
Abstract
Objectives:
For children and adolescents, the adverse effects from antipsychotic medicines exaggerate the already considerable burden of having a serious mental illness. Many of these young people face a future not only limited by stigmatizing psychiatric illness but also a life restricted and shortened by physical ill-health, particularly cardiovascular disease and type-2 diabetes. This review focuses on bridging the current gap between available evidence and practice guidelines and policies.
Method:
Following an extensive literature search, key papers focusing on the evidence of the nature and occurrence of metabolic morbidity in children and adolescents following the use of antipsychotic medication were included.
Results:
There is growing evidence to suggest that some of the key antecedents of metabolic syndrome occur soon after diagnosis and initiation of antipsychotic medication, and they accumulate over time.
Conclusion:
While guidelines and policies around the monitoring of metabolic syndrome in children and adolescents with mental illness receiving antipsychotic medication are limited, an opportunity lies in altering the trajectory towards cardiovascular disease and type-2 diabetes by early recognition and intervention to reduce cardiometabolic risk rather than waiting until disease end-points are reached later in life.
Keywords
Introduction
Young people on antipsychotic medication are at increased risk of weight gain and metabolic abnormalities that can appear within weeks of diagnosis (Correll et al., 2009; Foley and Morley, 2011) leading eventually to Metabolic Syndrome (MS) characterized by insulin resistance, abdominal obesity, dyslipidemia, hyperglycemia, and hypertension (Eapen and John, 2011). When viewed in the context of an epidemic of obesity and chronic disease sweeping through all young people (Yates et al., 2012), the increased risk of weight gain and MS in mentally ill young people on antipsychotic medication should be seen as an epidemic within an epidemic. The reasons for this increased risk are multifactorial and include genetic predisposition, lifestyle factors such as poor nutrition and lack of exercise, as well as smoking, substance abuse and adverse effects of antipsychotic medications. In this regard, weight gain and metabolic dysfunction may be the result of the psychiatric condition with consequent changes in appetite, activity level and metabolic rate both during the disease-state and linked to improvement and medication-induced effects such as sedation, dry mouth etc. as well as effects on neurotransmitter systems including monoamine, histamine and cholinergic transmission. While there is consensus about the need for close monitoring of young people on antipsychotic medication, there is less agreement on the definition as well as the optimal methods of detecting, preventing and treating metabolic risk (De Hert et al., 2012).
Definition
Metabolic syndrome is defined as a cluster of clinical and laboratory abnormalities that predicts future development of cardiovascular disease, type-2 diabetes and mortality (Alberti et al., 2005; Lakka et al., 2002; Tailor et al., 2010). There are several definitions including those created by the International Classification of Diseases, Ninth Revision (ICD–9), the International Diabetes Federation (IDF), the World Health Organization (WHO), the American Heart Association, the American Diabetes Association, the National Institute of Health (NIH), and the National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III) (Alberti and Zimmet, 1998; Expert Panel on Detection, 2001; International Diabetes Federation, 2006). The most commonly applied definition for weight gain and MS in children and adolescents includes the criteria provided by the Center for Disease Control (CDC) (Centers for Disease Control and Prevention, 2001) and the NCEP ATPIII Criteria modified by Cook for use in young people (Cook et al., 2003). Just as there are different definitions, there are also varying guidelines for monitoring, with different diagnostic criteria and recommendations.
Risk factors
Some individuals seem to have more of a propensity to develop metabolic side effects. Younger age; being overweight or obese; being underweight and having a lower baseline BMI; genetic and constitutional factors including family history of obesity, non-white ethnicity as well as lifestyle factors of diet and exercise; eating under stress; smoking; and alcohol and cannabis use are some examples of factors that increase the metabolic risk (Alvarez-Jimenez et al., 2008b; De Hert et al., 2011; Saddichha et al., 2008). Similarly, some medications cause more weight gain and metabolic abnormalities than others. In this regard, while Second Generation Antipsychotics (SGAs) are reported to carry a higher risk, first generation drugs can also cause weight gain, and there are differences between different antipsychotics, with some drugs causing more metabolic disturbances than others (Allison et al., 1999; Alvarez-Jimenez et al., 2008a). In this regard, dramatic levels of weight gain in treatment-naive first episode patients were reported by the European First Episode Schizophrenia Trial (EUFEST) (Kahn et al., 2008) where the occurrence of weight gain after one year of treatment was 86% for Olanzapine, 65% for Quetiapine, 53% for Haloperidol and 37% for Ziprasidone. Citing the findings of this study, Nasrallah (2011) commented that “Neither old antipsychotics, such as haloperidol, nor metabolically ‘benign’ atypicals, such as ziprasidone, are exceptions.” (Nasrallah 2011 p. 15).
Differences have also been observed in relation to the diagnosis for which the medication is being used, with young people treated with SGA for autism being reported to be at higher risk of developing weight gain and metabolic side effects (De Hert et al., 2011). Similarly, it has been suggested that persons with schizophrenia may have a predisposition toward developing MS that is exacerbated by their generally sedentary lifestyle, poor dietary habits, limited access to care, poor insight, and medication-induced adverse effects (Brown et al., 2000). In most cases, weight gain and central adiposity are major players in the pathophysiology of antipsychotic-induced MS mediated via insulin resistance, risk of diabetes, and dyslipidemias.
Clinical implications
A number of studies have addressed some of the issues pertaining to the effect of metabolic abnormalities on overall quality of life. Weight gain and obesity may limit the ability to engage in healthy physical activities as basic as walking, as well as damaging self-worth and confidence to participate in active physical pursuits (Vancampfort et al., 2011). This in turn may increase the risk of impaired physical health and may lead to treatment non-adherence and poor quality of life and well-being (Weiden et al., 2004). Schizophrenia patients with obesity have been observed to have inferior health-related quality of life (Allison et al., 2003), and medication-induced weight gain can also increase the risk of various co-morbidities, including cardiovascular morbidity, that can adversely affect the patient’s quality of life (Russell and Mackell, 2001). In this regard, recent trials estimate that rates of obesity and diabetes in persons with schizophrenia are nearly twice those of the general population (Cohn et al., 2004). It is also to be noted that occasionally diabetes and dyslipidaemia have been observed in the absence of weight gain, which underlines the importance of being alert to the possibility of serious metabolic disturbance occurring in those on antipsychotic medication who have not gained weight (McIntyre et al., 2001).
For the young population, the impact of weight gain on their self-esteem and its stigmatizing effect can in itself prompt them to discontinue medication, leading to relapse and poorer long term outcomes. This, coupled with the physical deleterious effects of weight gain and its consequences on the long-term prognosis and life expectancy, makes it critical that measures to prevent and treat weight gain in this population should take a center stage in their comprehensive management (Curtis et al., 2012; Foley and Morley, 2011). In this regard Correll et al. (2009) expose a powerful evidence of cardiometabolic adverse effects occurring rapidly in young people on antipsychotic medication. Further, incidence of myocardial infarction in young people with type-2 diabetes has been shown to be 14-fold higher than in those without diabetes (Hillier and Pedula, 2003). Prevalence of substance use and smoking is significantly higher in this group than in the general population, thus compounding the risk of cardiovascular morbidity and mortality compared with that of the general population (Scott and Happell, 2011).
Monitoring guidelines
A comprehensive model of care that integrates medical and psychiatric management can improve the overall health of young people with mental illness, but the current evidence suggests that we are failing to provide a reasonable standard of medical care to these patients (Eapen, 2012). While MS is a growing concern for persons with mental illness on SGAs, as indicated by Cohn and Sernyak (2006), controversies and debates surround issues such as the frequency of monitoring, which patients to monitor, who should do it, the utility of certain types of testing, and what happens after identification, with limited recommendations for child and adolescent populations. Even where guidelines have been put in place, the compliance with such guidelines is often suboptimal (Haupt et al., 2009). In this regard De Hert et al. recommend that:
Psychiatrists should monitor and record the BMI and waist circumference of every patient at each clinic visit regardless of the type of antipsychotic drug they have been prescribed; patients should also be encouraged to monitor and record their own weight. Waist circumference, which is simple and inexpensive to measure, is a better predictor than BMI of systolic blood pressure, HDL cholesterol and triglyceride levels.
There is considerable consensus among the published guidelines (De Hert et al., 2011, p. 151; Ho et al., 2011; Pringsheim et al., 2011) that the assessment in these cases should include weight and BMI; waist circumference; blood pressure; lipid levels; and glucose levels. According to the American Diabetes Association – American Psychiatric Association (ADA–APA) Consensus Guidelines (2004), weight should be assessed at four, eight, and 12 weeks after initiating or changing an antipsychotic agent, and quarterly thereafter. Fasting plasma glucose levels, lipid profile, and blood pressure should be assessed every three months on initiation of antipsychotic therapy, and sooner in persons who are at high risk at baseline. Compared with a fasting glucose test, a post-load oral glucose tolerance test is an earlier indicator of failing glucose control. Other important and potentially modifiable risk factors may also warrant consideration, including elevated levels of low-density lipoprotein (LDL) cholesterol, family history of premature coronary heart disease, diet, smoking, alcohol and substance use, and exercise or lack of activity either with or without weight changes. In order to assist the implementation of the guidelines, several recommendations and algorithms have been developed, such as the Australian monitoring guidelines (Waterreus and Laugharne, 2009).
Thus, while some consensus is emerging on what would be adequate and appropriate monitoring, there is less clarity on what should happen after identification of metabolic dysfunction, particularly in terms of who should treat and how best to treat. Also, there is currently a lack of consistency, clarity and message specificity in relation to dietary counseling for young people (Phillips et al., 2012). While specific data is not available on the efficacy of different types of diet in young people, based on the evidence from adult studies, it appears that caloric restriction is the key to weight loss regardless of which macronutrients they emphasize (Sacks et al., 2009). Guidelines suggest that clinicians consider switching the treatment to an antipsychotic with less risk of weight gain if a person gains more than 5% of his or her baseline weight or if dyslipidemia or hyperglycemia worsens (ADA–APA, 2004). Correll (2006) described eight distinct switch strategies when changing from one antipsychotic to another, including suggestions on situations in which the various strategies could be best used. However, further research is needed to develop guidelines on switching antipsychotics that are specific for children and adolescents and when and how to do this in a safe and effective way.
Guideline implementation: challenges and opportunities
While there is no doubt that the overall outcomes in young people with mental illness can be improved by the implementation of monitoring guidelines, there are significant challenges to this in the clinical setting. To facilitate this, clinical tools have been developed for cardiometabolic protection in youth with psychosis (Curtis et al., 2012). Previous research suggests that cardiac and metabolic risks are increased in patients receiving antipsychotic medication and that there is an appreciable yield of up to 66% for positive findings of metabolic abnormalities from routine testing (Bernardo et al., 2009). However, there is concern that screening programs are not being effective and that the implementation of monitoring guidelines is falling short of reasonable standards of care. The Atypical Antipsychotic Therapy and Metabolic Issues National Survey (Newcomer et al., 2004) and the nationwide database study by Cuffel and colleagues (Morrato et al., 2009) showed low rates of monitoring for metabolic risks. More recently, Mitchell and colleagues (2012), using pooled data from five countries on 218,940 adult patients at baseline and 71,594 post- guideline, found that metabolic monitoring rates for those receiving antipsychotics are low, with only blood pressure and triglycerides reaching above 50% but still sub-optimal. Inadequate testing was noted for cholesterol (41.5%), glucose (44.3%), and weight (47.9%). The rates were similar for those with schizophrenia as compared to other diagnoses in US and UK studies and in in-patient and out-patient settings. There was a modest but statistically significant increase in glucose testing following implementation of monitoring guidelines. However, the testing remained inadequate or sub-optimal for most testing procedures after guideline implementation except for weight (75.9%) and blood pressure (75.2%) monitoring, which were noted as just adequate.
There is also evidence to suggest that patients with psychiatric diagnoses receive inferior quality physical health care (Desai et al., 2002; Dixon et al., 2004; Frayne et al., 2005; Goldberg et al., 2007; Jones et al., 2004; Krein et al., 2006; Kreyenbuhl et al., 2006; Mitchell et al., 2009; Weiss et al., 2006), with physical co-morbidity in psychiatric patients often remaining unrecognized and inadequately treated (Bernardo et al., 2009; Holt et al., 2010; McEvoy et al., 2005; Mitchell et al., 2009; Taylor et al., 2005). In the Clinical Antipsychotics Trials of Intervention Effectiveness (CATIE) study, it was observed that around one third of patients met the NCEP criteria for MS at baseline but 38% with diabetes, 62% with hypertension and 88% with dyslipidaemia were untreated (Correll et al., 2007; Meyer et al., 2005; Nasrallah et al., 2006). Such findings highlight the fact that barriers to implementing metabolic monitoring guidelines that are patient-related, physician-related, and system-related, need to be acknowledged along with measures taken to overcome them so that patients receive adequate physical and psychiatric care (Sernyak, 2007).
Implications for policy and practice
Available evidence suggests that we are failing to provide reasonable standards of physical care for young patients with mental illness, and this is further exaggerated in the case of patients on antipsychotic medication due to the added metabolic risk. When balanced with the evidence of inadequate monitoring, there is an urgent need to transform mental health care through early identification of physical conditions followed by integrated medical and psychiatric care and customized treatments to improve overall outcome and quality of life. There is also a need to bridge the research gap through investigating the optimal methods of detecting, preventing and treating metabolic risk in mentally ill patients with special attention to service gaps both in terms of monitoring and early detection, as well as provision of adequate and appropriate medical care to those identified to be at risk of, or having, metabolic dysfunction (Eapen, 2012).
Policy recommendations:
A shift in population level behavior and attitudes is needed both from the perspective of the young population who are at risk and in terms of the health professionals involved in providing care and intervention. In this regard, the concept of “prevention paradox” (Rose, 1981, p. 1850) is applicable both at the population level and at the level of the clinicians, as prevention and intervention may be perceived as having little benefit while adding inconvenience to patients and work load to clinicians.
Clear policy guidelines are needed as to who should take lead clinical responsibility for supervising physical health, monitoring, cardiovascular disease risks, and acting when a need is revealed. While there is confusion as to who should monitor even in adult patients (Organ et al., 2010), there are particular considerations for the young population. For instance, GPs may lack confidence in dealing with serious mental illnesses that they rarely see in young people. Furthermore, many of the concerns that relate to antipsychotic adverse effects can emerge rapidly following antipsychotic initiation. The choice rests between GPs and psychiatrists as medical prescribers, but clarity in the shared care arrangements on this issue would be critical.
We believe the needs of this young population are best served in the early stages (for example within the first 12 months following antipsychotic initiation) by psychiatrists as lead prescribers.
The importance of accountable physical health care should apply irrespective of whether the young patient is in a community or in-patient setting.
Beyond the initial early phase it is important to establish local agreement on whether primary care or specialist services would be best placed to provide physical health care for ongoing needs.
Given the evidence that metabolic screening is low even after the introduction of monitoring guidelines, efforts at improving enforcement of guidelines matched with appropriate training of personnel and regular audits are indicated.
Lack of consistent and clear recommendations about dietary counseling and about non-pharmacological treatment options for management of metabolic risk is a major barrier at present and needs to be resolved.
Practice recommendations:
Rational, evidence-based and skilled medication management should take priority, with high thresholds for prescribing, balanced with access to psychological and family interventions to minimize clinical over-reliance on medication. Due consideration needs to be given to matching the evidence-base for diagnosis and the clinical picture with appropriate use of medication. Antipsychotic polypharmacy should be avoided as much as possible as this increases the risk of obesity (Maayan and Correll, 2011).
The initiation and “trial of treatment” using antipsychotics for every case should be underpinned by informed choice as well as intensive monitoring following initiation. While there is limited evidence to inform individualized treatment algorithms, comparative overview of side-effect profiles of SGAs in children and adolescents have been described (Correll et al., 2006).
Physical Health Clinics (Szpakowicz and Herd, 2008) similar to clozapine clinic where weight and/or waist circumference is monitored regularly and frequently would allow recognition of those with particularly rapid weight gain. Ideally, this should involve a weekly measurement of weight for the first eight weeks and a monthly measurement of lipids and glucose in the first three months. Just as for clozapine, systematic alert processes could be agreed upon that trigger appropriate clinical action, for example switching of the antipsychotic agent early if evidence for rapid weight or blood changes occurs.
Introduction of standards would encourage clinical governance and audit with particular focus on the following:
Antipsychotics should only be prescribed to young people with psychosis in the presence of regular monitoring of weight and Body Mass Index (BMI).
Assess for weight gain every one to two weeks in the first eight weeks following antipsychotic initiation, and then no less than three-monthly for the first year.
Results should always be clearly recorded in the clinical case record, and ideally charted for ease of comparison.
Where there is evidence of rapid weight gain (e.g. 7% within three months) or rapid development of abnormal lipids, BP, or glucose estimation, then a psychiatrist-led review should take place.
With young patients, a review about the need for continuing antipsychotic medication would be needed on an annual basis and planned withdrawal of antipsychotics is to be attempted after a two-year period, or earlier as appropriate.
It is recommended that a healthy lifestyle instruction or intervention program is offered at each clinic visit (Correll, 2008). Health promotion as well as intensive lifestyle and behavioral programs (Alvarez-Jimenez et al., 2008b; Brar et al., 2005; Curtis et al., 2011; Curtis et al., 2012; Kwon et al., 2006) should be made available for all patients, routinely including youth-friendly intervention strategies incorporating dietary counseling, exercise programs and information on healthy living to prevent weight gain occurring, and to assist those who have gained excess weight to lose it and remain at healthy levels (Eapen, 2012; Eapen et al., 2012).
Attention to co-morbid substance use and smoking cessation for tobacco users should be an important consideration (Myles et al., 2012), as well as the management of other modifiable risk factors.
Guidelines for children and adolescents need to be developed for the treatment of metabolic abnormalities, including the role of metformin in those with rapid weight gain refractory to lifestyle programs, or having other risk factors such as a family history of diabetes mellitus or premature cardiovascular disease.
Resource issues need urgent attention, as a lack of time and resources results in under-detection and under-treatment.
Given the rarity of severe mental disorders under the age of 18, specialist care is warranted in liaison with GPs and community mental health teams and in close collaboration with families. There should be a clear statement in the care plan as to who is responsible for monitoring and treating physical health conditions, and in which setting this would be managed, so that it is not assumed to be taking place elsewhere. Indecision and lack of clarity over this issue, as is often the case currently, cannot be supported. While it would seem that we are currently failing to provide a reasonable standard of physical health care for mentally ill young patients, there is a unique opportunity for mental health care providers to change their attitudes and practice and strive to provide holistic care to this vulnerable group of patients. Table 1 outlines a suggested clinical practice guideline for cardiometabolic monitoring in children and adolescents treated with antipsychotics. It is to be noted that these guidelines were not developed by a multidisciplinary team and these were not tested in patient or targeted clinician groups. There is an urgent need to develop user-friendly guidelines for children and adolescents with the participation of consumers and stakeholders.
Suggested practice guideline for cardiometabolic monitoring in children and adolescents on antipsychotic medication.
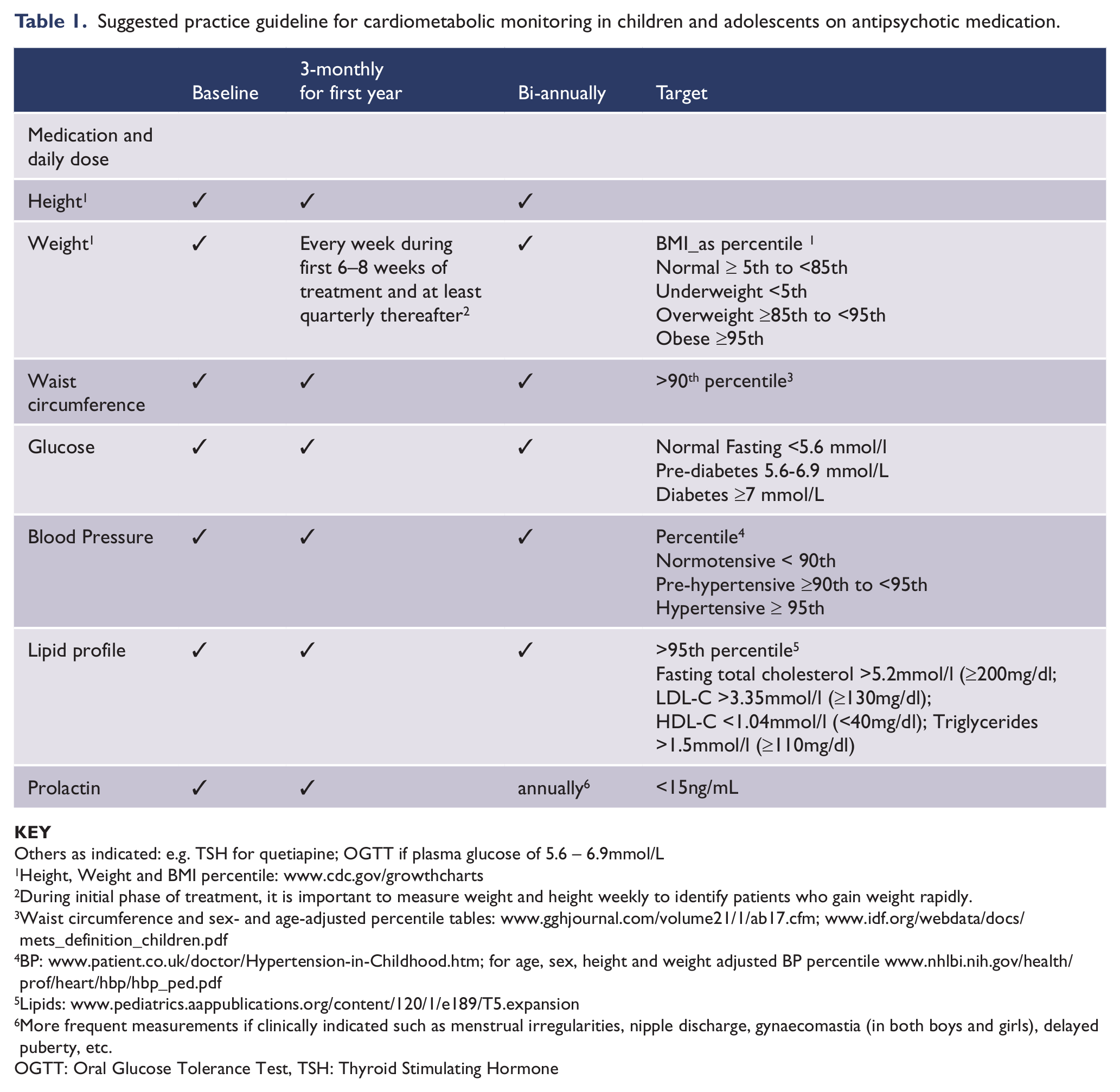
Others as indicated: e.g. TSH for quetiapine; OGTT if plasma glucose of 5.6 – 6.9mmol/L
Height, Weight and BMI percentile: www.cdc.gov/growthcharts
During initial phase of treatment, it is important to measure weight and height weekly to identify patients who gain weight rapidly.
Waist circumference and sex- and age-adjusted percentile tables: www.gghjournal.com/volume21/1/ab17.cfm; www.idf.org/webdata/docs/mets_definition_children.pdf
BP: www.patient.co.uk/doctor/Hypertension-in-Childhood.htm; for age, sex, height and weight adjusted BP percentile www.nhlbi.nih.gov/health/prof/heart/hbp/hbp_ped.pdf
More frequent measurements if clinically indicated such as menstrual irregularities, nipple discharge, gynaecomastia (in both boys and girls), delayed puberty, etc.
OGTT: Oral Glucose Tolerance Test, TSH: Thyroid Stimulating Hormone
Conclusion
Problematic weight gain and its potential cardiac and metabolic effects can become established within weeks of antipsychotic treatment initiation. Psychiatrists and GPs, with their medical training and role in prescribing, have a particular responsibility to actively intervene to promote physical wellbeing and protect cardiometabolic health for these young people. A prevention approach is badly needed to address the antipsychotic-induced metabolic disturbances constituting the metabolic syndrome if we are to avoid the consequences in physical ill-health that continue to blight the future lives of these young people.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declaration of interest
DS is Joint editor in receipt of royalties for the Wiley Blackwell publication Promoting Recovery in Early Psychosis (2010; ISBN 978-1-4051-4894-8); received a fee for a keynote presentation on early intervention in psychosis with a particular focus on the physical health issues from Jansen Cilag; and provides paid consultancy to the National Audit of Schizophrenia, Royal College of Psychiatrists’ Centre for Quality Improvement from May 2010 and ongoing. JC has received an unrestricted educational grant from Janssen-Cilag and speaker honoraria from Pfizer, Astra-Zeneca and Jansen-Cilag. DS is the Trustee for Rethink Mental Illness; Current member of two Guideline Development Groups (GDG) for NICE: a) NICE guidance for children and young people affected by psychosis and schizophrenia; and b) NICE guidance for adults with psychosis and schizophrenia (the views expressed in this paper are not those of either GDG, NCCMH or NICE); Joint editor in receipt of royalties for the Wiley Blackwell publication Promoting Recovery in Early Psychosis (2010; ISBN 978-1-4051-4894-8); received a fee for a keynote presentation on early intervention in psychosis with a particular focus on the physical health issues from Jansen Cilag; attended an educational meeting on September 22nd 2010 in Southampton; and provides paid consultancy to the National Audit of Schizophrenia, Royal College of Psychiatrists’ Centre for Quality Improvement from May 2010 and ongoing.