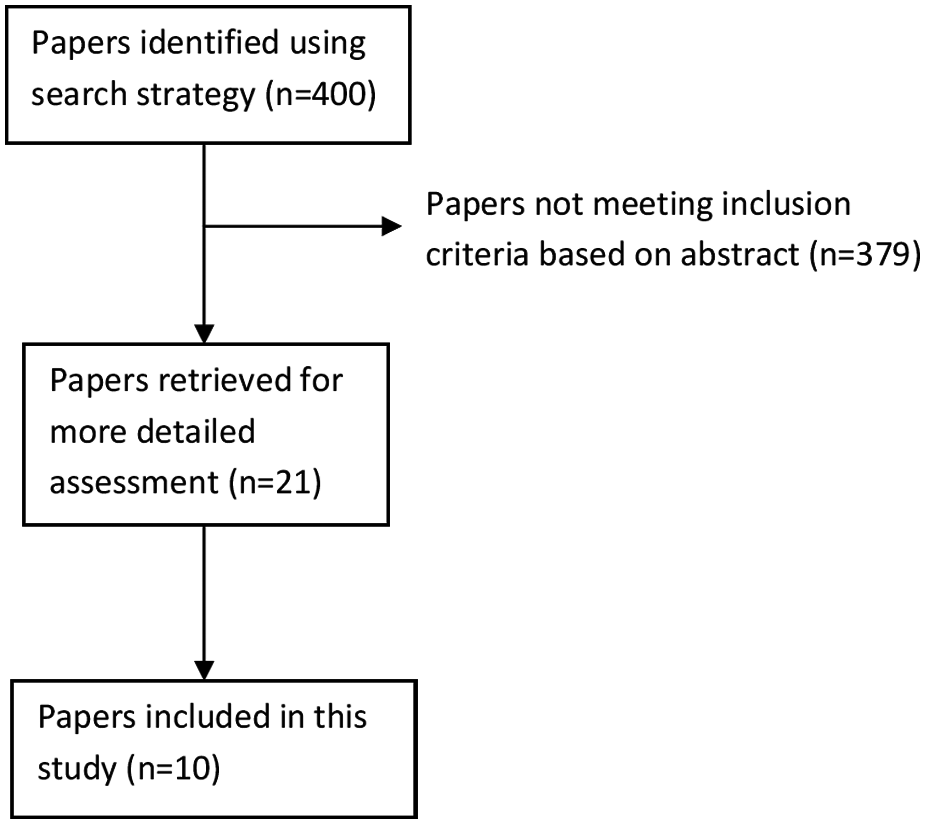
Flowchart showing identification of studies.
Studies included in this systematic review.
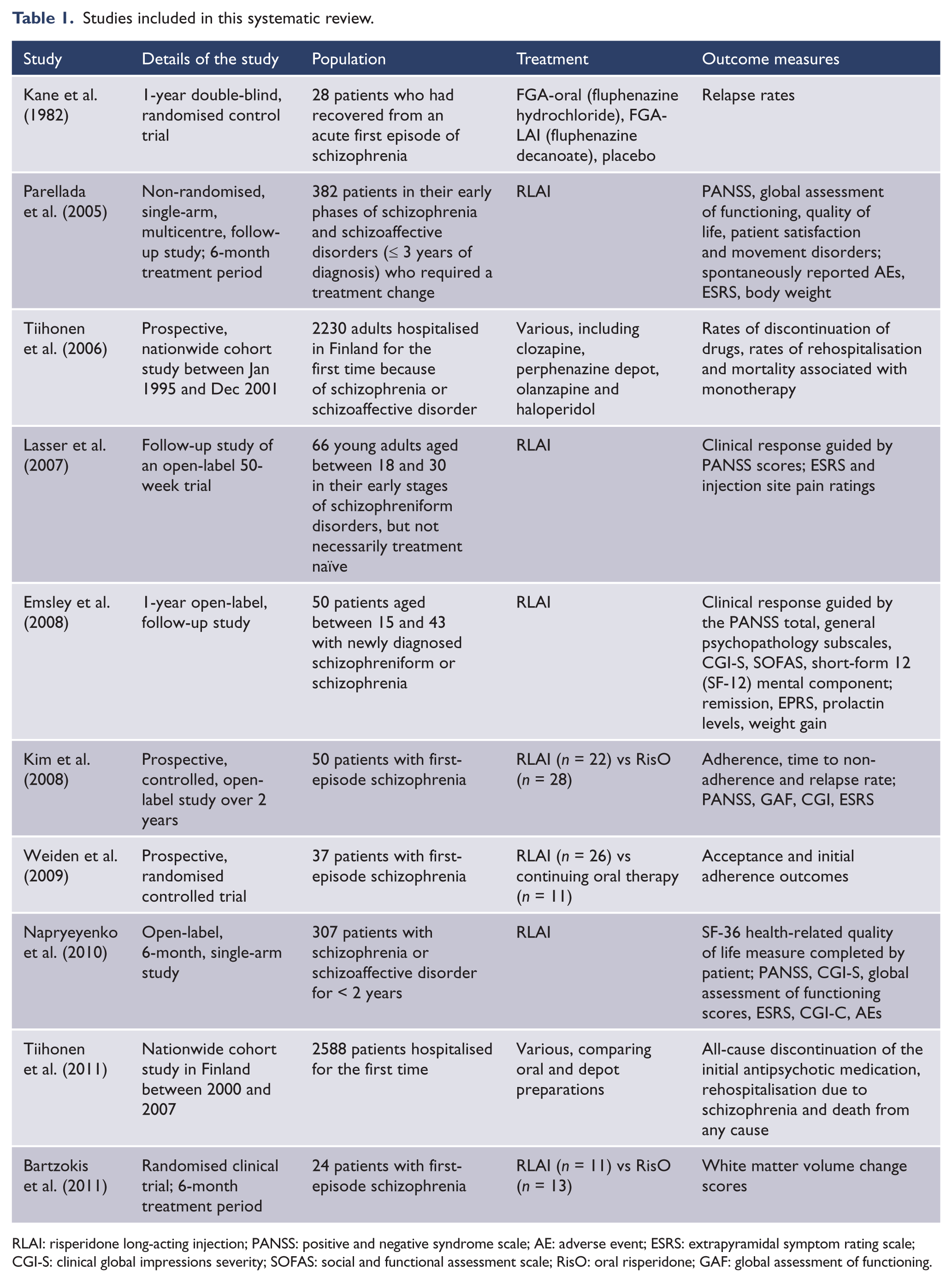
RLAI: risperidone long-acting injection; PANSS: positive and negative syndrome scale; AE: adverse event; ESRS: extrapyramidal symptom rating scale; CGI-S: clinical global impressions severity; SOFAS: social and functional assessment scale; RisO: oral risperidone; GAF: global assessment of functioning.
Efficacy
PANSS scores
In the open-label study by Emsley et al. (2008), there was an improvement from the baseline to the end point on the positive and negative syndrome scale (PANSS) total, positive, negative and general psychopathology subscales. Of the 50 patients who completed the study taking risperidone long-acting injection (RLAI), 46 of the patients (92%) achieved ≥ 20% reduction in the PANSS total scores and 42 (84%) achieved ≥ 50% reduction in PANSS scores (Emsley et al., 2008). In another open-label study for RLAI (Lasser et al., 2007), mean PANSS scores improved significantly from baseline, with 64% of patients showing clinical improvement (≥ 20% reduction in the PANSS score) at end point. Parellada et al. (2005) carried out an open-label study in patients requiring a treatment change. The total PANSS and all its subscale scores improved significantly (p < 0.0001) following treatment with RLAI, and 40% of patients showed ≥ 20% reduction in PANSS scores, 10% showed ≥ 30% improvement, and 5% showed ≥ 50% improvement at the end of the study. Improvement from baseline to end point was apparent in all subscales. An open-labelled, non-comparative study by Napryeyenko et al. (2010) showed that 68.4% (n = 201) of patients had a clinical response of ≥ 20% reduction on PANSS total. Kim et al.’s (2008) 2-year open-label study with RLAI also showed a significant reduction in PANSS scores.
Discontinuation of medication, rehospitalisation, relapse and remission
The early study by Kane et al. (1982) showed that seven out of 17 patients (41%) who received a placebo experienced a relapse, whereas none of the patients treated with oral or LAI fluphenazine (n = 11) relapsed. Tiihonen et al. (2006) showed that the use of perphenazine depot had one of the lowest rates of discontinuation for any reason when compared to oral haloperidol (adjusted relative risk, 0.24; 95% CI, 0.13–0.47) and even oral perphenazine. Perphenazine, the only LAI included in this study, was associated with the lowest rate of rehospitalisation (0.32; 95% CI, 0.22–0.49).
A separate cohort study by Tiihonen et al. (2011), which was a pooled analysis of oral and LAI medications (haloperidol, perphenazine, risperidone and zuclopenthixol), revealed that LAI antipsychotics had a significantly lower risk of discontinuation of medication (59%) when compared with oral antipsychotics (hazard ratio, 0.41; 95% CI, 0.27–0.61; p < 0.0001). LAIs were also associated with a significantly lower risk of rehospitalisation than oral formulations (adjusted hazard ratio, 0.36; 95% CI, 0.17–0.75; p = 0.007; weighted mean, 0.53; 95% CI, 0.32–0.88).
A randomised controlled trial (RCT) by Weiden et al. (2009) found that patients accepting RLAI were significantly more adherent (89%; 95% CI, 64–97%) than those staying on oral antipsychotics (59%; 95% CI, 32–78%).
In Emsley et al.’s (2008) open-label study, 32 patients (64%) achieved remission (Andreasen et al., 2005) during the trial and 39 (78%) showed a meaningful clinical response, from which only four relapsed. The relapse rate was 8% and relapse was related to hospitalisation in three cases and a suicide attempt in one of the cases. Napryeyenko et al.’s (2010) trial of the 201 patients showing clinical response found that only five patients relapsed. Of the 199 patients who did not meet the PANSS symptom remission criteria on entering the study, 40% (n = 80) attained and maintained remission for 3 months. Kim et al. (2008) demonstrated that medication adherence at 1 and 2 years (RLAI = 81.4 ± 26.6, oral risperidone (RisO) = 54.6 ± 32.1; p < 0.01) was significantly higher and relapse rates at 1 and 2 years (RLAI = 23%, RisO = 75%; p < 0.01) were significantly lower in the RLAI group compared to the RisO group.
White matter volumes
A randomised clinical trial by Bartzokis et al. (2011) showed that white matter (WM) volume was not significantly changed when patients were treated with RLAI (n = 11), while treatment with RisO (n = 13) showed a reduction in WM volumes. The covariate adjusted mean change score from baseline for the RisO treatment group was −0.567 (p < 0.05).
Safety
Movement disorders
There were 32 extrapyramidal symptom-related adverse effects (AEs) in Emsley’s (2008) open-label study of 50 people. In Napryeyenko’s (2010) open-label study, a total of 44 extrapyramidal symptom-related AEs were reported by 17 (5.6%) patients and the mean change in the extrapyramidal symptoms rating scale (ESRS) from baseline was −0.5 following treatment with RLAI. Lasser et al. (2007) showed that the severity of movement disorders (ESRS) was improved with RLAI from 3.1 ± 3.2 at baseline to 1.6 ± 2.4 at end point (p < 0.0001), and the physicians rated parkinsonism as significantly improved whilst physician ratings for dyskinesia, akathisia and dystonia were consistently low throughout the study (mean score < 1). Parellada et al.’s study (2007) revealed that ESRS total and subscale scores, including assessment of parkinsonism, dystonia, dyskinesia and akathisia improved significantly from baseline to end point (p ≤ 0.01) when treated with RLAI. In Kim et al.’s (2007) study there were no significant differences in scores of ESRS between the RLAI and RisO treatment groups.
Weight gain
Emsley et al. (2007) found weight gain to be substantial, especially in the first 12 months of the study. The mean increase in body mass index (BMI) was 4.8 kg/m2 (SD 3.8 kg/m2). In Parellada’s study (2005), mean body weight and BMI increased by 1.8 kg and 0.6 kg/m2 from baseline to end point (p < 0.001) when treated with RLAI. Napryeyenko et al.’s (2010) study documented a mean weight gain of 0.2 kg/month and a mean change in BMI of 0.07 kg/m2 in the patients.
Metabolic disturbances
Five patients (10% of total) had an increase in blood cholesterol in Emsley et al.’s (2008) study. A total of 18 patients had increased prolactin levels, and there were four reported possible prolactin-related AEs, including amenorrhoea and galactorrhoea. Napryeyenko et al. (2010) found that 13 patients potentially had prolactin-related AEs. Parellada et al. (2005) noted one patient (0.3%) developed diabetes.
Other adverse effects
In the Parellada et al. (2005) study, the most frequently reported AEs were insomnia (7%) and exacerbation of psychosis (6%), and six patients (6%) reported injection site pain. Other AEs described in Emsley’s study (2008) included headache, sedation, aggression, insomnia, depression and psychotic disorder.
Discussion
LAIs were developed in the 1960s to specifically address the problem of poor adherence in the maintenance treatment of psychosis. Poor adherence remains one if not the major challenge in chronic disease management. The main advantages of LAIs over their oral counterparts are the ability to provide assured medication delivery; the beneficial dose-averaging effect, which obviates any toxic diurnal peaks and troughs; and, importantly, their built-in therapeutic contact with health service staff (Hogarty et al., 1979). Usually, the use of LAIs has been reserved for patients suspected to be poorly adherent, uncooperative, or those with refractory illness (Kane and Garcia-Ribera, 2009). It is also worth observing that there are varying international patterns of LAI usage, with some government funded healthcare systems such as the UK and Scandinavia employing LAIs in ~30% of those with chronic schizophrenia, whereas differently funded systems such as the US appear to have a lower LAI usage (Patel et al., 2009).
Individuals in the early stages of their disease may be ideal candidates for treatment with an antipsychotic LAI. In psychosis, the initial treatment period represents a critical window which might determine the disease trajectory (Birchwood et al., 1998). These individuals are sensitive to medication side effects (Weiden et al., 2009) and often have limited insight or acceptance of their illness, which in turn contributes to the poor adherence (Coldham et al., 2002), high treatment discontinuation rates and relapse rates (Robinson et al., 1999). Also, many individuals in the early stages of the disease pathway do not accept the gravity of their illness, and there can be a false sense of treatment being unnecessary or an unwanted imposition (Kane and Garcia-Ribera, 2009). Balanced against this, is the recognition that 20% of individuals who suffer a psychotic episode will never relapse. Additionally, many clinicians may have the preconceived view that patients are unwilling to accept injections in the early stages of their disease (Heres et al., 2011). This presumption of rejection could be viewed as physician prejudice, in an era when fully informed patient choice is advocated (Samele et al., 2007).
In our literature search, we identified over 400 articles and yielded only 10 that satisfied our study question: researching the outcome of LAIs in early stages of schizophrenia. Not all studies identified were RCTs. Therefore, it was appropriate to perform a systematic review and not a meta-analysis. We reviewed five studies that included first-episode schizophrenic patients (Bartzokis et al., 2011; Emsley et al., 2008; Kane et al., 1982; Kim et al., 2008; Weiden et al., 2009), three studies that included patients with early schizophrenia (Lasser et al., 2007; Napryeyenko et al., 2010; Parellada et al., 2005), and two studies that included patients hospitalised for the first time (Tiihonen et al., 2006, 2011).
The use of RLAI improved symptom reduction in five initiation studies for first-episode cases (Emsley et al., 2008; Kim et al., 2008; Lasser et al., 2007; Napryeyenko et al., 2010; Weiden et al., 2009), perhaps unsurprisingly. In patients receiving a treatment switch to RLAI in the early stages of schizophrenia, 40% of patients had at least a 20% reduction in their PANSS (Parellada et al., 2005). Emsley et al.’s (2008) preliminary study examining the efficacy and safety of directly initiated RLAI in 50 patients with first-episode psychosis, showed that remission was achieved in almost two-thirds of the patients and relapse rates were low, which is comparable with the results achieved in the RLAI treatment of subjects with chronic schizophrenia (Parellada, 2006). Kim et al.’s (2008) RCT showed that adherence to medication was higher and relapse rates lower in patients treated with RLAI compared to oral RisO. The improvement in symptom profile supports the efficacy of RLAI in early schizophrenia, and the results are comparable with those obtained in a study of over 1800 patients with schizophrenia or other psychoses (Moller et al., 2005). However, studies of RLAI in non-first-episode (i.e. chronic unstable) cases have not suggested a superiority of RLAI over oral antipsychotic medication (Keks et al., 2007; Rosenheck et al., 2011), and there is retrospective data (Shajahan et al., 2010) suggesting that RLAI may not be as effective as another LAI, zuclopenthixol decanoate.
Bartzokis et al.’s (2011) study showed that there was a significant differential in WM volumes in patients treated with LAI and RisO. Frontal lobe WM volume, which was estimated using inversion recovery MRI images, deceased significantly in the RisO treatment group. They also showed that increased WM volumes were associated with faster reaction times in tasks involving frontal functioning. It is possible that RLAI favours the promotion and stabilisation of WM tracts in the frontal lobe. However, this study involved small sample sizes followed up for a short period. In addition, treatment before the study was not standardised and analysis was only performed at two time points.
Cohort studies in patients hospitalised for the first time with schizophrenia or schizoaffective disorder revealed that the LAI form of antipsychotics had one of the lowest rates for discontinuation and lowers the risk of rehospitalisations (Tiihonen et al., 2006, 2011). Adherence with LAIs was shown to be significantly better than patients staying on oral medication (89% vs 59%) in one prospective RCT (Weiden et al., 2009). These data support the feasibility and acceptability of introducing LAIs in early schizophrenia.
Tolerability of antipsychotics is a particular concern in first-episode cases. Movement disorders as an adverse effect were assessed in five studies we reviewed, using the ESRS. The mean maximum change in the ESRS was 1.4 in medication-naïve patients treated with RLAI (Emsley et al., 2008). In patients with early psychosis who were not treatment naïve, ESRS scores decreased from baseline to end point when treated with RLAI (Lasser et al., 2007; Napryeyenko et al., 2010; Parellada et al., 2005). Weight gain and resultant increases in BMI were, however, significant adverse effects (Emsley et al., 2008; Napryeyenko et al., 2010; Parellada et al., 2005). Considerable hyperprolactinaemia was also observed in first-episode cases (Emsley et al., 2008) and in cases diagnosed for less than 2 years (Napryeyenko et al., 2010). Usually, medication-naïve individuals are acutely sensitive to antipsychotics in terms of responsiveness as well as side effects, including extrapyramidal symptoms (Chatterjee et al., 1995) and weight gain (Strassnig et al., 2007). However, it is generally thought that LAIs have a more acceptable side-effect profile in comparison with their oral counterparts due to their differences in pharmacokinetics, and any concerns over debilitating side effects may be due to dosing errors (Taylor, 2009). Peaks and troughs in drug concentrations can be minimised via the dose averaging of LAIs, reducing the risk of some adverse effects of these medications (Taylor, 2009).
Public heath principles promote early prevention of morbidity and mortality. If LAIs are effective and feasible in early psychosis, many clinical advantages may ensue before a patient can ‘prove’ themselves to be non-adherent. Results from the limited number of studies available suggest that the use of LAI in early phases of the disease could result in effective delivery of antipsychotic medications, helping patients to achieve remission. However, the studies reviewed (Emsley et al., 2008; Kim et al., 2008; Lasser et al., 2007; Napryeyenko et al., 2010; Parellada et al., 2005) have limitations including their open-label nature, the absence of a control group for comparison and the small sample sizes. The heterogeneous definitions of relapse and remission pose difficulties when comparing results of studies. These limitations prompt caution in interpreting the data on efficacy and safety. Although Weiden et al.’s (2009) RCT showed that patients were more adherent to RLAI compared to oral antipsychotics, the study was small and the treatment given by clinicians was not blinded. In addition, outcomes were evaluated 12 weeks after RLAI treatment so long-term attitudes and behaviours on adherence cannot be deduced from this study. Of the 10 studies reviewed, seven investigated the effects of RLAI; therefore, conclusions drawn from this review cannot be generalised to reflect the safety and efficacy of all LAIs. There is a need for a long-term RCT comparing the effectiveness of oral and LAI antipsychotics in early psychosis and first-episode schizophrenia whilst also examining the safety and tolerability of these agents, once a consensus on the definition of early psychosis is established.
The use of LAIs is not without problems. LAIs require the burden of frequent travel to outpatient clinics or home visits by community nurses for their administration. LAIs are not ideal for people who dislike injections, and overt non-adherence to LAIs can occur, indicating the importance of shared decision-making when prescribing such medications. On surveying psychiatrists, Heres et al. (2011) found that the three main factors influencing their choice not to prescribe a LAI for first-episode psychosis were: (a) limited availability of different second-generation antipsychotic depot drugs; (b) the frequent rejection of the depot offer by patients; and (c) the patient’s skepticism based on an inexperience of relapse, demonstrating the importance a patient-centred approach when discussing LAI as a treatment option. The prescription of a LAI should also involve a collaborative psychosocial approach concentrating on the individual’s needs and involving the multidisciplinary team in order to optimise outcomes. This approach would be consistent with first-episode or early intervention services (Weiden et al., 2007).
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of interest
MT has received hospitality and / or fees from various pharmaceutical firms including Janssen, the manufacturers of risperidone LAI. KYBN has no conflicts to declare. No external funding or advice was received in connection with this paper.