
Abstract
Objective:
Participation in mainstream education and employment facilitates both the recovery and the social inclusion of people with psychotic disorders. As part of the second Australian survey of psychosis, we assessed labour force activity and participation in formal education among working age adults with psychotic disorders.
Method:
Data were drawn from a large national community prevalence survey of adults with psychotic disorders. Known as the Survey of High Impact Psychosis (SHIP), it was conducted in seven Australian catchment areas during March to December 2010. Current and past year labour force activity, current employment, past year participation in formal education and vocational training, and key clinical and demographic characteristics were examined in a sample of 1825 participants.
Results:
Only 22.4% of people with psychotic disorders were found to be employed (either full-time or part-time) in the month prior to the survey. In the previous 12 months, 32.7% were employed at some time. Of those in competitive employment, the majority worked part-time (63.9%), while a quarter worked 38 or more hours per week (23.4%). In terms of educational attainment, 18.4% reported difficulties with reading or writing, while 31.9% completed high school, which represents 12 years of formal education.
Conclusions:
The proportion currently employed has remained stable at 22% since the last national survey in 1997. Policy makers and service providers could do more to ensure people with psychotic disorders obtain access to more effective forms of assistance with respect to both their continuing education and employment. More effective vocational and educational interventions for people with psychotic disorders appear to be urgently needed.
Keywords
Introduction
People with psychotic disorders are among the most socially and economically marginalised members of the community. In particular, because of the disabling nature of these disorders, educational and employment-related outcomes are often compromised. Apart from the impact on the individual, these issues result in substantial economic consequences at the societal level (Kessler et al., 2008). Based on surveys from 19 nations, reduced earnings associated with serious mental disorders (which include psychotic disorders) account for 0.3–0.8% of total national earning (Levinson et al., 2010).
With respect to employment, those with psychotic disorders experience high levels of non-participation and exclusion from the labour force. Population level studies show consistently severe impacts on employment among people with psychotic disorders. For instance, in the UK, only 27% of 200 people with probable psychotic disorder were found to be employed (O’Brien et al., 2002). In the USA, the proportion of those with schizophrenia employed was even lower (20.5–22.5%) (Mechanic et al., 2002; Zwerling et al., 2002).
In Australia, the proportions of those with schizophrenia and employed based on studies conducted in 1998 and 2003 were 19% and 16%, respectively (Waghorn et al., 2009). This contrasts with employment rates of 74% and 77% among healthy working age Australians in 1998 and 2003. In the first national survey of psychotic disorders undertaken in 1997 (Jablensky et al., 1999, 2000; Waghorn and Chant, 2002; Waghorn et al., 2003), of those not in long-term psychiatric institutions (n = 782), only 23.9% of females (n = 69) and 21.3% of males (n = 105) were employed at the time of interview (n = 174; 22.2%).
Over the years since the first survey, labour market conditions have changed and demand for labour has increased. National unemployment rates (seasonally adjusted) were 8.5% in 1997, and 5.2% in 2010 (Australian Bureau of Statistics, 1997, 2010). In addition, the availability of suitably intensive employment services in Australia has increased due to continuing expansion and improvements to the program over the past decade (Australian Government, 2009b).
Australia has three types of labour force programs relevant to people with psychotic disorders (Waghorn et al., 2012), which are widely available throughout Australia. Labour force programs are the responsibility of the Federal Government and are administered by the Department of Education, Employment, and Workplace Relations (DEEWR) as the sole purchaser of contracted services. Services are typically provided by non-government organizations (for-profit and not-for-profit) and consist of: (1) mainstream services for unemployed persons and sole parents (known as Job Services Australia) with four levels of service intensity depending on the extent of the job-seekers’ disadvantage; and (2) Disability Employment Services, which are further divided into two distinct programs. Disability Management Services are for job seekers with disability, injury or health conditions, who require the assistance of a disability employment service, but who are not expected to need long-term support, greater than 6 months, in the workplace. The second Disability Employment Service program is an Employment Support Service for job seekers with permanent disability, and with an assessed need for more long-term and more regular support in the workplace. Of these three systems, the latter two are intended to include people with severe mental illness such as psychotic disorders. The Job Services Australia system is not intended for, and not considered suitable for, people with severe mental illness unless they can be described as no longer having, or at future risk of having, work restrictions, impairments, or disabilities related to their current or previous diagnosis.
With respect to educational achievements, the 1997 survey of psychosis found that 47.8% of the participants with psychosis had neither completed secondary schooling nor attained any further post-school qualification (compared to 36.8% for the Australian population) (Jablensky et al., 1999). Not completing 12 years of formal education can limit employment options to less skilled jobs, flatten career trajectories and reduce potential earnings (Tsang et al., 2010; Waghorn et al., 2003, 2004).
As part of the second national survey of psychosis, we had the opportunity to explore employment and education-related outcomes in a large representative sample of individuals with psychotic disorders. The main aim of this paper was to present key descriptive statistics related to: (a) current and past year labour force activity; (b) educational achievements; and (c) demographic and clinical correlates of these parameters. In light of the policy changes implemented during the 14 years since the first national survey, and in light of the increased demand for labour in recent years, we predicted that educational outcomes would have improved in the second national survey of psychosis. In addition, we wished to examine the association between educational outcomes with employment outcomes – we predicted that those with better educational achievements would be more likely to be employed.
Methods
Participants
Participants were drawn from the second national survey of psychosis, the Survey of High Impact Psychosis (SHIP). The full details of the methodology are described elsewhere in this volume (Morgan et al., 2012). In summary, SHIP encompassed seven catchment areas (including inner city, urban and rural settings) covering some 62,000 square kilometres and a population of 1.5 million people aged 18–64 years (approximately 10% of the Australian population in this age group). A two-phase design was used. In Phase 1, screening for psychosis took place in public specialised mental health services and in non- government organisations supporting people with a mental illness. In Phase 2, people who were screen-positive for psychosis in Phase 1 were randomly selected, stratified by age group (18–34 years and 35–64 years), for interview and assessment. The census month was March 2010. Of 7955 people who were screen-positive for psychosis and eligible, 1825 were interviewed in Phase 2. Diagnoses were derived from 10th edition of the International Classification of Disease (ICD-10) (World Health Organization, 1992). For details related to the use of the psychosis screen item, further details are described elsewhere in this volume (Morgan et al., 2012).
Measures
Data were collected on symptomatology, substance use, cognitive ability, functioning, disability, physical health, mental health service utilisation, medication use, education, employment and housing. Trained interviewers (all health care professionals) administered the survey. Further details of the survey are available in the full report (Morgan et al., 2011). The study was approved by institutional human research ethics committees at each of the seven study sites and all participants provided written, informed consent.
With respect to employment and education, a broad range of items were designed to assess the previous 4 weeks’ and past 12 months’ engagement with the workforce and formal education. Definitions for employment and education were similar to those used in the first national survey (Castle et al., 2006; Jablensky et al., 2000). An internationally agreed definition of labour force activity was used, as recommended by the Australian Bureau of Statistics (Australian Bureau of Statistics, 2010). By this definition, unemployment is defined as a proportion of labour force participants, a reference group typically including people aged 15–64 years, who when surveyed are either currently employed (worked 1 hour or more in the reference week) or who met criteria for actively looking for work. Those classified as not participating in the labour force include discouraged job seekers no longer actively looking for work, those not registered with an employment service, home-makers, parents, carers, students, people who consider the labour force not applicable, or those who consider themselves retired from the labour force. In keeping with standard definitions used in this field, we examined the participants in terms of whether they were employed or not in the previous 4 weeks, and defined full-time work as at least 38 hours’ work per week. However, looking for work, not participating in the labour force, and other activities could only be examined in the previous 12 months.
International definitions of labour force activity were applied to determine three mutually exclusive categories of labour force activity: employed (competitive and non-competitive), looking for work (LFW), and not participating in the labour force (NILF) in the previous 12 months. ‘Competitive employment’ (also known as ‘open employment’ in Australia) is defined as part-time or full-time work in the open labour market at or above minimum award wages, in jobs not reserved for people with disabilities, where supervision is provided by personnel regularly employed by the business. ‘Non-competitive employment’ has been defined as ‘unpaid work of any type, jobs that pay below award wages, jobs reserved for people with disabilities, jobs where the employer continues to receive a wage subsidy, wages paid under the supported wage scheme award, or jobs in work environments designed specifically to employ people with health conditions or disabilities’.
For the assessment of global functioning, we examined quartiles derived from the Personal and Social Performance Scale (PSP) (Morosini et al., 2000). The PSP is a clinician-rated measure of severity of personal and social dysfunction. Patient functioning is assessed in four main areas: socially useful activities; personal and social relationships; self-care; and disturbing and aggressive behaviours. Difficulty in each area is rated on a single item using a six-point scale: absent; mild; manifest but not marked; marked; severe; or very severe. Scores range from 1 to 100 (in 10-point intervals), where lower scores indicate poorer functioning. It has good inter-rater reliability (intraclass correlation coefficient = 0.87) and good test–retest reliability (intraclass correlation coefficient > 0.90) (Patrick et al., 2009).
Descriptive statistics (frequency and proportions) were used to summarize key variables. Unadjusted correlates of labour force activity (current and 12 months) were estimated using univariate Wald chi-squared test. All analyses were conducted with SAS (version 9.2; SAS Institute, Cary, NC, USA).
Results
Demographic and clinical characteristics of participants by labour force activity in the previous 12 months and current employment (in the previous 4 weeks) are shown in Table 1. Of the 1825 participants with psychotic disorders, the majority were male (60.0%), non-partnered (82.9%), aged 18–44 years (69.5%), and Australian-born (82.2%). In addition, 9.2% reported speaking a first language other than English at home. The majority met ICD-10 research diagnostic criteria for schizophrenia (46.7%), schizoaffective disorder (16.1%) and bipolar affective disorder (17.5%).
Demographic and clinical correlates of labour force activity among people with psychotic disorders.
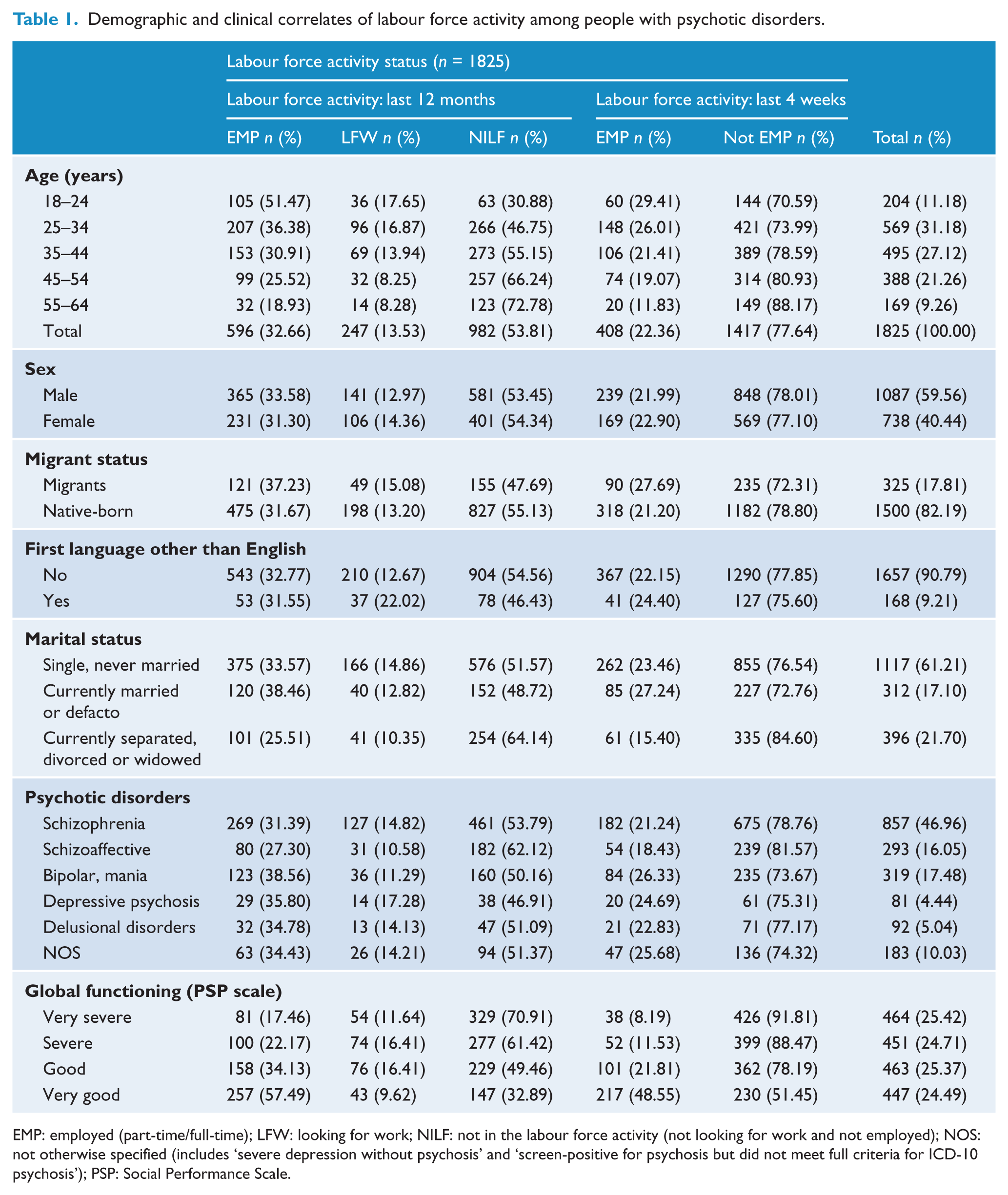
EMP: employed (part-time/full-time); LFW: looking for work; NILF: not in the labour force activity (not looking for work and not employed); NOS: not otherwise specified (includes ‘severe depression without psychosis’ and ‘screen-positive for psychosis but did not meet full criteria for ICD-10 psychosis’); PSP: Social Performance Scale.
Current employment
Overall, 22.4% (n = 408) were currently employed (in the previous 4 weeks) either full-time or part-time; 32.7% (n = 596) had been employed in the previous 12 months. Similar proportions of males and females were currently employed (22.0 vs 22.9%, χ2 = 0.21, p = 0.65). There was no association between language spoken at home (English versus other) and current employment (χ2 = 0.45, p = 0.50). However, migrants were more likely to be employed during the previous 4 weeks (27.7 vs 21.2%; χ2 = 6.49, p = 0.01), as were those with partners (χ2 = 16.09, p = 0.0003). There was a negative monotonic gradient between age and current employment, with older age groups less likely to be employed and participating in the labour force (χ2 = 23.67, p < 0.0001). Overall, employment did not vary significantly by diagnostic category (χ2 = 7.56, p = 0.18), yet at a trend level, more participants with bipolar affective disorder (38.6%) were employed in the previous year than those with schizophrenia (31.4%) or schizoaffective disorder (27.3%). There was a negative, monotonic gradient between global functioning and current employment, as rated by interviewers using the PSP. Those rated as in the most severe category of illness were less likely to be currently employed (χ2 = 212.69, p < 0.0001) (see Table 1).
Employment in the previous year
Of the 596 participants who were employed during the previous year, 82.8% (n = 491) worked in open competitive employment, and 17.2% in non-competitive forms of employment (Table 2). Those in competitive employment worked more hours per week (mean = 25.3,SD = 15.7) compared to those in non-competitive forms of employment (mean = 13.5, SD = 9.6). Those in competitive employment were more likely to receive wages at or above the minimum wage (94.9% vs 5.1%). Proportionally, those in non-competitive employment were more severely ill than those in competitive employment (χ2 = 50.86, p < 0.0001) (Table 3). Yet, of those currently employed whose illness was classified as very severe (n = 81), the majority (61.7%, n = 50) were competitively employed. In addition, 42.1% (n = 43) of those in non-competitive employment had global functioning ratings of good to very good. These results highlight the limitations of severity of disability as the basis for allocating people to either competitive or non-competitive forms of employment assistance.
Characteristics of work force activity among those employed, last 12 months (n = 596).
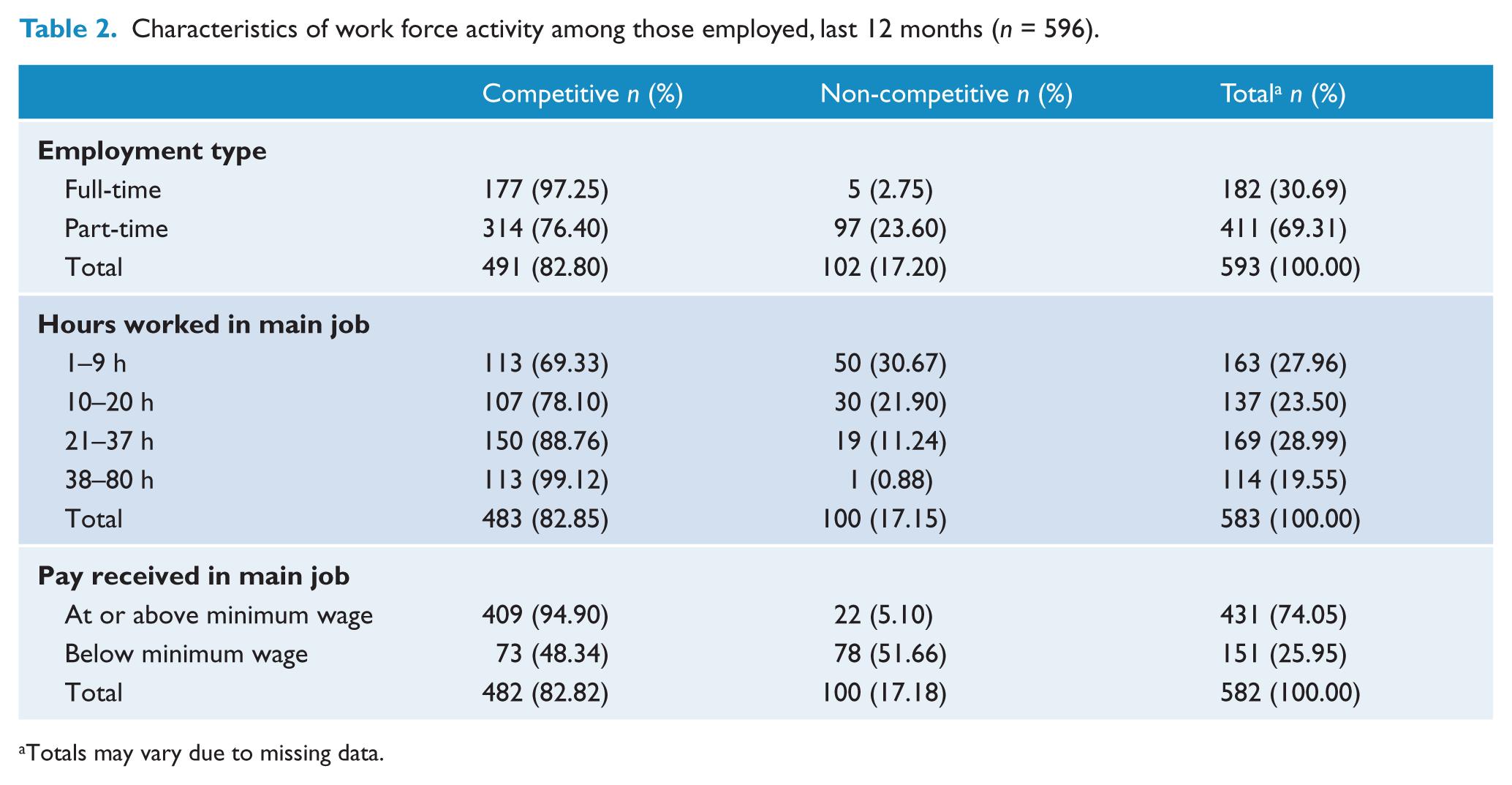
Totals may vary due to missing data.
Global functioning (PSP scale) and status of employment among those employed, last 12 months (n = 596).
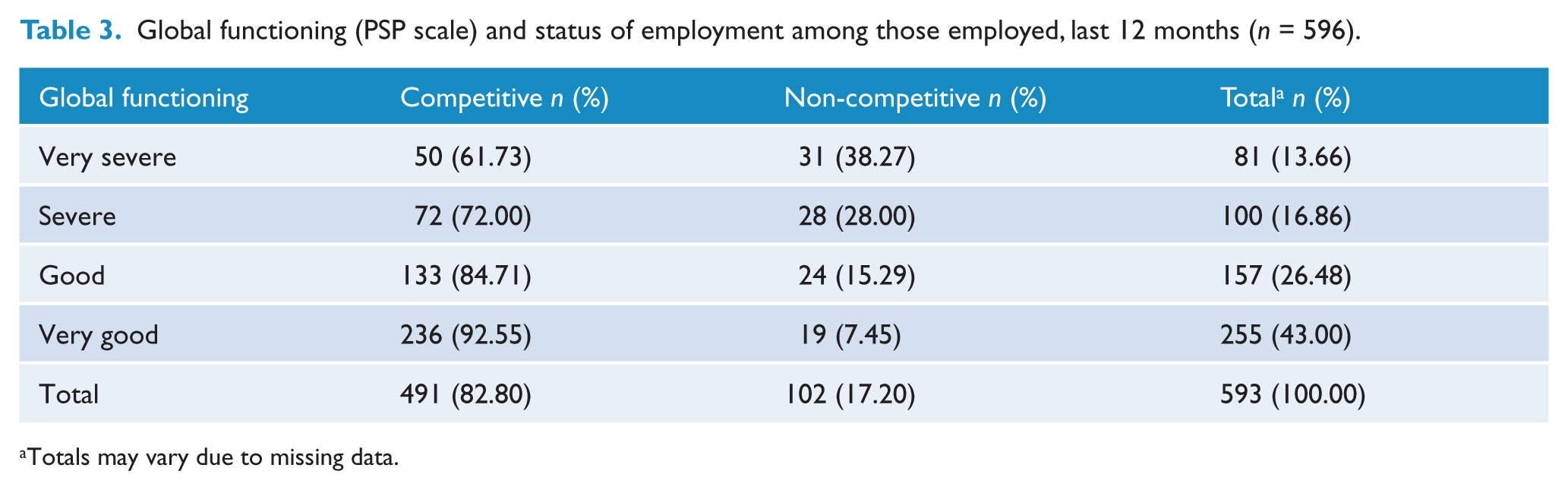
Totals may vary due to missing data.
Pathways to employment
Of the 408 participants who were currently employed, only 22.1% reported obtaining their main job through an employment agency or a disability employment service (Table 4). Disability employment services are considered the most appropriate forms of employment assistance for people with severe forms of mental illness or psychiatric disabilities. Most reported using their own resources to secure employment (76.2%, derived from Table 4). Among those actively looking for work (LFW), the majority (69.1%, n = 170) had searched advertisements (newspapers, internet sites, noticeboards), while over half (55.7%, n = 137) had registered with an employment agency. Most did not rely on these strategies alone, because 52.0% (n = 128) also directly ‘wrote, phoned, or applied in person’ for jobs (Table 5). Among those looking for work in the previous year (n = 247), 32.1% (n = 79) received assistance from a mainstream unemployment service, and only 30.5% received assistance from a disability employment service (Table 6).
Pathways to employment in those currently employed (n = 408) and not currently employed (n = 1417), last 4 weeks.
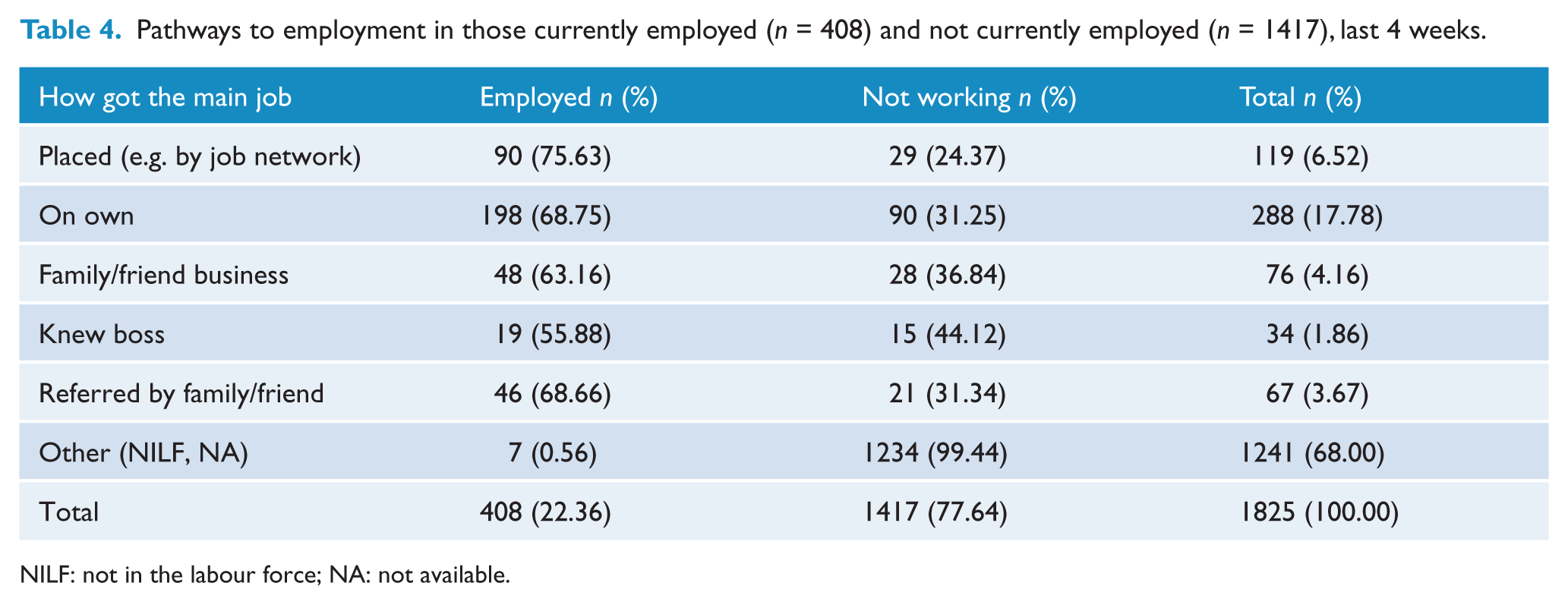
NILF: not in the labour force; NA: not available.
Job-seeking activities in those looking for work (LFW, n = 247), last 12 months.
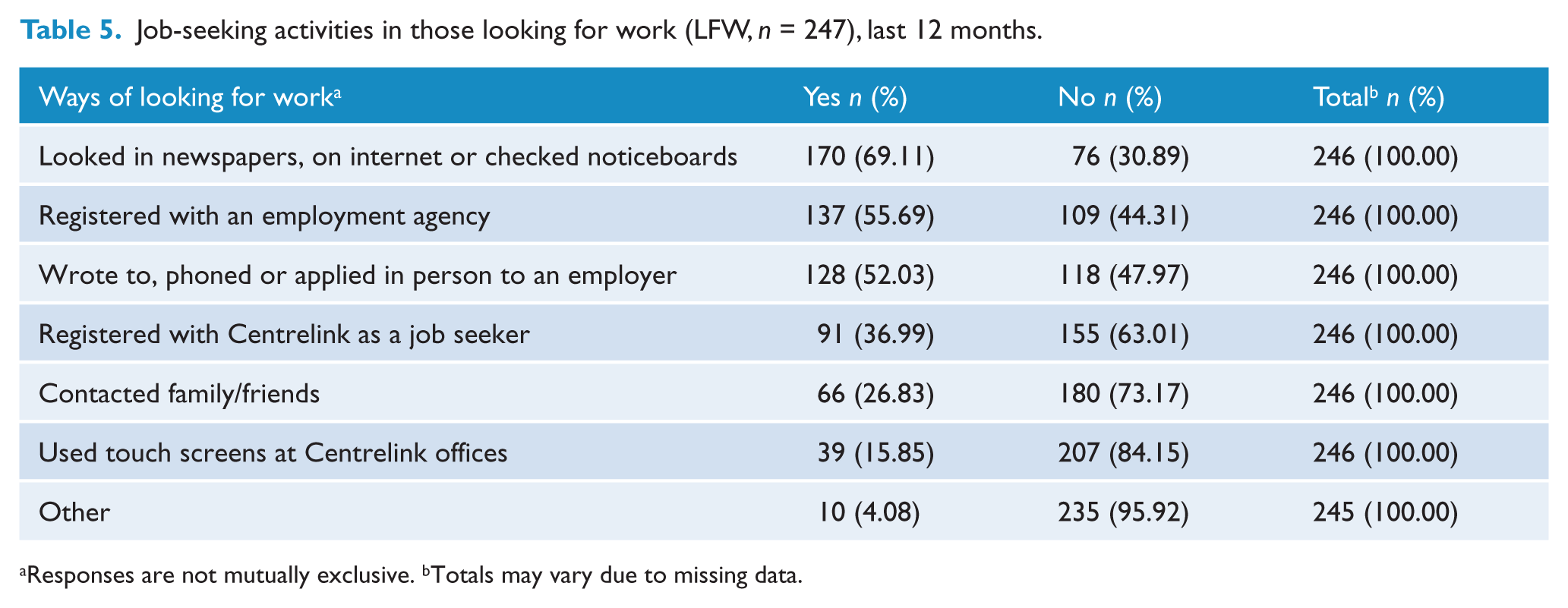
Responses are not mutually exclusive. bTotals may vary due to missing data.
Type of assistance received by those looking for work (LFW, n = 247), last 12 months.
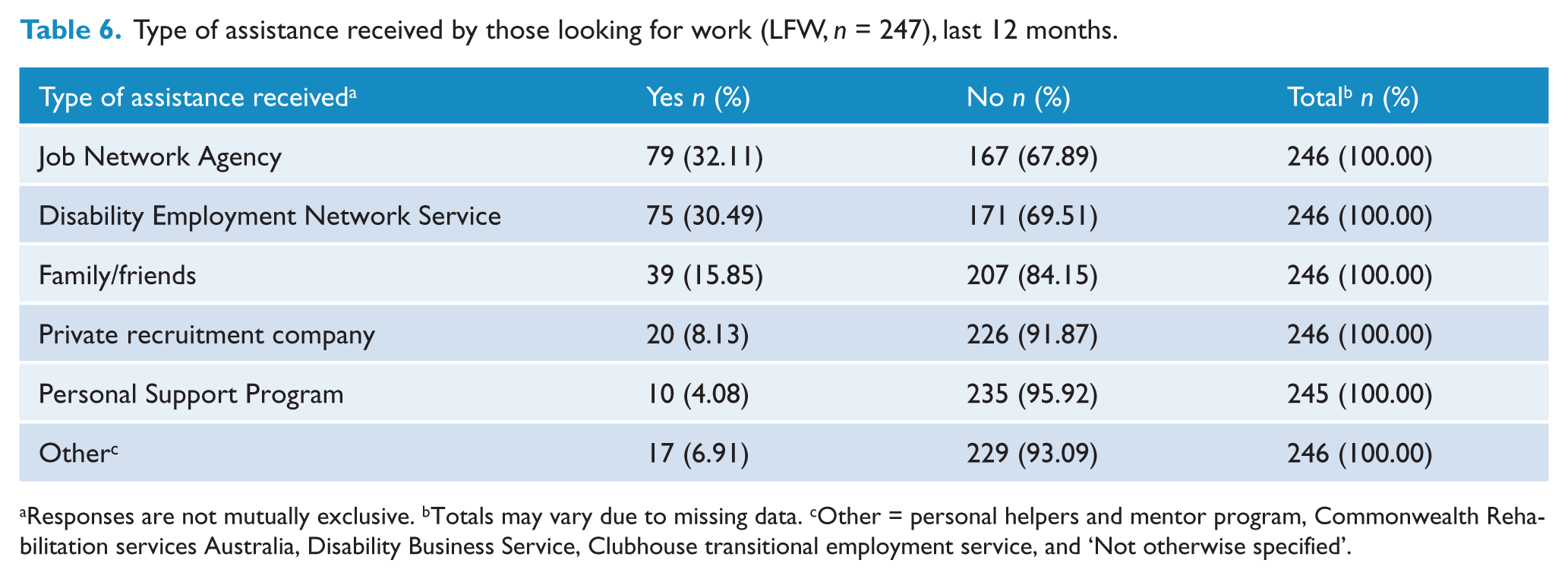
Responses are not mutually exclusive. bTotals may vary due to missing data. cOther = personal helpers and mentor program, Commonwealth Rehabilitation services Australia, Disability Business Service, Clubhouse transitional employment service, and ‘Not otherwise specified’.
Reasons for not participating in the labour force
Among those not participating in the labour force (NILF, n = 982), the most frequently given reasons for not looking for work were: ‘own ill health or physical disability’ (80.1%); ‘not wanting to work’ (31.9%); and ‘lacks necessary schooling, training, skills or experience’ (24.5%). Although 68.1% reported wanting to work, 23.1% feared the impact on welfare payments, and 9.3% endorsed childcare as a reason for not looking for work. Further reasons given included: ‘family considerations’ (7.4%); ‘employers think they are too young or too old’ (7.4%); ‘don’t know what assistance is available to help find work’ (6.1%); ‘ill health of others’ (5.7%); and ‘has difficulties with language or due to ethnic background’ (1.0%). These responses are not mutually exclusive because the survey question permitted more than one reason to be endorsed (Table 7).
Reasons for not looking for work among those not in the work force (NILF, n = 982), last 12 months.
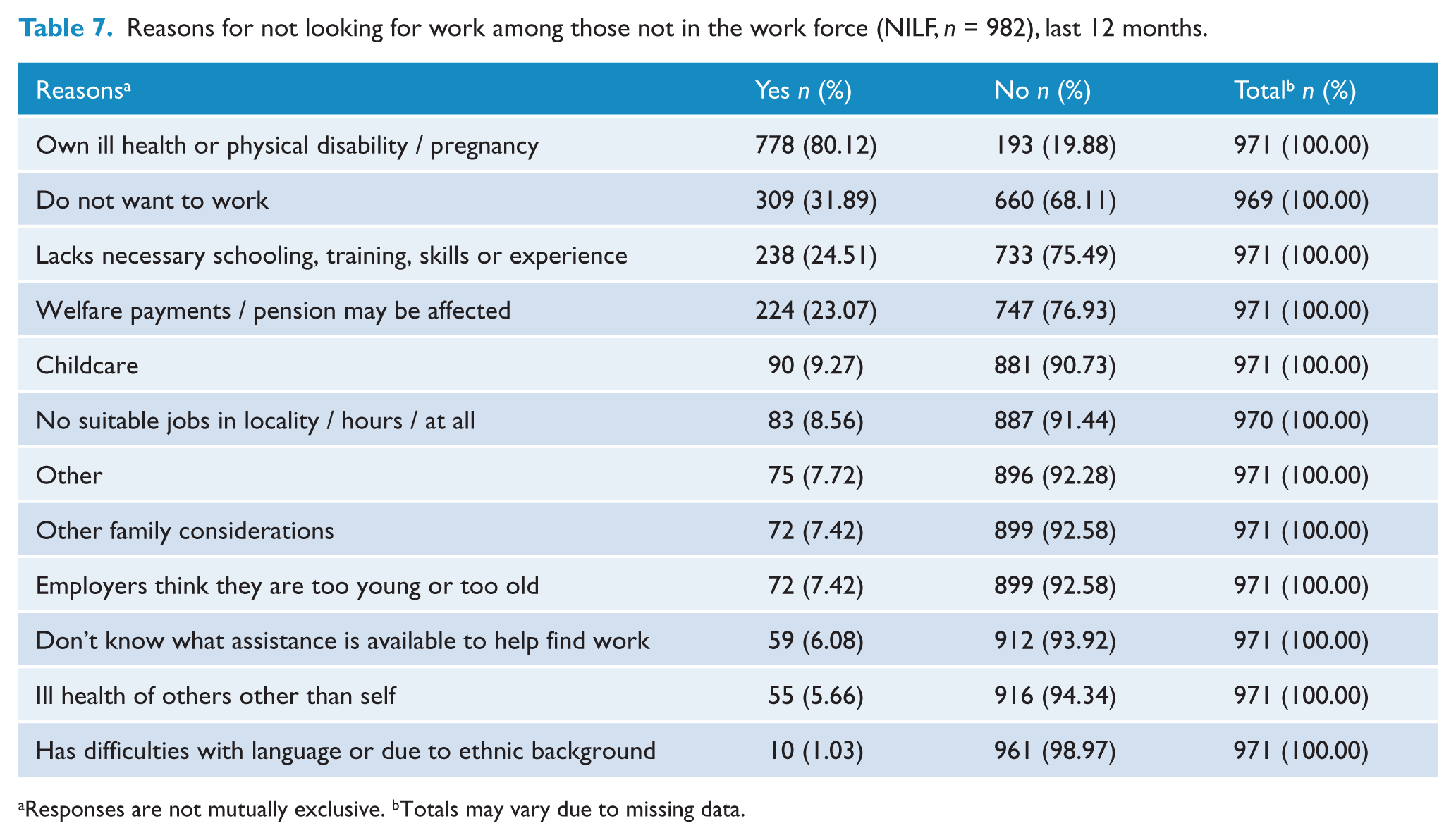
Responses are not mutually exclusive. bTotals may vary due to missing data.
Educational attainment
More males (36.3%) than females (30.6%) did not attain a secondary school or post-school qualification, and more females than males attained post-school qualifications (55.5% vs 45.0%) (Table 8). More migrants held post-school qualifications than Australian-born participants (53.4% vs 48.3%). Those with current partners (57.9%) were more likely to have post-school qualifications than those single or never married (45.3%), or those separated, divorced or widowed (53.6%). Having no secondary school or post-school qualifications was more common in those with schizophrenia (36.6%) or schizoaffective disorder (36.8%) compared to those with bipolar affective disorder (27.6%) and depression with psychosis (25.9%) (Table 9). These differences were all statistically significant. Differences in educational attainment by diagnostic category were also statistically significant (χ2 = 17.52, p = 0.004). There was a negative monotonic gradient between global functioning and the attainment of post-school qualifications (χ2 = 110.59, p < 0.0001).
Demographic correlates of educational attainment among those with psychotic disorders (n = 1825).
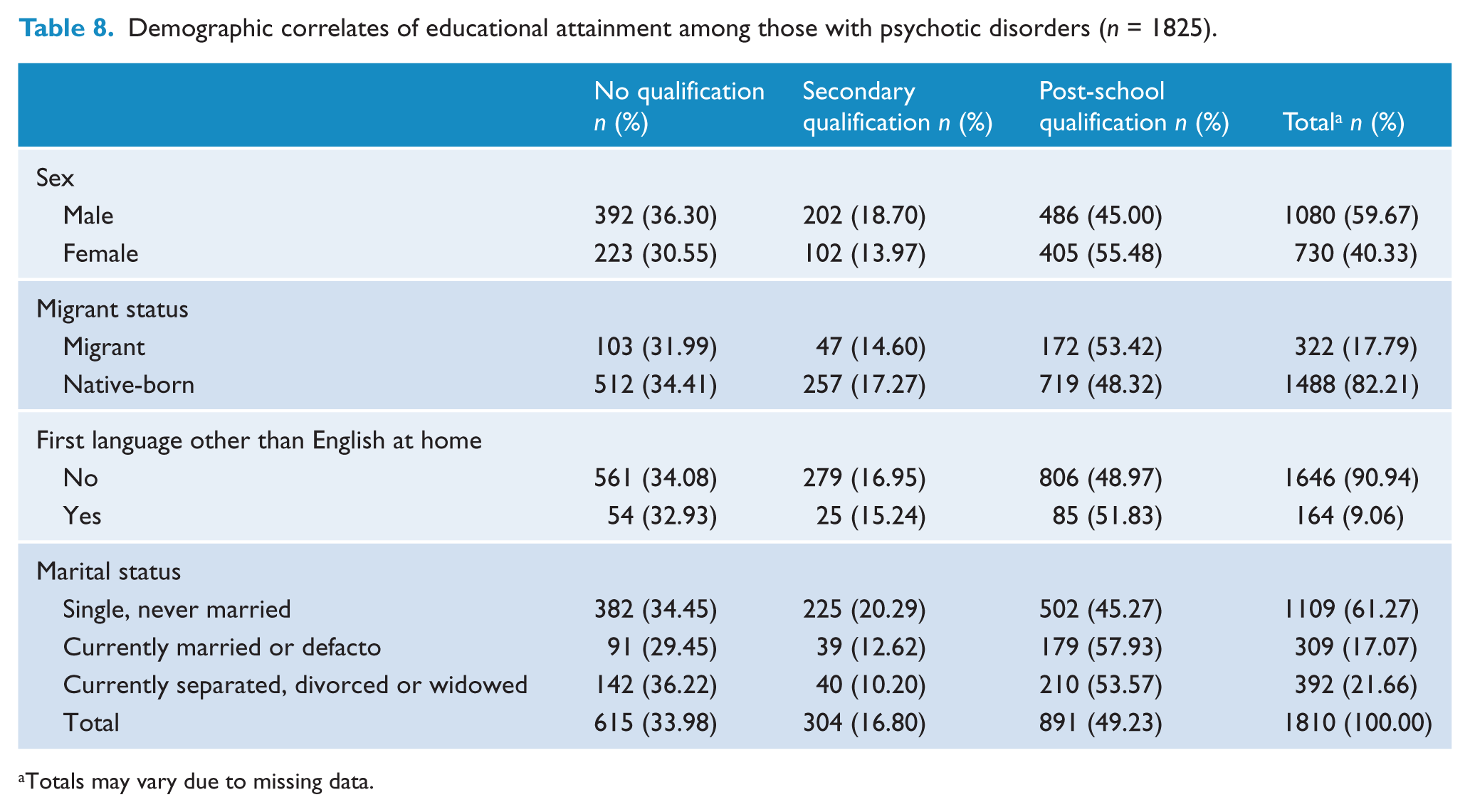
Totals may vary due to missing data.
Educational attainment among those with psychotic disorders (n = 1825).
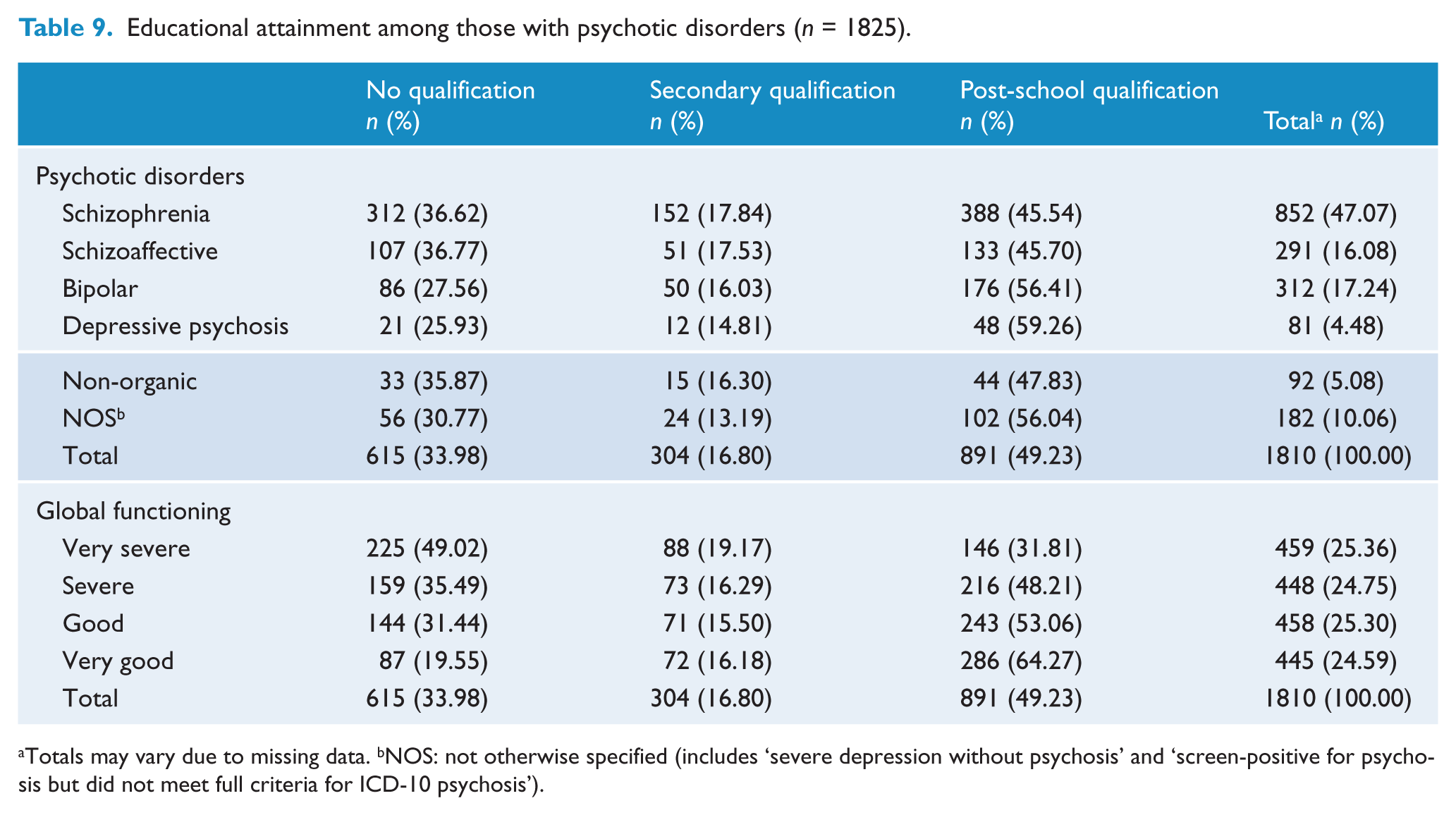
Totals may vary due to missing data. bNOS: not otherwise specified (includes ‘severe depression without psychosis’ and ‘screen-positive for psychosis but did not meet full criteria for ICD-10 psychosis’).
Educational attainment was consistently associated with employment status (Table 10). Thus, those who attained secondary school (χ2 = 62.78, p < 0.0001) or post-school qualifications (χ2 = 35.23, p < 0.0001) were more likely to be currently employed. Employment status increased monotonically with age of leaving school (10–15 years, 13.6%; 16 years, 20.3%; 17–23 years, 29.8%) (χ2 = 51.59, p < 0.0001). In addition, those who reported difficulty with reading and writing were less likely to be employed (16.4%) than those reporting no difficulty (23.7%) (χ2 = 8.43, p = 0.004).
Educational attainment and labour force activity among people with psychotic disorders (n = 1825).

EMP: employed (part-time/full-time); LFW: looking for work; NILF: not in the labour force activity (not looking for work and not employed).
Totals may vary due to missing data.
The impact of global functioning on employment was exacerbated by low educational attainment. Among those with severe or very severe forms of illness, the proportion employed increased from 3.2% (29 of 907) to 6.6% (60 of 907) with high school qualifications. Whereas among those whose global functioning was classified as good to very good, the proportion employed increased with high school qualifications or higher, from 6.6% (60 of 903) to 28.5% (257 of 903).
Discussion
Less than a quarter of individuals with psychotic disorder had been employed in the previous month. Compared with Australia’s first survey of people with psychotic disorders, the overall proportion employed remained stable at 22.2% in 1997 (Waghorn and Chant, 2002) versus 22.4% in 2010. The lack of improvement in employment outcomes is disappointing in light of key changes since the first survey in 1997: (a) a reduction in national unemployment from 8.5% to 5.2%; (b) a national mental health strategy leading to an increased recovery focus for mental health services (Australian Government, 2009a); and (c) continuing improvements to disability employment services since 1997 (Australian Government, 2009b).
Reasons for not participating in the labour force
Unlike the first survey of psychosis in 1997, the SHIP survey enabled a more detailed examination of the utilization of employment services and reasons for not participating in the labour force. Among those looking for work, only 30.5% of people with psychotic disorders had received assistance from the most appropriate type of employment assistance program (Disability Employment Services, previously known as Disability Employment Network services). Worryingly, 32.1% received assistance from the least appropriate source of assistance; that is, mainstream services for unemployed persons (now known as Job Services Australia providers). Since it is not possible to receive both types of assistance concurrently, nor self-select the type of program the participants are referred to, the implication is that the mandatory national job capacity assessment system may be misclassifying up to 30% of people with psychotic disorders, by underestimating their assistance needs. If so, less intensive services will be burdened by many clients who have greater assistance needs than the service typically provides, reducing the likelihood of successful employment.
Regarding reasons for not looking for work, compared to similar reasons endorsed by people with schizophrenia in a previous 2003 population level survey (Waghorn et al., 2011b), ‘own ill health or disability’ was endorsed more frequently in the current survey (80.1% vs 58.4% in 2003); as was ‘lacking necessary schooling, training and experience’ (24.5% vs 5.8% in 2003). Although the reasons for this are unknown, it is possible that respondents in the most recent survey perceived the labour market as more demanding, and subsequently had reduced expectations of success, or experienced a disability-labelling effect after receiving treatment, or in response to assessments for a disability support pension (Waghorn et al., 2011a). If either is the case, such perceptions could be countered by more information about: (a) the feasibility of employment when effective forms of assistance are provided; and (b) how this assistance can be provided in parallel with treatment and care services (Bond, 2004; Bond et al., 2008; Drake and Bond, 2011; Robson et al., 2010). With respect to other reasons for not looking for work, similar proportions endorsed ‘childcare reasons’ (9.3% vs 10.7%) and ‘other’s ill health’ (5.7% vs 5.3%). The ‘effect on welfare payments’ as a reason for not looking for work, was endorsed by 23.1% in 2010, but there was no equivalent reason in the 2003 study. Perceptions of a changing labour market may provide some explanation for the increased endorsements of ‘own ill health or disability’ and ‘lacking necessary schooling, training and experience’ as reasons for not looking for work since 2003. Nevertheless, it is clear that people with psychotic disorders can be easily discouraged from participating in the labour force, and this seems to be exacerbated by perceptions of welfare disincentives, and by the fact that so many end up in the least suitable stream of assistance (Job Services Australia). It is likely that people with psychoses actively weigh up the positives and negatives of employment, and consider job-related, social and societal factors when making employment-related decisions (Fossey and Harvey, 2010). If this is the case, better information could help people with psychotic disorders understand the many incentives available in the welfare system, and the suitable forms of more intensive assistance available when choosing a competitive employment pathway.
Competitive and non-competitive employment
The findings with respect to competitive and non-competitive employment were particularly informative. The first Australian survey of psychosis in 1997 did not differentiate competitive from non-competitive forms of employment. Of those employed during the previous year, 17.2% worked in non-competitive employment. Although at least some of the people with non-competitive employment may have chosen this type of employment, it is likely that a proportion were directed to this assistance as a result of the mandatory job capacity assessment. Among those currently employed whose illness was classified as very severe, the majority (61.7%) was competitively employed (only 38.3% were in non-competitive employment). This suggests that illness and disability is not a valid criterion by which to stream people into either competitive or non-competitive forms of employment. These results suggest that participant (job-seekers’) preferences, rather than global functioning and disability, ought to be considered during mandatory job capacity assessments where people are directed to different types of employment programs.
Although the proportion of people with psychotic disorders in current employment is low, three to five times lower than for the general population in 2010, this is in line with results from studies from the UK and USA (O’Brien et al., 2002; Mechanic et al., 2002; Zwerling et al., 2002). While these studies were based on schizophrenia rather than the broader category of psychotic disorders (as was used in the current study), we found that key employment outcomes did not differ significantly by diagnosis. This suggests that the restricted/limited employment of people with psychotic disorders in Australia is a problem of similar magnitude compared to other developed market economies.
Educational qualifications
The survey also confirms that many individuals with psychosis have suboptimal educational outcomes, and, unsurprisingly, these same individuals tend to do worse on employment outcomes. Services should remain mindful that their clients may have experienced disruption to educational and vocational training opportunities, and that these factors warrant due recognition in recovery programs, or more direct action as per Robson et al. (2010). Hopefully, recent Commonwealth funding related to readily accessible services for adolescents and young adults with mental health problems may ameliorate the impact of psychotic disorders on educational achievements. Additional research to identify the best ways to assist people with mental illnesses of all ages in pursuing their educational goals is also warranted.
Limitations and future studies
The survey design did not include those entirely in the care of private mental health providers (e.g. general practitioners or psychiatrists), nor those who had dropped out of all contact with agencies (e.g. it is feasible that these individuals may have better employment outcomes). Only those 18 years of age and higher were eligible for inclusion, hence the survey does not estimate the impact of psychotic disorders on educational and vocational outcomes in those aged 15–18 years.
In addition, the majority of labour force activity questions were asked in a 12-month context, rather than from a 7-day or 1-month timeframe; thus, fine-grained information about time course and relative proportion of different types of labour force activity was not obtained. For instance, the variable actively looking for work was only available in a 12-month context. While this may seem problematic, it was not a major limitation because the boundary between looking for work and not participating in the labour force, as defined in labour force surveys, is difficult to measure among people with psychotic disorders. This is because many receive sickness benefits or a disability support pension, and consequently may not have obligations to look for work, although they may in fact be interested in employment and keen to take up employment opportunities. Second, whether or not they have obligations to look for work, being currently registered with a government-funded employment agency would usually meet those obligations. We managed this limitation by collapsing the three mutually exclusive categories of labour force activity (employed, looking for work, or not in the labour force) into two categories (employed vs not employed). This does not change the meaning of ‘employed’ or ‘not employed’ because in labour force survey terminology ‘not employed’ includes those ‘actively looking for work’ as well as those ‘not looking for work’ who are, by definition, considered ‘not in the labour force’.
Limited information was available about the nature of competitive and non-competitive forms of employment. Although these categories were differentiated better than in previous population level surveys, it would be helpful to know more about conditions of current employment (e.g. whether the job was reserved for people with disabilities, or in a family owned business, a Social Firm, a Business Enterprise funded by the Australian Government, or whether it is a temporary job, a job under the Supported Wage Scheme, or a job where the employer received a wage subsidy etc.). We plan to explore the correlates of competitive versus non-competitive employment in more detail in future publications. In addition, we plan to explore if comorbid physical disorders (which are common in those with psychotic disorders) may have contributed to this initial analysis.
Conclusions
Psychotic disorders continue to be a major source of disruption to educational attainment and to participation in the labour force. However, much of this vocational disruption is avoidable and is not a necessary consequence of having a psychotic disorder. Barriers to employment at an individual level are also well known (Caltruax, 2003; Corrigan and Watson, 2002; Rinaldi et al., 2008; Rutman, 1994; Waghorn and Lloyd, 2005; Waghorn et al., 2009). In addition, low expectations among health professionals (Blankertz and Robinson, 1996) and discrimination from potential employers (Kay et al., 2011) contribute to poor employment outcomes. Intensive programs have been developed to support adults with psychotic disorders to return to high school and to higher education (Mowbray et al., 1999). Programs are also available that have proven successful in establishing competitive employment for 60% or more of program volunteers (Bond, 2004; Bond et al., 2008; Drake and Bond, 2011). While progress has been made in recent years, these programs are still not yet widely available in Australia. Employment issues were identified by the participants of the SHIP as one of the top three challenges they face (Morgan et al., 2012). The finding that a large gap remains between the aspirations of people with psychotic disorders and their actual educational attainment and participation in the labour force, implies that policy makers can do more to ensure the availability of intensive and effective forms of education and employment assistance for people with psychotic disorders.
Footnotes
Acknowledgements
This publication is based on data collected in the framework of the 2010 Australian National Survey of High Impact Psychosis. Members of the Survey of High Impact Psychosis Study Group are: V Morgan (Project Director); A Jablensky (Chief Scientific Advisor); A Waterreus (Project Coordinator); A Mackinnon (Statistician); R Bush, D Castle, M Cohen, C Galletly, C Harvey, P McGorry, J McGrath, H Stain (Site Directors); V Carr (Australian Schizophrenia Research Bank); A Neil (Health Economics); B Hocking (SANE Australia); and S Saw (Australian Government Department of Health and Ageing). Ethics approvals for the study were obtained from relevant institutional human research ethics committees. The study was funded by the Australian Government Department of Health and Ageing. This report acknowledges, with thanks, the hundreds of mental health professionals who participated in the preparation and conduct of the survey and the many Australians with psychotic disorders who gave their time and whose responses form the basis of this publication.
Funding
This research was funded under contract to the Australian Government Department of Health and Ageing
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.