
Abstract
Objective:
Regular physical activity may be an important contributor to psychological well-being. This link has not been explored in ethnically distinct, low- and middle-income countries (LMIC), especially in countries affected by war. This study aimed to examine the relationship between physical activity and levels of psychological distress in an epidemiological cross-representative sample of Vietnamese living in the Mekong Delta region of Vietnam.
Methods:
The sample was drawn from an urban (Cần Thơ City) and a rural (Hậ u Giang) region, using a multi-stage probabilistic cluster sampling frame. The measures applied included the Composite International Diagnostic Interview (CIDI 2.0) yielding 12-month prevalence rates of common mental disorders, including anxiety, mood and substance use disorders; the Phan Vietnamese Psychiatric Scale (PVPS), a culturally specific self-report measure; and the Harvard Trauma Questionnaire. The Global Physical Activity Questionnaire (GPAQ version 1) was used to measure activity. Analyses were conducted using SAS software v.9.1.3. The population was assigned to three (high, moderate and low) physical activity levels. Analyses included chi-square tests and univariable and multivariable logistic models.
Results:
Physical activity was greater in males, the middle-aged group (30–54 years), those who were married, the rural population, less educated individuals and those who were employed. High physical activity was significantly associated with low levels of psychological distress (indexed by a combination of CIDI and PVPS cases identified) when controlling for socio-demographic factors and number of medical conditions). Membership of the lowest of the three physical activity groups was associated with a psychological distress odds ratio of 2.19 (95% CI 1.28–3.75). The results remained consistent when analyses were undertaken separately for males and females.
Conclusions:
Low levels of physical activity appear to be associated with greater psychological distress in the Mekong Delta of Vietnam. The association remained after adjusting for the influence of socio-demographic characteristics, exposure to past trauma, urban–rural residency and the presence of self-reported physical disorders. These data provide a foundation for exploring the role of physical activity as an adjunct to conventional interventions for common mental disorders in resource-poor LMIC countries.
Introduction
Regular physical activity has long been regarded as an important contributor to health and psychological well-being (Pate et al., 1995), with scientific evidence providing support for that link, particularly in relation to common symptoms of depression and anxiety (Taylor et al., 1985; Wiles et al., 2007). Nevertheless, the results of studies examining this association are not conclusive. Whilst a recent review comparing exercise with no treatment or a control intervention indicated a large clinical effect, the only three trials with adequate allocation concealment, intention-to-treat analysis and blinded outcome assessment resulted in a moderate, non-significant effect (Rimer et al., 2012). Nevertheless, to our knowledge, no epidemiological studies have examined for such a link in ethnically distinct, low- and middle-income countries (LMIC). We report the findings of a study examining associations between physical activity and a range of psychiatric symptoms undertaken in the Mekong Delta region of Vietnam.
There is some evidence from western settings that increasing physical activity can lead to a reduction in symptoms of anxiety and depression, although methodological constraints limit the confidence with which such inferences can be drawn (Dunn et al., 2001). If it can be demonstrated that physical activity is linked to common psychiatric symptoms in LMICs, this may provide the impetus to trialling exercise-based interventions for conditions such as depression and anxiety, particularly given that more complex and expensive treatments such as psychotherapy are not available in many of these settings.
Several factors could influence the relationship between physical activity and symptoms of anxiety and depression in LMICs. Ethnic factors, whether biological or cultural, may modify the nature or strength of the association but little is known about these influences. In addition, the association may be stronger in LMICs where health services are less developed and physical disorders may be more severe or chronic. Importantly, in war-affected countries such as Vietnam, past exposure to combat and other trauma could influence the rates of residual physical disorder and long-term mental illness (Steel et al., 2009b). Whether respondents live in urban or rural settings also may influence physical activity, a difference that may have become more pronounced in countries such as Vietnam with the accelerated transition to modern transport systems and an increase in sedentary working conditions in urban settings (Van Minh et al., 2003). For these reasons, we included indices of physical illness, trauma exposure and urban–rural residency in the multivariable models tested in the present study.
In undertaking mental health studies in transcultural settings, it is important to supplement western-derived diagnostic measures with assessments of culturally specific idioms of distress (Steel et al., 2009b). For example, culturally expressed somatic symptoms commonly indicate psychological distress amongst populations such as the Vietnamese (Steel et al., 2009b). A previous analysis of the present data set found that an indigenously derived measure of distress detected a substantial number of cases not identified by a commonly applied Composite International Diagnostic Inventory (CIDI) (Steel et al., 2009a, 2009b). Each method identified unique cases of disability indicating that together, they provided a comprehensive account of the level of mental health dysfunction in the community.
The aim of the present study was to examine the relationship between physical activity and indices of psychological distress in an epidemiological sample of Vietnamese living in a rural and urban setting in the Mekong Delta region of Vietnam. The composite index of psychological distress was based on an international and indigenous measure. Analyses controlled for socio-demographic factors, war trauma exposure and reported physical health status.
Methods
A full description of survey methods has been provided elsewhere (Steel et al., 2009b).
Mekong Delta Survey
The research project had ethics approval granted from the University of New South Wales, Australia, Human Research Ethics Committee. The sample was recruited between November 2004 and March 2005 in Cần Thơ City and Hậu Giang province in the Mekong Delta region of Vietnam, thereby including both an urban and a rural population. The survey applied a multi-stage probabilistic cluster sampling frame with the commune or hamlet, the smallest geographic area for which census information is available, specified as the primary sampling unit. The first stage applied probability proportional to size sampling to identify 15 of 478 hamlets in Hậu Giang province and 16 of 503 hamlets in Cần Thơ City. In each hamlet, we selected 100 consecutive households using a random commencement point. Within each household, a single respondent aged 18 years or older was selected using a Kish grid without replacement due to non-response.
Twenty-five local personnel (five mental health physicians, 16 mental health nurses and four general staff) conducted the interviews. All interviewers received 40 hours of training in the administration of the research instruments, as well as ongoing supervision.
Survey instruments
The CIDI 2.0 is a lay administered instrument yielding 12-month prevalence rates of mental disorders defined by the Diagnostic and Statistical Manual, fourth edition (DSM-IV) of the American Psychiatric Association. The instrument is the most widely used diagnostic measure applied in contemporary international studies in mental health (Kessler and Ustün, 2004). We included the modules for anxiety disorders (panic disorder, agoraphobia, social phobia, generalized anxiety disorder, obsessive–compulsive disorder and post-traumatic stress disorder), mood disorders (depression, dysthymia, mania, hypomania and bipolar disorder) and substance use disorders (alcohol and substance harmful use/abuse and dependence). In addition, assessed for neurasthenia, a condition in which somatic symptoms reflect underlying psychological disturbance, a category of the International Classification of Diseases, 10th revision system (ICD-10) not included in DSM-IV. Persons meeting criteria for any one of the disorders measured were treated as a case in the present analysis.
The Phan Vietnamese Psychiatric Scale (PVPS) is a self-report measure designed to identify culturally relevant idioms and expressions of psychological distress in that ethnic group. A full description of the ethnographic and psychometric studies conducted in developing the measure has been published previously (Phan et al., 2004). We included the anxiety and depression scales in the present study. We applied established threshold scores to allocate persons in making case assignments. In the analyses, we have combined cases identified by the CIDI or the PVPS as meeting criterion for the threshold of psychological distress.
Exposure to 24 events was assessed using the trauma events component of the Harvard Trauma Questionnaire expanded to include coverage of domains assessed by the CIDI 2.0.
Physical activity instrument
The Global Physical Activity Questionnaire was developed by the World Health Organization (GPAQ version 1) to measure this index in LMICs (WHO, 2011). The questionnaire was modified from the International Physical Activity Questionnaires (long- and short-form IPAQ), which has been used worldwide (Craig et al., 2003). Previous psychometric testing of the measure amongst diverse populations has indicated both sound test–retest reliability and concurrent validity against the IPAQ (Bull et al., 2009).
Our preliminary analyses indicated that the components of the measure assessing activity in work/employment and commuting together comprised the greatest portion of overall activity, with a minimal contribution from recreation. We therefore did not disaggregate components of the measure in analyses, instead applying the composite index of total physical activity to test, in the most general manner, the relationship between activity and psychological distress.
Statistical analysis
Analyses were conducted using SAS software v.9.1.3 (SAS Institute Inc., Cary, NC, USA: 2002–2003). The analysis was weighted for sampling design effects and post-stratification adjustments to reflect the structure of the population under study. The population was assigned to standard levels of physical activity (high, moderate and low) as per the GPAQ Analysis Guide (WHO, 2011). Analyses included chi-square tests and univariable and multivariable logistic regression models. Logistic regression models examine the association between psychological distress and levels of physical activity. Factors controlled for in the models are rural–urban residence, sex, age group, marital status, educational level, employment status and number of medical conditions. The results are presented as the percentage prevalence and odds ratios, with 95% confidence intervals.
Results
Demographic data
The sample comprised 3039 persons (response rate, 98%). The demographic characteristics of the sample are recorded in Table 1. Eighty five percent were 54 years or younger. There was a balance in sexes and in the numbers living in rural and urban areas. A total of 603 (19.8%), 595 (19.6%) and 1841 (60.6%), respectively, were assigned to the high, medium and low physical activity categories of the GPAQ (Table 1). Table 1 compares the socio-demographic characteristics of the sample with levels of physical activity. Physical activity was greater in males, the middle-age group (30–54 years), those who were married, the rural population, less educated individuals and those who were employed.
Mekong Delta mental health survey: Respondent characteristics by physical activity level.
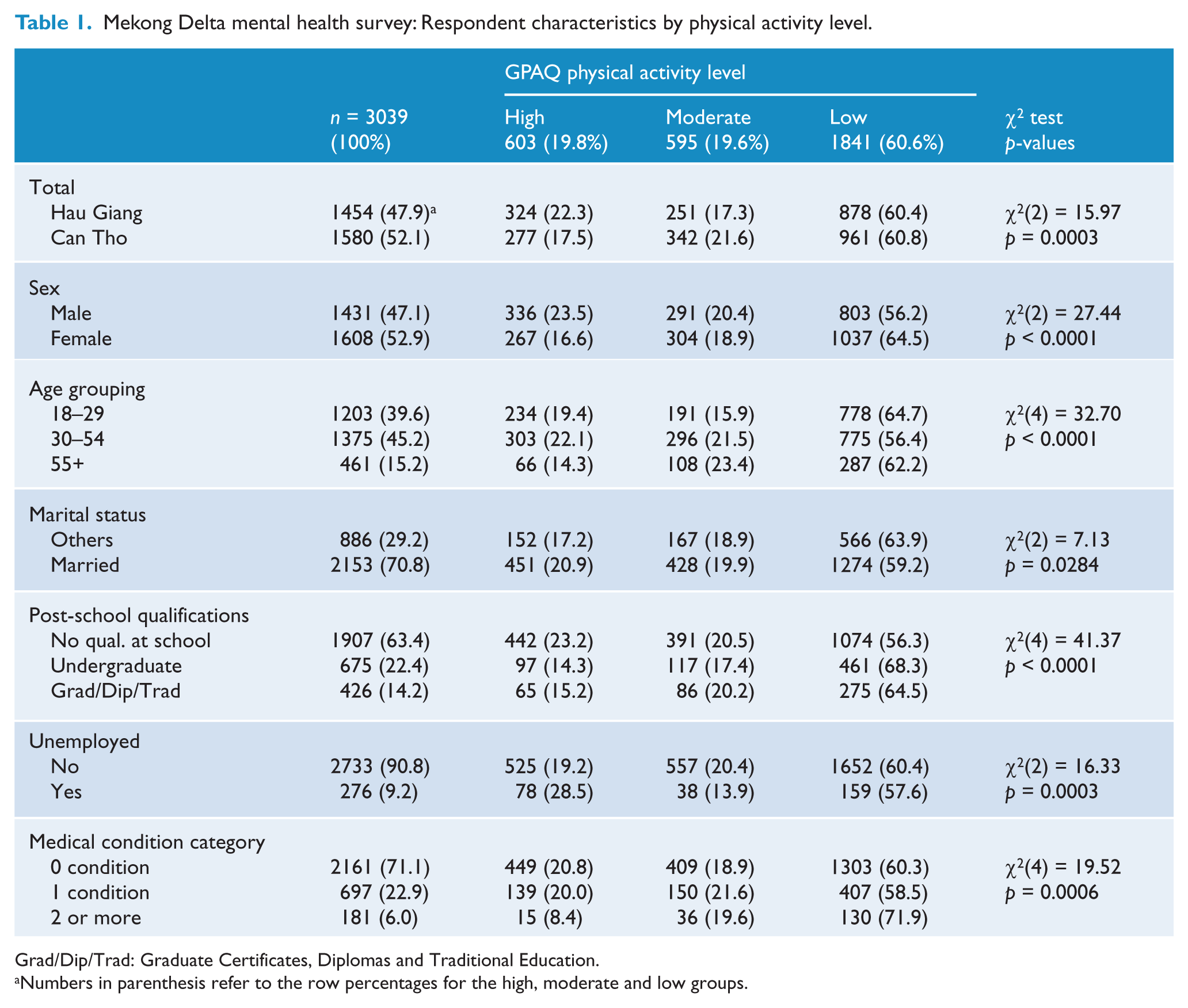
Grad/Dip/Trad: Graduate Certificates, Diplomas and Traditional Education.
Numbers in parenthesis refer to the row percentages for the high, moderate and low groups.
Psychological distress
The CIDI yielded a 12-month mental disorder prevalence rate of 1.9%. The prevalence rate produced by the indigenous measure was 7.4%. The combined index of distress (those meeting case threshold on either or both measures) was 8.8%, noting that there was some overlap in the cases identified by each method.
Associations of physical activity with the index of psychological distress
Table 2 reports univariable and multivariable associations of the relevant predictor variables with indices of psychological distress. In the univariable analysis, the highest level of physical activity was associated with the lowest risk of psychological distress assessed by the CIDI alone, indigenous measure alone and the combined index of distress. As indicated in Table 2, high physical activity continued to be significantly associated with low levels of psychological distress across all three psychological indices when controlling for other factors (age, sex, physical disorder, rural–urban residence, trauma count). Membership of the low physical activity group was associated with a psychological distress odds ratio of 2.19 (95% CI 1.28–3.75). Further examination of the data (not reported in tables) indicated that the results remained consistent when analyses were undertaken separately for males and females.
Association between mental disorder and levels of physical activity.
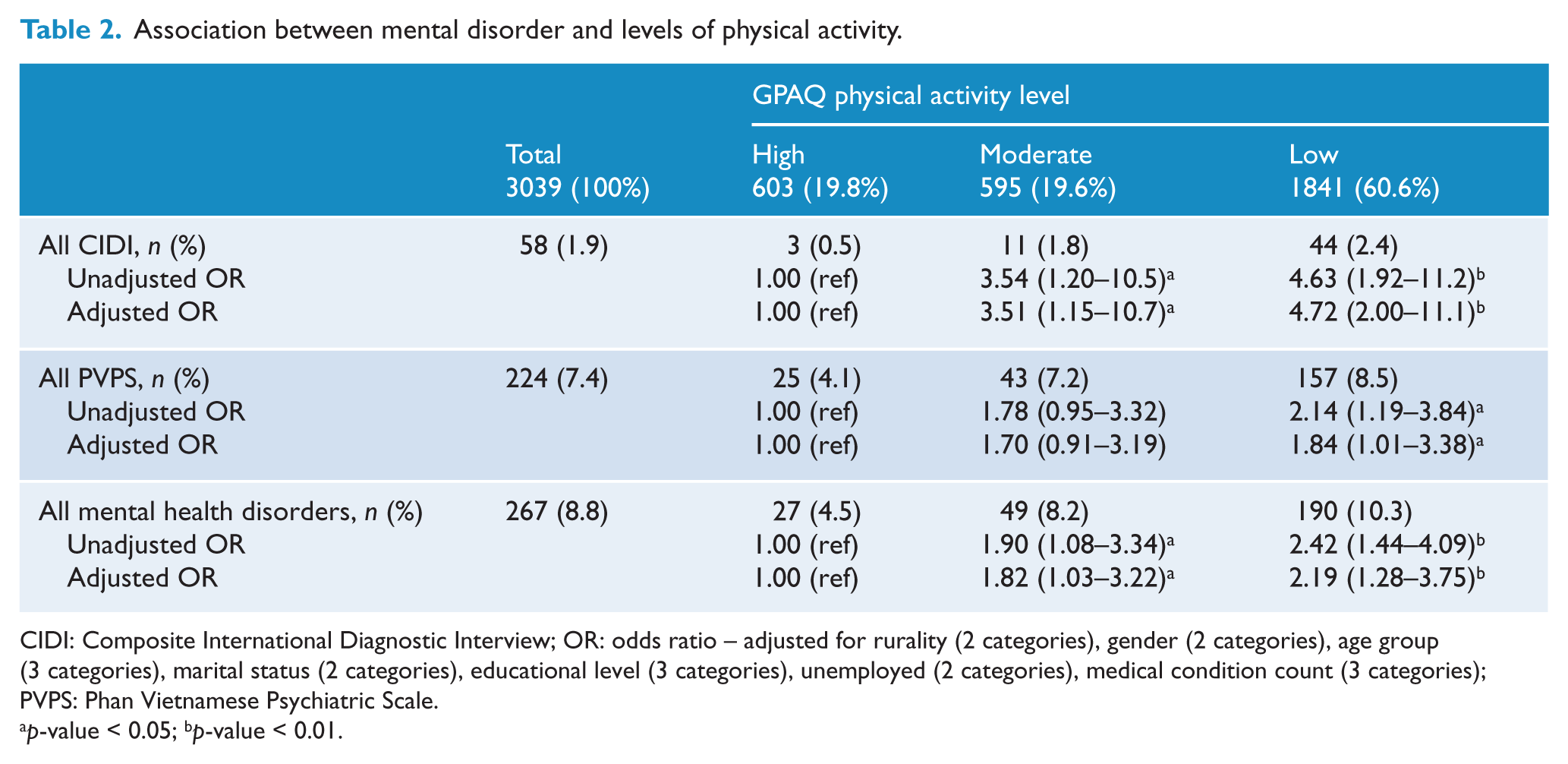
CIDI: Composite International Diagnostic Interview; OR: odds ratio – adjusted for rurality (2 categories), gender (2 categories), age group (3 categories), marital status (2 categories), educational level (3 categories), unemployed (2 categories), medical condition count (3 categories); PVPS: Phan Vietnamese Psychiatric Scale.
p-value < 0.05; b p-value < 0.01.
Discussion
Overview of findings
To our knowledge, this is the first study to indicate a link between physical activity and psychological distress in a LMIC that is culturally distinct from countries of the west. The association was robust for the western and the indigenous index of mental disorder. In addition, the association remained significant after taking into account other potential influences including socio-demographic characteristics, reported physical disorder, urban–rural residency and past exposure to trauma.
Strengths and limitations of the study
The data are derived from a large, probabilistic sample with a high response rate. The association of physical activity with rural residency, female sex and lower education add support to the validity of the findings overall, since similar associations have been identified in other settings (Trost et al., 2002). Similarly, the findings are consistent with those of a large body of research worldwide that have shown associations between female sex, past trauma, and the presence of medical conditions and risk of psychological distress (Piccinelli and Wilkinson, 2000; Steel et al., 2009a). Finally, the finding that physical activity was associated with both indices of distress adds to the robustness of the findings.
The study was limited to one region of Vietnam so that it cannot be assumed that the results are generalisable to the whole country. The cross-sectional nature of the study cautions against drawing definitive causal inferences, an issue that will be considered further below. Transcultural factors may have added to measurement error in spite of the rigorous translation and back-translation methodology we applied. The GPAQ is a comprehensive index of physical activity including scales for work, commuting and recreation. We did not disaggregate these sub-domains after preliminary analyses indicated that the major contributors to activity were the highly inter-correlated work and commuting domains, with recreation being minimally endorsed. We note that the Vietnamese reported only moderate levels of physical activity across all age groups compared with other populations in LMICs (Craig et al., 2003). Finally, the CIDI yielded a relatively low rate of anxiety and depressive disorders so that it was not possible to examine these categories separately.
Implications
Given the cross-sectional nature of the study, several possible explanations need to be considered. First, it is possible that high levels of psychological distress impact directly on the level of physical activity. Symptoms of depression such as low motivation, interest and energy may reduce the person’s activity level overall (Patten et al., 2009). Similarly, anxiety is commonly associated with phobias and avoidant behaviour, symptoms that restrict activity outside the home. At the same time, there is a growing consensus that the level of physical activity can influence symptoms of depression and anxiety (Taylor et al., 1985; Wiles et al., 2007). It is possible that this effect is mediated by psychological factors via an enhanced sense of well-being and efficacy and/or biologically, for example, via changes in neurotransmitter or neurohormonal systems implicated in modulating mood (Borer, 2003).
It is also possible that other mechanisms may mediate the relationship; for example, abnormalities in neurotransmitter or neurohormonal functions could lead to reduced activity and adverse psychological consequences. Alternatively, social stresses or deprivations could lead to psychological distress and constraints in the person’s lifestyle that inhibit physical activity. Hence, further research is needed to delineate precisely the mechanisms that mediate the relationship involving activity and psychological distress.
Irrespective of the mechanisms involved, the demonstration of an association between physical activity and psychological distress in a LMIC such as Vietnam may have direct public health implications. Epidemiologic research undertaken in high income countries has demonstrated that low physical activity is a risk factor for a range of chronic physical illnesses including coronary heart disease, hypertension, non-insulin-dependent diabetes mellitus, osteoporosis and colonic cancer (Pate et al., 1995). There is evidence that the prevalence of these disorders is increasing in the developing world (Joubert et al., 2007; Popkin, 2001; Popkin and Gordon-Larsen, 2004). In addition, depression (one component of our index of distress) is a risk factor for chronic physical illness, particularly cardiovascular disease (Glassman and Shapiro, 1998). Hence, by focusing public health attention on persons exhibiting low levels of activity and high levels of psychological distress, it may be possible to address two modifiable risk factors relevant to a wide range of emerging chronic diseases in the developing world.
In summary, our findings support an association between low levels of physical activity and prevalence of psychological distress in the Mekong Delta of Vietnam. The association remained after adjusting for the influence of socio-demographic characteristics, exposure to past trauma, urban–rural residency and the presence of self-reported physical disorders. Further research using longitudinal designs will be needed to establish whether strategic increases in physical activity lead to an amelioration of psychological distress in these settings (Wiles et al., 2007). If such strategies prove effective, then this relatively simple intervention may have substantial utility in primary care, particularly in settings such as Vietnam where more complex and costly psychological and pharmacological treatments, for example for depression, are not yet widely available.
Footnotes
Funding
Funding for this research is from a National Health and Medical Research Council (NHMRC) program grant and a NHMRC project grant. There are no financial or non-financial competing interests.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.