
Abstract
Objective:
To examine the temporal stability of the category ‘acute and transient psychotic disorders’ (ATPDs), ICD-10 Classification of Mental and Behavioural Disorders, including subtypes characterised by polymorphic, schizophrenic and predominantly delusional features.
Method:
We checked the readmission patterns of all patients aged 15–64 years (n = 5426), whether admitted to hospital or treated as outpatients, who were enrolled for the first time in the Danish Psychiatric Register with a diagnosis of ATPDs between 1995 and 2008.
Results:
An increasing number of cases with ATPDs changed diagnosis in subsequent admissions after 1, 2 and 5 years, mainly either to schizophrenia and related disorders or affective disorders. In their last admission, on average after 7.3 years, there were 2429 patients listed with ATPDs, accounting for an overall stability of 44.8%. Females were less likely than males to develop another diagnosis. Among the ATPD subtypes, polymorphic psychotic disorder without schizophrenic symptoms had a higher stability than those featuring schizophrenic or predominantly delusional features.
Conclusions:
The low diagnostic stability of ATPDs reflects the lack of clearly defining features and argues against their validity as a distinct category.
Introduction
The International Classification of Mental and Behavioural Disorders, 10th revision (ICD-10; WHO, 1992), introduced the category of ‘acute and transient psychotic disorders’ (ATPDs) within the F2 group ‘schizophrenia and related disorders’. Influenced by findings of the WHO study on acute psychoses (Cooper et al., 1999), ATPDs are characterised by: (a) acute onset; (b) polymorphic, schizophrenic or predominantly delusional syndromes; and (c) association (or not) with stressful life events. Early remission within 1 or 3 months distinguishes the ATPD subtypes with schizophrenic symptoms from schizophrenia and those with polymorphic or delusional features from persistent delusional disorder. Though emotional changes and affective symptoms may be prominent, the diagnostic criteria of ATPDs exclude both depressive and manic disorder.
The Diagnostic and Statistical Manual of Mental Disorders of the American Psychiatric Association has, since its fourth edition (DSM-IV; APA, 1994), listed ‘brief psychotic disorder’ (BPD), which features delusions, hallucinations, disorganised speech, and grossly disorganised or catatonic behaviour lasting less than 1 month. Another DSM-IV category, i.e. ‘schizophreniform disorder’ (SFD), includes short-lived psychotic disorders, which are intermediate in duration between BPD and schizophrenia. Because of differences in onset, duration and symptomatology, ATPDs overlap only partially with the DSM-IV categories BPD and SFD (Nugent et al., 2011).
ATPDs are rare conditions showing high rates of change to schizophrenia and, to a lesser extent, affective disorders in the short- and longer-term (Aadamsoo et al., 2011; Castagnini et al., 2008; Chang et al., 2009; Jørgensen et al., 1997; Pillmann and Marneros, 2005; Singh et al., 2004). Acute onset, short duration, shifting polymorphic symptoms, and absence of premorbid dysfunctions are features common to patients whose condition may be distinct from schizophrenia in course and outcome (Aadamsoo et al., 2011; Chang et al., 2009; Jäger et al., 2003; Linden et al., 2009; Pillmann and Marneros, 2005; Sajith et al., 2002; Salvatore et al., 2011; Singh et al., 2004; Suda et al., 2005), but it remains unclear to what extent such features identify the same category owing to the lack of diagnostic specificity (Castagnini and Berrios, 2011).
The aim of this paper is to address the validity of ATPDs by studying their diagnostic stability. It is important that these diagnostic concepts prove useful in making predictions of treatment and outcome.
Method
We checked the readmission patterns of all subjects aged 15–64 years, whether admitted to hospital or treated as outpatients, who were listed for the first time in the Danish Psychiatric Central Register (DPCR; Mors et al., 2011) with ATPDs between 1 January 1995 and 31 December 2008. The electronic database of the DPCR has stored information on all inpatients since 1969 and on outpatients since 1995. It provides data for national statistics, mental health planning and research. Register entries include information from case notes and, since 1994, diagnosis according to ICD-10 Diagnostic Criteria for Research. The quality of psychiatric assessment is enhanced by uniformity of training throughout the country, including supervision and courses in ICD-10 and related diagnostic instruments. The Danish National Health Service provides free treatment for all residents, and no private facilities exist.
In identifying diagnosis changes, we relied on the following ICD-10 categories: organic mental disorders (F0-9); psychotic disorders induced by substance or alcohol intoxication (F1x.5 and F1x.7); schizophrenia and related disorders, i.e. schizophrenia (F20), schizotypal disorder (F21), persistent delusional disorder (F22), schizoaffective disorder (F25), other and unspecified psychotic disorders (F28–29); affective disorders, i.e. manic episode (F30), bipolar disorder (F31), depressive episode (F32), recurrent depression (F33), persistent affective disorder (F34), other and unspecified affective disorders (F38–39); any other ICD-10 category.
This study will also examine the diagnostic stability of the different ATPD subtypes: acute polymorphic disorder without schizophrenic symptoms (APPD; F23.0), acute polymorphic disorder with schizophrenic symptoms (F23.1), acute schizophrenia-like psychotic disorder (F23.2), acute predominantly delusional disorder (F23.3), other and unspecified (F23.8 and F23.9) ATPDs for cases that cannot be classified elsewhere.
Statistical analysis
Temporal stability of ATPDs was estimated using the Cox proportional hazard model. Patients first admitted with ATPDs were followed-up to the date they changed diagnosis by 1, 2 and 5 years, and to their last admission by the end of the study (December 2008). Those patients who were not readmitted or did not develop another diagnosis were censored at the date of death or at the end of follow-up. A likelihood ratio test (LRT) was used to compare hazard rates; hazard rate ratios (HR) with 95% confidence interval (CI) were also calculated. Data analysis was conducted using Stata statistical software, version 11.2.
Ethical issues
Data comply with appropriate protection standards for anonymity. Ethical approval for this study was not required.
Results
There were 5426 patients (52.6% males) enrolled in the DPCR with ATPDs in 1995–2008. Females were older than males, mean age 36.9 years (SD 12.5) vs 33.3 years (SD 11.9). Only a few cases (3.6%) were rated as associated with acute stress.
The distribution of ATPD subtypes was as follows: acute predominantly delusional disorder 26.0%, APPD 20.4%, acute schizophrenia-like psychotic disorder 10.0%, and acute polymorphic psychotic disorder with schizophrenic symptoms 7.4%. The residual ‘other’ and ‘unspecified’ ATPDs accounted for 36.1% of the total sample. While APPD was preponderant in females (25.3% vs 16.0%), mean age 37.1 years (SD 12.1) vs 35.2 (SD 12.4), acute polymorphic psychotic disorder with schizophrenic symptoms and acute schizophrenia-like psychotic disorder were more common in males (19.8% vs 14.8%), mean age 29.0 years [SD 9.3] vs 33.4 years [SD 12.0]. For both subtypes with schizophrenic features, males had an earlier age of onset than females (29.5 years [SD 9.3] vs 33.2 years [SD 11.9] and 28.7 years [SD 9.3] vs 33.7 years [SD 12.1]). The corresponding figures for acute predominantly delusional disorder were 26.8% and 25.1%; mean age 36.5 years (SD 11.9) and 40.9 years (SD 11.9), respectively.
An increasing number of cases with ATPDs developed another diagnosis in successive admissions, mainly either to F2 schizophrenia and related disorders or F3 affective disorders. The overall stability, including those patients who were not readmitted after the initial episode, was 62.0% by 1 year, 56.0% by 2 years and 48.4% by 5 years (Table 1). In their last admission, on average after 7.3 years, 2429 (44.8%) cases were listed with ATPDs, 1701 (31.3%) with schizophrenia and related disorders, and 711 (13.1%) with affective disorders. The remaining had organic disorders (2.7%), substance-induced psychosis (2.1%), and other mental disorders (6.0%) (Table 2). Females were less likely than males to change diagnosis (HR 0.9 [95% CI 0.8–1.0]; χ2 = 10.0; p < 0.01) (Figure 1); the latter developed more often schizophrenia and related disorders (34.2% vs 28.1%); particularly those with acute schizophrenic features. A greater diagnostic shift to affective disorders was found for females (16.1% vs 10.4%).
Changes in diagnosis (ICD-10 codes) in 5426 patients with acute and transient psychotic disorders (ATPDs) by 1, 2 and 5 years since first admission.
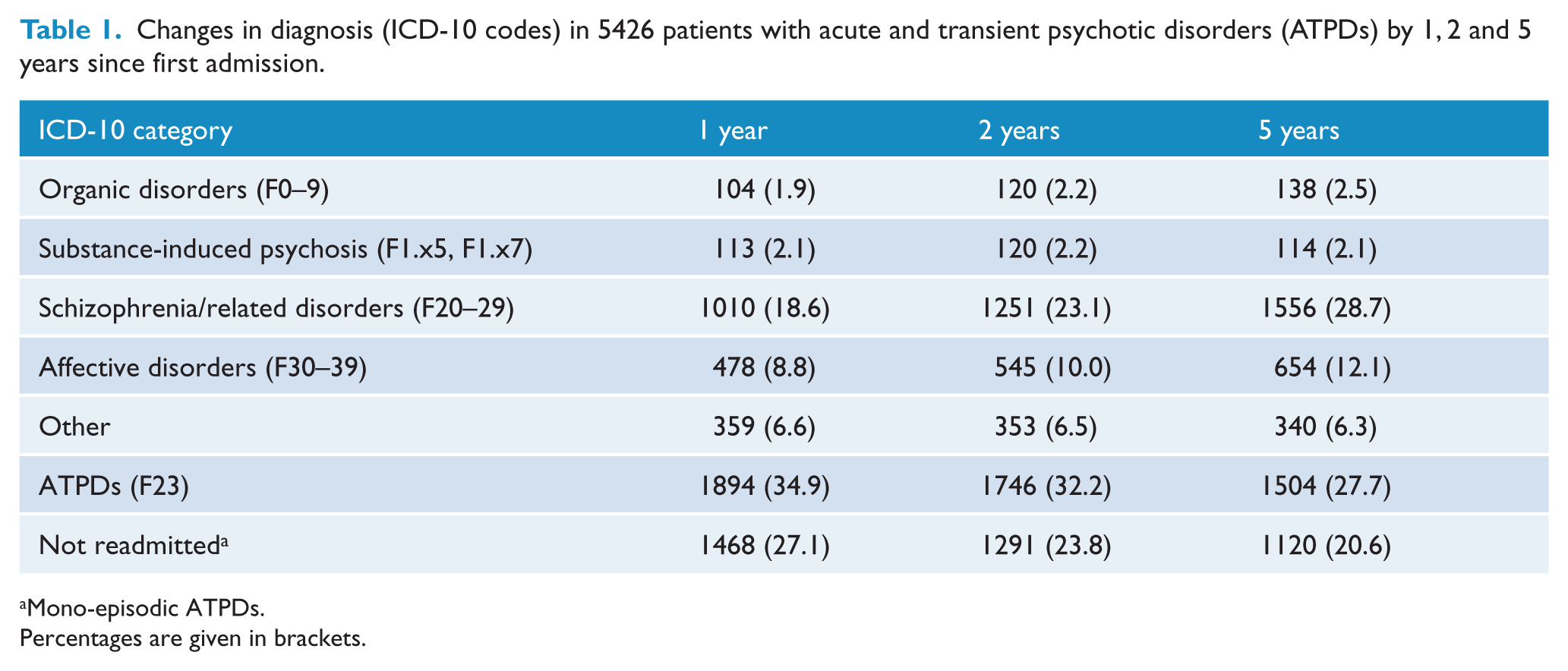
Mono-episodic ATPDs.
Percentages are given in brackets.
Last-admission diagnoses (ICD-10 codes) in patients first admitted with acute and transient psychotic disorders (ATPDs) in 1995–2008 by subtypes.
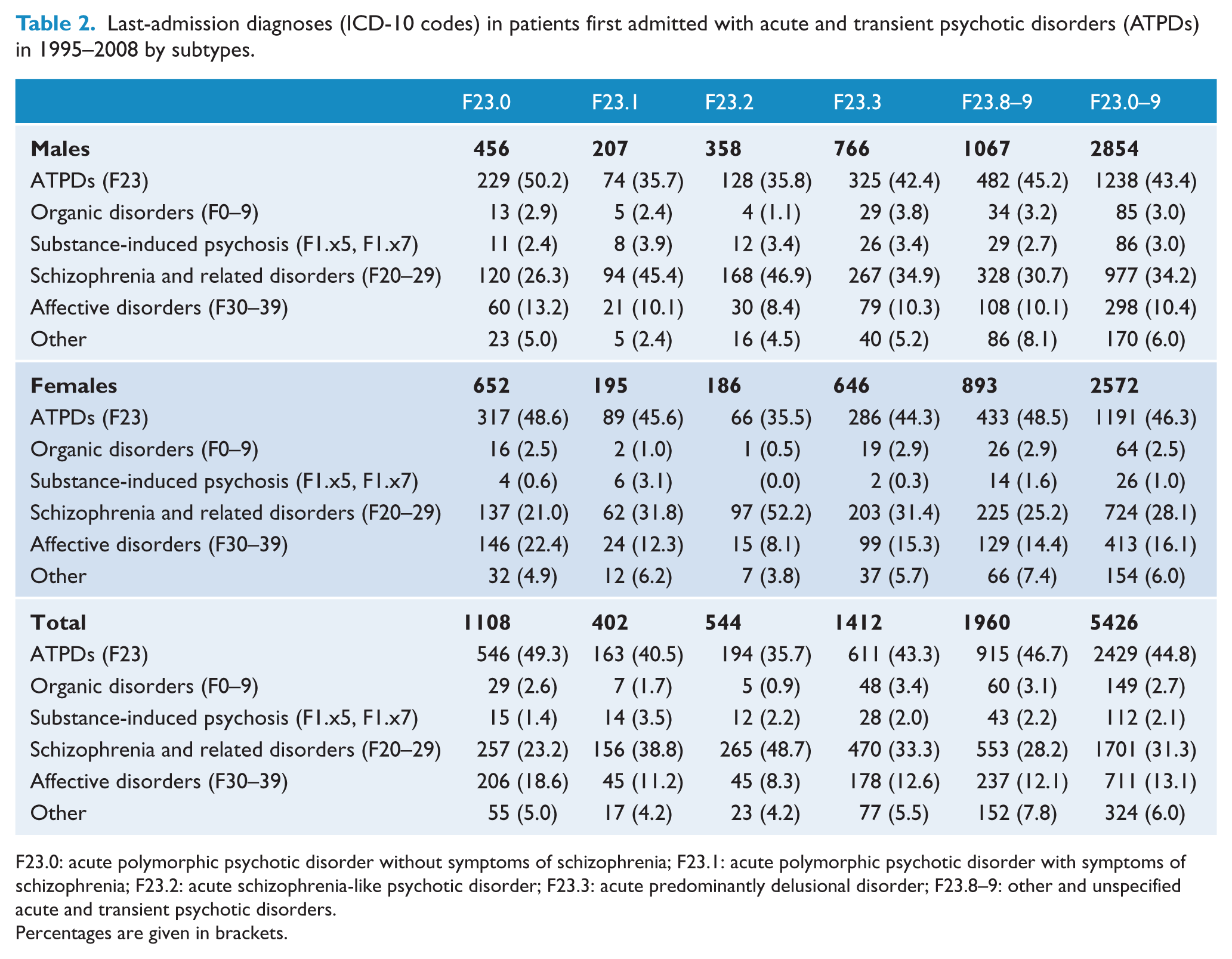
F23.0: acute polymorphic psychotic disorder without symptoms of schizophrenia; F23.1: acute polymorphic psychotic disorder with symptoms of schizophrenia; F23.2: acute schizophrenia-like psychotic disorder; F23.3: acute predominantly delusional disorder; F23.8–9: other and unspecified acute and transient psychotic disorders.
Percentages are given in brackets.
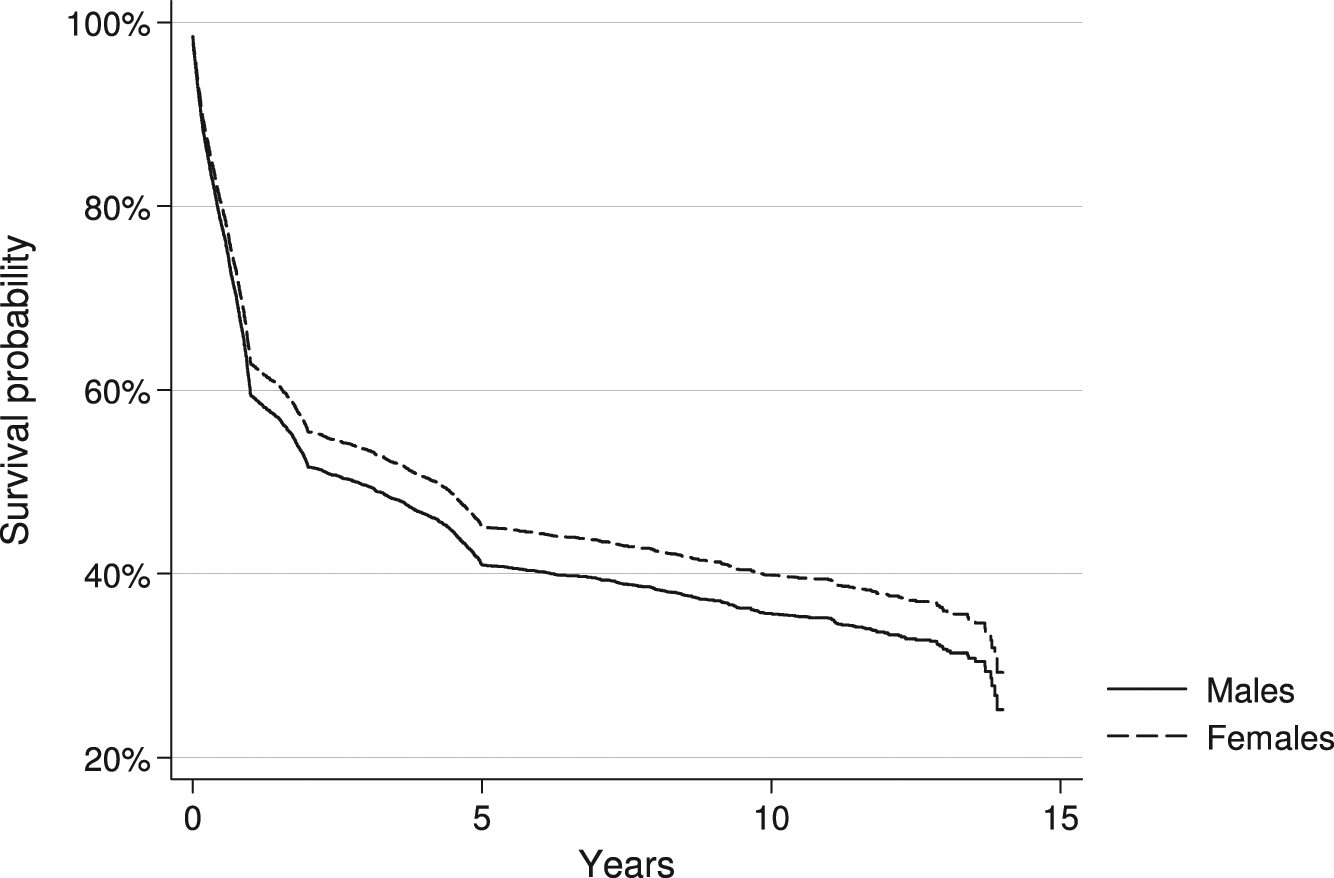
Survival curves showing the probability that patients with acute and transient psychotic disorders (ATPDs) did not change diagnosis over 1995–2008 by gender.
Among the ATPD subtypes, APPD showed a higher stability than those featuring schizophrenic (HR 0.7 [95% CI 0.7–0.8]; χ2 = 26.5; p < 0.01) or predominantly delusional symptoms (HR 0.9 [95% CI 0.8–1.0]; χ2 = 8.0; p < 0.01). A significantly higher diagnostic stability was also observed for predominantly delusional disorder than the subtypes with schizophrenic features (HR 0.9 [95% CI 0.8–1.0]; χ2 = 7.4; p < 0.01).
Discussion
To our knowledge, this is the first large-scale study examining the temporal stability of ATPDs. It marks a clear advance from previous studies, which used small samples of cases, and is representative of the entire ATPD category, subsuming polymorphic, schizophrenia-like and delusional syndromes. This knowledge is essential for enhancing the understanding of ATPDs and contributing to build a case for their revision in future psychiatric classifications. In the absence of aetiological factors and biological markers, statements about clinical validity pertain mainly to the predictive power of the diagnostic categories (Kendell, 1989).
The findings of this study suggest that an increasing number of patients with ATPDs have their diagnosis changed in subsequent admissions, either to schizophrenia and related disorders or, to a lesser extent, affective disorders. The overall stability of ATPDs, comprising both mono-episodic and recurrent remitting forms, was relatively low and varied across the different subtypes. Such diversity is to be expected as ATPDs is a heterogeneous category including subtypes that are set apart from schizophrenia only by temporal criteria. Indeed, about one in two of cases followed-up with acute schizophrenic features were likely to develop schizophrenia or another F2 category. These subtypes are also associated with a male preponderance and have an increased risk of schizophrenia in family members, pointing out a close kinship to schizophrenia (Aadamsoo et al., 2011; Castagnini et al., 2008; Chang et al., 2009; Das et al., 1999; Singh et al., 2004). Yet, it seems that APPD is not only more common in females, but also has a higher diagnostic stability. Such findings add weight to earlier reports showing that APPD has distinctive features from the ATPD subtypes characterised by schizophrenic symptoms and may bear a closer relationship to affective disorders (Chang et al., 2009; Pillmann and Marneros, 2005; Sajith et al., 2002; Salvatore et al., 2011). APPD refers to the French concept of bouffée delirante (Magnan, 1893; Weibel and Metzger, 2005) and Kleist (1928) and Leonhard’s (1957) cycloid psychoses, featuring varied and rapidly changing delusions, hallucinations, perceptual disturbances, agitation, perplexity and emotional turmoil. However, whether APPD identifies a separate category, or links schizophrenia and affective psychoses, has yet to be established.
Furthermore, the current findings indicate that ATPDs are associated with a higher stability in females, and that the greatest variability occurred early, as almost half of patients developed another diagnosis in the first 2 years following the initial admission. This is consistent with the view that ATPDs may herald the onset of longer-lasting psychotic and affective disorders.
Available evidence suggests that acute onset, short duration, female gender and good premorbid functioning are factors associated with temporal stability and favourable outcome, though differences in method, design and length of follow-ups being conducted make meaningful comparisons difficult (Castagnini and Berrios, 2011). There may also be variations in course and outcome of ATPDs between developing countries and industrialised ones. Sajith et al. (2002) found high diagnostic stability and low rates of relapse in a selected cohort of Indian patients with APPD over 3 years. Further reports from developing countries indicate that most cases with ATPDs enjoyed complete remission 1 year later (Amini et al., 2005; Thangadurai et al., 2006).
In Denmark, Jørgensen et al. (1997) reported that about half of their 46 patients with ATPDs converted into schizophrenia, persistent delusional disorder, or affective disorders, and a third relapsed over 1 year. Subsequent studies have shown that cases with ATPDs tended to experience recurrent affective or psychotic episodes, 30% developed mood disorders and a relatively small number schizophrenia or schizoaffective disorder. Although only a third of them had stable remission and discontinued medication after 7 years, they fared better than patients with schizophrenia (Pillmann and Marneros, 2005). Further evidence from the Nottingham first-episode psychosis study (Singh et al., 2004) supports the view that ATPDs have a more favourable clinical and social outcome than schizophrenia, though two-thirds of cases changed diagnosis 3 years later. In keeping with findings of the Münich first-admission psychosis study (Möller et al., 2011), the long-term prognosis of ATPDs proved to be more favourable than for schizophrenia or delusional disorder. Moreover, Chang et al. (2009) and Aadamsoo et al. (2011) have found that 35–50% of patients first admitted with ATPDs did not develop another diagnosis. In the latter study, most cases with ATPDs had recovered and 40% were no longer prescribed antipsychotic drugs after 2 years (Aadamsoo et al., 2011).
Lastly, the McLean-Harvard international first-episode psychosis study (Salvatore at al., 2011) reported that a third of patients with APPD and 72% of those with schizophrenia-like features developed schizophrenia or affective psychoses 2 years later, and that Schneider’s first-rank symptoms of schizophrenia were associated with diagnostic changes. Attempts to differentiate schizophrenia from ATPDs on the basis of the first-rank symptoms have failed as they occur in both clinical groups; only negative symptoms can distinguish schizophrenia from ATPDs (Jäger et al., 2003).
Related conditions such as the ‘acute non-affective remitting psychoses’ (Susser and Wanderling, 1994) have shown high stability and favourable outcome, particularly in developing countries, but seldom fulfil the criteria for ATPDs lasting longer than 1–3 months (Mojtabai et al., 2000). These psychotic disorders have clinical and epidemiological features which distinguish them from schizophrenia, such as a characteristic geographic distribution, a higher incidence in females and association with stress, fever or systemic infections (Nugent et al., 2011).
Clinical and nosological implications
ATPDs are a problematic category for clinical practice and research owing to the fleeting nature of polymorphic features, which can include schizophrenic symptoms, and high rates of cases with ‘other’ and ‘unspecified’ subtypes. Likewise, acute predominantly delusional disorder is a diagnosis by exclusion from polymorphic psychotic disorder, schizophrenia and persistent delusional disorder (Sartorius et al., 1995).
The lack of clearly defining features argues against the subdivision into different subtypes (Aadamsoo et al., 2011; Castagnini et al., 2008; Chang et al., 2009; Jørgensen et al., 1997; Pillmann and Marneros, 2005; Singh et al., 2004). It has been suggested that the ATPD subtypes with schizophrenic symptoms should be withdrawn, and temporal criteria of less than 1 or 3 months should be raised up to 6 months (Mojtbai et al., 2000; Nugent et al., 2011). Although the changes proposed would bring ATPDs closer to DSM-IV BPD and SFD, it would be difficult to extend ATPD criteria, as that would involve changes in duration of both schizophrenia and persistent delusional disorder. It also seems questionable whether to maintain the separation of BPD and SFD given their uncertain validity.
Furthermore, what is an adequate stress and its relationship to ATPDs needs clarification. ATPDs seem more often to be associated with life events than schizophrenia or manic disorder, pointing out that environmental factors play a part in their causation (Chakraborty et al., 2007; Das et al., 2001; Linden et al., 2009). However, ‘acute stress’ is coded only as an additional diagnostic feature and the temporal relationship to ATPDs restricted to 2 weeks may have underestimated the number of cases triggered by stressful events (Castagnini et al., 2008).
Methodological limitations
The main limitation of this study hinges on the fact that the DPCR records information routinely collected about inpatients and outpatients from the entire country and the diagnosis of ATPDs has not yet been validated using operational criteria. In addition, diversity in distribution of ATPD subtypes from previous reports, which included relatively higher rates of polymorphic psychotic disorders, may be related to the fact that acute predominantly delusional disorder conforms more to the concept of reactive psychosis, a traditional diagnosis in Denmark before the introduction of ICD-10 (Castagnini, 2010).
Conclusions
Although these findings suggest that ATPDs is a composite category and the low predictive power argues against its validity, APPD has distinctive features from the subtypes characterised by schizophrenic symptoms and deserves further research.
Footnotes
Acknowledgements
Thanks are due to Mrs G Pilgaard Perto, programmer of the DPCR, for assistance with data collection.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.