
Abstract
Objective:
Lack of capacity to consent to psychiatric treatment has been promoted as a better basis for compulsion than mental disorder plus risk of harm. Previous research has examined how that legal change would affect acutely unwell inpatients. There is little research on forensic patients. This research aimed to assess capacity to consent in forensic patients at different stages of recovery and to consider the implications of respecting their competent treatment decisions.
Method:
Capacity to consent was assessed in a cross-sectional sample of 109 forensic patients both in hospital and in community settings.
Results:
The majority of participants (67.6%) had treatment-related decision-making capacity. Very few patients with capacity refused treatment.
Conclusions:
Change to a capacity-based legal approach may alter treatment for some forensic patients but would not necessarily increase risk of harm to others. The implications for release decisions are less clear.
Introduction
Mental health legislation is often criticised for being fundamentally inconsistent with a rights-based approach to healthcare because it may permit the treatment choices of compulsory patients with capacity to be overridden (Campbell, 1994; Szmukler and Holloway, 1998). In many jurisdictions this concern has produced legal reforms that give greater respect to individual autonomy in treatment decisions, granting patients with capacity the right to refuse treatment even if it could lead to the clinically and ethically fraught situation of detention without treatment.
Previous research examining the impact of such legal change has tended to focus on acutely unwell inpatients where the effect of reform may be surprisingly limited, as a high proportion of such patients lack capacity (Bellhouse et al., 2003a, 2003b; Cairns et al., 2005). However, very little is known about the epidemiology of capacity to consent to treatment among forensic patients and patients subject to community treatment orders, who may not be acutely unwell. In many jurisdictions, including New Zealand, there are many more patients on community-based orders than under compulsory treatment in hospital (Ministry of Health, 2011), and a significant proportion of forensic patients are treated in community settings. Furthermore, where third party risks require consideration the assessment of capacity takes on additional complexity.
Most forensic inpatients have committed an act of violence in the context of an acute mental illness. They will not usually be released into the community unless mentally stable and compliant with treatment. The justification for this approach in most jurisdictions is rooted in concerns about third party risks in the context of future relapse. A capacity-based approach could see forensic patients with an understanding, appreciation and ability to provide reasoned responses to these issues being assessed as having decision-making capacity. However, uncertainty surrounds the long-term consequences of respecting these competent treatment decisions, particularly whether third parties would be exposed to unreasonable risks.
The aim of this research was to assess capacity to consent to treatment in a cross-sectional population of forensic patients in hospital and community settings, and to consider the implications of respecting their mentally competent treatment-related decisions.
Method
A cross-sectional design was used to sample forensic patients at all stages of recovery from acute admission to community care, both on forensic and subsequent civil treatment orders.
New Zealand has a population of 4.3 million persons. Forensic mental healthcare is delivered by five regional services, all of which provide compulsory care for patients in both hospital units and the community. At the commencement of the study, there were 215 forensic inpatients plus approximately 160–180 forensic patients residing in the community, a national total of roughly 400.
Participants were recruited from users of the two largest regional forensic services in New Zealand, centred in Auckland and Wellington, which care for about half of all forensic patients nationally. All were compulsorily treated under the Mental Health Act (MHA), either as so-called special patients (various categories of forensic patient), or on subsequent civil orders. They were domiciled in various settings from highly secure inpatient units to open community care settings, and were provided with a NZ$25 gift voucher for participating. Potential participants took no further part if they were: unwilling to consent to the research; on no prescribed medication; presenting no assessed risk of harm to others; unable to communicate adequately in English; too unwell to participate; or had a DSM-IV diagnosis of mental retardation, delirium, dementia, amnesia or other cognitive disorder.
Ethical approval was granted by the New Zealand Health and Disability Ethics Committee.
Assessment measures
The main assessment instrument was the MacArthur Competence Assessment Tool for Treatment (MacCAT-T) (Grisso et al., 1997). This semi-structured interview provides relevant treatment information to the patient and then assesses their capacity to consent to that treatment in four domains: understanding of the disorder and treatment-related information; appreciation of the significance of that information; reasoning ability; and ability to express a treatment choice.
A binary determination of capacity to consent to treatment was made, using the UK Mental Capacity Act 2005 criteria. This Act states that persons are unable to make a decision for themselves if they are unable to: understand the information relevant to the decision; or retain the information relevant to the decision; or use the information relevant to the decision as part of the process of making the decision; or communicate the decision.
The initial part of the interview established the subject’s basic demographic information including age, sex, ethnicity, marital status, educational background, living circumstances, sources of income, legal status, index offence, primary and secondary diagnoses, and the principal medication that would be the focus of subsequent questioning with the MacCAT-T. An abbreviated standard psychiatric history was then taken, focusing on the presenting complaint on admission, the history of the presenting complaint, and past psychiatric history. Particular care was taken to identify symptoms of illness related to risk to others that would be used in the MacCAT-T interview.
Current psychopathology was assessed with the Brief Psychiatric Rating Scale (Ventura et al., 1993). Insight was further explored by completion of the Schedule for Assessment of Insight – expanded version (SAI-E) (Kemp and David, 1997). Risk of violence was assessed with the HCR-20 (Webster et al., 1997). The MacArthur Admission Experience Survey was adapted to explore different dimensions of perceived coercion in relation to medication. Questions probed issues of influence, control, choice, freedom, and ideas regarding the patient’s perceptions of decision-making about taking medication (Gardner et al., 1993).
Participants were ultimately categorised into one of the following categories: competent consenters, competent treatment refusers, incompetent treatment refusers and incompetent assenters (those who agreed to take treatment but lacked capacity).
Competent treatment refusers were further assessed as to the likely consequences of any medication change. Their treating clinician was also asked about the likely impact of the proposed changes in terms of: expected duration of symptoms; severity of symptoms; side effects; days in hospital; utilisation of seclusion or restraint; risk of harm to self; and risk of harm to others. A five-point scale was used to rate the impact of respecting the patient’s medication choice.
The interview focused on the medication that was judged to be the patient’s main treatment for the disorder causing symptoms that resulted in the patient being a risk to others. This information was disclosed to the patient during the MacCAT-T interview together with standardised information about the nature, benefits and risks of the recommended treatment, and of the ‘no treatment’ option. A ‘no treatment’ alternative was chosen, rather than undertaking discussion about alternative medication from a similar class, to avoid raising matters that may have inadvertently undermined the participant’s treatment plan.
Forty assessments were rated by two psychiatrists observing the same interview to evaluate inter-rater reliability.
Statistical analysis
Data analysis was performed using the Statistical Package for the Social Sciences (SPSS version 15). Conventional bivariate statistical procedures were used.
Two-sided p-values with α = 0.05 are reported.
Results
Participant recruitment and bias evaluation
A total of 177 of the 206 (85.9%) forensic patients under the care of the Auckland and Wellington services were eligible to participate and 109 (61.6% of those eligible) agreed to take part, somewhat more than a quarter of the national forensic inpatient and community population. A comparison of participants and eligible non-participants revealed no statistically significant differences in terms of sex, ethnicity, age, legal status or treatment setting, suggesting no evidence of a participation bias (Table 1).
Assessment of participation bias.
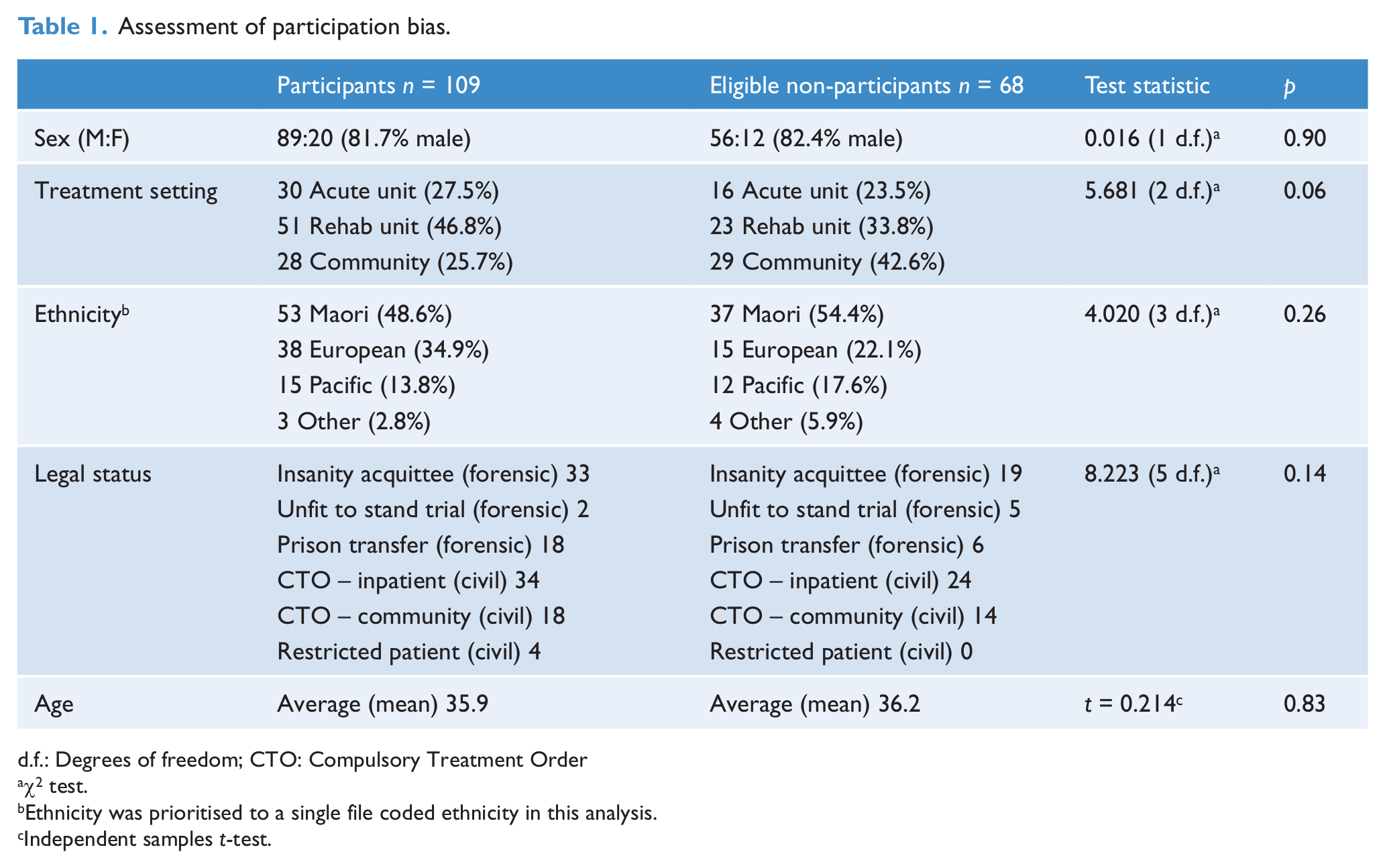
d.f.: Degrees of freedom; CTO: Compulsory Treatment Order
χ2 test.
Ethnicity was prioritised to a single file coded ethnicity in this analysis.
Independent samples t-test.
Participant characteristics
The 109 participants had a mean age of 37.2 (standard deviation 10.1) and were predominantly male (81.7%). A total of 52% of participants identified themselves as Maori, 45% European and 15% Pacific Nations (multiple ethnicities could be endorsed by participants, whereas ethnicity was prioritised to a single file coded ethnicity for eligible non-participants as reported in Table 1).
A violent index offence was recorded for most participants (83.5%), which was murder in 21.1% of cases. There were 32.1% under forensic orders (called ‘special patients’ in New Zealand), following a finding of insanity or of being unfit to stand trial. A further 16.5% were also ‘special patients’ after transfer from prison under the MHA. Some 3.7% were restricted patients (civil patients deemed to present special risks of harm to others). All others (47.7%) were detained under non-forensic (civil) orders, which are also dispositional options on conviction, on a finding of insanity or unfitness to stand trial, or on later reclassification from forensic to civil status. All were under treatment by forensic mental health teams.
A total of 74.3% of participants were resident in inpatient units at different levels of security, but 25.7% were resident in community housing with various levels of professional support, up to on-site professional staffing 24 hours per day.
Most participants (68.8%) were welfare beneficiaries and did not undertake any paid employment; 25.6% of inpatients and 10.9% of outpatients received income from salary or wages of some sort, most of which was supported work provided specifically for mental health service users.
The majority of participants (89.0%) had a primary diagnosis of a psychotic disorder (76 schizophrenia, 18 schizoaffective disorder, two delusional disorder and one psychotic disorder not otherwise specified), though many had secondary diagnoses such as personality disorder.
The medication discussed for the purpose of the MacCAT-T assessment was the participant’s primary antipsychotic or mood-stabilising medication. Clozapine, olanzapine, risperidone or quetiapine accounted for 92% of all primary medication.
Overall, 64.8% were assessed as competent consenters. This group included some competent participants whose agreement to take treatment was apparently more related to their desire for early release than to their analysis of the risks and benefits of treatment as such. A total of 13.0% were incompetent treatment assenters, 2.8% were competent treatment refusers and 19.4% were incompetent treatment refusers. The majority of study participants (67.6%) had treatment-related decision-making capacity. Beyond the acute phase of recovery, no differences in capacity to consent were identified between patients resident in the community and those in hospital.
Correlates of capacity
Demographic variables examined included age, sex, ethnicity, employment, marital status, legal status, education and place of residence (Table 2).
Demographic and clinical correlations with capacity.
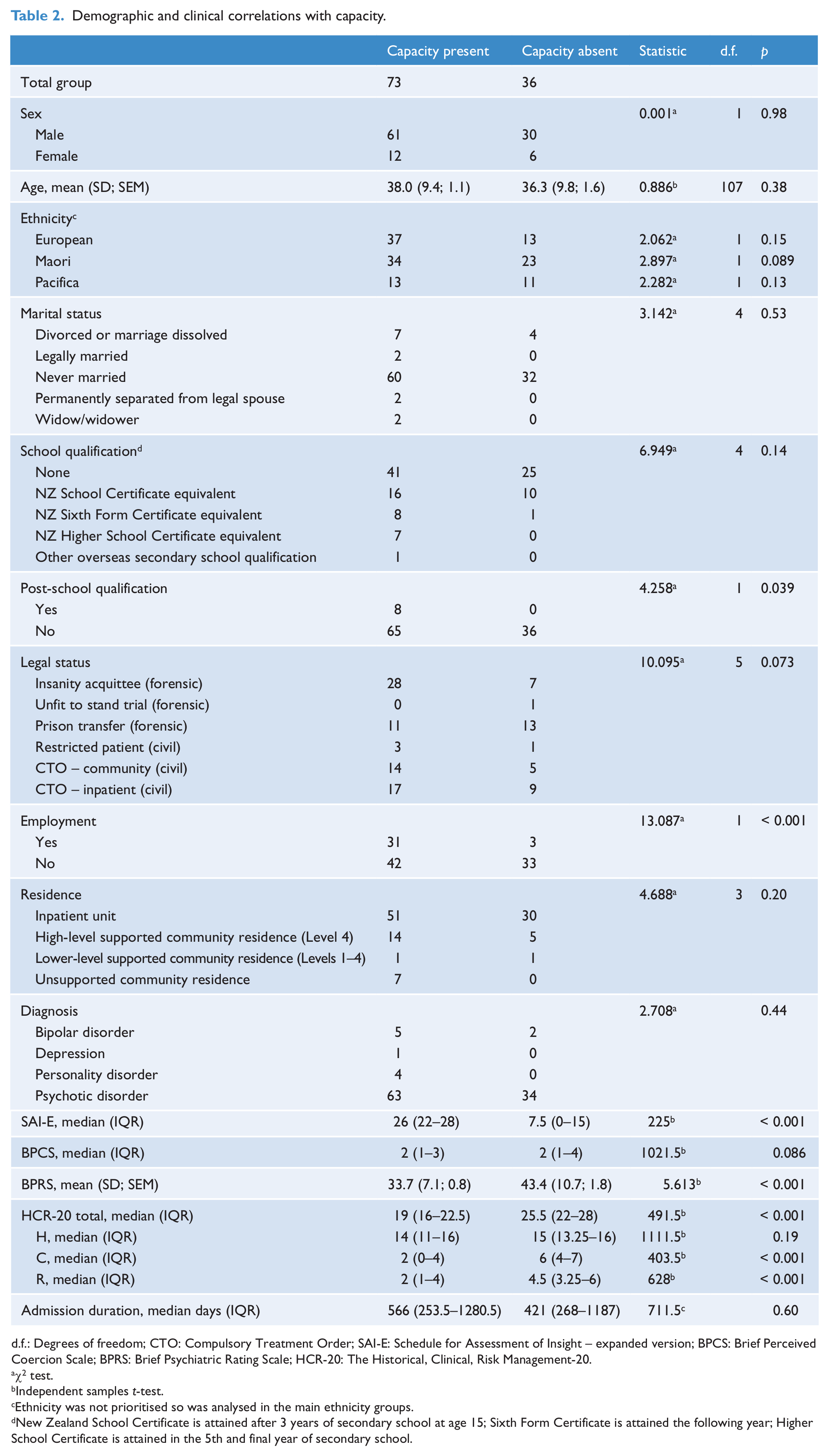
d.f.: Degrees of freedom; CTO: Compulsory Treatment Order; SAI-E: Schedule for Assessment of Insight – expanded version; BPCS: Brief Perceived Coercion Scale; BPRS: Brief Psychiatric Rating Scale; HCR-20: The Historical, Clinical, Risk Management-20.
χ2 test.
Independent samples t-test.
Ethnicity was not prioritised so was analysed in the main ethnicity groups.
New Zealand School Certificate is attained after 3 years of secondary school at age 15; Sixth Form Certificate is attained the following year; Higher School Certificate is attained in the 5th and final year of secondary school.
The only demographic variable that differed significantly (p < 0.001) between those with and without capacity was employment.
Diagnosis, admission duration (for inpatients) and perceived coercion did not differ between those groups. However, participants without capacity scored significantly higher on the Brief Psychiatric Rating Scale (BPRS) total score (p < 0.001), with significantly elevated individual items including bizarre behaviour, conceptual disorganisation, emotional withdrawal, motor retardation, tension, distractibility and motor tension.
Some positive symptoms, such as hallucinations, were not associated with incapacity while others, such as delusions, showed a tendency to significance. Conceptual disorganisation was strongly correlated with mental incapacity. Of negative symptoms, only emotional withdrawal and motor retardation were correlated with incapacity, while depression and mood elevation were not strongly correlated. However, these symptoms were uncommon and therefore statistical power may have been lacking.
Insight was strongly correlated with capacity. Receiver operating characteristic (ROC) curve analysis revealed area under the curve (AUC) values of 0.86 to 0.90 for the different sub-domains of insight, while the overall insight AUC was 0.92 (95% CI 0.87–0.98), which yielded a sensitivity of 0.92 and a specificity of 0.78 using a cut-off score of greater than or equal to 16 on the SAI-E.
All MacCAT-T sub-domains except ‘Expressing a Choice’ strongly predicted capacity status. Using a ROC analysis, ‘Appreciation’ had the highest AUC at 0.95, ‘Reasoning’ and ‘Understanding’ were similar at an AUC of 0.89 and 0.92, respectively, while ‘Expressing a Choice’ was barely better than chance correlation at 0.59. Using a cut-off score of greater than or equal to 2.5 on the ‘Appreciation’ sub-domain alone, 85% sensitivity and 86% specificity in capacity status was achieved. Similar but not quite so impressive sensitivity and specificity were achieved with reasoning and understanding sub-domains.
Logistic regression was used to assess the contribution to capacity status from statistically significant clinical variables (SAI-E; BPRS activation, depression/anxiety, and negative symptoms clusters; and HCR-20 clinical and risk management items), and to determine the effect size of the independent variables on the dependent. A forward stepwise (conditional) procedure was used. The most powerfully discriminating variable was the SAI-E, which yielded an R2 value of 0.67, suggesting that 67% of the variance in capacity status depended on insight. Further power was added to the regression equation when the BPRS activation cluster was added (model R2 value of 0.75), and a three-factor model with the BPRS depression/anxiety cluster also included yielded an R2 value of 0.78 (p < 0.001). Other variables failed to add significantly to the discriminant power of the regression equation.
Treatment refusal
A total of 23.1% of participants indicated to the interviewing researcher that, if it was up to them, they would not take the prescribed treatment, even though in many cases they were not complaining about their treatment to their responsible clinician. These ‘treatment refusing’ patients were statistically more likely to be judged to lack capacity (see Discussion).
There were 2.8% of study participants identified as competent treatment refusers. They comprised two men and one woman. All were insanity acquittees: two on a charge of murder and one of attempted murder. All three were inpatients. One suffered from schizoaffective disorder, one from schizophrenia and one from delusional disorder. All were prescribed antipsychotic medication. In all three cases reducing or stopping medication was predicted to have minimal impact on symptomatology, side effects, management and risk during the ensuing year, assuming the participant remained in hospital. However, the risk of relapse and of future violence was predicted to be significantly higher without treatment in the community and, in the context of third party risks, a conservative approach to enforcing treatment in hospital was recommended by the treating clinician.
A total of 4.6% of participants were competent consenters who would have refused treatment if it were entirely over to them. However, these patients understood that treatment refusal was futile in the context of their forensic order, and saw adherence as the only sensible option to secure release. Some were returning to prison where they knew treatment could not be enforced. It is likely that the number of such cases is an underestimate as some participants said they did not feel comfortable disclosing their reservations about treatment to researchers.
Thirty-nine of the 40 assessments rated for reliability by two psychiatrists were in agreement on capacity status (κ = 0.947).
Discussion
Principal findings
The majority of participants in this study (66%) had treatment-related decision-making capacity. Although a non-forensic population may differ, these results suggest that in jurisdictions where most patients under mental health legislation are beyond the acute admission phase of treatment and on community treatment orders, as is the case for two-thirds of compulsory patients under New Zealand’s MHA, decision-making capacity may be common.
Notably, participants without capacity in the present study performed relatively poorly on the ‘appreciation’ MacCAT-T items, often because they failed to appreciate that their disorder may lead to risk to others, and that their treatment was in part directed at that risk. In many cases, this was despite accepting that for other patients with a similar mental illness there may be an issue with risk to others (and as a result scoring well on the ‘understanding’ items). It might be surmised that the most challenging and psychologically threatening aspect of appreciating one’s illness and treatment needs as a forensic patient is the extent to which one appreciates the impact of one’s illness on others. However, risk of harm to others is by no means an exclusively forensic issue (Buchanan, 2010). In New Zealand, 54% of civilly committed patients are detained at least in part on these grounds (Ministry of Health, 2007).
While previous research tends to associate incapacity with psychotic rather than non-psychotic diagnostic groups (Okai et al., 2007), there is wide variation reported in populations with schizophrenia (Jeste et al., 2006). However, lack of capacity is more robustly associated with specific symptoms and severity of psychopathology. Our findings, that certain symptoms and symptom clusters, but not diagnoses, were associated with incapacity, are congruent with this literature. Although correlations with positive, excitement and cognitive Positive and Negative Syndrome Scale (PANSS) factor scores are often reported (Beckett and Chaplin, 2006; Howe et al., 2005), generally, as here, these are not found with negative symptoms or depression in psychotic populations.
The finding that socio-demographic variables generally did not predict capacity is consistent with most previous research (Okai et al., 2007). However, there was an indication that when variables were linked directly or indirectly with cognitive performance, such as work function or academic performance, they had a weak relationship with capacity, reflecting some overlap in the cognitive demands of these different tasks.
Another key finding was the importance of insight to mental capacity in this sample. Two-thirds of the variance in capacity status could be predicted by the SAI-E alone, with only an additional 10% of variance in capacity status achieved by adding other significant clinical variables to the regression equation. Further, of all the MacCAT-T sub-domains, that of ‘appreciation’, which is conceptually related to insight, was the most highly correlated with capacity. This is consistent with other work (Capdevielle et al., 2009), suggesting a remarkable degree of agreement between these clinical and legal concepts in this patient group. Much of the association appears related to conceptual overlap in the way these constructs are defined, and to procedural difficulties that make teasing them apart very difficult.
Overall, lack of insight in terms of appreciating the extent to which a participant’s illness may lead to third party risks was a pivotal issue for these participants. In many cases, this argument was used to justify the use of compulsion: if the patient fails to appreciate third party risks, there can be no expectation that they will take responsibility for managing these risks, and they may consequently be found to lack decision-making capacity. By this reasoning, clinicians may equate lack of insight into risk to others with the patient’s lack of competence to consider their own treatment.
Participants who refused treatment were significantly more likely to be found to lack mental capacity. Similar results have been obtained from several other studies (Okai et al., 2007). The most likely reason for this finding is the higher capacity threshold inevitably applied in circumstances of treatment refusal. We were left with the strong impression that some forensic patients said they were willing to accept continuing treatment only because they thought this response was vital to their prospects of liberty. On giving this response, however, they were more likely to be judged competent treatment consenters. If they had refused, they would have been judged incompetent to make that choice. Accordingly, assessing the effect of coercion on apparent consent – and on capacity assessment – was an important underlying issue.
It is suggested that a different methodology would be required to more completely understand the motivation for forensic patients agreeing to take treatment. In reality it may only be possible to retrospectively assess the patient’s true motivation after their circumstances have changed and coercion is no longer applied.
These results should serve as a reminder to forensic clinicians seeking informed consent from their patients that there are unavoidably coercive elements associated with compulsory treatment in forensic settings that may affect patient choice, capacity threshold and judgements of mental capacity. Even though treating patients in a procedurally fair and respectful manner can reduce perceived coercion and promote autonomy and choice, it is important to realise that what appears to be competent consent may be entirely the product of concerns about a patient’s liberty. Although the coercive nature of the forensic environment should not automatically invalidate consent, it would appear wise in seeking informed consent from forensic patients to pay special attention to the interplay between perceived coercion, patient choice and capacity threshold in determining capacity.
This study provides some evidence that a small number of forensic patients with capacity will refuse treatment even if their liberty is at stake. This is consistent with the practice whereby some forensic patients issue advance directives stating a preference for no psychotropic medication under any circumstances. However, methodological shortcomings in this study prevent a definitive comment on how long this position would be maintained if detention became prolonged, and release was conditional on compliance. Nevertheless, because of the limited numbers, the risks of permitting treatment refusal by patients with capacity might be seen as manageable, and it may be considered that the disadvantages of that outcome are outweighed by the advantages of promoting patient autonomy if capacity principles are fully respected.
Finally, these results would suggest that if the detention of forensic patients is driven by capacity status, it may not be possible to maintain a compulsory treatment order beyond the acute phase of illness. The same point would apply to civilly committed patients in general psychiatric settings. In a forensic context, however, respecting refusals by patients with capacity may render long-term prison-to-hospital transfers problematic. Moreover, courts may be unwilling to consider therapeutic dispositions if restoration of capacity, rather than risk reduction, terminates an order and leads to early release.
Strengths of the study
This study is one of the few studies to explore capacity to consent to treatment in forensic populations, and there are even fewer of community-based populations under mental health orders. The representative nature and significant size of the study sample give some confidence that we can generalise these findings to at least the national level. Further, the current sample is clinically similar to cross-sectional forensic populations reported elsewhere in terms of diagnosis and risk profile (Rutledge et al., 2008), but is less symptomatic than acute admission populations (e.g. Cairns et al. 2005: overall mean BPRS score was 45.28, compared to 36.94 in the present study). Importantly, the cross-sectional design employed in this study allowed exploration of capacity status beyond the acute phase of illness. If an association between capacity and psychopathology is accepted, capacity findings derived from acutely admitted populations should not be generalised to populations detained beyond the acute admission phase, such as forensic and community-based patients.
In line with previous work, a high degree of inter-rater reliability regarding the binary determination of capacity was found when two psychiatrists assessed the same interview (Okai et al., 2007).
Limitations and future research
Our cross-sectional methodology tended to focus on patients in long-term care, not the position of forensic patients at the point of admission. Further, because the current study was based on a single assessment, fluctuations in mental capacity may have been overlooked. The stability of mental capacity findings has previously been highlighted as an important issue (Dawson and Kampf, 2006), and future research may usefully explore this.
More generally, our results are derived from a specific forensic population. The extent to which they can be generalised beyond this context is unclear. However, they provide a provisional basis for further work in longer-term compulsory care settings outside forensic services. Our methods were not able to determine whether patients with capacity who wished to refuse treatment would maintain such a refusal if that would prolong their loss of liberty.
Policy implications
Assessments of capacity to consent to treatment appear no less reliable or valid in a forensic context than in other mental health settings, but certain assessment issues require special consideration. We suggest that in policy and regulation, when consent is at issue in the context of forensic treatment, it should perhaps be framed in terms of ‘assent’ or ‘agreement’ rather than ‘consent’ because consent in medicine usually means voluntary agreement on the part of the patient. Our evidence suggests that the coercive (and non-voluntary) elements of forensic settings may affect patient choice, capacity threshold and judgements of mental capacity. Further, where third party risks are at stake, assessors need to pay particular attention to the extent to which these risks are competently addressed by patients, as this is likely to be a critical capacity limiting issue for many patients. The relevance of these issues may well extend to a general mental health context, particularly where civil patients are detained on the basis of third party risks.
Finally, while changing to a capacity-based legal approach may alter treatment for some forensic patients, we found no evidence to support the proposition that increased risks to third parties would commonly arise, as very few forensic patients with capacity actually refused treatment in this study. However, this will not necessarily permit early release of forensic patients, whose detention is governed in part by a criminal justice agenda of proportionality and in part by a political agenda, which requires balancing public and victim interests with those of the forensic patient.
Footnotes
Acknowledgements
The authors wish to thank Drs Richard Worrall and Blair Leslie for their considerable assistance with data collection.
The work was carried out at the following institutions: Auckland Regional Forensic Psychiatry Services, Waitemata District Health Board, Avondale, Auckland, New Zealand and Central Regional Forensic Service, Porirua, New Zealand.
Funding
This study was supported by funding of $20,000 from the New Zealand Ministry of Health.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.