
Abstract
Objective:
Innovative models of care for people with a severe mental illness have been developed across Australia to more effectively address comorbidity and disability by enhancing the collaboration between clinical and non-clinical services. In particular, this review paper focuses on collaboration that has occurred to address comorbidities affecting the following domains: homelessness; substance addiction; physical ill-health; unemployment; and forensic issues.
Method:
The identification of relevant collaborative care models was facilitated by carrying out a review of the published peer-reviewed literature and policy or other published reports available on the Internet. Contact was also made with representatives of the mental health branches of each Australian state and territory health department to assist in identifying examples of innovative collaborative care models established within their jurisdiction.
Results:
A number of nationally implemented and local examples of collaborative care models were identified that have successfully delivered enhanced integration of care between clinical and non-clinical services. Several key principles for effective collaboration were also identified. Governmental and organisational promotion of and incentives for cross-sector collaboration is needed along with education for staff about comorbidity and the capacity of cross-sector agencies to work in collaboration to support shared clients. Enhanced communication has been achieved through mechanisms such as the co-location of staff from different agencies to enhance sharing of expertise and interagency continuity of care, shared treatment plans and client records, and shared case review meetings. Promoting a ‘housing first approach’ with cross-sector services collaborating to stabilise housing as the basis for sustained clinical engagement has also been successful.
Conclusions:
Cross-sector collaboration is achievable and can result in significant benefits for mental health consumers and staff of collaborating services. Expanding the availability of collaborative care across Australia is therefore a priority for achieving a more holistic, socially inclusive, and effective mental health care system.
Introduction
The 2007 Australian National Survey of Mental Health and Wellbeing estimated that approximately 3.2 million Australians aged 16–85 years, experience a mental illness in a 12-month period (Australian Bureau of Statistics, 2008). For most people, symptoms resolve independently or with minimal intervention, whereas for a smaller proportion symptoms are more severe and persistent, impairing multiple aspects of functioning. While definitions of severe mental illness (SMI) vary, approximately 3% of adult Australians experience a SMI (Commonwealth of Australia, 2009), determined by the type of illness, intensity of symptoms, length of illness and degree of disability caused. Most people with a SMI have schizophrenia or bipolar disorder, with the remainder primarily presenting severe depressive or anxiety disorders.
The vast personal and community cost stemming from SMIs was demonstrated in two reports (Access Economics, 2002, 2003). It was estimated that the real financial costs that included direct (e.g. health system costs, medical and other clinician expenditure, residential care, and pharmaceuticals) and indirect costs (e.g. lost earnings due to unemployment or premature death, carer costs, welfare support payments, and the involvement of prisons, the police, and the legal system) totaled AUD$1.85 billion for schizophrenia in 2001 and AUD$1.59 billion for bipolar disorder in 2003.
The reason for the significant cost burden is that despite intensive treatment and therapy, having a SMI can be a lifelong issue and can impact on multiple areas of quality of life and attainment of educational, occupational, and social roles (Gunatilake et al., 2004). These factors include an increased risk of suicide (Kooyman et al., 2007), lowered motivation to participate in leisure, vocational, or social roles (Velligan et al., 2006), and impaired memory and reasoning plus impulse control issues (Bowie et al., 2010). Aggression and violence risk is also increased in some mental illnesses (Barlow et al., 2000; Lamb and Weinberger, 2011), along with homelessness (Folsom et al., 2005; Mental Health Council of Australia, 2009), comorbid alcohol or other drug misuse (Australian Bureau of Statistics, 2008; Lai and Huang, 2009), poor physical health (Coghlan et al., 2001; McDermott et al., 2005), and forensic issues (Lamb et al., 2002; Ogloff et al., 2007). Experiencing these comorbidities also complicates the efforts to treat psychiatric symptoms.
The level of disability in Australians with a SMI was recently demonstrated. A study published in 2007 found that of 347 adults with schizophrenia, only 11% were in paid employment and 13.2% were educated beyond a high school level (Kulkarni et al., 2007). A study published in 2008 found that of 176 adults with bipolar I disorder, 32% had been hospitalised in the past 3 months, 22% were unemployed, 53% were not in a romantic relationship, and only 34% reported good to very good enjoyment of recreational activities (Kulkarni et al., 2008).
In light of the often comorbid difficulties and complex care needs experienced by people with a SMI, multiple formal and informal sources of support can be accessed (Figure 1). Public mental health services often lead in the delivery of clinical care (focused primarily on managing psychiatric symptoms), while also providing the primary crisis and acute psychiatric response via a hospital (e.g. acute inpatient unit) or community-based services (e.g. mobile crisis assessment and treatment services). Private inpatient and outpatient services are available along with primary care services, in particular general practitioners (GPs), who coordinate the management of less severely unwell people or monitor broader physical health. Non-governmental mental health services have played an increasing role in offering centre- or home-based services to help people achieve recovery and social participation goals. Specialist employment, education, housing, or justice agencies may also either be referred people with a SMI to address specific difficulties, or may identify users of their services who are experiencing the symptoms of a mental illness and need input from specialist mental health services.
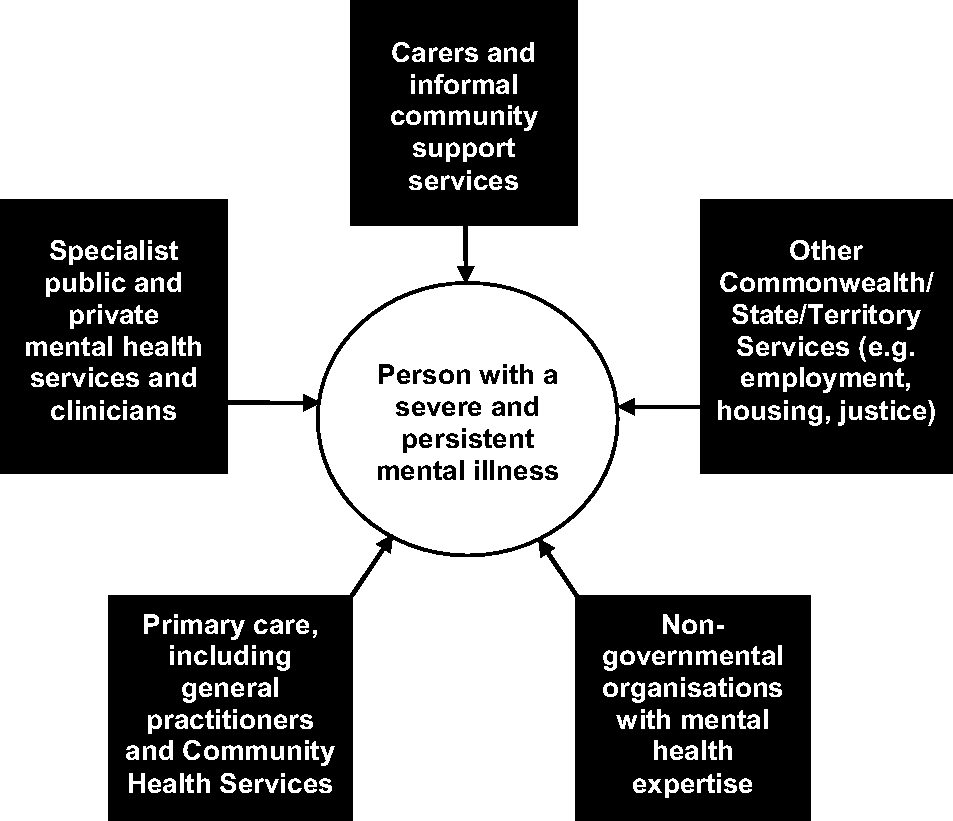
Systems and services that can support people with a severe mental illness.
Difficulty performing tasks of daily living often means that carers (family or friends) must assist with these tasks. Carers and other community groups (e.g. sporting clubs) therefore form a significant informal support network for people with a SMI. A previous report estimated that individual carers contributed on average 104 h per week caring for someone with a mental illness, often with little formalised training (Mental Health Council of Australia, 2000). The capacity to maintain community living for many people with a SMI is therefore dependent on the well-being, capacity, and willingness of carers to continue providing care.
Despite the potentially large number of resources available, many people with a SMI and their carers have struggled to access the right care at the right time. The 2005 Not for Service report presented feedback from an extensive series of stakeholder consultations (Mental Health Council of Australia, 2005). It was concluded that ‘… the available evidence suggests that persons with mental illness still struggle on a daily basis to access appropriate health care or be treated with respect or dignity when they do enter our health care systems’ (Mental Health Council of Australia, 2005: 15). Multiple stakeholders have highlighted particular difficulties with access to acute care, continuity of care, and the availability of rehabilitation (Morgan et al., 2012; Whiteford and Buckingham, 2005), as well as a lack of respect or dignity shown by some mental health professionals (Mental Health Council of Australia, 2005). A reluctance from some mental health staff to assess for, and provide support or referral to specialist services to address such comorbid issues as unemployment or addiction, has also been reported (Mental Health Council of Australia, 2005). This means that if a consumer wants to work or address substance issues, they or their carers often must negotiate for referrals to occur. A lack of coordination between services often supporting the same people, has also been identified (Gerrand et al., 2007). In many cases this is related to a lack of knowledge about the involvement of other services, or different approaches to providing care (e.g. harm minimisation compared with abstinence of psychiatric symptoms) that create barriers to integrated care (Todd et al., 2002).
In part stemming from the receipt of such feedback, new Australian models of care have been implemented to enhance cross-sector collaboration. The aim of the current review paper was to identify Australian collaborative care models for adults with a SMI, with a particular emphasis on models that have addressed comorbidities to SMI, to demonstrate key principles needed to promote collaborative care.
Method
The identification of eligible collaborative models of care occurred via a process of consultation with key national stakeholders as well as a process of reviewing published peer-reviewed journals and policy or project report publications. The initial phase of consultation involved a discussion between two project groups that included representatives from the Mental Health Reform Branch of the Australian Government, the Department of Health and Ageing, and the National Advisory Council on Mental Health. There was also representation from carer and consumer advocacy services, public and non-governmental mental health services, and from research groups. A second phase of consultation involved a discussion with representatives from the Australian State and Territory Department of Mental Health to assist in identifying innovative models of collaborative care within their jurisdictions. To conduct this, a list of representatives in each state and territory was provided by the Mental Health Reform Branch. The primary author then conducted a phone interview either with the representative or a nominated alternative to gather verbal or written feedback regarding suitable models.
Supplementing this stakeholder consultation, a literature review was used to broaden the scoping of suitable Australian collaborative care models. The following search engines or databases where used to search the literature: Google (www.google.au); PsycINFO (www.apa.org/pubs/databases/psycinfo/index.aspx); and PubMed (www.ncbi.nlm.nih.gov/pubmed). Search terms used included ‘Australian’; ‘collaborative’; ‘integrated care’; and ‘mental health’. More targeted search terms relating to key comorbidities included ‘employment’; ‘forensic’; ‘homelessness’; ‘housing’; ‘physical health’; and ‘substance’. A second phase of literature searching was conducted to seek and access reports relating to identified collaborative models that discussed in greater detail components of each model, and evaluation data demonstrating model efficacy. Where necessary, this included liaison with project contacts if prepared reports were not publicly available.
In selecting the final collaborative models to include, the primary determinants were that the models:
were delivered by Australian services to adults with a SMI;
involved collaboration between public mental health services and either non-governmental mental health services or other cross-sector agencies; and
had been evaluated or reviewed in some capacity to enable some comment on model effectiveness.
Findings
Collaborative care to be grounded in promoting recovery
Early in the consultation phase it became clear that a motivator for collaborative care was the capacity for recovery in people with a SMI. A recent review which asked ‘Is recovery possible?’ reported on findings from 15- and 25-year longitudinal studies of people with schizophrenia, finding that between 41% and 48% of patients were rated as being in recovery when followed up (Bellack, 2006). While definitions of recovery have varied, primarily they reflect a capacity to achieve improvements in symptoms, engagement in productive (e.g. work or study) and recreational activities, and familial and peer relationships (Warner, 2009). The process of recovery is also in most cases associated with a subjective experience of hope, empowerment, and a belief that symptoms and difficulties experienced can be coped with or overcome (Liberman, 2008). ‘Principles of recovery oriented mental health practice’ have also been incorporated within the Australian National Standards for Mental Health Services 2010 (Commonwealth of Australia, 2010). With many people with a SMI experiencing multiple difficulties, no single service in isolation has the expertise to optimise each person’s recovery. This requires involvement of services with complementary expertise to work in a coordinated manner to help each person define and work to achieve their own goals.
Carers and consumers to have a stronger say in how collaboration occurs
A second factor identified as being key to how collaboration occurs, was the need for mental health consumers and carers to have a stronger voice or involvement in decisions about treatment options or referrals to collaborating services. Consumers have often reported experiencing a lack of choice being offered to them about options for treatment or therapy, or mental health professionals not asking about or supporting efforts to achieve the consumer’s own goals (Bradshaw et al., 2007; Goodwin and Happell, 2006; Mental Health Council of Australia, 2005). Carers have reported not being provided with sufficient information about a consumer’s mental illness or treatment or how best to provide them with care (Gray et al., 2008; McAuliffe et al., 2009; Mental Health Council of Australia, 2000). Carers and consumers expressed that as the ones living with the mental illness and its consequences, they were the experts in what treatments or therapies helped or did not help, what were the warning signs or markers of relapse, and what were the motivators for change. Both consumers and carers (with the consent of consumers) wanted to be involved in determining what collaboration occurred and what goals were being worked towards.
Collaboration to promote housing stability
Demonstration of need
The need to address homelessness or housing instability as a comorbidity of SMI has recently been highlighted. A study of 210 people living in primary homelessness in inner Sydney found that 75% had at least one mental disorder (Teesson et al., 2004). A study of people in marginal accommodation in inner Melbourne found an estimated lifetime prevalence of a psychotic disorder of 42% (compared to approximately 1% in the general population), accompanied in most cases by persistent disability despite public mental health service involvement (Herrman et al., 2004). The implications of homelessness for engagement with mental health care have also been demonstrated. In a sample of 142 people case managed by a Victorian public mental health service, 48% had spent at least 1 day in a homeless setting in the past 12 months, with homelessness reducing service engagement (Holmes et al., 2005b). Insufficient income, lack of employment or suitable housing, drug or alcohol addiction, insufficient education or training, and having a mental health condition have all been reported as the major reasons for people with a mental illness either losing housing or continuing in homelessness (Mojtabai, 2005). Addressing the causes and sustainers of homelessness concurrently with psychopathology is therefore important to improve the overall outcomes.
Model review
A number of models were identified that adopted a ‘housing first’ approach to stabilise housing before providing clinical, psychosocial, and tenancy support. The Housing and Accommodation Support Initiative (HASI) in New South Wales (NSW) (Muir et al., 2007), Project 300 in Queensland (Meehan et al., 2011), the Independent Living Program in Western Australia (Smith and Williams, 2008), the Housing and Support Program in Queensland and Victoria, the Neami Community Housing Program in Victoria, and the South Australia’s Returning Home Program (Carter et al., 2008), are all examples.
HASI is the most rigorously evaluated supported housing model with stage 1 (first 100 participants) and 2 (895 participants) evaluation reports published (McDermott et al., 2011; Muir et al., 2007). Beginning in 2002/2003, HASI was jointly funded by NSW Health and NSW Housing, and provided permanent social housing, long-term community participation and housing support, and active mental health case management. Delivery occurred via a partnership between the HASI participant, their local public mental health service, a mental health non-governmental organisation, and a housing provider. The stage 1 report documented 2-year longitudinal outcomes for the first 100 participants (Muir et al., 2007). This found improved housing stability (85% remained with the same housing provider), increased community participation (43% were working or studying and 94% had established friendships), improved family connectedness, and improved social and living skills (69%). The annual cost per person was AUD$57,530 (inclusive of accommodation support, program management, and housing costs). This was offset by cost savings from an 84% reduction in costs of psychiatric admission or emergency department care, a 78% decrease in imprisonment, and a threefold increase in paid and voluntary workforce participation (Muir et al., 2007). Factors identified as underpinning model success were:
management and direct care staff shared an understanding and commitment to the partnership model;
staff understood roles and respected the skills and experience of partner services;
partners freely shared information (under a shared commitment to confidentiality) and met regularly to establish jointly developed support plans; and
consumers were centrally involved in establishing support plans and provided support to minimise tenancy risk.
Beyond models for people already identified as being at risk of housing instability, models in Victoria (Holmes et al., 2005a; Lee et al., 2010) and Queensland (Lloyd and Bassett, 2010) were identified that operated homeless outreach psychiatric services. In each model, collaboration occurred through regular co-location of public mental health service staff (e.g. nurses, psychiatrists, social workers, or occupational therapists) on-site at services accessed by people who were homeless (e.g. drop-in or crisis accommodation services). In one Victorian model, the welfare non-governmental organisations were also funded to appoint one mental health staff member. Shared formal and informal (e.g. via secondary consultation) education opportunities also enabled collaborating staff to learn from one another. Evaluation of one model (Lee et al., 2010) identified significant reductions in presentations to the crisis assessment team from clients of the non-governmental welfare organisations, and improved housing stability for participants engaged in case management. Key principles for engagement were reported as being a focus on the consumer’s goals (e.g. housing, linkage into support services, and regaining access to one’s children) that helped in establishing trust and a therapeutic relationship before trying to address the symptoms of mental illness. Challenges were also identified, in particular stemming from the limited availability of staff outside of normal business hours. Enhancing cross-sector communication (e.g. sharing of assessment outcomes or progress following referral) and knowledge of the capacities and resources available to each service that assisted in fostering professional respect were also needed.
Co-location of staff from a housing service within a public mental health service inpatient unit was a third identified approach. For the Housing Mental Health Pathways Program (HomeGround Services, 2008), the housing worker participated in inpatient unit staff meetings and either identified or was referred consumers with housing issues. Based on the complexity of the person’s needs, the housing worker was then able to either provide an assessment, referral, and practical support only, or short- to longer-term outreach (bridging support) to link the person into transitional housing or the housing service’s housing stock. A 12-month review conducted with 40 participants in 2005/2006, found that before admission 50% had been sleeping rough, 43% were in temporary accommodation, and 20% had experienced repeated episodes of homelessness for 5–10 years. At the end of the program support period, 7% had accessed private rental accommodation, 13% long-term public housing, 27% transitional or non-governmental organisation supported housing, and 23% crisis accommodation. Staff feedback highlighted that the co-location facilitated an improved working relationship between mental health and housing staff and the capacity for collaborative decision-making. However, the need for improved collaboration in following up consumers in the community, which was often complicated by a lack of a stable home to facilitate ongoing service engagement, remained an ongoing challenge.
Collaboration to enhance physical health
Demonstration of need
The 2001 Duty to Care report found that the death rate for people with a mental illness was 2.5 times that of the general population, due in particular to heart disease and suicide (Coghlan et al., 2001). The use of medical treatment in hospital was also lower than for the general population for illnesses of comparable seriousness, suggesting a reluctance to seek or access care for non-psychiatric medical illnesses, or else health providers only enquiring about and treating psychiatric symptoms.
The causes of elevated physical ill-health in people with a SMI have been extensively documented. Some medications (in particular atypical antipsychotics) can increase weight gain or impair metabolic functioning (Allison et al., 1999; De Hert et al., 2009). Poor engagement with general health care, poor diet, and limited physical exercise have also been proposed to increase medical morbidity (Morriss and Mohammed, 2005). Australians with a mental illness are also twice as likely to smoke as other Australians and smoke 16% more heavily (Access Economics, 2007), and have less appropriate diets (Leas and McCabe, 2007).
Despite the elevated risk for medical morbidity, improvements in health functioning have been found with some programs such as the Healthy Lifestyles Project, a multi-component risk factor intervention that found significant reductions at the 20-week follow-up in coronary heart disease risk, smoking, and weight for smokers with psychosis (Baker et al., 2009). Comprehensive metabolic monitoring protocols have also been introduced effectively into core business for some public mental health services (Organ et al., 2010). This provides evidence that improvements in physical health can be achieved.
Model review
HealthRight established a trial of a Peer Advocacy and Support Service to improve GP engagement and reduce the presence of health risk factors for people with a SMI (Bates et al., 2008). The model involved a partnership between two non-governmental organisations, two public mental health services, and a mobile medical primary care service, with a reference group established to oversee implementation and evaluation. Peer support workers were employed by the non-governmental organisations and received training from HealthRight staff, before offering co-located support to consumers of the clinical services. Key strategies involved liaising with the local divisions of general practice to find ‘mental health friendly’ GPs, enhancing the communication between public mental health service case managers and GPs, and the raising of awareness of physical health issues among case managers. Peer support workers assisted consumers in establishing achievable physical health goals, making and attending GP appointments, and liaising with case managers about progress. A 6-month review found that nine of 25 participants receiving peer support were helped to find a GP. Increased physical activity was reported by 20 participants, weight loss by eight, change in diet by seven, and five said they had stopped smoking. Success was facilitated by the inclusion of peer supporters in team meetings, ‘champions’ (e.g. senior medical staff) within the clinical services to promote the use of the peer support workers, and making staff from all partner services aware of the role of peer support workers and model successes.
A second reviewed model established a partnership between GPs and public mental health services in South Australia (Division of Mental Health Noarlunga Health Services, n.d.). The model established four phases of collaborative care for 60 public mental health service case-managed consumers, dependent on the stage of recovery. This varied from sole case management to sole GP care, with interim steps involving shared care or consultation to GPs providing care. Mechanisms to promote integration of care included the establishment of joint multidisciplinary care plans (funded through the Medicare Enhanced Primary Care items), enhanced opportunities for shared training and either face-to-face or phone consultation, and enhanced communication of mental health documentation (e.g. Transfer of Care form to communicate diagnosis, ongoing symptoms, early warning signs, and steps to maintain stability). Findings revealed that 30% of consumers were transferred to a less intensive mode of care and 57% of consumers were effectively managed in joint care with a GP. Reductions in psychiatric hospitalisations and emergency department presentations were also seen. With a number of participants treated with the antipsychotic clozapine, which requires intensive physical monitoring (Castle et al., 2006), another positive outcome was the success in managing clozapine patients in GP shared care. Similar models of shared care for the management of consumers on clozapine have also been implemented in other Australian states (Filia et al., 2012), highlighting the capacity for effective collaborative care between mental health and primary care services.
Collaboration to address substance addiction
Demonstration of need
The comorbidity of alcohol and other drug use in people with a mental illness has been extensively documented. The 2007 Australian National Survey of Mental Health and Wellbeing estimated that 17.6% of people with an affective disorder and 11.9% with an anxiety disorder had a comorbid substance use disorder (Teesson et al., 2009). In a sample of 643 patients treated for first-episode psychosis, 61.6% had substance abuse disorders at baseline (Lambert et al., 2005). At the 18-month follow-up, persistent substance abuse lowered the likelihood of remission, whereas remission was more likely with decreased or ceased substance. Substance comorbidity can therefore impact on treatment outcome. The impact of substance intoxication on presentations to Australian hospital emergency departments was also recently demonstrated. A study of 3702 mental health presentations to five Victorian emergency departments found that 39.1% were intoxicated, most commonly with alcohol (15.7%), benzodiazepines (7.1%), or amphetamines (2.2%) (Knott et al., 2007).
Providing a useful context, two studies surveying staff from mental health or alcohol or other drug treatment services have identified barriers to effective collaboration (Cleary et al., 2009; Kavanagh et al., 2000). Both staff groups wanted increased availability of dual disorder services or integrated models of treatment; however, a number of barriers to integration were identified. These included clients not being motivated to address their substance use, difficulties coordinating care across mental health and alcohol or other drug services, including who held duty of care, and difficulties with intersectoral communication. To address the issues with regard to communication, improved opportunities to exchange client information, developing shared treatment plans, conducting joint case conferences, and offering consultation when encountering an issue outside of care expertise, were proposed (Kavanagh et al., 2000). The routine implementation of comorbidity screening and education about identifying and responding to the comorbidity for staff from both sectors was also recommended. Attitudinal barriers held by some clinicians must also be addressed. Such beliefs as ‘addiction is not the business of mental health services’ have been reported (Todd et al., 2002: 795), which limit the ability and willingness of mental health clinicians to address substance issues in collaboration with addiction services.
Model review
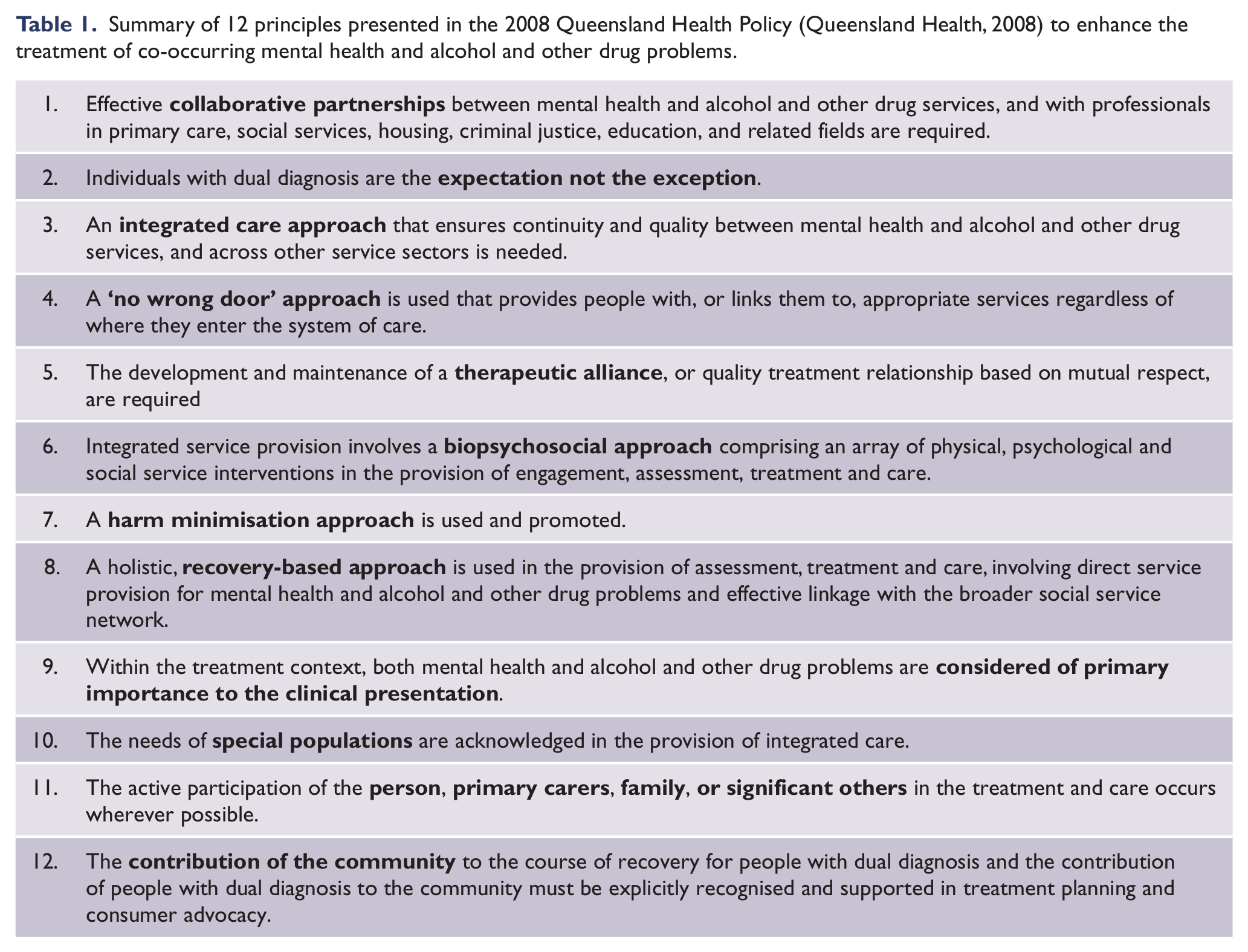
A statewide response was led by Queensland Health through the publication, in 2008, of the policy for the ‘Service delivery for people with dual diagnosis (co-occurring mental health and alcohol and other drug problems)’ (Queensland Health, 2008). Twelve principles, articulated to underpin the promotion of care for this population, are summarised in Table 1. Unfortunately, a formal evaluation was not completed, so the full impact of the policy implementation is unclear.
Summary of 12 principles presented in the 2008 Queensland Health Policy (Queensland Health, 2008) to enhance the treatment of co-occurring mental health and alcohol and other drug problems.
A statewide response that has been evaluated is the Victorian Dual Diagnosis Initiative with the acronym (VDDI). Beginning in 2001, the VDDI was jointly funded by the Mental Health and Drugs Policy and Services branches of government to build the capacity of alcohol and other drug, public, and non-governmental mental health services in managing dual diagnosis clients (Australian Healthcare Associates, 2011). This was achieved through the delivery of education, consultation, supervision and case reviews, network facilitation and partnership development, and organisational change management. An expanded role for the VDDI in 2005 saw the delivery of three new projects: the Reciprocal Rotations Project; Additional Psychiatric Support; and the establishment of an Education and Training Unit (Australian Healthcare Associates, 2011). A more detailed evaluation of the Reciprocal Rotations Project has been presented (Hasking and Sellars, 2008), allowing for a more detailed review. Available to staff from public and non-governmental mental health services and alcohol or other drug services, the project made provision for staff to have a 3-month placement in a service from another sector. Rotating staff members were seconded to a VDDI during their placement, and an experiential program was developed in conjunction with the staff member, the host organisation, and the VDDI. Rotation outcomes were assessed via a questionnaire completed with 29 rotation participants and 44 managers from the host or parent organisation. Significant improvements in knowledge, confidence, and skill in relation to the comorbid disorder were found. This suggested enhanced dual disability capacity following the rotation. A limitation to the reach of the Reciprocal Rotations Project was, however, identified (Australian Healthcare Associates, 2011). A telephone survey of Victorian agencies eligible for participation in the program found that 55% did not, at the time, have any staff who had participated, reported to be due in part to staff completing a rotation then later moving on. Ensuring mechanisms to promote sustainability of cross-sector collaboration is therefore important.
A review of 17 Australian services offering comorbidity treatment was found, although the reviewed models were primarily non-governmental alcohol or other drug or combined mental health and alcohol and other drug services and not public or specialist mental health services (Merkes et al., 2010). Most of the reviewed models reported being engaged in collaborating relationships with mental health treatment services (from which referrals were regularly generated). No comparison was made, however, of outcomes achieved via different collaborative arrangements preventing assessment of outcomes of individual models. Current evidence highlighting how effective collaboration can occur between mental health and addiction services is therefore limited, suggesting a need for further research.
Collaboration to enhance workforce participation
Demonstration of need
The 2003 Australian Survey of Disability, Ageing and Carers, found that in persons aged 15–64 years, a greater proportion of people with anxiety (46.1%) or affective disorders (51.6%) were not in the labour force compared to well controls (19.1%) (Waghorn et al., 2009a). Even greater levels of unemployment have been found for people with either a psychotic disorder (75%) or schizophrenia (81%) (King et al., 2006). This is not simply due to people with a SMI not being motivated to work. Many want to, but are not able to obtain competitive work (Marwaha and Johnson, 2005), highlighting an unmet need.
Internal and external barriers to workforce participation for people with a SMI have previously been documented (Bond and Drake, 2008; Marwaha and Johnson, 2005; Rosenheck et al., 2006). Internal factors include: experiencing psychiatric symptoms (e.g. amotivation, depression, positive and negative psychotic symptoms); cognitive impairments (e.g. impaired attention, memory or problem-solving); reduced educational attainment; and the presence of substance misuse or forensic involvement. External or systemic barriers have also been identified and include: stigma that leads to employers not taking on people with a mental illness; labour market pressures that limit the availability of suitable roles; and low expectations of health professionals not supporting participation in employment due to perceiving it as a potential stressor or else assessing the person as unable to work. Interventions that simultaneously address internal and external barriers are therefore needed.
Model review
Supported employment models have been identified as the most effective interventions to promote workforce participation for people with a SMI (Campbell et al., 2011; Crowther et al., 2001). This is over and above other models such as pre-vocational training, which assume that people with a SMI are not ready for employment participation so first develop workforce readiness. The core feature of supported employment models is that vocational specialists work alongside mental health clinicians in identifying and securing suitable employment, before offering support to the person and employer to address the barriers to employment sustainability. Examples were first implemented in North America in the 1990s, and in some cases have been supplemented by peer support workers to provide additional lived experience support to the client and mental health case managers (e.g. Mowbray et al., 1994).
Within an Australian context, Waghorn et al. (2009b) articulated seven principles (expanded to eight by Drake et al. 2012) underpinning evidence-based supported employment for people with a SMI (Table 2). A review of seven sites that delivered a supported employment program was recently conducted (Bond et al., 2007). One site (Orygen Youth Health) adopted a model that added a full-time employment specialist to one clinical service (Killackey and Waghorn, 2008). The remaining sites adopted a model partnering a public mental health service and either a specialist employment service or a non-governmental mental health organisation contracted to deliver disability employment services (e.g. Mental Illness Fellowship Victoria).
Eight evidence-based principles for supported employment services.
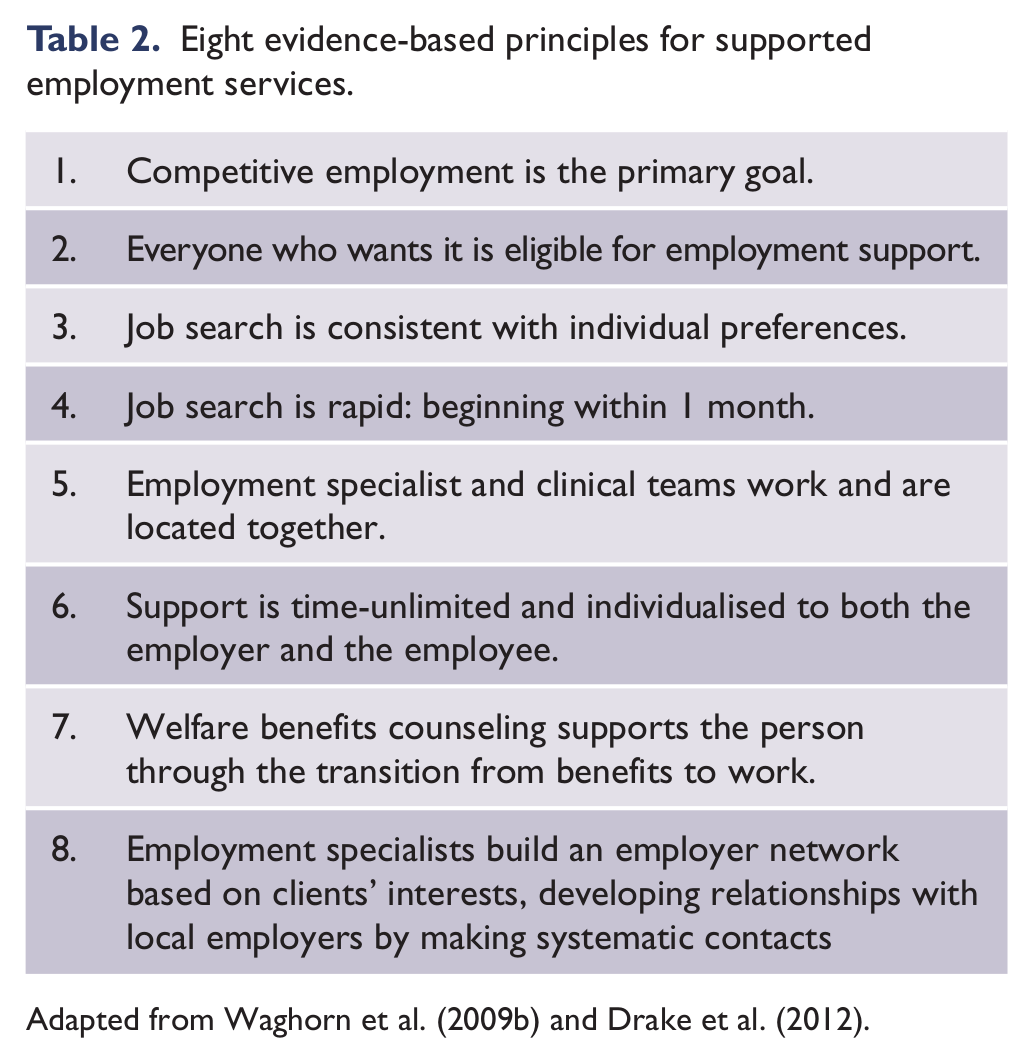
Adapted from Waghorn et al. (2009b) and Drake et al. (2012).
The most detailed published evaluation was from the NSW Vocational Education, Training and Employment (VETE) Service (Sherring et al., 2010). The model consisted of two occupational therapists employed by the public mental health service that acted as dedicated employment clinicians (not performing generic case management duties) and were responsible for liaising with consultants from three local employment services. VETE occupational therapists, situated within an early psychosis team, assessed consumers’ vocational abilities and needs, assisted consumers in accessing employment services, and provided clinical support (e.g. anxiety management, relapse prevention planning, social skills training, stigma and disclosure counseling, and dealing with cognitive deficits). Employment consultants performed all job search and preparation activities and negotiated with and provided on-site support to employers. VETE occupational therapists could also provide cognitive assessments in the workplace or mental health education to employers. Communication was facilitated through the exchange of assessment information, monthly case reviews, and regular joint appointments, as well as frequent updates on progress. Forty-three people participated during the 24-month evaluation. Thirty-three (77%) obtained competitive employment and 20 (47%) were still employed at the end of the evaluation period. This level of obtained employment is consistent with an international review of 11 randomised controlled trials of supported employment, which found that 61% of participants obtained competitive employment (Bond et al., 2008).
A number of barriers and facilitators to model effectiveness have previously been found. Leadership to challenge the way of thinking about the capacity of people with a SMI and embedding collaborative practice into routine care are particularly important (Waghorn et al., 2009b). The publication of partnership agreements that specify roles for partner services, and outline the expectations for communication, professional interaction, and participant throughput are also of importance for underpinning partnership accountability. Establishing zero-exclusion criteria for referral (e.g. anyone sufficiently motivated to want to find employment is offered support) and rapid communication pathways to communicate if there is a change in a consumer’s mental state, also improve the efficiency of cross-sector continuity of care. For co-location to be successful, adequate office space and resources (e.g. Internet, computer) must be available for co-locating staff, along with the capacity for co-locating staff to participate in team case discussions, have access and contribute to shared care plans, and retain professional supervision with colleagues from their core discipline (Bond et al., 2007). Consideration of funding models and the capacity to access disability employment and mental health funding streams is also important for model sustainability.
Collaboration to address forensic comorbidity
Demonstration of need
The symptoms of some mental illnesses, such as paranoia, impulsivity, thought disorder, and agitation, as well as comorbid conditions, such as personality disorders or substance abuse, can increase the risk of people with a SMI acting aggressively (Lamb and Weinberger, 2011; Volavka and Citrome, 2008). On some occasions, the level of risk results in police providing the first response (Lamb et al., 2002). The consequence can be excessive criminalisation of people with a SMI, or otherwise police officers who often have limited mental health expertise serving the role of gatekeepers to the mental health system (Lamb et al., 2004). Barriers to effective collaboration between the police and mental health services has also been identified, in particular related to the difficulty in accessing, communicating with, and transferring care to the interfacing service (Hollander et al., 2012). With a recent study finding that 19.7% of mental health presentations to a Sydney hospital emergency department were brought in by the police (Lee et al., 2008), models to enhance collaboration between the police and mental health services are sorely needed.
The significant level of mental illness in Australian correctional facilities was highlighted in a 2009 report (Australian Institute of Health and Welfare, 2010). Of 549 prison entrants, 37% reported having a mental disorder at some time, 18% a past history of self-harm, and 71% had used illicit drugs in the past 12 months. A NSW study screening 916 consecutive prisoners admitted to the state’s correctional facilities in 2001, found that 80% had any psychiatric disorder, most commonly a substance abuse disorder (66%), personality disorder (43%), or anxiety disorder (38%) (Butler et al., 2006). Post-release mental health care is also needed. A study of 13,667 people released from West Australian prisons in 1995–2001, found substantially higher risks of death following release than the general population, with the excess mortality principally due to alcohol and other drug addiction, or to injury and poisoning (Hobbs et al., 2006). Following release, 13% of prisoners required contact with or admission to a mental health service.
Model review
Two identified models, the Police, Ambulance and Crisis Assessment Team Early Response (PACER) and the Police Mental Health Intervention Team (PMHIT), focused on enhancing the collaboration between the police and mental health services.
PACER was informed by the ‘ride-along’ or outreach police-mental health models from North America (e.g. Lamb et al., 1995) and involved co-location of a crisis assessment and treatment team clinician and police officer that could be requested by frontline police officers to respond to people experiencing an acute mental illness. Co-location enabled immediate access to the police and mental health databases and immediate mental state and risk assessments to be completed, enabling more efficient access to treatment. The police officer could also maintain safety and be a primary liaison point with the frontline police officers. Findings from a 90-day pilot found that 279 requests for PACER were made, with 68% responded to on-site and the remainder via telephone (Victoria Auditor-General, 2009). The need for transportation to a mental health service was avoided in 11% of cases owing to PACER response and only 4% of cases required force. For the police, involvement with PACER improved their understanding of mental illness, which mental health clinicians reported as also resulting in fewer unnecessary callout requests. A number of challenges were identified. Primarily, these related to the limited operation of PACER (single unit operating an 8-h shift each day) and often multiple demands, imperfect information for decision-making, and differing service criteria and priorities.
Instead of adopting a primary police response delivered by mental health-trained police officers, the NSW PMHIT model was informed by North American Crisis Intervention Team models (Compton et al., 2008). Built on a funding partnership between the NSW police and NSW Department of Health, the PMHIT was staffed by clinicians and police, as well as policy and education officers (Laing et al., 2009). As of 2010, 300 officers had completed a mental health education package lasting four days with plans to train 10% of frontline police by 2015. An evaluation was completed in 2009 (Herrington et al., 2009). Qualitative data from trained police showed that training led to an increased use of de-escalation techniques by the police and an improved understanding of and confidence in dealing with people with a mental illness. NSW mental health staff had also observed improved police knowledge about mental illness and the ability to engage with people with a mental illness. Sharing of information between the police and mental health staff had also improved and self-reported data suggested that PMHIT-trained officers were spending less time in resolving mental health events than non-PMHIT-trained officers.
Beyond collaboration with the police, models were also identified in which mental health services collaborated with the justice system via court liaison services, inreach into prisons, or post-release support. Highlighted in a recent benchmarking project with four Australian forensic mental health services (Coombs et al., 2011), multiple court liaison services are currently provided. However, published evaluations were found only for the West Australian statewide mental health court liaison service (Brett, 2010; Brett and Blumberg, 2006). The aim of the model is to divert people experiencing a mental illness from court and to accelerate their access to care. The model is staffed by senior nurses authorised under the West Australian Mental Health Act (1996) to perform assessments and refer people to hospital for psychiatric assessment. Specialist assessment and opinions have successfully been delivered to remote court services via videoconferencing. To assist with case finding, evidence-based criteria (e.g. the defendant being held in custody overnight) has been used to more effectively target recipients of mental health assessments. The 2010 review found that case finding of mentally disordered offenders was effectively achieved, although it would be improved through increased routine use of mental health screening. Court diversion was also less effectively achieved for minor offenders, highlighting the need for police-led diversion programs to be targeted to less serious offences perpetrated by mentally disordered offenders.
Providing a framework for assessing models addressing SMIs in prisons, a set of core elements for mental health services in prisons was articulated by Ogloff (2002), These included: the capacity to screen for a mental illness (in particular, suicide risk) and provide crisis intervention; assessing for and treating an identified mental illness; and delivering institutional and post-release community planning and case management. Aligned with many of these elements was a Queensland youth detention centre model. Jointly funded by Queensland Health and the Queensland Department of Families, it delivered multidisciplinary care (psychiatry, psychology, social work, and alcohol and other drug) to adolescents remanded to the centre (Letters and Stathis, 2004). A full-time Indigenous health worker was also employed to provide culturally sensitive care. Awareness of mental health and substance issues was raised through the delivery of basic education about mental illness and substance abuse. The model also established links with the Child and Youth Forensic Outreach Service that engaged with identified young people while still in remand, where possible, to facilitate follow-up clinical care in the community. Between 2001 and 2004 a total of 946 referrals were received, of which 53% were for mental health, 10% for dual diagnosis (mental health and drug and alcohol) and 38% for drug and alcohol (Stathis et al., 2006). An increase in the referral rate for alcohol and drug issues was also achieved.
The Victoria statewide Forensic Mental Health Service (Forensicare) also operates an inreach service into the Melbourne Assessment Prison (MAP). All newly received prisoners undergo a medical assessment, and if mental health issues are identified, they are referred for a mental health assessment by a Forensicare nurse. Individuals in prisons needing a more thorough assessment may be admitted to the 16-bed multidisciplinary acute assessment unit (AAU) operated by Forensicare staff within the MAP. Short-term intervention and after-hours crisis intervention is offered. As a demonstration of use, between 1 July 2009 and 31 January 2010, 3276 mental health assessments were undertaken, 166 prisoners were admitted to the AAU, 158 crisis calls were attended to by psychiatric nurses, and 3.3 prisoners on average were managed in observation cells because of suicide risk (Forensicare, 2010). However, the lack of publication of any formal evaluation limits any determination of model effectiveness.
A number of models transitioning people experiencing mental illness from prison to the community were identified (e.g. Justice Health Connections Project in NSW and the Community Integration Program in Victoria); however, evaluations of these models were not found. One model for which some outcomes were described, involved a partnership between the Queensland’s Prison Mental Health Service and a non-governmental mental health organisation (Richmond Fellowship) to deliver a Transition Support Service (Evans and Stapleton, 2010). Clients receiving care coordination from the Prison Mental Health Service (inclusion criteria: active mental illness requiring case management in the community and at risk of homelessness or failed transition of care) could receive additional assistance from a Transition Support Service worker. The worker would meet the client and the Prison Mental Health Service transition clinician (who provides the clinical support) prior to release, to assess needs and goals following transitioning. A joint service plan is prepared and often a referral is made to the public mental health service in the area to which they are moving. Following release, the support worker visits the client weekly to monitor and review their goals/achievements. The model was reported to have produced ‘high’ engagement rates and client satisfaction survey results. A continued willingness to work collaboratively, built on mutual respect and understanding, was also reported. A more detailed evaluation is currently being completed to more robustly assess model effectiveness.
Summary
As the Australian mental health system continues to embrace community-based care that promotes recovery as intervention goals, greater integration of care between public and non-governmental mental health services, and cross-sector services is needed. The preceding review identified examples of Australian models of care that have involved cross-sector collaboration, with a particular focus on addressing the prominent comorbidities, which are often barriers to effective treatment of psychiatric symptoms and impair quality of life. Despite addressing often quite different comorbidities, a number of consistent factors that promoted or inhibited collaboration were identified.
Most of the identified models recognised that consumers and carers often want to address comorbid issues. An important first step in promoting recovery is therefore for mental health services to screen for and discuss with consumers how best to address identified comorbid issues. The need for collaboration also stemmed from services recognising that they could not address all issues of their clients in isolation. Another important factor was that while some models established novel partnerships to address specific comorbidities, many were built on pre-existing relationships between services, using a history of mutual referral or networking that enhanced collaboration.
At the government level, partnership between government departments (e.g. the joint funding of HASI by NSW Housing and NSW Health) promoted organisational collaboration through expanding access to resources (e.g. housing stock or the amount of available service delivery funding). In other examples (e.g. integrated homeless mental health initiatives), one government department was the sole funder, but provided funding to both the mental health and non-mental health services, with the proviso that the service was delivered in partnership. Actions from government can therefore motivate services to collaborate.
At the organisational level, clearly defining the respective roles and expectations for the delivery of collaborative models was important, as was establishing mechanisms to ensure accountability to model expectations. In many cases, memoranda of understanding or service agreements were documented to enable communication and the measurement of expected performance metrics (e.g. the number of cross-service referrals, education sessions provided, joint assessments performed, or expectations regarding communication or professional respect). Establishing model steering groups that reviewed performance against agreed metrics and provided a forum to present and resolve collaboration issues was also important.
At the clinician level, raising awareness of the need for addressing comorbidity, enhancing the knowledge of and the professional respect for the staff of collaborating services, and ensuring effective communication were particularly important factors. Education about the presence and impact of comorbidity and how to screen or assess for it was a commonly identified first step. Such models as the Reciprocal Rotations Project also provided clinicians with a better understanding of the way that collaborating services intervene, their available resources or treatment models used, and how to access their care. A lack of effective communication (e.g. not providing feedback following a referral, not responding in accordance with an agreed and coordinated intervention plan, not communicating relevant risk, health or social issues) was found to prevent effective collaboration.
Resolving logistical issues was a further priority. For co-location or inreach models, external staff needed suitable office space and equipment to conduct assessments and perform their role. Similarly, thought must be given for how they can best be integrated into the routine work of the on-site service (e.g. attendance at team meetings, mechanisms to offer secondary consultation). Promoting continuity of collaboration was also an issue. In some cases, individual professionals had received training to enhance their dual disorder capacity or had established effective relationships with staff from the collaborating services before leaving the service, thereby disrupting collaboration success. Efforts to minimise staff turnover and prepare for the event of staff turnover are therefore important.
While a number of positive outcomes were highlighted for the identified models, a consistent lack of published evaluation findings meant that many identified models could not be considered in this review. Evaluation should therefore occur alongside service innovation to ensure that achieved outcomes can be documented and that the lessons learned from implementing new models are disseminated to promote best practice in collaborative mental health care across Australia.
Recommendations for practice
In light of the review findings, the following are recommendations that may assist in promoting collaborative practice:
Collaboration should be led by the needs and goals of consumers and carers and be built on recognition that recovery is achievable.
Government, organisational, and clinical leadership is needed to promote and reward collaborative practice and establish incentives to facilitate integrated care.
Prior to commencing collaborative initiatives, the roles for staff of partner agencies and the mechanisms facilitating collaboration (e.g. expectations for communication and professional standards, expected partnership outcomes) must be agreed upon and documented (e.g. partnership agreement) to assist in holding partners accountable.
Governance structures must be established (e.g. project steering committees), independent of clinical partnership mechanisms, which regularly meet to review progress against project expectations and resolve any partnerships difficulties.
Collaboration should be built on respect, understanding of the complementary roles of partnering services, and shared knowledge for staff of the capacities and skill set of partnering services.
All staff should be trained on the impact of comorbidity, how to identify it, and how to engage staff from partnering services in supporting shared consumers.
Mechanisms to enhance communication and continuity of care between sectors (e.g. co-location, use of shared client record and care plans, joint assessments or case review meetings, secondary consultation on request, planned formalised education sessions, and zero-exclusion criteria for referrals) should be implemented.
Mechanisms to promote sustainability beyond existing staff (e.g. protocols outlining expectations regarding comorbidity and how to work with partner services, orientation to allow new staff to meet and learn how to work with collaborating services, shared opportunities for education or consultation) should be implemented.
Evaluation should accompany model implementation to demonstrate effectiveness and to serve a quality improvement role to identify whether aspects of the model are not working effectively.
Conclusion
As Australia progresses further towards adopting a community-based focus for mental health care, enhanced integration of care between all stakeholders able to support people with a serious mental illness is critically important to deliver more effective and recovery-focused mental health care.
Footnotes
Funding
Conduct of the literature review and stakeholder consultations was supported by funding received from the Australian Government Department of Health and Ageing.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.