
Abstract
Objective:
To determine the prevalence of cardiometabolic risk factors in Australian adults with a psychotic disorder.
Method:
Data were collected during the interview phase of the second Australian survey of psychosis, a population-based survey of Australians aged 18 to 64 years with a psychotic disorder. Body mass index, waist circumference and blood pressure were measured. Participants were asked about diagnoses of relevant medical conditions, medications, smoking and physical activity. Fasting blood samples were analysed for glucose, high-density lipoprotein cholesterol, total cholesterol and triglycerides. The prevalence of metabolic syndrome was determined using the harmonized criteria developed by the International Diabetes Federation and other bodies.
Results:
A total of 1087 men (60%) and 738 women (40%) participated. Their mean age was 38.36 (SD 11.16) years; 773 (42%) were aged 18–34 years and 1052 (58%) 35–64 years. Three-quarters were overweight or obese and 82% had abdominal obesity. Almost half were hypertensive. Two-thirds were current smokers and 81% had a lifetime history of smoking. Levels of physical activity were very low. About 30% reported a diagnosis of hypertension or high cholesterol, 20% knew they had diabetes or high blood sugar and 18% had cardiovascular disease. Half of those with self-reported hypertension were taking antihypertensive drugs, and about 40% with hypercholesterolemia or hyperglycaemia were receiving medication for these conditions. Seventy per cent (N = 1286) of participants provided fasting blood samples. Abnormal levels of high-density lipoprotein cholesterol and triglycerides were each found in almost half of participants and almost one-third had elevated fasting glucose. More than half of participants (54.8%) met criteria for metabolic syndrome.
Conclusions:
Australians living with psychosis have high rates of cardiometabolic risk factors. There are a number of obvious targets for prevention and treatment, including obesity (especially in women), smoking (more prevalent in men), hypertension, hyperlipidaemia and sedentary lifestyle.
Introduction
People with psychotic disorders have high rates of medical co-morbidity and premature mortality. The life expectancy of men and women with schizophrenia is 18.7 and 16.3 years less than the general population and the life expectancy of men and women with bipolar disorder is reduced by 13.6 and 12.1 years (Laurson, 2011). High rates of cardiovascular disease make a substantial contribution to the poor health and early deaths of people with psychoses (Saha et al., 2007).
Whilst people with psychotic disorders are subject to the usual lifestyle determinants of cardiovascular risk, such as poor diet and lack of exercise, there is additional susceptibility associated with psychosis and its treatment. Some studies suggest that drug-naïve people with first-episode psychosis show evidence of dysglycaemia even before starting antipsychotic medication (Fernandez-Egea et al., 2009). Antipsychotic medications are associated with weight gain (Allison et al., 1999) and Foley and Morley (2011) have demonstrated that cardiovascular risk increases after first exposure to any class of antipsychotic drug. Animal studies have shown that some antipsychotic drugs perturb lipid and triglyceride metabolism independently of weight gain (Skrede et al., 2012). In addition, people with psychotic disorders have higher rates of smoking than the general population (McClave et al., 2010).
The metabolic syndrome has recently come to prominence (Alberti et al., 2009). This is a cluster of closely related risk factors for diabetes and cardiovascular disease, comprising abdominal obesity, hypertension, and at-risk levels of blood glucose, triglycerides and high-density lipoprotein cholesterol (HDL-C). Whilst diabetes is often found in people with metabolic syndrome, metabolic syndrome predicts cardiovascular disease independent of diabetes (Motillo et al., 2010). Several sets of criteria for metabolic syndrome have been developed and we evaluated our participants according to the harmonized criteria developed jointly by a number of bodies representing experts in cardiometabolic risk (Alberti et al., 2009).
The largest previous study to have assessed metabolic syndrome in people with psychotic disorders, the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE), reported on 687 people (McEvoy et al., 2005). CATIE was restricted to people with schizophrenia willing to participate in a clinical trial, so differs from our randomly selected sample of people with any psychotic disorder. Depending on the definition used, metabolic syndrome was found in 40.9% to 42.7% of CATIE participants (over a third of the men and more than half of the women). Compared to the normal US population, matched for age, sex and ethnicity, men in the CATIE study were 138% more likely to meet criteria for metabolic syndrome, and women in the CATIE study were 251% more likely to meet these criteria. Comparisons between the rates of metabolic syndrome in the CATIE and our study are limited by the use of country-specific criteria for abdominal obesity (Alberti et al., 2009). CATIE and other US studies require a waist measurement of more than 102 cm for men and 88 cm for women, whilst the threshold for at-risk waist circumference in Australian studies is 94 cm for men and 80 cm for women.
Many other studies have shown high rates of metabolic syndrome in people with psychotic disorders (de Hert et al., 2006; Khatana et al., 2011; Saari et al., 2005). Baptista et al. (2011) found no difference in rates between their sample of people with psychiatric disorders and a matched general population sample, but there were differences in some of the variables that contribute to metabolic syndrome. Above-threshold waist circumference was significantly more common in people with schizophrenia or bipolar disorder, and in the relatives of people with schizophrenia. All groups of patients and relatives of patients had higher proportions of abnormal blood glucose levels, and this reached significance in those with bipolar disorder and their relatives. In Australia, studies with small sample sizes have found proportions of metabolic syndrome in people with psychotic disorders ranging from 12.5% of an early psychosis sample (Curtis et al., 2011) to 54% of outpatients of a public mental health service (John et al., 2009). Despite recognition of the importance of monitoring cardiometabolic risk factors in people with psychosis, rates of assessment in routine clinical practice are low (Hetrick et al., 2010).
The second Australian survey of psychosis presented an excellent opportunity to collect information on cardiometabolic risk at a national level, utilizing an epidemiological framework, in a large population-based sample of adults with psychotic disorders. To the best of our knowledge, this is the first population-based psychosis prevalence study that has included detailed assessment of cardiometabolic risk factors (including fasting blood samples). The wealth of other data collected in the survey will enable investigation of many factors potentially associated with cardiometabolic health in people with psychotic disorders. This information was not collected in the first Australian survey of psychosis in 1997–98 (Jablensky et al., 2000) and its inclusion in the present study reflects increased recognition of the importance of physical health in people with psychosis. Representative epidemiological data are critical for the estimation of public health impacts and to identify factors, particularly modifiable factors, which place people with psychosis at elevated risk of morbidity relative to the general population. Accurate information is essential for planning effective interventions to reduce morbidity and mortality caused by cardiovascular disease, diabetes and related conditions in this very disadvantaged population.
Methods
Sample
The catchment for the second Australian survey of psychosis covered a population of 1.5 million people aged 18–64 years, approximately 10% of the Australian population in this age group. A two-phase design was used. In Phase 1, screening for psychosis took place in public mental health services and in non-government organizations supporting people with a mental illness. In Phase 2, people who were screen positive for psychosis in Phase 1 were randomly selected, stratified by age group (18–34 years and 35–64 years), for interview and assessment. This process identified 7955 people who were screen positive for psychosis and eligible for interview. Potential participants were randomly selected and approached to participate in the study; 1825 interviews were undertaken in Phase 2 of the study. Diagnostic assessment was based on a semi-structured clinical research interview, the Diagnostic Interview for Psychosis (DIP) (Castle et al., 2006). Diagnoses were made using the ICD-10 classification system (World Health Organization, 1992).
The study was approved by institutional human research ethics committees at each of the seven study sites and all participants provided written, informed consent. Full details of the survey methodology are described by Morgan et al. (2012).
Measures
Status on a range of cardiometabolic risk factors was assessed. Participants’ blood pressure, height, weight and waist circumference were measured by trained research staff using identical equipment and following standardized procedures. Blood pressure was measured electronically. Participants were seated, the arm was freed of constricting clothing, and the appropriate cuff size was selected and wrapped around the upper arm 2–3 cm above the elbow. Electronic scales measuring up to 200 kg were used to assess weight; height (metres) was taken against a measure on a wall. Body mass index (BMI) was calculated as weight/height2. Participants were categorized according to WHO criteria (World Health Organization, 1995) as underweight (BMI < 18.5), normal (BMI 18.50–24.99), overweight (BMI 25.00–29.99) or obese (BMI ≥ 30). Waist circumference was measured by locating the top of the hip bone and placing the tape measure evenly around the abdomen at the level of the hip bone. The participant was asked to breathe out gently and the measurement was taken at the end of a normal expiration.
Participants were asked if they had a history of high blood pressure or high cholesterol and if they had diabetes or had been told that their blood sugars were high. Diagnosed cardiovascular disease was ascertained by asking participants if they had ever been told by a doctor that they had any of the following: heart attack, angina, stroke/transient ischaemic attack (TIA), or other heart disease, e.g. arrhythmias. They were asked to bring all medications to the interview and those relevant to cardiometabolic conditions were identified. Lifetime smoking status was determined by asking whether they had ever regularly smoked cigarettes, tobacco, cigars or a pipe. Current smoking was defined as self-reported smoking in the 4 weeks prior to the interview. The International Physical Activity Questionnaire (Craig et al., 2003) was used to assess the amount of time participants spent in both vigorous and moderate exercise, and the amount of time they spent sitting on a typical weekday, during the last 7 days. The total time spent in various activities over the previous 7 days was classified according to criteria from the National Survey of Mental Health and Wellbeing (Australian Bureau of Statistics, 2008) into four levels of activity: very low, low, moderate and high.
Participants fasted overnight (minimum of 8 hours) then provided venous blood samples for measurement of plasma glucose, triglyceride, HDL-C and total cholesterol concentrations. These analyses were undertaken by standard methods in accredited pathology laboratories in each catchment area. More than 70% (N = 1286) of the 1825 survey participants provided fasting blood samples. A further 106 people provided blood samples which were non-fasting and these samples were not included in the analyses.
Metabolic syndrome
Metabolic syndrome was defined using the harmonized criteria developed by the International Diabetes Federation Task Force on Epidemiology and Prevention and related expert organizations (Alberti et al., 2009). These criteria for metabolic syndrome require three of the following five risk factors to make the diagnosis: abdominal obesity (at-risk waist circumference); at-risk diastolic and/or systolic blood pressure; at-risk levels of fasting blood glucose, triglycerides or HDL-C. Abdominal obesity was defined as a waist circumference ≥ 94 cm for men and ≥ 80 cm for women. Hypertension was diagnosed if the person had a systolic blood pressure ≥ 130 mmHg and/or a diastolic pressure ≥ 85 mmHg. The thresholds for blood glucose, triglycerides and lipids were: glucose ≥ 5.6 mmol/l; triglycerides ≥ 1.7 mmol/l; HDL-C < 1.0 mmol/l for men and < 1.3 mmol/l for women. People receiving medications for hypertension, hyperlipidaemia or hyperglycaemia were considered to meet the relevant criterion. In addition to HDL-C, required for the diagnosis of metabolic syndrome, we also report rates of elevation of total cholesterol, defined as levels ≥ 5.5 mmol/l.
Analysis
Descriptive statistics were used to summarise characteristics of the participants. Reflecting age stratification in the survey design, two age groups were formed, those aged 18–34 years and those aged 35–64 years. All group differences were evaluated using a χ2 test for categorical variables and t-tests for continuous variables. Analyses were conducted using the Statistical Package for Social Sciences Version 20.
Results
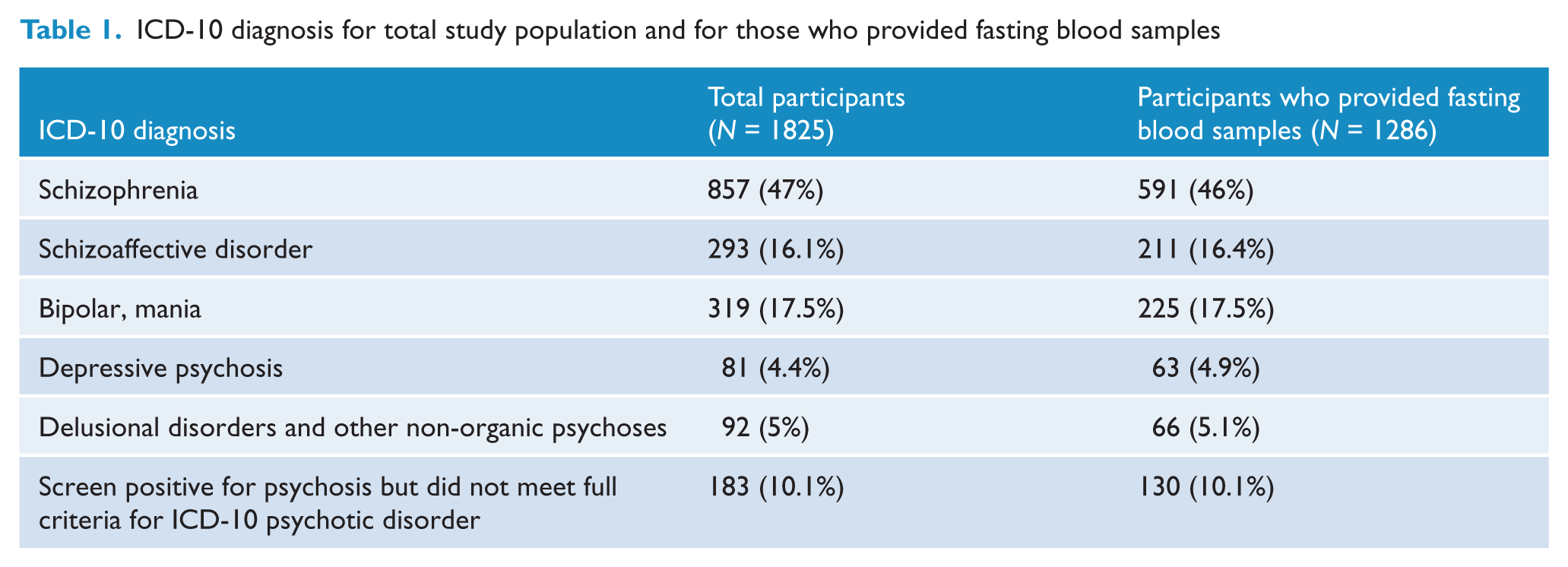
In total, 1087 (59.6%) men and 738 (40.4%) women gave consent and were interviewed. Their mean age was 38.36 (SD = 11.15) years; 37.46 (SD = 10.92) years for men and 39.7 (SD = 11.37) years for women (t = −4.22, df = 1823, p = 0.000). Just under half (N = 773; 42.4%) were aged 18–34 years and 1052 (57.6%) were aged 35–64 years. A higher proportion of men (46.5%) than women (36.3%) were in the younger age group (χ2 = 18.52, df = 1, p = 0.000). Diagnoses, based on the ICD-10 classification system (World Health Organisation, 1992), are presented in Table 1 for both the total survey population and for those who provided fasting blood samples.
ICD-10 diagnosis for total study population and for those who provided fasting blood samples
Smoking
Smokers reported an average of 21 cigarettes per day. Current tobacco use was significantly more common in men than women (χ2 = 31.06, df = 1, p = 0.000) and in the younger compared to the older cohort (χ2 = 9.83, df = 1, p = 0.001) (Table 2). The difference between male and female rates of current smoking was more pronounced in the younger cohort (χ2 = 16.04, df = 1, p < 0.0001) compared to the older cohort (χ2 = 12.9, df = 1, p = 0.001) but was highly significant in both age groups. Lifetime smoking was also more common in men (χ2 = 43.69, df = 1, p < 0.0001) but there was no difference in rates of lifetime smoking between the younger and older age groups.
Current and lifetime tobacco use by age and sex
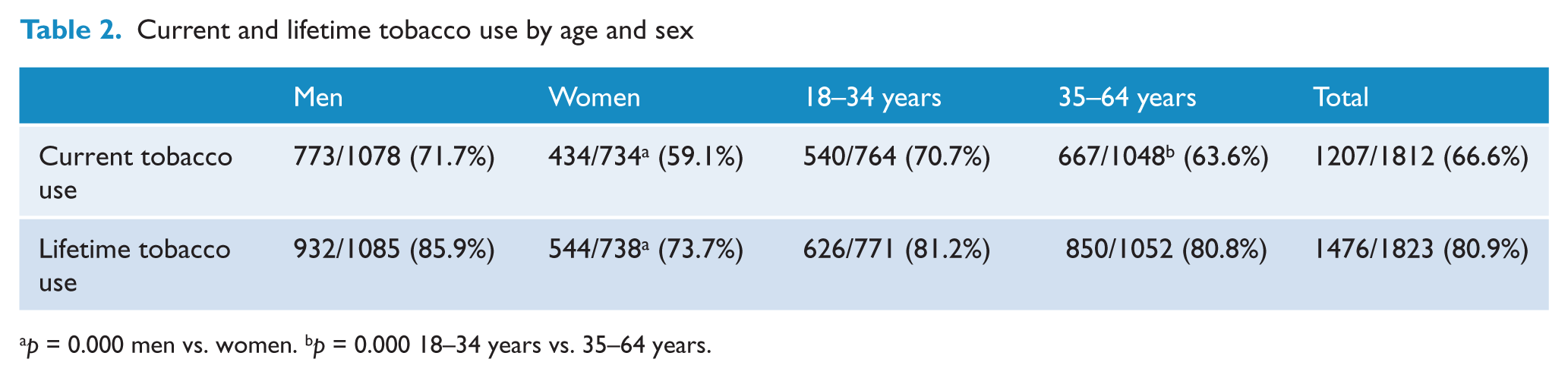
p = 0.000 men vs. women. bp = 0.000 18–34 years vs. 35–64 years.
Physical activity
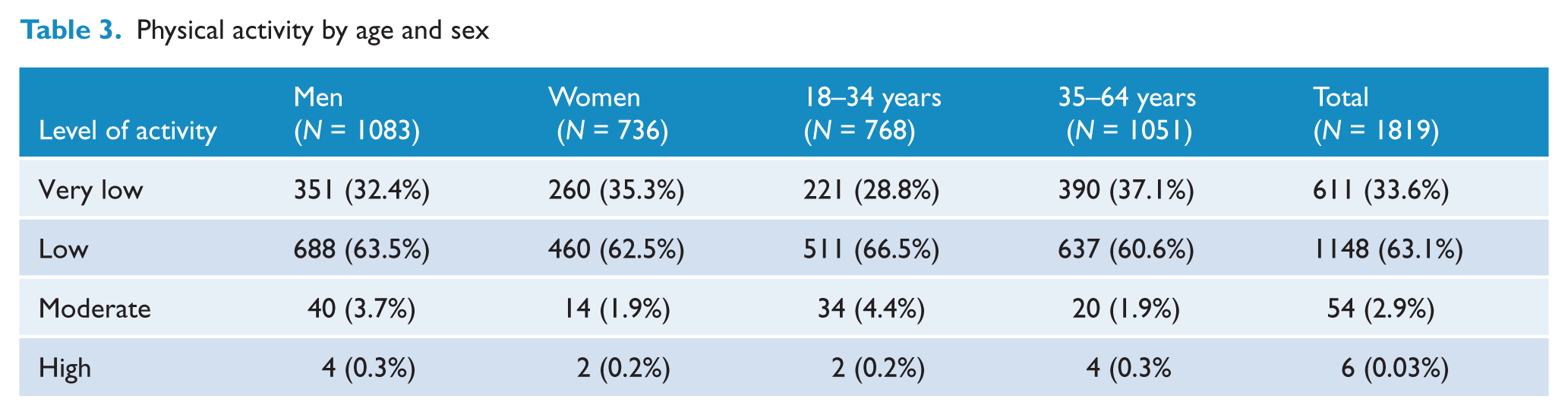
Almost all (96.7%) participants engaged in low or very low levels of activity (Table 3). The younger participants were more active in that they were significantly more likely to engage in low rather than very low levels of exercise, compared to the older age group (χ2 = 11.42, df = 1, p = 0.000). There was no difference between men and women in the level of physical activity.
Physical activity by age and sex
Obesity
BMI
Table 4 shows that 75.5% of the total sample was overweight or obese. The proportion of men and women who were underweight or normal weight was similar, but in the overweight/obese categories women were more likely to be obese rather than overweight compared to men (χ2 = 24.67, df = 3, p < 0.0001). The older cohort was more likely to be overweight or obese than the younger cohort (χ2 = 54.12, df = 3, p < 0.0000).
BMI by age and sex
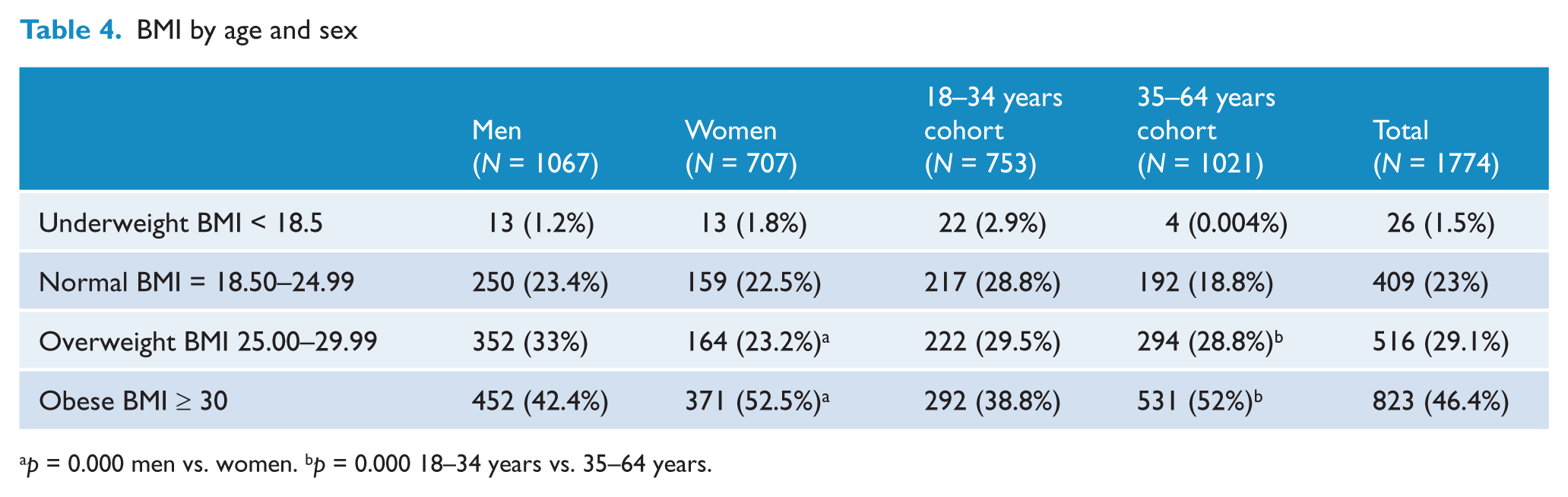
p = 0.000 men vs. women. bp = 0.000 18–34 years vs. 35–64 years.
Waist circumference
Abdominal obesity was present in 82.1% of participants; 91.2% (641/703) of women and 76.1% (807/1060) of men; 74.5% (555/745) of the younger cohort and 87.7% (893/1018) of the older cohort. Younger and older women were more likely to have abdominal obesity than younger and older men (87.3% vs. 68%, χ2 = 32.86, df = 1, p < 0.0001; 93.3% vs. 83.2%, χ2 = 23.80, df = 1, p < 0.0001, respectively), but the sex difference was most marked in the younger age group.
Blood pressure
Overall, 861 participants (47.2%) met criteria for hypertension. Whilst diastolic hypertension was equally common in men and women, men had higher rates of systolic hypertension (χ2 = 35.59, df = 1, p = 0.000) (Table 5). Both systolic and diastolic hypertension were more common in the older age group (χ2 = 46.07, df = 1, p = 0.000 for diastolic; χ2 = 27.9, df = 1, p = 0.000 for systolic). The higher rate of systolic hypertension in men was more pronounced in the younger (χ2 = 31.12, df = 1, p = 0.000) than the older age group (χ2 = 17.03, df = 1, p = 0.000).
Hypertension by age and sex
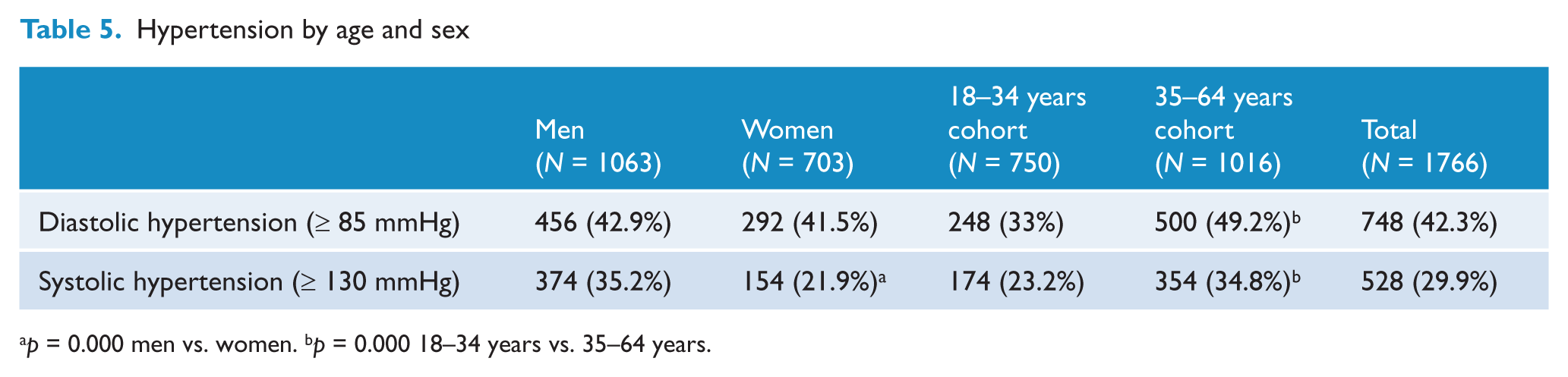
p = 0.000 men vs. women. bp = 0.000 18–34 years vs. 35–64 years.
Diagnosed hypertension, hypercholesterolemia, hyperglycaemia/diabetes and cardiovascular disease
A declared diagnosis of high cholesterol was significantly more common in women (χ2 = 46.07, df = 1, p = 0.014) whilst there was no gender difference in diagnosed hypertension or hyperglycaemia/diabetes (Table 6). Cardiovascular disease, including stroke, had been diagnosed in 238 of 1811 participants (13.1%), 134 men (12.4%) and 104 women (14.3%); this gender difference was not significant.
Diagnoses of diabetes/hyperglycaemia, hypertension and hypercholesterolemia by age and sex
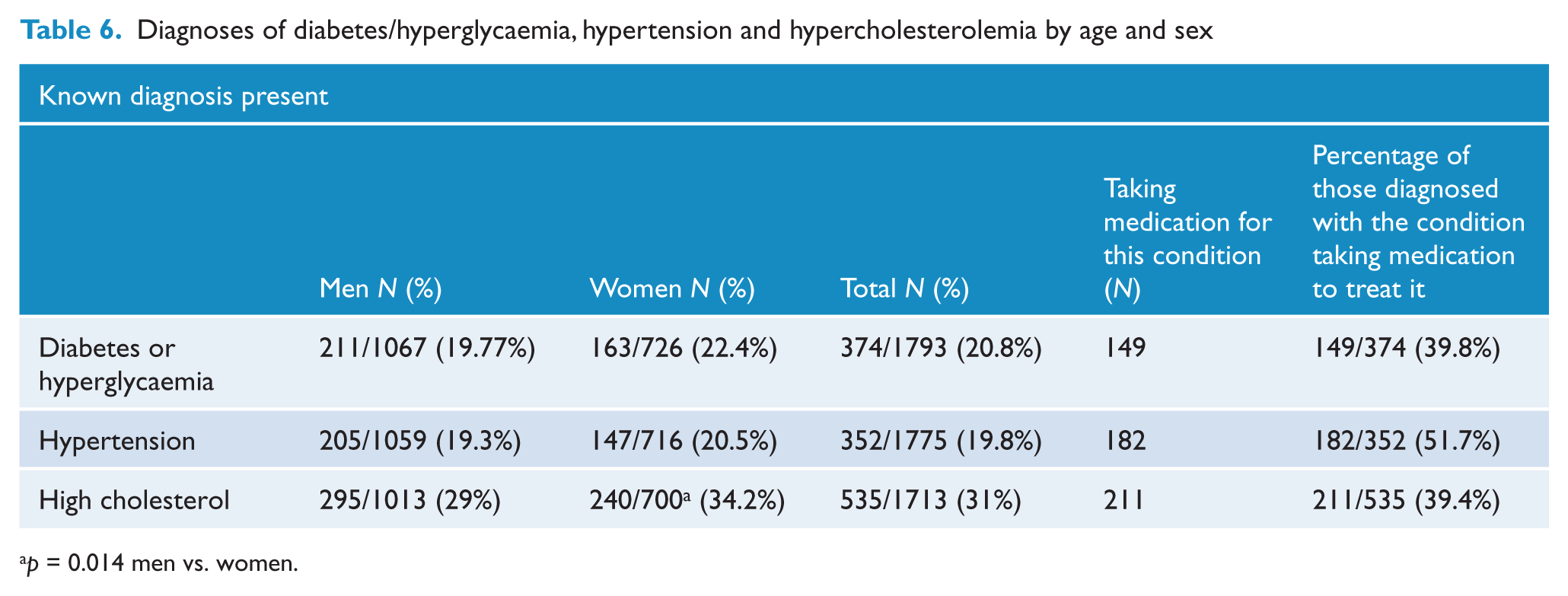
p = 0.014 men vs. women.
Fasting plasma cholesterol, glucose and triglycerides
Fasting blood samples were provided by 1286 participants. Of these, 586 were aged 18–34 years and 806 were 35–64 years; 851 (61%) were men. Their mean age was 38.37 (SD = 10.96) years. There was no difference between participants who provided fasting blood samples and those who did not in terms of age group, gender, BMI category, level of education, school-leaving age, lifetime smoking or waist circumference.
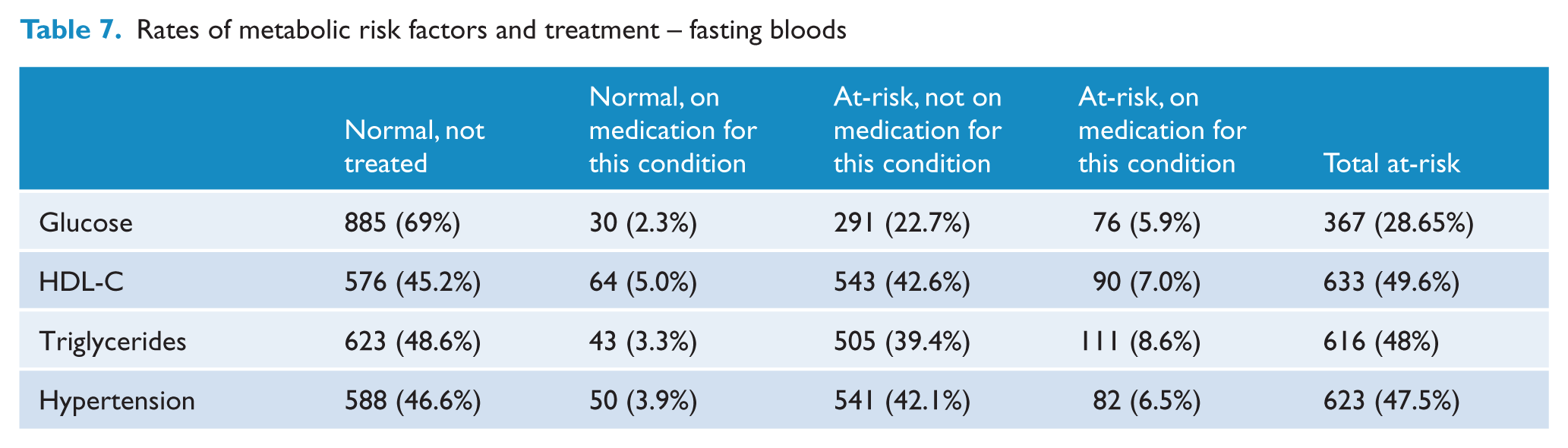
One-third of these participants (N = 426) had elevated total cholesterol. Sixty per cent of those with elevated cholesterol were men; this gender difference was not significant. Table 7 shows the proportion with abnormal levels of glucose, HDL-C and triglycerides. Men were more likely to have elevated glucose (χ2 = 3.78, df = 1, p = 0.03) and triglycerides (χ2 = 8.08, df = 1, p = 0.003); there was no significant gender difference in HDL-C. Most people with elevated levels of glucose, triglycerides or HDL-C were untreated, and the majority of those receiving treatment still had abnormal levels (Table 7).
Rates of metabolic risk factors and treatment – fasting bloods
Metabolic syndrome
When the harmonized criteria were applied, 704 (54.8%) of participants met criteria for metabolic syndrome, 420 (54.6%) of the men and 284 (55%) of the women. There was no significant gender difference in the prevalence of metabolic syndrome.
Discussion
More than half of people with psychotic disorders participating in this study had metabolic syndrome. General population data for Australians aged 25 years and over indicates that the proportion with metabolic syndrome is 13.4% to 30.7%, depending on the definition used (Cameron et al., 2007). The second Australian survey of psychosis therefore establishes at a population level that the cardiometabolic health of Australians living with a psychotic illness is substantially poorer than the cardiometabolic health of the general population. Our findings are consistent with previous studies that report worryingly high proportions of metabolic syndrome in people with psychotic disorders (de Hert et al., 2006; Khatana et al., 2011; McEvoy et al., 2005; Saari et al., 2005).
The prevalence of metabolic syndrome was approximately 10% higher in our sample than in the US CATIE sample. However, the difference in prevalence could be fully or partially accounted for by the use of a higher threshold for abdominal obesity in CATIE (McEvoy et al., 2005). There were a number of other important differences – the CATIE sample was restricted to schizophrenia, and excluded people with serious and unstable medical conditions. CATIE participants had been treated with antipsychotics for an average of 14 years, and despite such lengthy treatment were somewhat treatment refractory as they had agreed to switch their medications in a randomized trial. There is a clear need to further explore whether Australians receiving treatment for psychosis are at greater risk of metabolic syndrome than people with psychosis treated in other settings.
We found that more than 80% of our participants had abdominal obesity. Antipsychotic medications are a major cause of weight gain (Foley and Morley, 2011) and 81.6% of our sample was taking antipsychotics, with 74.0% of the total using atypical antipsychotics and 15.2% using typical antipsychotics. Some 37.5% reported weight gain associated with medication use (Waterreus et al., 2012). The mean amount gained in the previous 6 months was 9 kg. Medication is therefore likely to be a major contributor to the high rates of obesity in survey participants.
Abdominal obesity was present in over 90% of women and in 76% of men participating in the survey. The gender difference was more pronounced in those with the highest BMI (> 30). The CATIE study found more than double the rate of abdominal obesity in women (McEvoy et al., 2005). In contrast, the Ausdiab study (Barr et al., 2006) reported only a small gender difference in the general Australian population, with abdominal obesity present in 56.5% of women and 55.2% of men. There has been surprisingly little research into the reasons why women with psychotic disorders are especially prone to obesity.
Virtually all of our participants were sedentary or undertook very little exercise. Such a lack of exercise would be expected to have an adverse effect on health, lifestyle and emotional well-being. There are numerous factors that could contribute to the low levels of physical activity in people with psychosis, including subsidiary symptoms such as depression and negative symptoms. Exercise could be less enjoyable due to low levels of fitness, aggravated by obesity, poor physical health and smoking. Lack of money and poor social engagement might also limit opportunities to take part in physical activities. Several small studies have shown that improvements in physical activity are possible in people with psychotic disorders, using a range of approaches including motivational interventions (Beebe et al., 2011) and the use of internet-enabled mobile devices (Killackey et al., 2011).
The self-reported prevalence of cardiovascular disease was 18% and this may underestimate the actual prevalence, given the likelihood of under-ascertainment. Further investigation of the standardized mortality risk of cardiovascular disease in our cohort relative to the background population is required. The extent to which traditional risk factors account for the excess cardiovascular disease in our patients is uncertain. It is likely that other unmeasured factors, such as hypercortisolism, hyperadrenergic stimulation, inflammation, oxidative stress, endothelial dysfunction and genetic susceptibility play a major role. It is noteworthy that the metabolic syndrome may be a more important marker of longer-term risk of cardiovascular disease, whereas traditional risk factors, such as cholesterol, smoking and diabetes, might be more useful in predicting shorter-term risk of cardiovascular disease (Grundy et al., 2004).
About half the participants with diagnosed hypertension were taking antihypertensive medications, and about 40% were receiving medication for known diabetes/hyperglycaemia or elevated cholesterol. Whilst some might have been offered dietary and lifestyle advice rather than medication, the very high rates of obesity and metabolic syndrome suggest that such measures alone would generally not be adequate. When these parameters were measured, between 22% and 43% of participants were hypertensive or had abnormal fasting blood glucose or lipids and were not taking appropriate medications. These results indicate a failure of treatment when these conditions are diagnosed, with an even higher rate of undiagnosed and untreated metabolic abnormalities. Despite improvements in the early detection of psychosis, and the implementation of community-based services for those with severe and persistent mental illness, our health systems are failing to provide optimal care for their co-morbid physical health problems (Organ et al., 2010). This problem is widely appreciated and features prominently in the Fourth National Mental Health Plan (Commonwealth of Australia 2009).
Two-thirds of participants in the survey were currently smoking. In contrast, Australian population figures from 2010 showed that only 15.1% (16.4% of males and 13.9% of females) currently smoked and 42.2% reported that they had ever smoked (Australian Institute of Health and Welfare, 2011). In both our sample and the general population, males were more likely to smoke. Public health programmes to reduce smoking have had little impact on the high rates of smoking by people with psychoses. This highlights the need for specific smoking cessation programmes for people with mental illness, and previous research (Ashton et al., 2010) has shown that this approach can be successful.
This study had some limitations. Ethnicity is an important correlate of metabolic syndrome, and whilst the survey asked about country of birth, this did not provide accurate information about ethnicity. We excluded people who could not speak English sufficiently well to participate in the interview, so migrants from non-English-speaking backgrounds will be under-represented. Not all participants provided fasting blood samples, and whilst no differences were found between those who did and did not provide fasting bloods, there may have been an undetected bias. We were not able to include concurrent assessment of the general population. However, future studies will compare the variables of interest in survey participants with an age- and sex-matched Australian general population sample.
In conclusion, the second Australian survey of psychosis establishes that Australians with psychotic disorders are at very high levels of cardiometabolic risk. A number of factors involving the illness itself, lifestyle, antipsychotic drugs, and lack of treatments targeting cardiometabolic disorders, are clearly important. There is an urgent need to develop and evaluate effective interventions, targeting the specific needs of people with severe mental illnesses. In terms of possible interventions to address the increased morbidity and mortality from physical illness, the most comprehensive population-based study was the ‘Duty to Care’ project from Western Australia (Lawrence et al., 2001). This project suggested that much of the mortality was avoidable and that assertive management of co-morbid physical disorders had the potential to close the differential mortality gap. Monitoring programmes have since been developed but their implementation has been quite limited (Mitchell et al., 2012). There are several models for treatment services including shared care with general practitioners, and monitoring and treatment on-site in community mental health services (De Hert et al., 2010). Greater awareness of the differential weight gain caused by the various antipsychotic drugs might be helpful in reducing obesity. Data from the second Australian survey of psychosis provides a compelling picture of the extent of the cardiometabolic risks and morbidity suffered by people living with psychotic disorders, and it is essential that this be addressed.
Footnotes
Acknowledgements
This paper is based on data collected in the framework of the 2010 Australian National Survey of High Impact Psychosis. The members of the Survey of High Impact Psychosis Study Group are: V Morgan (National Project Director), A Jablensky (Chief Scientific Advisor), A Waterreus (National Project Coordinator), R Bush, V Carr, D Castle, M Cohen, C Galletly, C Harvey, B Hocking, A Mackinnon, P McGorry, J McGrath, A Neil, S Saw and H Stain. Ethics approvals for the study were obtained from relevant institutional human research ethics committees.
The authors acknowledge, with thanks, the hundreds of mental health professionals who participated in the preparation and conduct of the survey and the many Australians with psychotic disorders who gave their time and whose responses form the basis of this publication.
Funding
This study was funded by the Australian Government Department of Health and Ageing.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.